
Targeted Genomic Profiling and Chemotherapy Outcomes in Grade 3 Gastro-Entero-Pancreatic Neuroendocrine Tumors (G3 GEP-NET)

 , , ,
, , ,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
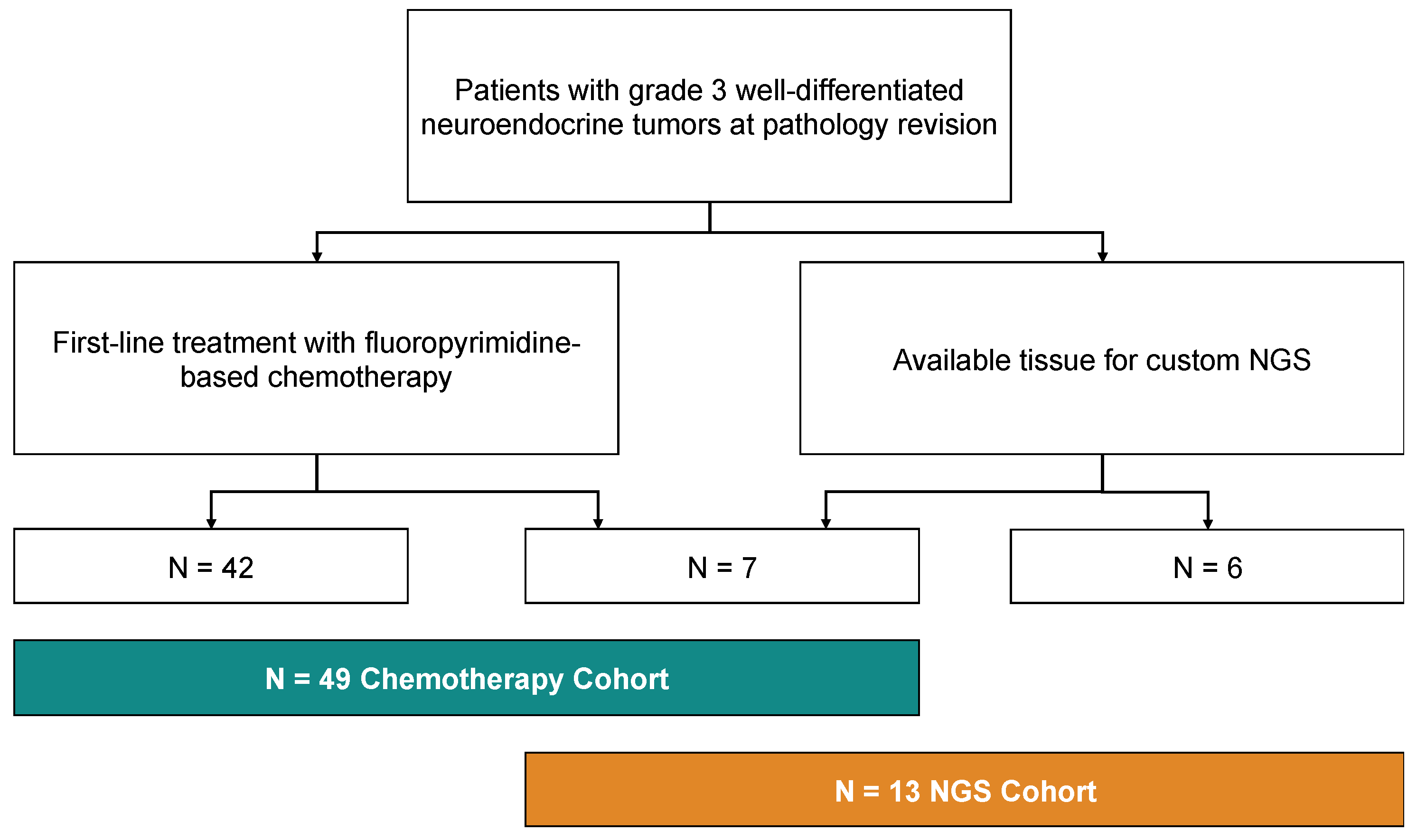
2.1. Patient Selection
2.2. Next-Generation Sequencing
2.3. Statistical Analysis
3. Results
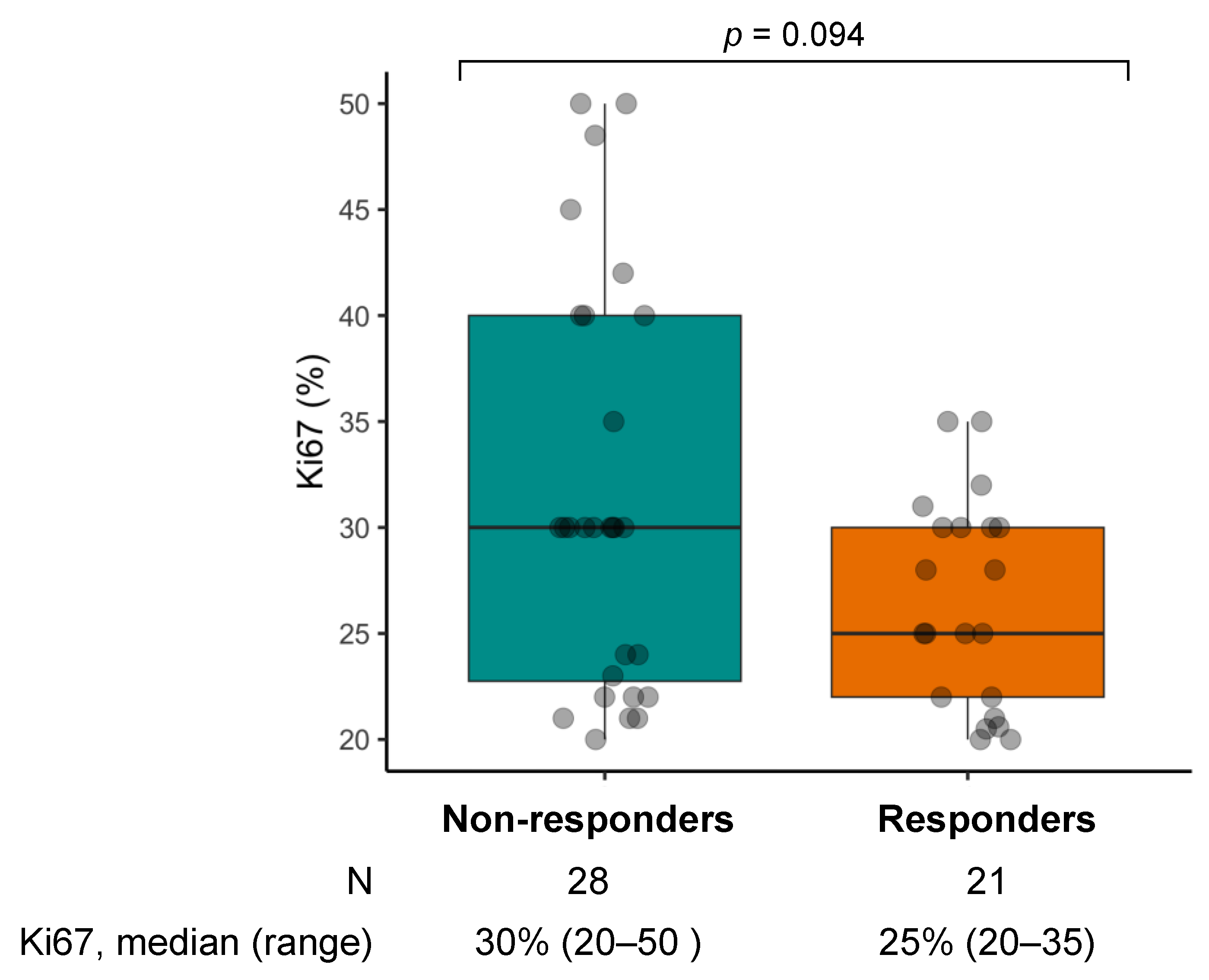
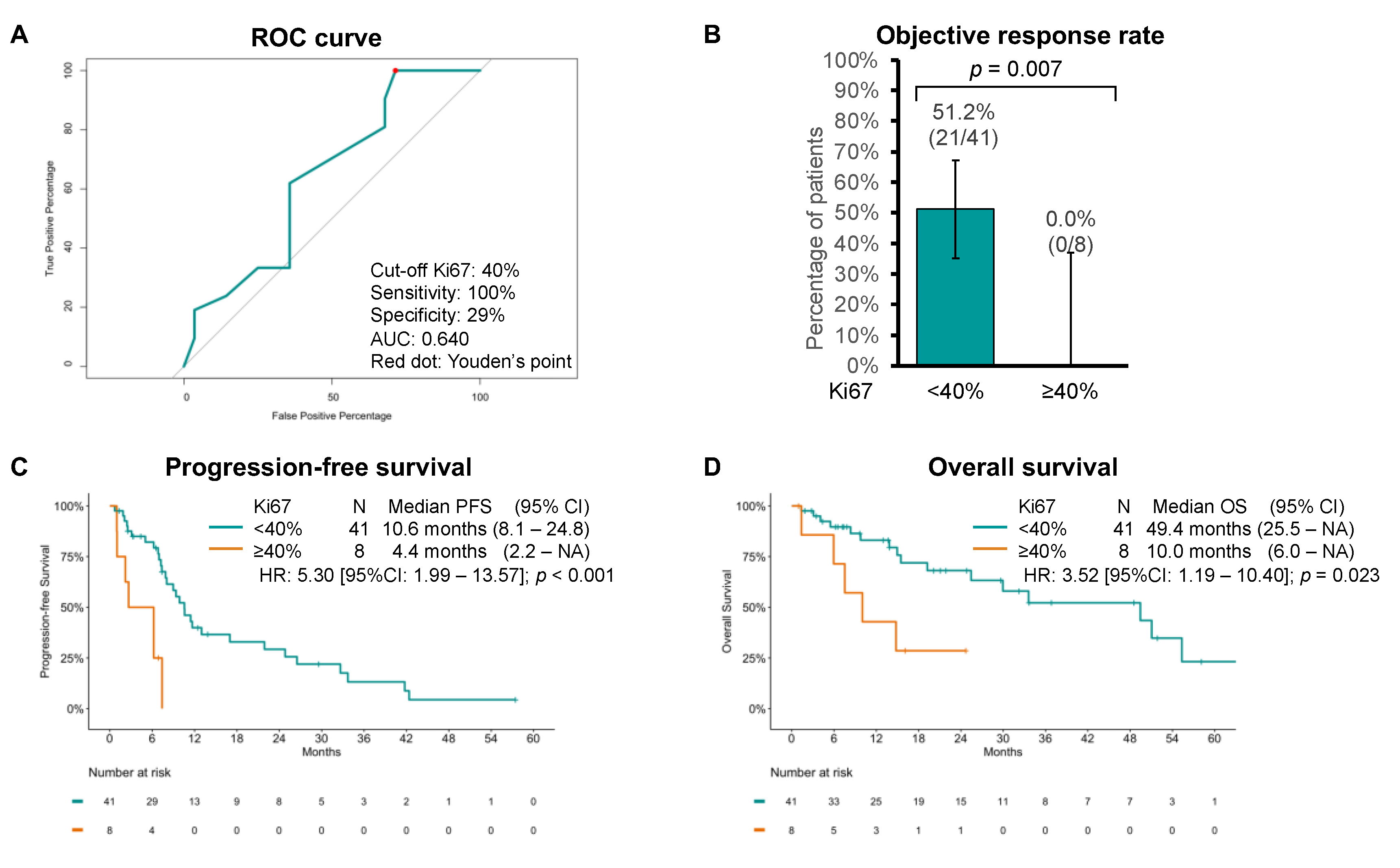
3.1. Chemotherapy Cohort
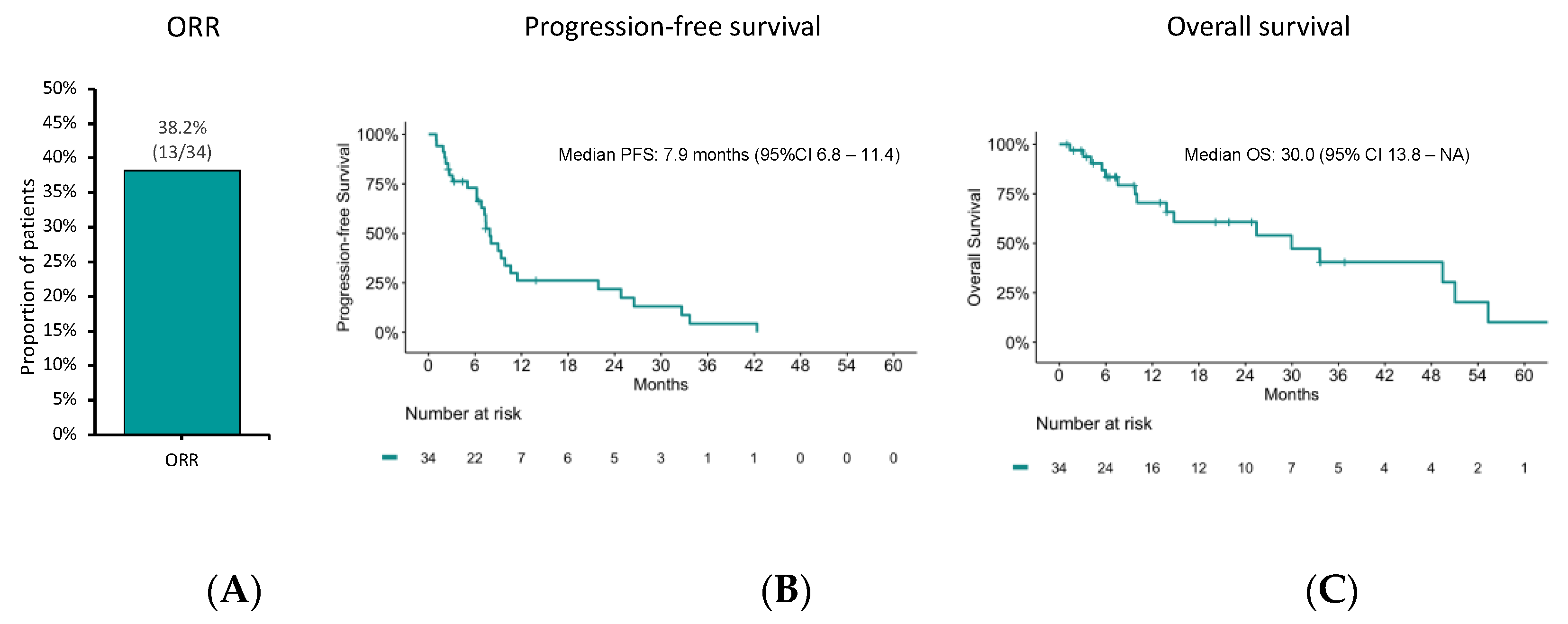
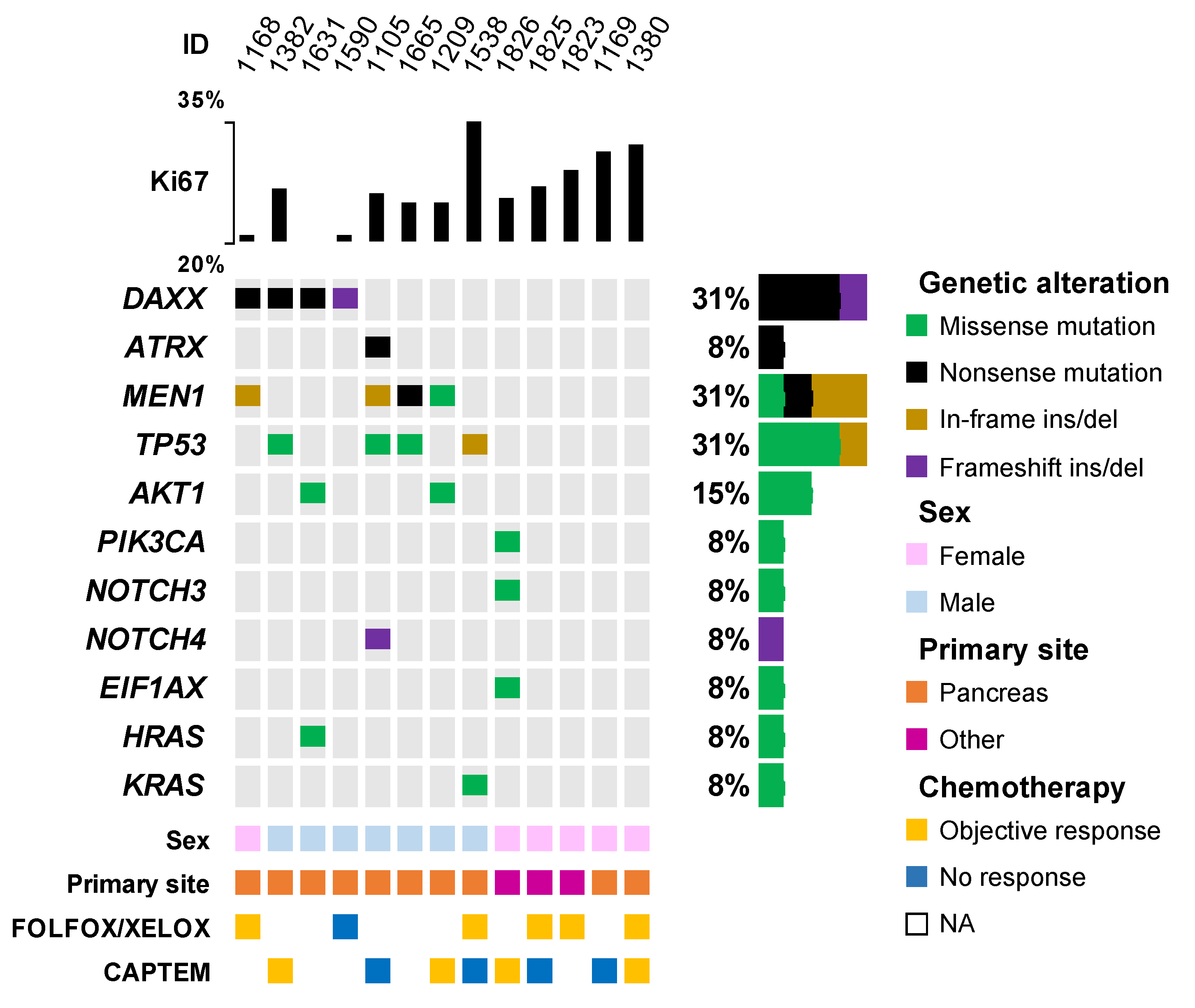
3.2. NGS Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.M.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Zappi, A.; Persano, I.; Galvani, L.; Parlagreco, E.; Andrini, E.; Campana, D.; Brizzi, M.P.; Lamberti, G.; La Salvia, A. Chemotherapy in Well Differentiated Neuroendocrine Tumors (NET) G1, G2, and G3: A Narrative Review. J. Clin. Med. 2023, 12, 717. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.-F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Sorbye, H.; Welin, S.; Langer, S.W.; Vestermark, L.W.; Holt, N.; Osterlund, P.; Dueland, S.; Hofsli, E.; Guren, M.G.; Ohrling, K.; et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): The NORDIC NEC study. Ann. Oncol. 2013, 24, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Chakravarty, D.; Gao, J.; Phillips, S.; Kundra, R.; Zhang, H.; Wang, J.; Rudolph, J.E.; Yaeger, R.; Soumerai, T.; Nissan, M.H.; et al. OncoKB: A Precision Oncology Knowledge Base. JCO Precis. Oncol. 2017, 2017, 1–16. [Google Scholar] [CrossRef]
- Landrum, M.J.; Lee, J.M.; Benson, M.; Brown, G.R.; Chao, C.; Chitipiralla, S.; Gu, B.; Hart, J.; Hoffman, D.; Jang, W.; et al. ClinVar: Improving access to variant interpretations and supporting evidence. Nucleic Acids Res. 2017, 46, D1062–D1067. [Google Scholar] [CrossRef]
