
Computational Intelligence in Cancer Diagnostics: A Contemporary Review of Smart Phone Apps, Current Problems, and Future Research Potentials

 ,
,  , and
, and 
Abstract
1. Introduction
1.1. Contribution of This Review
- We provide a comprehensive study on the various machine learning and deep learning models used for cancer diagnosis. A brief explanation of several machine learning and deep learning methodologies is included;
- A contemporary review of cancer diagnosis as well as an application-oriented analysis of their datasets is given;
- We highlight the current open challenges and future research possibilities in cancer diagnosis for aspiring researchers and enthusiasts to investigate;
- We have covered almost all types of cancer diagnosis, which is a unique feature of our paper.
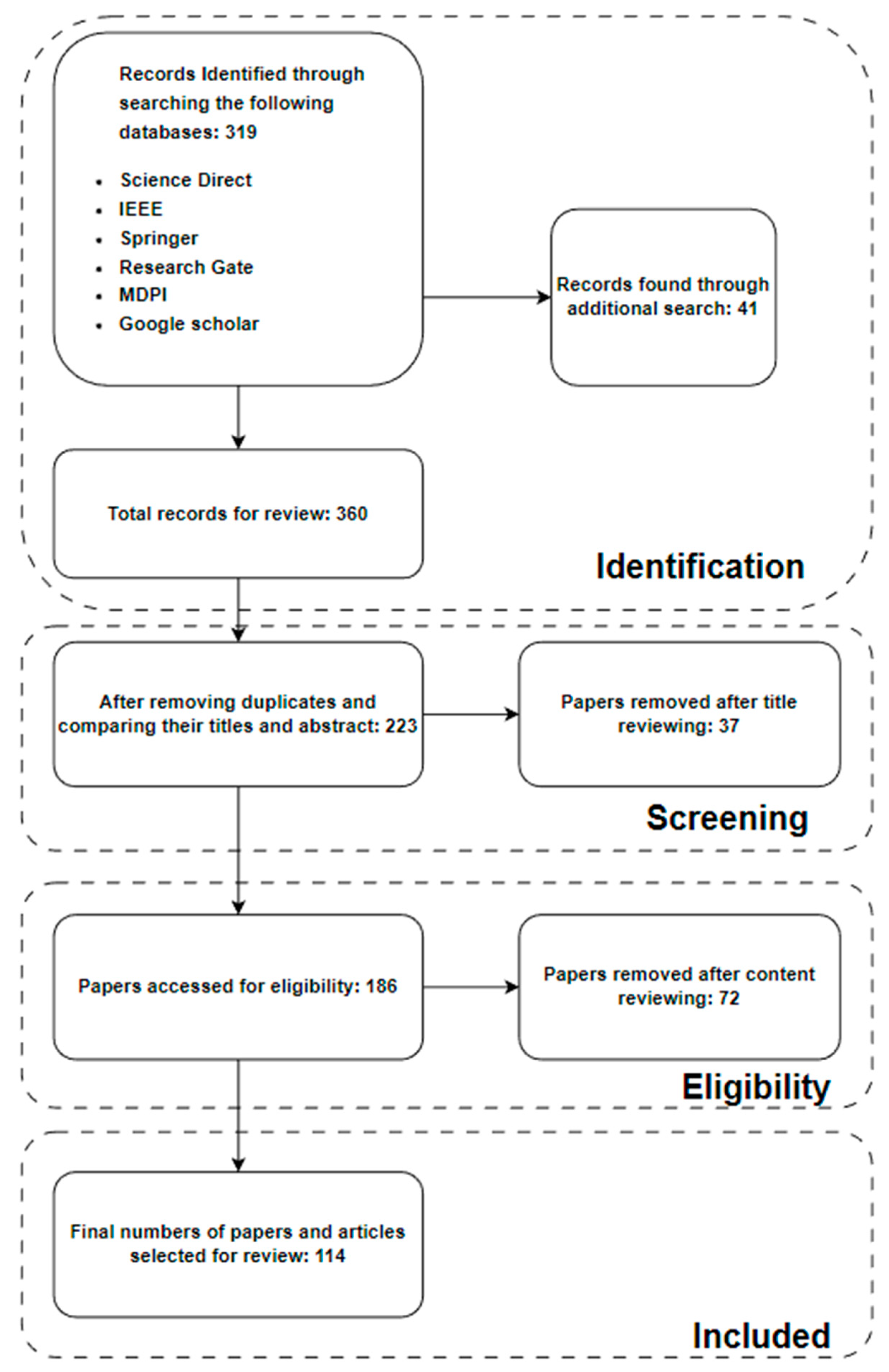
1.2. Review Methodology
1.3. Search Strategy and Literature Sources
1.3.1. Inclusion Criteria
- The significance of the articles determined their inclusion. The papers were chosen for this review depending on how novel they were;
- Research comparing different ML, AI, and deep learning models for cancer diagnosis;
- Relatively new articles were preferred;
- English-language studies that were published in full text and reported accuracy and other performance measures.
1.3.2. Elimination Criteria
- The articles were eliminated because they were irrelevant;
- Duplicate articles, non-English articles, or papers with sloppy writing;
- No use of deep learning, machine learning, or AI models.
1.3.3. Results
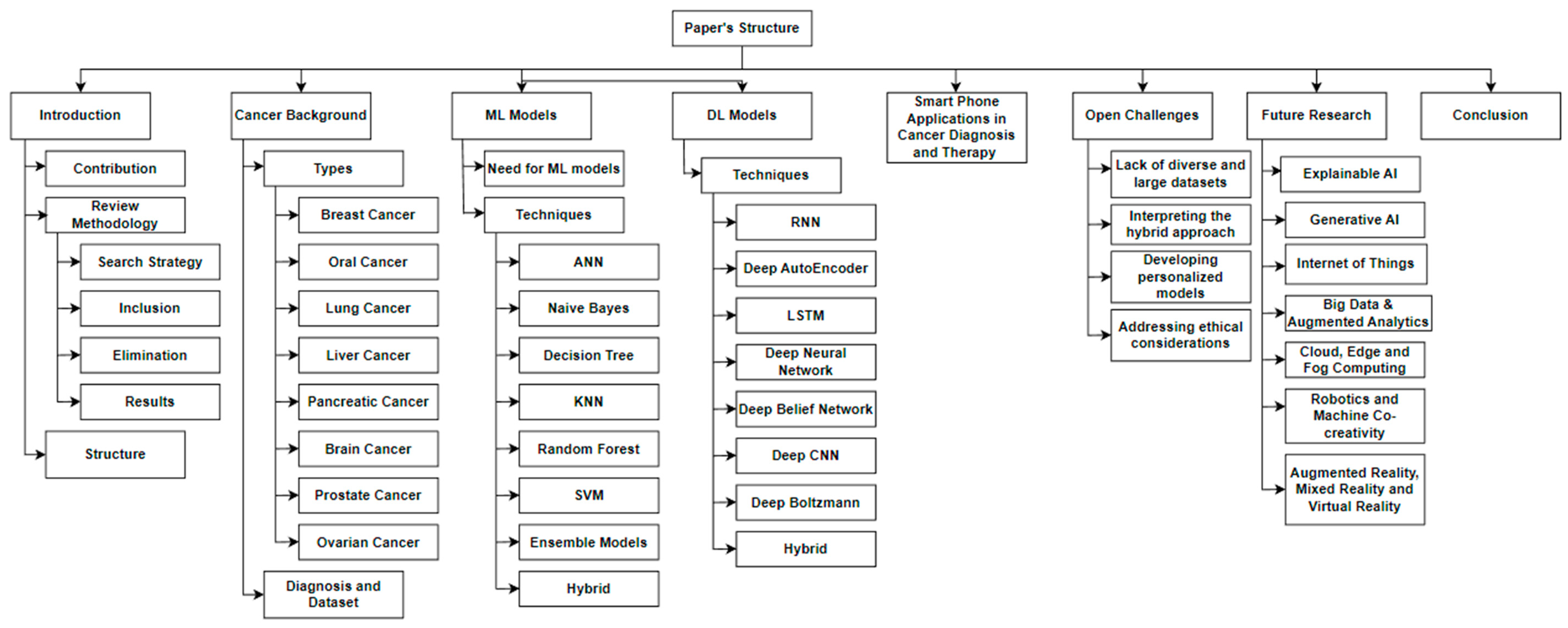
1.4. Structure of This Review
2. Cancer—Background
2.1. Cancer—Types
2.1.1. Breast Cancer
- Stage 0: The cancer is non-invasive and confines itself to the breast tissue’s milk ducts or lobules;
- Stage 1: refers to a cancer that is localized to the breast tissue, is tiny, and has not migrated to the lymph nodes or other regions of the body;
- Stage 2: The cancer has not yet moved outside of the breast tissue, but it may have moved to adjacent lymph nodes;
- Stage 3: Lymph nodes and more breast or chest-wall tissues have been affected by the malignancy;
- Stage 4: The cancer has spread to the bones, lungs, or liver, among other organs.
2.1.2. Oral Cancer
- Stage I: The cancer is minor, less than 2 cm in size, and limited to the site of genesis;
- Stage II: The cancer is more advanced than stage I and often measures 2–4 cm;
- Stage III: The cancer has grown to a size of 4 cm or has spread to adjacent lymph nodes;
- Stage IV: The cancer has progressed to the liver or lungs, among other organs.
2.1.3. Lung Cancer
- Stage 1: The cancer is only present in the lung and has not spread to other parts of the body or lymph nodes;
- Stage 2: The cancer has disseminated to nearby tissues or lymph nodes within the chest;
- Stage 3: The cancer has spread to organs in the chest or lymph nodes located in the middle of the chest;
- Stage 4: The cancer has metastasized to other organs, including but not limited to the liver or bones.
2.1.4. Liver Cancer
- Stage 1: The cancer is in its early stages and has not progressed beyond the liver;
- Stage 2: The cancer may be more advanced than stage 1 but is still limited to the liver;
- Stage 3: The cancer has metastasized to neighboring blood arteries or organs such as the pancreas or gallbladder;
- Stage 4: The disease has spread to the bones, lungs, or brain, among other organs.
2.1.5. Pancreatic Cancer
- Stage 1: The pancreas is the only location where the cancer has spread;
- Stage 2: The pancreas is still intact, but the cancer has migrated to neighboring lymph nodes;
- Stage 3: The liver, spleen, stomach, or other surrounding blood vessels or organs have been affected by the malignancy;
- Stage 4: The cancer has metastasized to additional tissues or organs, such as the lungs or bones.
2.1.6. Brain Cancer
- Grade 1: The slow-growing cancer cells resemble healthy ones in appearance;
- Grade 2: The cancer cells have a less-normal appearance and develop more quickly;
- Grade 3: Cancer cells develop quickly and have a markedly different appearance compared to healthy ones;
- Grade 4: The cancer cells show a high level of abnormality, are quickly growing, and spread.
2.1.7. Prostate Cancer
- Stage I: The cancer is tiny and slow growing, localized to the prostate gland;
- Stage II: The cancer has moved beyond the prostate gland but not to other bodily organs;
- Stage III: The seminal vesicles or other surrounding tissues or organs have been affected by the malignancy;
- Stage IV: The cancer has spread to other organs, including the lungs, liver, and bones.
2.1.8. Ovarian Cancer
- Stage 1: One or both ovaries are the only sites of the malignancy;
- Stage 2: The cancer has metastasized to surrounding tissues such as the uterus or fallopian tubes;
- Stage 3: The cancer has spread to the abdominal lining, surrounding lymph nodes, or further pelvic organs;
- Stage 4: Distant organs such as the liver or lungs have been affected by the malignancy.
2.2. Cancer Diagnosis—Datasets
3. Models for Deep Learning and Machine Learning in Cancer Diagnosis
3.1. Requirement for Deep Learning and Machine Learning Models for Diagnosis of Cancer
3.2. Machine Learning Techniques
- Supervised learning: This entails building a model using labelled data, where each input is paired with the appropriate output. For example, a model might be trained on a dataset of medical images that have been labelled as either normal or cancerous. The model can then be used to predict the likelihood of cancer for new images.
- Unsupervised learning: This entails feeding a model unlabeled data and allowing it to determine linkages and patterns on its own. This can be useful for identifying unusual or unexpected patterns in medical data that may indicate the presence of cancer.
- Reinforcement learning: This entails teaching a model to make decisions in a setting by rewarding or punishing specific actions. This can be used to optimize treatment plans for cancer patients based on their individual characteristics and needs.
- Transfer learning: Instead of building a model from scratch, this method uses a model that has already been trained as the foundation for a new job. The pre-trained model can serve as a helpful basis for activities when there is a limited quantity of training data available.
3.2.1. Artificial Neural Network
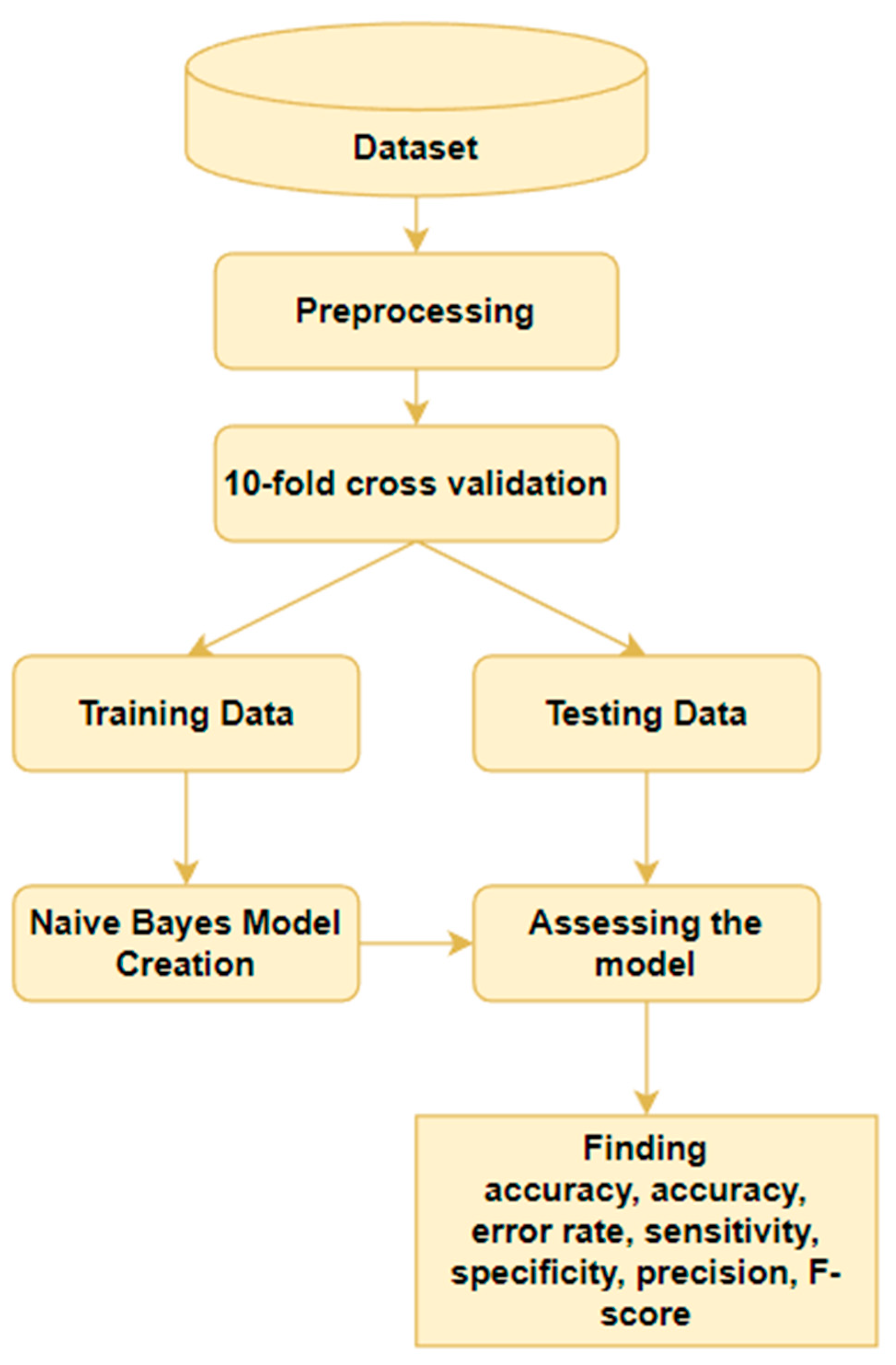
3.2.2. Naïve Bayes
3.2.3. Decision Tree
3.2.4. K-Nearest Neighbor
3.2.5. Random Forest
3.2.6. Support Vector Machine
3.2.7. Ensemble Models
3.2.8. Logistic Regression (LR)
3.2.9. Hybrid Models
3.3. Deep Learning Models
3.3.1. Recurrent Neural Networks
3.3.2. Deep Autoencoder
3.3.3. Long Short-Term Memory
3.3.4. Deep Neural Network
3.3.5. Deep Belief Network
3.3.6. Deep Convolutional Neural Network
3.3.7. Deep Boltzmann Machine
3.3.8. Hybrid Models
4. Smart Phone Applications in Cancer Diagnosis and Therapy
5. Open Challenges—Computational-Intelligence-Based Cancer Diagnosis
5.1. Lack of Diverse and Large Datasets
5.2. Interpreting the Hybrid Approach
5.3. Developing Personalized Models
5.4. Addressing Ethical Considerations
5.5. Clinical Challenges
6. Future Research Directions
6.1. Explainable AI
- Developing more interpretable models: One goal of explainable AI is to create models that are more transparent and interpretable so that the decision-making process can be better understood by humans. In the field of cancer diagnosis, this could involve developing models that are more easily explainable, such as decision tree-based models or linear models;
- Improving transparency and accountability: Another goal of explainable AI is to improve the transparency and accountability of AI systems. In the context of cancer diagnosis, this could involve developing methods for explaining the predictions made by AI systems in a way that is understandable to both doctors and patients;
- Integrating human expert knowledge: Another direction for future research could involve integrating human expert knowledge into explainable AI systems. For example, this could involve developing models that can incorporate expert knowledge about cancer diagnosis into their decision-making processes in order to improve the accuracy and reliability of the predictions;
- Improving the efficiency of explainable AI: Finally, there is also a need to improve the efficiency of explainable AI systems, so that they can be used in practical applications. This could involve developing methods for reducing the computational cost of explainable AI models or developing methods for scaling these models to larger datasets [100].
6.2. Generative AI
- Improving the accuracy of generative models: One goal of generative AI is to create models that can accurately generate realistic data, such as images or text. In the field of cancer diagnosis, this could involve developing generative models that are able to generate high-quality medical images or other types of patient data that are useful for diagnosis [101];
- Developing more efficient generative models: Another direction for future research could involve developing more efficient generative models, which can generate data more quickly or with fewer computational resources. This could be particularly important in the context of cancer diagnosis, wherein time is often of the essence and there is a need to process large amounts of data quickly;
- Integrating generative models with other AI approaches: Another potential direction for future research could involve integrating generative models with other types of AI algorithms, such as discriminative models or reinforcement-learning algorithms. This could allow for the development of more powerful and flexible AI systems for cancer diagnosis;
- Applying generative models to new types of data: Finally, there may also be opportunities to apply generative models to new types of data that have not been used extensively in the past for cancer diagnosis [102]. For example, this could include data from wearable sensors, social media, or other sources that have not been widely used in the past.