- Adzhubei, I.A.; Schmidt, S.; Peshkin, L.; Ramensky, V.E.; Gerasimova, A.; Bork, P.; Kondrashov, A.S.; Sunyaev, S.R. A method and server for predicting damaging missense mutations. Nat. Methods 2010, 7, 248–249. [Google Scholar] [CrossRef]
- Yin, J.; Tian, L. Joint confidence region estimation for area under ROC curve and Youden index. Stat. Med. 2013, 33, 985–1000. [Google Scholar] [CrossRef]
- Kunz, P.L.; Graham, N.T.; Catalano, P.J.; Nimeiri, H.S.; Fisher, G.A.; Longacre, T.A.; Suarez, C.J.; Martin, B.A.; Yao, J.C.; Kulke, M.H.; et al. Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendocrine Tumors (ECOG-ACRIN E2211). J. Clin. Oncol. 2022, 41, 1359–1369. [Google Scholar] [CrossRef] [PubMed]
- Elvebakken, H.; Perren, A.; Scoazec, J.-Y.; Tang, L.H.; Federspiel, B.; Klimstra, D.S.; Vestermark, L.W.; Ali, A.S.; Zlobec, I.; Myklebust, T.Å.; et al. A Consensus-Developed Morphological Re-Evaluation of 196 High-Grade Gastroenteropancreatic Neuroendocrine Neoplasms and Its Clinical Correlations. Neuroendocrinology 2020, 111, 883–894. [Google Scholar] [CrossRef]
- Rinke, A.; Müller, H.-H.; Schade-Brittinger, C.; Klose, K.-J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.-F.; Bläker, M.; et al. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors: A Report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Pavel, M.; Cwikla, J.B.; Phan, A.T.; Raderer, M.; Sedlackova, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Anti-tumour effects of lanreotide for pancreatic and intestinal neuroendocrine tumours: The CLARINET open-label extension study. Endocr. Relat. Cancer 2016, 23, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.; Ćwikła, J.B.; Lombard-Bohas, C.; Borbath, I.; Shah, T.; Pape, U.F.; Capdevila, J.; Panzuto, F.; Thanh, X.-M.T.; Houchard, A.; et al. Efficacy and safety of high-dose lanreotide autogel in patients with progressive pancreatic or midgut neuroendocrine tumours: CLARINET FORTE phase 2 study results. Eur. J. Cancer 2021, 157, 403–414. [Google Scholar] [CrossRef]
- Lamberti, G.; Faggiano, A.; Brighi, N.; Tafuto, S.; Ibrahim, T.; Brizzi, M.P.; Pusceddu, S.; Albertelli, M.; Massironi, S.; Panzuto, F.; et al. Nonconventional Doses of Somatostatin Analogs in Patients with Progressing Well-Differentiated Neuroendocrine Tumor. J. Clin. Endocrinol. Metab. 2020, 105, 194–200. [Google Scholar] [CrossRef]
- Ricci, C.; Lamberti, G.; Ingaldi, C.; Mosconi, C.; Pagano, N.; Alberici, L.; Ambrosini, V.; Manuzzi, L.; Monari, F.; Malvi, D.; et al. Treatment of Advanced Gastro-Entero-Pancreatic Neuro-Endocrine Tumors: A Systematic Review and Network Meta-Analysis of Phase III Randomized Controlled Trials. Cancers 2021, 13, 358. [Google Scholar] [CrossRef]
- Fazio, N.; Buzzoni, R.; Fave, G.D.; Tesselaar, M.E.; Wolin, E.; Van Cutsem, E.; Tomassetti, P.; Strosberg, J.; Voi, M.; Bubuteishvili-Pacaud, L.; et al. Everolimus in advanced, progressive, well-differentiated, non-functional neuroendocrine tumors: RADIANT-4 lung subgroup analysis. Cancer Sci. 2017, 109, 174–181. [Google Scholar] [CrossRef]
- Yao, J.C.; Pavel, M.; Lombard-Bohas, C.; Van Cutsem, E.; Voi, M.; Brandt, U.; He, W.; Chen, D.; Capdevila, J.; De Vries, E.G.E.; et al. Everolimus for the Treatment of Advanced Pancreatic Neuroendocrine Tumors: Overall Survival and Circulating Biomarkers from the Randomized, Phase III RADIANT-3 Study. J. Clin. Oncol. 2016, 34, 3906–3913. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.-L.; Bang, Y.-J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib Malate for the Treatment of Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef]