6.3. Internet of Everything
- Improving data security and privacy: One of the main challenges in using the IoE for cancer diagnosis is ensuring the security and privacy of patient data. This could involve developing methods for encrypting and protecting data as they are transmitted over the internet as well as developing protocols for controlling access to sensitive data;
- Developing new sensors and devices: Another direction for future research could involve developing new types of sensors and devices that can be used to collect data for cancer diagnosis. This could include wearable sensors, such as smart watches or fitness trackers, as well as more traditional medical devices, such as imaging machines or laboratory equipment;
- Integrating data from multiple sources: Another potential direction for future research could involve developing methods for integrating data from multiple sources, including both traditional medical sources and non-medical sources, such as social media or wearable devices. This could allow for a more comprehensive and accurate view of a patient’s health status;
- Improving the interoperability of devices: Finally, there is also a need to improve the interoperability of devices and systems within the IoE so that they can communicate and exchange data more easily. This could involve developing standards and protocols for data exchange, as well as developing methods for enabling devices from different manufacturers to work together seamlessly [103].
6.4. Big Data and Augmented Analytics
- Improving data quality and accuracy: One challenge in using big data for cancer diagnosis is ensuring the quality and accuracy of the data. This could involve developing methods for cleaning and pre-processing data, as well as developing methods for verifying the accuracy of the data;
- Developing personalized treatment plans: One potential application of big data and augmented analytics in cancer diagnosis could be the development of personalized treatment plans based on a patient’s unique characteristics and risk factors. This could involve analyzing large amounts of data to identify patterns and trends that are specific to individual patients and using this information to tailor treatment recommendations;
- Improving the accuracy of prognoses: Another potential use of big data and augmented analytics could be to improve the accuracy of prognoses for cancer patients. This could involve analyzing large amounts of data to identify factors that are associated with better or worse outcomes and using this information to make more accurate predictions about a patient’s likely course of treatment and outcome;
- Identifying new treatment options: Big data and augmented analytics could also be used to identify new treatment options for cancer patients. For example, by analyzing large amounts of data from clinical trials and other sources, it may be possible to identify promising new treatments that have not yet been widely adopted;
- Developing new drug compounds: Finally, big data and augmented analytics could be used to develop new drug compounds for the treatment of cancer. This could involve analyzing large amounts of data on the molecular mechanisms of cancer, as well as data on the effects of different drug compounds, to identify potential candidates for further development [104].
6.5. Cloud, Edge, and Fog Computing
- Improving data security and privacy: One challenge in using cloud, edge, and fog computing for cancer diagnosis is ensuring the security and privacy of patient data. This could involve developing methods for encrypting and protecting data as they are transmitted between different devices and servers as well as developing protocols for controlling access to sensitive data;
- Improving data interoperability: One potential direction for future research could involve developing methods for improving the interoperability of data between different devices and servers in cloud, edge, and fog computing environments. This could involve developing standards and protocols for data exchange as well as developing methods for enabling devices from different manufacturers to work together seamlessly;
- Enabling real-time data analysis: Another potential application of cloud, edge, and fog computing in cancer diagnosis could include enabling real-time data analysis. This could involve using these technologies to process and analyze data as they are being collected in order to make more timely and accurate diagnoses;
- Developing new types of distributed systems: Another direction for future research could involve the development of new types of distributed systems that are specifically designed for use in healthcare applications such as cancer diagnosis. This could include the development of new types of cloud, edge, and fog computing architectures as well as new types of software and hardware tools for these systems;
- Enhancing the scalability of distributed systems: Finally, there may also be opportunities to enhance the scalability of distributed systems in cloud, edge, and fog computing environments. This could involve developing methods for scaling these systems to larger datasets or more complex workloads in order to support the increasing demands of healthcare applications [105].
6.6. Robots and Machine Co-Creativity
- Developing new co-creativity algorithms: Another potential direction for future research could involve the development of new algorithms and software tools that enable robots and humans to work together more effectively in the context of cancer diagnosis and other healthcare applications. This could involve the development of machine learning algorithms or other types of artificial intelligence (AI) tools that are specifically designed for co-creative tasks;
- Enhancing the safety and reliability of robots: There is also a need to focus on the safety and reliability of robots in healthcare applications in order to ensure that they can be used safely and effectively. This could involve developing methods for testing and verifying the performance of robots as well as developing methods for mitigating potential risks and hazards;
- Enhancing the flexibility and adaptability of robots: Another potential direction for research could involve developing methods for improving the flexibility and adaptability of robots in healthcare applications. This could involve the development of new algorithms and software tools that enable robots to adapt to changing environments or tasks as well as new types of sensors and actuators that allow for greater flexibility and adaptability;
- Developing new ways to incorporate human expertise: Another potential direction for future research could involve developing new ways to incorporate human expertise in the decision-making process of robots in healthcare applications. This could involve the development of new machine learning algorithms or other types of AI tools that are able to learn from human experts or the development of new types of user interfaces that enable humans to collaborate more effectively with robots;
- Enhancing the reliability and maintainability of robots: Finally, there is also a need to focus on the reliability and maintainability of robots in healthcare applications. This could involve developing methods for testing and verifying the performance of robots as well as developing methods for maintaining and repairing these systems when necessary.
6.7. Augmented Reality (AR), Mixed Reality (MR), and Virtual Reality (VR)
- Enhancing the capabilities of existing AR, MR, and VR systems: Another potential direction for research could involve enhancing the capabilities of existing AR, MR, and VR systems by improving their accuracy, resolution, or field of view. This could involve the development of new software and hardware tools as well as new types of sensors and displays;
- Developing new interaction techniques: One potential direction for future research could involve developing new interaction techniques that enable users to more effectively interact with AR, MR, and VR systems in healthcare applications. This could involve the development of new types of gesture recognition or voice control algorithms as well as new types of haptic interfaces;
- Enhancing the realism of virtual environments: Another potential direction for research could involve developing methods for enhancing the realism of virtual environments in AR, MR, and VR systems. This could involve the development of new graphics and rendering algorithms as well as new types of sensors and displays that enable more realistic representations of physical objects and environments;
- Enhancing the usability and user experience of AR, MR, and VR systems: Finally, there is also a need to focus on the usability and user experience of AR, MR, and VR systems in healthcare applications. This could involve developing methods for improving the ease of use and comfort of these systems, as well as developing methods for enhancing the realism and immersion of virtual environments.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acronym | Definition |
| AI | Artificial Intelligence |
| ANN | Artificial Neural Network |
| BP | Back-Propagation |
| CNN | convolutional neural network |
| SVM | Support Vector Machine |
| RNN | recurrent neural network |
| LR | Logistic Regression |
| LSTM | Long short-term memory |
References
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-65. [Google Scholar] [CrossRef] [PubMed]
- Carbonara, R.; Bonomo, P.; Di Rito, A.; Didonna, V.; Gregucci, F.; Ciliberti, M.P.; Surgo, A.; Bonaparte, I.; Fiorentino, A.; Sardaro, A. Investigation of Radiation-Induced Toxicity in Head and Neck Cancer Patients through Radiomics and Machine Learning: A Systematic Review. J. Oncol. 2021, 2021, 5566508. [Google Scholar] [CrossRef] [PubMed]
- Priyanka, K.S. A review paper on breast cancer detection using deep learning. In IOP Conference Series: Materials Science and Engineering; IOP Publishing: Bristol, UK, 2021; Volume 1022, p. 012071. [Google Scholar]
- Dildar, M.; Akram, S.; Irfan, M.; Khan, H.U.; Ramzan, M.; Mahmood, A.R.; Alsaiari, S.A.; Saeed, A.H.M.; Alraddadi, M.O.; Mahnashi, M.H. Skin cancer detection: A review using deep learning techniques. Int. J. Environ. Res. Public Health 2021, 18, 5479. [Google Scholar] [CrossRef]
- Luo, W. Predicting Cervical Cancer Outcomes: Statistics, Images, and Machine Learning. Front. Artif. Intell. 2021, 4, 627369. [Google Scholar] [CrossRef] [PubMed]
- Amin, J.; Sharif, M.; Haldorai, A.; Yasmin, M.; Nayak, R.S. Brain tumor detection and classification using machine learning: A comprehensive survey. Complex Intell. Syst. 2021, 8, 3161–3183. [Google Scholar] [CrossRef]
- Iqbal, M.J.; Javed, Z.; Sadia, H.; Qureshi, I.A.; Irshad, A.; Ahmed, R.; Malik, K.; Raza, S.; Abbas, A.; Pezzani, R.; et al. Clinical applications of artificial intelligence and machine learning in cancer diagnosis: Looking into the future. Cancer Cell Int. 2021, 21, 270. [Google Scholar] [CrossRef]
- Saba, T. Recent advancement in cancer detection using machine learning: Systematic survey of decades, comparisons and challenges. J. Infect. Public Health 2020, 13, 1274–1289. [Google Scholar] [CrossRef]
- Ralbovsky, N.M.; Lednev, I.K. Towards development of a novel universal medical diagnostic method: Raman spectroscopy and machine learning. Chem. Soc. Rev. 2020, 49, 7428–7453. [Google Scholar] [CrossRef]
- Abbasi, A.A.; Hussain, L.; Awan, I.A.; Abbasi, I.; Majid, A.; Nadeem, M.S.A.; Chaudhary, Q.-A. Detecting prostate cancer using deep learning convolution neural network with transfer learning approach. Cogn. Neurodyn. 2020, 14, 523–533. [Google Scholar] [CrossRef]
- Tandel, G.S.; Biswas, M.; Kakde, O.G.; Tiwari, A.; Suri, H.S.; Turk, M.; Laird, J.R.; Asare, C.K.; Ankrah, A.A.; Khanna, N.N.; et al. A Review on a Deep Learning Perspective in Brain Cancer Classification. Cancers 2019, 11, 111. [Google Scholar] [CrossRef]
- Bakator, M.; Radosav, D. Deep learning and medical diagnosis: A review of literature. Multimodal Technol. Interact. 2018, 2, 47. [Google Scholar] [CrossRef]
- Senders, J.T.; Zaki, M.M.; Karhade, A.V.; Chang, B.; Gormley, W.B.; Broekman, M.L.; Smith, T.R.; Arnaout, O. An introduction and overview of machine learning in neurosurgical care. Acta Neurochir. 2017, 160, 29–38. [Google Scholar] [CrossRef] [PubMed]
- TCIA Dataset. Common Disease or Image Modality or Type. Available online: https://www.cancerimagingarchive.net/collections/ (accessed on 14 February 2023).