- Fine, R.L.; Gulati, A.P.; Tsushima, D.; Mowatt, K.B.; Oprescu, A.; Bruce, J.N.; Chabot, J.A. Prospective phase II study of capecitabine and temozolomide (CAPTEM) for progressive, moderately, and well-differentiated metastatic neuroendocrine tumors. J. Clin. Oncol. 2014, 32, 179. [Google Scholar] [CrossRef]
- de Mestier, L.; Walter, T.; Brixi, H.; Evrard, C.; Legoux, J.-L.; de Boissieu, P.; Hentic, O.; Cros, J.; Hammel, P.; Tougeron, D.; et al. Comparison of Temozolomide-Capecitabine to 5-Fluorouracile-Dacarbazine in 247 Patients with Advanced Digestive Neuroendocrine Tumors Using Propensity Score Analyses. Neuroendocrinology 2019, 108, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Spada, F.; Fumagalli, C.; Antonuzzo, L.; Messerini, L.; Radice, D.; Di Rocco, R.; Galdy, S.; Barucca, V.; Pisa, E.; Barberis, M.; et al. Capecitabine plus temozolomide (CAP-TEM) in patients with advanced neuroendocrine neoplasms (NEN): An Italian multicenter retrospective analysis. J. Clin. Oncol. 2014, 32, 281. [Google Scholar] [CrossRef]
- Strosberg, J.R.; Fine, R.L.; Choi, J.; Nasir, A.; Coppola, D.; Chen, D.-T.; Helm, J.; Kvols, L. First-line chemotherapy with capecitabine and temozolomide in patients with metastatic pancreatic endocrine carcinomas. Cancer 2010, 117, 268–275. [Google Scholar] [CrossRef]
- Campana, D.; Walter, T.; Pusceddu, S.; Gelsomino, F.; Graillot, E.; Prinzi, N.; Spallanzani, A.; Fiorentino, M.; Barritault, M.; Dall’olio, F.; et al. Correlation between MGMT promoter methylation and response to temozolomide-based therapy in neuroendocrine neoplasms: An observational retrospective multicenter study. Endocrine 2018, 60, 490–498. [Google Scholar] [CrossRef]
- Saranga-Perry, V.; Morse, B.; Centeno, B.; Kvols, L.; Strosberg, J. Treatment of Metastatic Neuroendocrine Tumors of the Thymus with Capecitabine and Temozolomide: A Case Series. Neuroendocrinology 2013, 97, 318–321. [Google Scholar] [CrossRef]