- NLST. Available online: https://cdas.cancer.gov/ (accessed on 14 April 2023).
- LUNA16. Lung Cancer Dataset. 2021. Available online: https://www.kaggle.com/datasets/fanbyprinciple/luna-lung-cancer-dataset (accessed on 14 February 2023).
- BRATS Dataset. 2015. Available online: https://www.smir.ch/BRATS/Start2015 (accessed on 14 February 2023).
- BRATS Dataset. 2016. Available online: https://www.smir.ch/BRATS/Start2016 (accessed on 14 February 2023).
- BRATS Dataset. 2017. Available online: https://www.kaggle.com/datasets/xxc025/unet-datasets (accessed on 14 February 2023).
- BRATS Dataset. 2018. Available online: https://www.kaggle.com/datasets/sanglequang/brats2018 (accessed on 14 February 2023).
- Lung Image Database Consortium and Image Database Resource Initiative(LIDC-IDRI). 2023. Available online: https://wiki.cancerimagingarchive.net/pages/viewpage.action?pageId=1966254 (accessed on 14 February 2023).
- Breast Cancer Wisconsin (Diagnostic) Data Set. 2015. Available online: https://www.kaggle.com/datasets/uciml/breast-cancer-wisconsin-data (accessed on 14 February 2023).
- MIAS Mammography. Breast Cancer. 2018. Available online: https://www.kaggle.com/datasets/kmader/mias-mammography (accessed on 14 February 2023).
- Sadeeq, H.T.; Ameen, S.Y.; Abdulazeez, A.M. Cancer Diagnosis based on Artificial Intelligence, Machine Learning, and Deep Learning. In Proceedings of the 2022 International Conference on Innovation and Intelligence for Informatics, Computing, and Technologies (3ICT), Virtual, 20–21 November 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 656–661. [Google Scholar]
- Simin, A.T.; Baygi, S.M.G.; Noori, A. Cancer Diagnosis Based on Combination of Artificial Neural Networks and Reinforcement Learning. In Proceedings of the 2020 6th Iranian Conference on Signal Processing and Intelligent Systems (ICSPIS), Mashhad, Iran, 23–24 December 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 1–4. [Google Scholar]
- Gong, S.; Gao, W.; Abza, F. Brain tumor diagnosis based on artificial neural network and a chaos whale optimization algorithm. Comput. Intell. 2020, 36, 259–275. [Google Scholar] [CrossRef]
- Navaneethakrishnan, R.; Alagumeenaakshi, M.; Ajay, V.P.; Shawkat, T.B.; Priya, S.B. Breast Cancer Diagnosis through Soft Computing Approaches: A Survey. In Proceedings of the 2021 International Conference on Advancements in Electrical, Electronics, Communication, Computing and Automation (ICAECA), Coimbatore, India, 8–9 October 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 1–4. [Google Scholar]
- Houssein, E.H.; Emam, M.M.; Ali, A.A.; Suganthan, P.N. Deep and machine learning techniques for medical imaging-based breast cancer: A comprehensive review. Expert Syst. Appl. 2021, 167, 114161. [Google Scholar] [CrossRef]
- Yue, W.; Wang, Z.; Chen, H.; Payne, A.; Liu, X. Machine Learning with Applications in Breast Cancer Diagnosis and Prognosis. Designs 2018, 2, 13. [Google Scholar] [CrossRef]
- Mathur, M.; Jindal, V.; Wadhwa, G. Detecting malignancy of ovarian tumour using convolutional neural network: A review. In Proceedings of the 2020 Sixth International Conference on Parallel, Distributed and Grid Computing (PDGC), Waknaghat, India, 6–8 November 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 351–356. [Google Scholar]
- Gupta, A.; Koul, A.; Kumar, Y. Pancreatic cancer detection using machine and deep learning techniques. In Proceedings of the 2022 2nd International Conference on Innovative Practices in Technology and Management (ICIPTM), Gautam Buddha Nagar, India, 23–25 February 2022; IEEE: Piscataway, NJ, USA, 2022; Volume 2, pp. 151–155. [Google Scholar]
- Raoof, S.S.; Jabbar, M.A.; Fathima, S.A. Lung Cancer prediction using machine learning: A comprehensive approach. In Proceedings of the 2020 2nd International conference on innovative mechanisms for industry applications (ICIMIA), Bangalore, India, 5–7 March 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 108–115. [Google Scholar]
- Datasets Used for Classification Comparison of Results. Available online: https://www.is.umk.pl/~duch/projects/projects/datasets.html#Hepatitis (accessed on 3 March 2023).
- Deepa, B.G.; Senthil, S. Constructive Effect of Ranking Optimal Features Using Random Forest, SupportVector Machine and Naïve Bayes forBreast Cancer Diagnosis. In Big Data Analytics and Intelligence: A Perspective for Health Care; Emerald Publishing Limited: Bradford, UK, 2020; pp. 189–202. [Google Scholar]
- Gupta, G.; Sharma, M.; Choudhary, S.; Pandey, K. Performance Analysis of Machine Learning Classification Algorithms for Breast Cancer Diagnosis. In Proceedings of the 2021 9th International Conference on Reliability, Infocom Technologies and Optimization (Trends and Future Directions) (ICRITO), Noida, India, 3–4 September 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 1–6. [Google Scholar]
- Silva, F.; Pereira, T.; Neves, I.; Morgado, J.; Freitas, C.; Malafaia, M.; Sousa, J.; Fonseca, J.; Negrão, E.; de Lima, B.F.; et al. Towards machine learning-aided lung cancer clinical routines: Approaches and open challenges. J. Pers. Med. 2022, 12, 480. [Google Scholar] [CrossRef]
- Fatima, N.; Liu, L.; Hong, S.; Ahmed, H. Prediction of Breast Cancer, Comparative Review of Machine Learning Techniques, and Their Analysis. IEEE Access 2020, 8, 150360–150376. [Google Scholar] [CrossRef]
- Zhao, R.; Wen, X.; Pang, H.; Ma, Z. Liver disease prediction using W-LR-XGB Algorithm. In Proceedings of the 2021 International Conference on Computer, Blockchain and Financial Development (CBFD), Nanjing, China, 23–25 April 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 245–248. [Google Scholar]
- Tabrizchi, H.; Tabrizchi, M. Breast cancer diagnosis using a multi-verse optimizer-based gradient boosting decision tree. SN Appl. Sci. 2020, 2, 752. [Google Scholar] [CrossRef]
- Ghiasi, M.M.; Zendehboudi, S. Application of decision tree-based ensemble learning in the classification of breast cancer. Comput. Biol. Med. 2021, 128, 104089. [Google Scholar] [CrossRef]
- Aditya, M.; Amrita, I.; Kodipalli, A.; Martis, R.J. Ovarian cancer detection and classification using machine leaning. In Proceedings of the 2021 5th International Conference on Electrical, Electronics, Communication, Computer Technologies and Optimization Techniques (ICEECCOT), Mysuru, India, 10–11 December 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 279–282. [Google Scholar]
- Bhattacharjee, S.; Singh, Y.J.; Ray, D. Comparative performance analysis of machine learning classifiers on ovarian cancer dataset. In Proceedings of the 2017 Third International Conference on Research in Computational Intelligence and Communication Networks (ICRCICN), Kolkata, India, 3–5 November 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 213–218. [Google Scholar]
- Lavanya, L.; Chandra, J. Oral cancer analysis using machine learning techniques. Int. J. Eng. Res. Technol. 2019, 12, 596–601. [Google Scholar]
- Arora, M.; Som, S.; Rana, A. Predictive Analysis of Machine Learning Algorithms for Breast Cancer Diagnosis. In Proceedings of the 2020 8th International Conference on Reliability, Infocom Technologies and Optimization (Trends and Future Directions) (ICRITO), Noida, India, 4–5 June 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 835–839. [Google Scholar]
- MurtiRawat, R.; Panchal, S.; Singh, V.K.; Panchal, Y. Breast Cancer detection using K-nearest neighbors, logistic regression and ensemble learning. In Proceedings of the 2020 International Conference on Electronics and Sustainable Communication Systems (ICESC), Coimbatore, India, 2–4 July 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 534–540. [Google Scholar]
- Yeganeh, P.N.; Mostafavi, M.T. Use of machine learning for diagnosis of cancer in ovarian tissues with a selected mRNA panel. In Proceedings of the 2018 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Madrid, Spain, 3–6 December 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 2429–2434. [Google Scholar]
- Alam, M.; Tahernezhadi, M.; Vege, H.K.; Rajesh, P. A machine learning classification technique for predicting prostate cancer. In Proceedings of the 2020 IEEE International Conference on Electro Information Technology (EIT), Chicago, IL, USA, 31 July–1 August 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 228–232. [Google Scholar]