- Ekeblad, S.; Sundin, A.; Janson, E.T.; Welin, S.; Granberg, D.; Kindmark, H.; Dunder, K.; Kozlovacki, G.; Orlefors, H.; Sigurd, M.; et al. Temozolomide as Monotherapy Is Effective in Treatment of Advanced Malignant Neuroendocrine Tumors. Clin. Cancer Res. 2007, 13, 2986–2991. [Google Scholar] [CrossRef]
- Bongiovanni, A.; Liverani, C.; Foca, F.; Fausti, V.; Di Menna, G.; Mercatali, L.; De Vita, A.; Riva, N.; Calpona, S.; Miserocchi, G.; et al. Temozolomide Alone or Combined with Capecitabine for the Treatment of Metastatic Neuroendocrine Neoplasia: A “Real-World” Data Analysis. Neuroendocrinology 2021, 111, 895–906. [Google Scholar] [CrossRef]
- Raj, N.; Klimstra, D.S.; Horvat, N.; Zhang, L.; Chou, J.F.; Capanu, M.; Basturk, O.; Do, R.K.G.; Allen, P.J.; Reidy-Lagunes, D. O6-Methylguanine DNA Methyltransferase Status Does Not Predict Response or Resistance to Alkylating Agents in Well-Differentiated Pancreatic Neuroendocrine Tumors. Pancreas 2017, 46, 758–763. [Google Scholar] [CrossRef]
- Merola, E.; Buono, A.D.; Denecke, T.; Arsenic, R.; Pape, U.-F.; Jann, H.; Wiedenmann, B.; Pavel, M.E. Efficacy and Toxicity of 5-Fluorouracil–Oxaliplatin in Gastroenteropancreatic Neuroendocrine Neoplasms. Pancreas 2020, 49, 912–917. [Google Scholar] [CrossRef]
- Spada, F.; Antonuzzo, L.; Marconcini, R.; Radice, D.; Antonuzzo, A.; Ricci, S.; Di Costanzo, F.; Fontana, A.; Gelsomino, F.; Luppi, G.; et al. Oxaliplatin-Based Chemotherapy in Advanced Neuroendocrine Tumors: Clinical Outcomes and Preliminary Correlation with Biological Factors. Neuroendocrinology 2016, 103, 806–814. [Google Scholar] [CrossRef]