- Begum, A.; Kumar, V.D.; Asghar, J.; Hemalatha, D.; Arulkumaran, G. A Combined Deep CNN: LSTM with a Random Forest Approach for Breast Cancer Diagnosis. Complexity 2022, 2022, 9299621. [Google Scholar] [CrossRef]
- Akter, L.; Akhter, N. Ovarian Cancer Classification from Pathophysiological Complications using Machine Learning Techniques. In Proceedings of the 2021 12th International Conference on Computing Communication and Networking Technologies (ICCCNT), Kharagpur, India, 6–8 July 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 1–6. [Google Scholar]
- Tounsi, S.; Kallel, I.F.; Kallel, M. Breast cancer diagnosis using feature selection techniques. In Proceedings of the 2022 2nd International Conference on Innovative Research in Applied Science, Engineering and Technology (IRASET), Meknes, Morocco, 3–4 March 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 1–5. [Google Scholar]
- Zemmal, N.; Azizi, N.; Dey, N.; Sellami, M. Adaptive Semi Supervised Support Vector Machine Semi Supervised Learning with Features Cooperation for Breast Cancer Classification. J. Med. Imaging Health Inform. 2016, 6, 53–62. [Google Scholar] [CrossRef]
- Nam, Y.-J.; Shin, W.-J. A Study on Comparison of Lung Cancer Prediction Using Ensemble Machine Learning. Korean Artif. Intell. 2019, 7, 19–24. [Google Scholar] [CrossRef]
- Al-Rawi, N.; Sultan, A.; Rajai, B.; Shuaeeb, H.; Alnajjar, M.; Alketbi, M.; Mohammad, Y.; Shetty, S.R.; Mashrah, M.A. The Effectiveness of Artificial Intelligence in Detection of Oral Cancer. Int. Dent. J. 2022, 72, 436–447. [Google Scholar] [CrossRef]
- Turki, T. An empirical study of machine learning algorithms for cancer identification. In Proceedings of the 2018 IEEE 15th International Conference on Networking, Sensing and Control (ICNSC), Zhuhai, China, 27–29 March 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1–5. [Google Scholar]
- Meng, L.; Wen, C.; Li, G. Support vector machine based liver cancer early detection using magnetic resonance images. In Proceedings of the 2014 13th International Conference on Control Automation Robotics & Vision (ICARCV), Singapore, 10–12 December 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 861–864. [Google Scholar]
- Pradhan, K.S.; Chawla, P.; Tiwari, R. HRDEL: High ranking deep ensemble learning-based lung cancer diagnosis model. Expert Syst. Appl. 2023, 213, 118956. [Google Scholar] [CrossRef]
- Gupta, S.; Gupta, M.K.; Kumar, R. A Novel Multi-Neural Ensemble Approach for Cancer Diagnosis. Appl. Artif. Intell. 2021, 36, 2018182. [Google Scholar] [CrossRef]
- Filias, F.; Mylona, E.; Blekos, K.; Supiot, S.; de Crevoisier, R.; Acosta, O. Ensemble Learning for Prediction of Toxicity in Prostate Cancer Radiotherapy: Comparison between Stacking and Genetic Algorithm Weighted Voting. In Proceedings of the 2020 IEEE 20th International Conference on Bioinformatics and Bioengineering (BIBE), Cincinnati, OH, USA, 26–28 October 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 884–889. [Google Scholar]
- Song, X.; Liang, K.; Li, J. WGRLR: A Weighted Group Regularized Logistic Regression for Cancer Diagnosis and Gene Selection. IEEE/ACM Trans. Comput. Biol. Bioinform. 2022, 20, 1563–1573. [Google Scholar] [CrossRef]
- Burçak, K.C.; Uğuz, H. A New Hybrid Breast Cancer Diagnosis Model Using Deep Learning Model and ReliefF. Trait. Signal 2022, 39, 521–529. [Google Scholar] [CrossRef]
- Lakshmi, V.V.; Jasmine, J.S.L. A Hybrid Artificial Intelligence Model for Skin Cancer Diagnosis. Comput. Syst. Sci. Eng. 2021, 37, 233–245. [Google Scholar] [CrossRef]
- Polat, K.; Güneş, S. Breast cancer diagnosis using least square support vector machine. Digit. Signal Process. 2007, 17, 694–701. [Google Scholar] [CrossRef]
- Ravindran, U.; Gunavathi, C. A survey on gene expression data analysis using deep learning methods for cancer diagnosis. Prog. Biophys. Mol. Biol. 2023, 177, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Yong, B.; Lv, Q.; Shen, J.; Wang, X. Deep Autoencoder for Mass Spectrometry Feature Learning and Cancer Detection. IEEE Access 2020, 8, 45156–45166. [Google Scholar] [CrossRef]
- Gupta, S.; Kalaivani, S.; Rajasundaram, A.; Ameta, G.K.; Oleiwi, A.K.; Dugbakie, B.N. Prediction Performance of Deep Learning for Colon Cancer Survival Prediction on SEER Data. BioMed Res. Int. 2022, 2022, 1467070. [Google Scholar] [CrossRef] [PubMed]
- Munir, K.; Elahi, H.; Ayub, A.; Frezza, F.; Rizzi, A. Cancer Diagnosis Using Deep Learning: A Bibliographic Review. Cancers 2019, 11, 1235. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, M.; Kalofonou, M.; Toumazou, C. A deep autoencoder system for differentiation of cancer types based on DNA methylation state. arXiv 2018, arXiv:1810.01243. [Google Scholar]
- Liu, T.; Huang, J.; Liao, T.; Pu, R.; Liu, S.; Peng, Y. A hybrid deep learning model for predicting molecular subtypes of human breast cancer using multimodal data. IRBM 2022, 43, 62–74. [Google Scholar] [CrossRef]
- Deshmukh, G.; Susladkar, O.; Makwana, D.; Radhapuram, S.C.T.; Singaram, N.K.; Mittal, S. FEEDNet: A feature enhanced encoder-decoder LSTM network for nuclei instance segmentation for histopathological diagnosis. Phys. Med. Biol. 2022, 67, 195011. [Google Scholar] [CrossRef]
- Gong, B.; Shen, L.; Chang, C.; Zhou, S.; Zhou, W.; Li, S.; Shi, J. Bi-modal ultrasound breast cancer diagnosis via multi-view deep neural network SVM. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 1106–1110. [Google Scholar]
- Wu, X.; Wang, H.-Y.; Shi, P.; Sun, R.; Wang, X.; Luo, Z.; Zeng, F.; Lebowitz, M.S.; Lin, W.-Y.; Lu, J.-J.; et al. Long short-term memory model—A deep learning approach for medical data with irregularity in cancer predication with tumor markers. Comput. Biol. Med. 2022, 144, 105362. [Google Scholar] [CrossRef]
- Lim, B.; Lee, K.S.; Lee, Y.H.; Kim, S.; Min, C.; Park, J.-Y.; Lee, H.S.; Cho, J.S.; Kim, S.I.; Chung, B.H.; et al. External Validation of the Long Short-Term Memory Artificial Neural Network-Based SCaP Survival Calculator for Prediction of Prostate Cancer Survival. Cancer Res. Treat. 2021, 53, 558–566. [Google Scholar] [CrossRef]
- Wang, H.; Xing, L. Deep Learning’s Application on Radiology and Pathological Image of Lung Cancer: A Review. In Proceedings of the 2021 International Conference on Information Technology and Biomedical Engineering (ICITBE), Nanchang, China, 24–26 December 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 299–303. [Google Scholar]
- Rajalaxmi, R.R.; Kavithra, S.; Gothai, E.; Natesan, P.; Thamilselvan, R. A Systematic Review of Lung Cancer Prediction Using Machine Learning Algorithm. In Proceedings of the 2022 International Conference on Computer Communication and Informatics (ICCCI), Coimbatore, India, 25–27 January 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 1–7. [Google Scholar]
- Al-Ma’aitah, M.; AlZubi, A.A. Enhanced Computational Model for Gravitational Search Optimized Echo State Neural Networks Based Oral Cancer Detection. J. Med. Syst. 2018, 42, 205. [Google Scholar] [CrossRef]
- Wen, H.; Li, S.; Li, W.; Li, J.; Yin, C. Comparision of four machine learning techniques for the prediction of prostate cancer survivability. In Proceedings of the 2018 15th International Computer Conference on Wavelet Active Media Technology and Information Processing (ICCWAMTIP), Chengdu, China, 14–16 December 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 112–116. [Google Scholar]
- Maurya, B.; Hiranwal, S.; Kumar, M. A review on liver cancer detection techniques. In Proceedings of the 2020 5th IEEE International Conference on Recent Advances and Innovations in Engineering (ICRAIE), Jaipur, India, 1–3 December 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 1–5. [Google Scholar]
- Manickavasagam, S.; Sugumaran, P. Optimal Deep Belief Network Based Lung Cancer Detection and Survival Rate Prediction. Comput. Syst. Sci. Eng. 2023, 45, 939–953. [Google Scholar] [CrossRef]