- Al-Toubah, T.; Morse, B.; Pelle, E.; Strosberg, J. Efficacy of FOLFOX in Patients with Aggressive Pancreatic Neuroendocrine Tumors after Prior Capecitabine/Temozolomide. Oncologist 2021, 26, 115–119. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, Y.; Peng, Y.; Jin, K.-Z.; Li, Y.-L.; Liang, Y.; Tan, H.-Y.; Yu, X.-J.; Zhou, Z.-W.; Chen, J. A Ki-67 Index to Predict Treatment Response to the Capecitabine/Temozolomide Regimen in Neuroendocrine Neoplasms: A Retrospective Multicenter Study. Neuroendocrinology 2020, 111, 752–763. [Google Scholar] [CrossRef] [PubMed]
- Scarpa, A.; Chang, D.K.; Nones, K.; Corbo, V.; Patch, A.-M.; Bailey, P.; Lawlor, R.T.; Johns, A.L.; Miller, D.K.; Mafficini, A.; et al. Whole-genome landscape of pancreatic neuroendocrine tumours. Nature 2017, 543, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Kwon, M.J.; Kang, H.S.; Kim, Y.J.; Kim, N.Y.; Kim, M.J.; Min, K.-W.; Choi, K.C.; Nam, E.S.; Cho, S.J.; et al. Targeted next-generation sequencing of well-differentiated rectal, gastric, and appendiceal neuroendocrine tumors to identify potential targets. Hum. Pathol. 2019, 87, 83–94. [Google Scholar] [CrossRef]
- Samsom, K.G.; Levy, S.; van Veenendaal, L.M.; Roepman, P.; Kodach, L.L.; Steeghs, N.; Valk, G.D.; Dercksen, M.W.; Kuhlmann, K.F.; Verbeek, W.H.; et al. Driver mutations occur frequently in metastases of well-differentiated small intestine neuroendocrine tumours. Histopathology 2020, 78, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Garg, A.; Chen, D.; Capdevila, J.; Engstrom, P.; Pommier, R.; Van Cutsem, E.; Singh, S.; Fazio, N.; He, W.; et al. Genomic profiling of NETs: A comprehensive analysis of the RADIANT trials. Endocr. Relat. Cancer 2019, 26, 391–403. [Google Scholar] [CrossRef]
- Puccini, A.; Poorman, K.; Salem, M.E.; Soldato, D.; Seeber, A.; Goldberg, R.M.; Shields, A.F.; Xiu, J.; Battaglin, F.; Berger, M.D.; et al. Comprehensive Genomic Profiling of Gastroenteropancreatic Neuroendocrine Neoplasms (GEP-NENs). Clin. Cancer Res. 2020, 26, 5943–5951. [Google Scholar] [CrossRef]
- Lee, S.M.; Sung, C.O. Comprehensive analysis of mutational and clinicopathologic characteristics of poorly differentiated colorectal neuroendocrine carcinomas. Sci. Rep. 2021, 11, 6203. [Google Scholar] [CrossRef]
- Yachida, S.; Totoki, Y.; Noë, M.; Nakatani, Y.; Horie, M.; Kawasaki, K.; Nakamura, H.; Saito-Adachi, M.; Suzuki, M.; Takai, E.; et al. Comprehensive Genomic Profiling of Neuroendocrine Carcinomas of the Gastrointestinal System. Cancer Discov. 2022, 12, 692–711. [Google Scholar] [CrossRef]
- Idrees, K.; Padmanabhan, C.; Liu, E.; Guo, Y.; Gonzalez, R.S.; Berlin, J.; Dahlman, K.B.; Beauchamp, R.D.; Shi, C. Frequent BRAF mutations suggest a novel oncogenic driver in colonic neuroendocrine carcinoma. J. Surg. Oncol. 2018, 117, 284–289. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (N= 49) | CAPTEM (N= 15) | FOLFOX/XELOX (N= 34) | p | |
|---|---|---|---|---|
| Age | ||||
| Median [range] | 60.0 [18.0, 80.0] | 63.0 [39.0, 77.0] | 58.5 [18.0, 80.0] | 0.345 |
| Site of primary | ||||
| Pancreas | 32 (65.3%) | 10 (66.7%) | 22 (64.7%) | 1.00 |
| GI | 17 (34.7%) | 5 (33.3%) | 12 (35.3%) | |
| Stage | ||||
| IIIB | 4 (8.16%) | 2 (13.3%) | 2 (5.88%) | 0.576 |
| IV | 45 (91.8%) | 13 (86.7%) | 32 (94.1%) | |
| Ki67 | ||||
| Median [range] | 30.0 [20.0, 50.0] | 28.0 [20.0, 48.5] | 30.0 [20.0, 50.0] | 0.599 |
| 18F-FDG-PET | ||||
| Negative | 3 (11.5%) | 3 (30.0%) | 0 (0%) | 0.046 |
| Positive | 23 (88.5%) | 7 (70.0%) | 16 (100%) | |
| 68Ga-DOTANOC-PET | ||||
| Negative | 10 (25.0%) | 3 (27.3%) | 7 (24.1%) | 1.00 |
| Positive | 30 (75.0%) | 8 (72.7%) | 22 (75.9%) | |
| Concomitant use of SSA | 25 (51.0%) | 9 (60.0%) | 16 (47.1%) | 0.538 |
| Overall (N = 13) | |
|---|---|
| Age | |
| Median [range] | 53.0 [18.0, 83.0] |
| Sex | |
| Female | 6 (46%) |
| Male | 7 (54%) |
| Site of primary | |