- Novitasari, D.C.R.; Foeady, A.Z.; Thohir, M.; Arifin, A.Z.; Niam, K.; Asyhar, A.H. Automatic approach for cervical cancer detection based on deep belief network (DBN) using colposcopy data. In Proceedings of the 2020 International Conference on Artificial Intelligence in Information and Communication (ICAIIC), Fukuoka, Japan, 19–21 February 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 415–420. [Google Scholar]
- Painuli, D.; Bhardwaj, S. Recent advancement in cancer diagnosis using machine learning and deep learning techniques: A comprehensive review. Comput. Biol. Med. 2022, 146, 105580. [Google Scholar] [CrossRef] [PubMed]
- Xia, M.; Zhang, G.; Mu, C.; Guan, B.; Wang, M. Cervical cancer cell detection based on deep convolutional neural network. In Proceedings of the 2020 39th Chinese Control Conference (CCC), Shenyang, China, 27–29 July 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 6527–6532. [Google Scholar]
- Haq, A.U.; Li, J.P.; Saboor, A.; Khan, J.; Zhou, W.; Jiang, T.; Raji, M.F.; Wali, S. 3DCNN: Three-layers deep convolutional neural network architecture for breast cancer detection using clinical image data. In Proceedings of the 2020 17th International Computer Conference on Wavelet Active Media Technology and Information Processing (ICCWAMTIP), Chengdu, China, 18–20 December 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 83–88. [Google Scholar]
- Al Rahhal, M.M. Breast cancer classification in histopathological images using convolutional neural network. Int. J. Adv. Comput. Sci. Appl. 2018, 9, 64–68. [Google Scholar]
- Selma, M.; Mohamed, A.; Yassine, H.M.; Issam, B. How to have a structured database for lung cancer segmentation using deep learning technologies. In Proceedings of the 2021 International Conference on Networking and Advanced Systems (ICNAS), Annaba, Algeria, 27–28 October 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 1–5. [Google Scholar]
- Kadir, T.; Gleeson, F. Lung cancer prediction using machine learning and advanced imaging techniques. Transl. Lung Cancer Res. 2018, 7, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Alabi, R.O.; Almangush, A.; Elmusrati, M.; Mäkitie, A.A. Deep machine learning for oral cancer: From precise diagnosis to precision medicine. Front. Oral Health 2022, 2, 97. [Google Scholar] [CrossRef]
- Dharani, R.; Revathy, S. DEEPORCD: Detection of Oral Cancer using Deep Learning. J. Phys. Conf. Ser. 2021, 1911, 012006. [Google Scholar] [CrossRef]
- Arvidsson, I.; Overgaard, N.C.; Marginean, F.E.; Krzyzanowska, A.; Bjartell, A.; Åström, K.; Heyden, A. Generalization of prostate cancer classification for multiple sites using deep learning. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 191–194. [Google Scholar]
- Wu, M.; Yan, C.; Liu, H.; Liu, Q. Automatic classification of ovarian cancer types from cytological images using deep convolutional neural networks. Biosci. Rep. 2018, 38, BSR20180289. [Google Scholar] [CrossRef]
- Sun, C.; Wang, L.; Wang, W.; Cheng, X.; Li, Z.; Zhang, J.; Yang, F.; Huang, J.; Zhu, Y. Non-Small Cell Lung Cancer Staging Using Deep Restricted Boltzmann Machine. In Proceedings of the 2018 14th IEEE International Conference on Signal Processing (ICSP), Beijing, China, 12–16 August 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1175–1178. [Google Scholar]
- Li, Y.; Fauteux, F.; Zou, J.; Nantel, A.; Pan, Y. Personalized prediction of genes with tumor-causing somatic mutations based on multi-modal deep Boltzmann machine. Neurocomputing 2019, 324, 51–62. [Google Scholar] [CrossRef]
- Tomczak, J.M. Prediction of breast cancer recurrence using Classification Restricted Boltzmann Machine with Dropping. arXiv 2013, arXiv:1308.6324. [Google Scholar]
- Jeyaraj, P.R.; Nadar, E.R.S. Deep Boltzmann machine algorithm for accurate medical image analysis for classification of cancerous region. Cogn. Comput. Syst. 2019, 1, 85–90. [Google Scholar] [CrossRef]
- Al-Antari, M.A.; Al-Masni, M.A.; Kim, T.S. Deep learning computer-aided diagnosis for breast lesion in digital mammogram. Deep. Learn. Med. Image Anal. Chall. Appl. 2020, 1213, 59–72. [Google Scholar]
- Lahoura, V.; Singh, H.; Aggarwal, A.; Sharma, B.; Mohammed, M.A.; Damaševičius, R.; Cengiz, K. Cloud computing-based framework for breast cancer diagnosis using extreme learning machine. Diagnostics 2021, 11, 241. [Google Scholar] [CrossRef] [PubMed]
- Revett, K. Data Mining a Prostate Cancer Dataset Using Neural Networks. In Proceedings of the 2006 8th Seminar on Neural Network Applications in Electrical Engineering, Belgrade, Serbia, 25–27 February 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 157–160. [Google Scholar]
- Nahata, H.; Singh, S.P. Deep learning solutions for skin cancer detection and diagnosis. In Machine Learning with Health Care Perspective: Machine Learning and Healthcare; Springer: Cham, Switzerland, 2020; pp. 159–182. [Google Scholar]
- Sahu, B.; Mohanty, S.; Rout, S. A Hybrid Approach for Breast Cancer Classification and Diagnosis. EAI Endorsed Trans. Scalable Inf. Syst. 2018, 6, e2. [Google Scholar] [CrossRef]
- Zou, L.; Yu, S.; Meng, T.; Zhang, Z.; Liang, X.; Xie, Y. A Technical Review of Convolutional Neural Network-Based Mammographic Breast Cancer Diagnosis. Comput. Math. Methods Med. 2019, 2019, 6509357. [Google Scholar] [CrossRef]
- Xu, F.; Uszkoreit, H.; Du, Y.; Fan, W.; Zhao, D.; Zhu, J. Explainable AI: A brief survey on history, research areas, approaches and challenges. In Proceedings of the Natural Language Processing and Chinese Computing: 8th CCF International Conference, NLPCC 2019, Dunhuang, China, 9–14 October 2019; Springer International Publishing: Berlin/Heidelberg, Germany, 2019. Proceedings, Part II 8. pp. 563–574. [Google Scholar]
- Rabbani, M.; Kanevsky, J.; Kafi, K.; Chandelier, F.; Giles, F.J. Role of artificial intelligence in the care of patients with nonsmall cell lung cancer. Eur. J. Clin. Investig. 2018, 48, e12901. [Google Scholar] [CrossRef]
- Tanaka, I.; Furukawa, T.; Morise, M. The current issues and future perspective of artificial intelligence for developing new treatment strategy in non-small cell lung cancer: Harmonization of molecular cancer biology and artificial intelligence. Cancer Cell Int. 2021, 21, 454. [Google Scholar] [CrossRef]
- Miraz, M.H.; Ali, M.; Excell, P.S.; Picking, R. A review on Internet of Things (IoT), Internet of everything (IoE) and Internet of nano things (IoNT). In Proceedings of the 2015 Internet Technologies and Applications (ITA), Wrexham, UK, 8–11 September 2015; pp. 219–224. [Google Scholar]
- Andriole, S.J. Artificial intelligence, machine learning, and augmented analytics [life in C-suiteo]. IT Prof. 2019, 21, 56–59. [Google Scholar] [CrossRef]
- De Donno, M.; Tange, K.; Dragoni, N. Foundations and evolution of modern computing paradigms: Cloud, IoT, edge, and fog. IEEE Access 2019, 7, 150936–150948. [Google Scholar] [CrossRef]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.J.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef]
- Kaliyugarasan, S.K.; Lundervold, A.; Lundervold, A.S. Pulmonary Nodule Classification in Lung Cancer from 3D Thoracic CT Scans Using fastai and MONAI. Int. J. Interact. Multimed. Artif. Intell. 2021, 6, 83–89. [Google Scholar] [CrossRef]
- Khemchandani, M.A.; Jadhav, S.M.; Iyer, B. Brain Tumor Segmentation and Identification Using Particle Imperialist Deep Convolutional Neural Network in MRI Images. Int. J. Interact. Multimed. Artif. Intell. 2022, 7, 38–47. [Google Scholar] [CrossRef]
- Kumaar, M.A.; Samiayya, D.; Rajinikanth, V.; M, D.R.V.P.; Kadry, S. Brain Tumor Classification Using a Pre-Trained Auxiliary Classifying Style-Based Generative Adversarial Network. Int. J. Interact. Multimed. Artif. Intell. 2023, in press. [Google Scholar] [CrossRef]
- SkinVision. Available online: https://www.skinvision.com/ (accessed on 14 April 2023).
- Breast Check Now. Available online: https://play.google.com/store/apps/details?id=uk.org.breakthrough.ibreastcheck&hl=en&gl=US (accessed on 14 April 2023).
- Ada Health. Available online: https://ada.com/ (accessed on 14 April 2023).
- Cancer.Net. Available online: https://www.cancer.net/navigating-cancer-care/managing-your-care/cancernet-mobile (accessed on 14 April 2023).
- American Society of Clinical Oncology. Available online: https://old-prod.asco.org/practice-patients/guidelines (accessed on 14 April 2023).








| Reference | Year | One-Phrase Summary | Machine Learning | Deep Learning | Open Challenges | Future Directions |
|---|---|---|---|---|---|---|
| Our Review | - | This review explores the advantages and disadvantages of each model and provides an outline of how they are used in cancer diagnosis. It finishes with future work on the topic, outstanding questions, and potential for further study. | ✓ | ✓ | ✓ | ✓ |
| [2] | 2021 | This review highlights the use of a variety of imaging techniques and data analysis methods as it investigates the potential of radiomics and machine learning for investigating radiation-induced toxicity in head- and neck-cancer patients. According to the review, radiomics and machine learning have the potential to help improve our understanding of radiation-induced toxicity and assist in guiding treatment decisions in patients such as these. | ✓ | × | × | × |
| [3] | 2021 | The primary focus of this investigation is on visual data, and the CNN algorithm is currently the most widely used method for categorizing visual data. | ✓ | ✓ | × | × |
| [4] | 2021 | This paper provides a comprehensive and methodical review of deep learning approaches that can aid in the early detection of skin cancer. | × | ✓ | ✓ | ✓ |
| [5] | 2021 | This paper employs two approaches. The first approach uses radiobiological models such as those for tumor control probability (TCP), normal tissue complication probability (NTCP), and equivalent uniform dose. The second approach constructs statistical models that make use of all the information that is pertinent to disease prognosis, such as demographic information, laboratory test results, image data, and dosimetry, in order to determine the relationship between these factors and clinical outcomes. | ✓ | × | ✓ | ✓ |
| [6] | 2021 | This review includes topics related to the anatomy of brain tumors, including publicly accessible datasets, augmentation techniques, segmentation, feature extraction, classification, deep learning, transfer learning, and quantum machine learning for analysis. | ✓ | ✓ | ✓ | ✓ |
| [7] | 2021 | In this paper, emphasis is placed on presenting potentially game-changing technology of the future in clinical settings by bridging the gap between biology and artificial intelligence and explaining how AI-based assistance can assist oncologists in providing precise therapy. | ✓ | × | ✓ | ✓ |
| [8] | 2020 | Using machine learning, including supervised, unsupervised, and deep learning approaches, the process of diagnosing and curing cancer is facilitated in this paper. | ✓ | ✓ | ✓ | × |
| [9] | 2020 | This paper emphasizes Raman Spectroscopy and ML for better medical diagnostics in cancer. | ✓ | × | ✓ | ✓ |
| [10] | 2020 | This paper uses GoogleNet from CNN to train cancer images in a type of learning called “transfer learning.” A cancer-imaging database is used to pull out multimodal features such as texture, morphology, entropy, SIFT, and EFDs. The performance of both single features and combinations of features are evaluated using strong machine learning techniques. SVM Gaussian is used, along with a number of different features, including texture, morphological, and EFDs, in order to perform the machine learning analysis that gives the best results, with a sensitivity and total accuracy of 99.71%, followed by SVM Gaussian with texture + SIFT features, which gives a sensitivity of 98.83% and an area under the curve (AUC) of 0.999. When GoogleNet is used with the Deep Learning CNN approach, the results are 100% specificity, sensitivity, PPV, and TA and an AUC of 1.00. | × | ✓ | ✓ | ✓ |
| [11] | 2019 | This paper attempts to outline the pathophysiology, imaging modalities, and automatic computer-assisted approaches for the characterization of brain cancer within the context of machine learning and deep learning. | ✓ | × | ✓ | ✓ |
| [12] | 2018 | According to the findings of this paper, analysis using convolutional neural networks (CNN) has the greatest number of applications in deep learning and medical imaging. | × | ✓ | × | × |
| [13] | 2017 | In this paper, ML is utilized to aid in the surgical treatment of epilepsy, brain tumors, spinal lesions, neurovascular pathology, Parkinson’s disease, traumatic brain injury, and hydrocephalus. | ✓ | × | ✓ | ✓ |
| References | Dataset | Type of Dataset | Key Points Regarding the Dataset |
|---|---|---|---|
| [14] | TCIA | Radiomic | TCIA consists of a collection of medical images, which includes CT scans of people with lung cancer. The dataset contains data on the characteristics, diagnosis, and course of treatment for patients. |
| [15] | NLST | Radiologic and clinical data | The National Lung Screening experiment (NLST) dataset is a large-scale clinical experiment that was conducted at multiple institutions to examine the efficacy of low-dose CT screening for lung cancer. The collection contains CT scans obtained from approximately 53,000 participants, which include both those who had cancer and healthy controls. |
| [16] | LUNA16 | Radiomic | LUNA16 contains 888 CT scans, each with a resolution of 512 × 512 pixels and a slice thickness of 0.5–3.0 mm. The dataset includes annotations for nodules that indicate information such as where the nodule is, how big it is, and how likely it is to be cancerous. |
| [7] | ChEMBL and PubChem | Clinical and Genomic | Both ChEMBL and PubChem are large databases with significant amounts of information concerning chemical compounds and their functions in living things. It contains carefully chosen information about the properties and actions of small molecules such as drugs and drug candidates, natural products, and man-made compounds. Bioassay data, including how active a compound is against a certain target or in a certain cell line, are also included in ChEMBL. |
| [17,18] | BRATS 2015, 2016 | Radiomic | BRATS 2015 and 2016 contain 220 high-grade and 54 low-grade glioma MRIs. |
| [19] | BRATS 2017 | Radiomic | BRATS 2017 consists of 285 brain-tumor MRI scans. |
| [20] | BRATS 2018 | Radiomic | With each case including four MRI modalities, the BRATS 2018 dataset consists of 3D brain MRIs and ground-truth brain tumor segmentations annotated by physicians. |
| [21] | LIDC-IDRI | Radiomic | In all, there are 1018 low-dose lung computing tomography scans from 1010 lung patients in LIDC-IDRI. |
| [22] | WBCD | Clinical | In WBCD, to determine features, a digital image of a fine needle aspirate (FNA) of a breast mass is employed. |
| [23] | MIAS | Radiomic | MIAS contains original “Portable Gray Map” (PGM) format photos (322 in total (161 pairs)) captured at a 50-micron resolution as well as related ground-truth information. |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Breast | [27] | Depending on the strength of the connection, it acts and matches, producing the match as necessary. | Accuracy = 95% |
| [28] | In an ANN, a single neuron receives input from other neurons, multiplies it by the appropriate weight Wij, and then uses an activation function to create a weighted output f. (Xj). | AUC value, Accuracy, Sn value, Sp value | |
| [29] | Pre-processing was performed to increase accuracy by 2%. | More than 98% | |
| Ovarian | [30] | Classification of an ovarian tumor. | Accuracy = 80% (dermoid cyst) Accuracy = 70% (Follicular cysts) |
| Pancreatic | [31] | Identification of pancreatic cancer. | Sensitivity = 87.3% Specificity = 80.8% AUC = 0.86 |
| Lung | [32] | To reduce false-positive nodules, previously extracted characteristics were used. | 73% sensitivity to detection |
| Liver | [33] | Hepatitis data analysis. | Accuracy = 86.3 |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Lung | [36] | Prediction of false and true positives | 89.64% Accuracy |
| Breast | [37] | Data were collected with the help of doctors | 98.2% accuracy |
| Liver | [38] | Liver disease prediction model based on the CatBoost algorithm | Precision 0.67 Recall 0.66 F1-score 0.63 |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Ovarian | [41] | Classify types of ovarian tumors and cancer. | Accuracy = 89.52% (Using Median) |
| [42] | Comparison of the performances of different machine learning models. | Accuracy = 99.1% Sensitivity = 100% Specificity = 97.9% (Using Simple Tree) | |
| Lung | [43] | Contrast with other valued classification techniques such as SVM, KNN, MLP, and Logistic Regression. | Accuracy = 90.688% |
| Breast | [29] | Compared to ANN and linear regression, this method generated the best results. | Accuracy = 93.6% |
| Type of Cancer | References | Key Contribution | Performance Metrics | ||
|---|---|---|---|---|---|
| Brain | [11] | Tumor classification into different classes: normal region and abnormal region. | Statistical Features | Gabor Wavelet Features | |
| Linear Kernel | 94.8 ± 0.3% | 91.7 ± 0.4% | |||
| RBF Kernel | 96.1 ± 0.2% | 95.3 ± 0.6% | |||
| Brain | [108] | Novel and effective method for brain tumor segmentation and identification in MRI images. | Accuracy = 88.71% | ||
| Breast | [29] | K ranged from 1 to 15 and best was equaled when k = 1. | Accuracy = 98.25%(KNN) Accuracy = 98.83% (fuzzy KNN) | ||
| [37] | Data were collected with the help of doctors. | Accuracy = 98.8% | |||
| Ovarian | [41] | This method was used to classify types of ovarian tumors and cancer | Accuracy = 86.666% (Using Median) | ||
| [42] | The accuracy and false-positive rates of various machine learning models. | Accuracy = 93.5% Sensitivity = 93.5% Specificity = 93.5% (Using Weighted KNN) | |||
| [46] | Assessment of classification-model performance using data and selected features. | Balanced Accuracy = 84% Sensitivity = 90% Specificity = 77% F1 Measure = 92% | |||
| Assessment of classification-model performance using random features. | Balanced Accuracy = 71% Sensitivity = 96% Specificity = 46% F1 Measure = 91% | ||||
| Oral | [43] | Predict pathologic staging and TNM. | Accuracy = 85% | ||
| Prostate | [47] | Classifies positive and negative samples. | Accuracy = 78.75 | ||