| Pancreas | 10 (77%) |
| Other * | 3 (33%) |
| Stage | |
| IIIB | 5 (38%) |
| IV | 8 (62%) |
| Ki67 | |
| Median [range] | 26.5 [21.0, 35.0] |
| 18F-FDG-PET/CT | |
| Negative | 1 (11%) |
| Positive | 8 (89%) |
| 68Ga-DOTANOC-PET/CT | |
| Negative | 0 (0%) |
| Positive | 10 (100%) |
| Chemotherapy | |
| FOLFOX/XELOX | 6 (46%) |
| CAPTEM | 10 (69%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamberti, G.; Prinzi, N.; Bongiovanni, A.; Torniai, M.; Andrini, E.; Biase, D.d.; Malvi, D.; Mosca, M.; Berardi, R.; Ibrahim, T.; et al. Targeted Genomic Profiling and Chemotherapy Outcomes in Grade 3 Gastro-Entero-Pancreatic Neuroendocrine Tumors (G3 GEP-NET). Diagnostics 2023, 13, 1595. https://doi.org/10.3390/diagnostics13091595
Lamberti G, Prinzi N, Bongiovanni A, Torniai M, Andrini E, Biase Dd, Malvi D, Mosca M, Berardi R, Ibrahim T, et al. Targeted Genomic Profiling and Chemotherapy Outcomes in Grade 3 Gastro-Entero-Pancreatic Neuroendocrine Tumors (G3 GEP-NET). Diagnostics. 2023; 13(9):1595. https://doi.org/10.3390/diagnostics13091595
Chicago/Turabian StyleLamberti, Giuseppe, Natalie Prinzi, Alberto Bongiovanni, Mariangela Torniai, Elisa Andrini, Dario de Biase, Deborah Malvi, Mirta Mosca, Rossana Berardi, Toni Ibrahim, and et al. 2023. "Targeted Genomic Profiling and Chemotherapy Outcomes in Grade 3 Gastro-Entero-Pancreatic Neuroendocrine Tumors (G3 GEP-NET)" Diagnostics 13, no. 9: 1595. https://doi.org/10.3390/diagnostics13091595
APA StyleLamberti, G., Prinzi, N., Bongiovanni, A., Torniai, M., Andrini, E., Biase, D. d., Malvi, D., Mosca, M., Berardi, R., Ibrahim, T., Pusceddu, S., & Campana, D. (2023). Targeted Genomic Profiling and Chemotherapy Outcomes in Grade 3 Gastro-Entero-Pancreatic Neuroendocrine Tumors (G3 GEP-NET). Diagnostics, 13(9), 1595. https://doi.org/10.3390/diagnostics13091595