| Liver | [38] | Liver disease prediction model based on the CatBoost algorithm. | Precision 0.72 Recall 0.71 F1-score 0.70 | ||
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Brain | [11] | Used for glioma classification into benign and malignant types. | AUC = 0.91 |
| Ovarian | [30] | Early detection and prediction for Poly Cystic Ovarian Syndrome. | Accuracy = 89.02% |
| [41] | Used to classify types of ovarian tumors and cancer. | Accuracy = 90.476% (Using Median) | |
| [46] | Assessment of classification-model performance using data and selected features. | Balanced Accuracy = 89% Sensitivity = 96% Specificity = 83% F1 Measure = 96% | |
| Assessment of classification-model performance using random features. | Balanced Accuracy = 70% Sensitivity = 100% Specificity = 41% F1 Measure = 92% | ||
| [49] | Ovarian cancer classification using pathophysiological complications. | Accuracy = 72% Precision = 72% Recall = 85% F1 Score = 78% | |
| Oral | [43] | Contrast with other valued classification techniques such as SVM, KNN, MLP, and Logistic Regression. | 91% accuracy |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Breast | [28] | DDSM dataset classification as normal or abnormal. | AUC = 94.4% |
| [51] | SMV used on a DDSM dataset to classify into benign or malignant. | Accuracy = 93.1% Area under ROC curve = 0.7 | |
| [37] | Gene expression and DNA methylation data were filtered to obtain common genes to determine the presence of tumors. | Accuracy = 99.68% on spark Accuracy = 98.03% on Weka tool | |
| [37] | Recursive feature extraction was used to evaluate SVM. | Accuracies of 99% on linear kernel, 84% on sigmoid and 98% on RBF respectively | |
| Lung | [52] | SVM was helpful in prediction based on continuous and categorical data. | The overall accuracy was 100% |
| [36] | SVM was used to propose graph-based image representation with deep point cloud models. | Average of 95% accuracy | |
| [32] | SVM’s data-driven methodology and viability without a fictitious system that generates an accurate classification of cancer. | 97%-identification 87%-prediction | |
| Ovarian | [49] | Classification of ovarian cancer based on pathophysiological complications. | Accuracy = 71% Precision = 71% F1 Score = 78% Recall = 86% |
| [41] | SVM was used to classify different kinds of ovarian tumors and cancer. | Accuracy = 83.809% (SVC RBF) | |
| [42] | Performance evaluation of various machine learning models. | Accuracy = 94.4% Specificity = 89.7% Sensitivity = 94.1% (Using Quadratic SVM) | |
| [46] | Assessment of classification-model performance using data and selected features. | Balanced Accuracy = 85% Sensitivity = 96% Specificity = 74% F1 Measure = 94% | |
| Assessment of classification-model performance using random features. | Balanced Accuracy = 81% Sensitivity = 97% Specificity = 66% F1 Measure = 94% | ||
| Oral | [43] | Using a microarray analysis and expression profile on the patient, an SVM classifier was used to identify OSCC tumors. | Accuracy = 88% |
| [53] | The blue automatic technique component of the experimental outcome was successful. | Accuracy = 98.01% | |
| Liver | [54] | SVM was used to predicting tumor state in liver-cancer patients. | SD = 0.151 AMAUC = 0.897 SD = 0.143 AMACC = 0.895 |
| Liver | [54] | SVM was tasked with predicting the states of tumors in colon-cancer patients | SD = 0.153 AMAUC = 0.897 SD = 0.159 AMACC = 0.890 |
| Liver | [55] | Based on liver MR scans, a classification approach for diagnosing early-stage liver cancer was used. | Accuracy = 80% |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Ovarian | [42] | Performance evaluation of various machine learning models. | Accuracy = 93% Specificity = 89.9% Sensitivity = 95.7% (Using Subspace Discriminant) |
| Prostate | [58] | Substantially less expensive and more effective for predicting urinary toxicity. | Mean AUC = 0.63 ± 0.05 |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Prostate | [47] | It provides a methodological framework for modelling event likelihood. | Accuracy = 91.99% |
| Liver | [38] | Liver disease prediction model based on the CatBoost algorithm | Precision = 0.65 Recall = 0.63 F1-score = 0.62 |
| Type of Cancer | References | Models Used | Key Contribution | Performance Metrics |
|---|---|---|---|---|
| Brain | [11] | SVM and KNN | Hybrid models is used to make classifications during the process of acquiring HSI from patients for real-time image analysis, SVM is used to obtain a supervised classification map, and KNN is used for finding the spatial–spectral classification map. | Accuracy = 97.5% |
| Breast | [28] | KNN and SVM | WBDC dataset, | Accuracy = 97.38% |
| [62] | Rough Set and SVM | RS is used to determine the best features, and SVM increased its accuracy. | Accuracy = 98.53% |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Lung | [32] | RNN is used to examine and study medical imaging including computed tomography (CT), magnetic resonance imaging (MRI), and X-ray images. | Accuracy = 98.08% |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Ovarian | [64] | The model consists of 3 convolutional layers, which include a max-pooling and up-sampling layer. Pooling size is 9, and operator of convolution is set as 1. After feature extraction, ELM and SVM generated the best results. | Average using ELM = 95.6811 |
| Breast and Lung | [67] | An Eight-category classification approach was implemented to assess (a) whether a cell is healthy or malignant and (b) the type of cell (and consequently cancer type and state) it is associated with. | Accuracy = 87.5% Sensitivity = 80% MCC = 0.775 |
| Sensitivity = 94.73% Accuracy = 91.3% MCC = 0.697 |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Multiple Types mainly thyroid, lung and breast | [71] | There was just one hidden layer composed of 100 LSTM units. The sigmoid function was set as the default in the output layer. | AUC = 0.74 |
| Prostate | [72] | LSTM outperformed conventional cox-proportional hazards | AUC = 0.936 |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Lung | [74] | DNNs offer a way to validate the robustness of OPF in the classification problem. | Accuracy = 98.08% |
| Oral | [75] | DNN uses the Gravitational Search Optimized Echo State Neural Networks to analyze oral X-ray pictures and predict oral cancer. | Accuracy = 99.2% |
| Prostate | [76] | DNN is used to determine the survival times of people with prostate cancer. | Accuracy = 85.64% |
| Ovarian | [30] | DNN is used to detect cysts in females. | Accuracy = 92.11% |
| Liver | [77] | DNN is used to examine haemangioma, hepatocellular, and metastatic carcinoma tumors. | Accuracy = 99.39% |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Lung | [80] | DBNs are used to extract features for lung cancer detection. | Accuracy = 81.19% |
| Breast | [80] | DBs are used to extract features for breast cancer detection. | KPI Accuracy = 99.68% |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Lung | [84] | DCNNs support medical imaging techniques that tend to use structured databases. | All slicers of 75 patient folders of a LIDC-IDRI dataset were extracted and presented with lung reports and stored in .png file formats at 8-bit resolution. A total of 282 images with 282 masks were obtained. |
| [36] | DCNNs addressed the issue of overfitting that developed throughout the training process because of a dataset imbalance. | Average AUC = 85.0% | |
| [74] | DCNNs are used to classify NSCLC lymph node metastases | Accuracy = 94.73% | |
| [32] | A tumor is located using an attention-guided DCNN (AG-CNN). | Accuracy = 74.43 ± 6.01 | |
| [85] | DCNNs have significantly surpassed the prior generation of Radiomic/texture analysis techniques. | AUC of low 90 s | |
| [107] | Pulmonary nodules are classified as malignant or benign in lung cancer. | Accuracy = 92.4% (Nodule Classification) | |
| Oral | [86] | DCNNs have the ability to create their own representations, which are required for pattern recognition. | |
| [87] | The strategy used by the DCNN involved looking for images, training, data, quotations, and classification. | Accuracy = 97.21% | |
| [53] | The combination of WLI and AFI provide the most details on the type of lesion and the extent of the damaged area once problematic spots have been identified. | AUC = 90.8% | |
| Prostate | [88] | DCNNs radically improve the detection and treatment of prostate cancer. | Accuracy = 95% |
| Ovarian | [89] | DCNNs are used to identify ovarian disease using cytological images | Accuracy = 78.2% |
| Type of Cancer | References | Key Contribution | Performance Metrics |
|---|---|---|---|
| Breast | [92] | ClassRBM was trained with a learning rate of between 0.01 and 0.1, a momentum rate of 0.5, and 100,000 iterations. | Accuracy = 0.738 ± 0.015 (highest using classRBM + DropOut) |
| Oral | [93] | To train the Deep Boltzmann Machine network for class construction, 850 nm-wavelength cancer cell hyperspectral pictures were utilized. | Accuracy% = 95.5 Sensitivity% = 93.5 Specificity% = 94.94 False positive (FP) = 2.14 |
| Type of Cancer | References | Models Used | Key Contribution | Performance Metrics |
|---|---|---|---|---|
| Breast | [94] | YOLO, CNN, ResNet-50, and InceptionResNet-V2. | Two datasets, DDSM and INbreast, are used. | CNN 88.7% ResNet-50 92.5% InceptionResNet-V2 95.3% |
| Breast | [95] | Extreme learning machine (ANN). | Breast cancer detection. | Accuracy = 96.92% |
| Prostate | [96] | Radial basis function neural network (RBF). | Enhanced classification accuracy. | Accuracy = 94.1%l |
| References | Smart Phone Application-Name | Mobile Operating System | Availability | App Description and Features | Users | Utility |
|---|---|---|---|---|---|---|
| [110] | SkinVision | iOS 13.0 or Above Android 7.0 or Above | Partially Free | Skin tracking and skin spot analysis. | Patients | Assessment |
| [111] | Breast Check Now | iOS 10.0 or Above Android 4.4 or Above | Free | Breast self-exam instructions. | Women | Awareness |
| [112] | Ada Health | iOS 13.0 or Above Android 5.0 or Above | Free | Symptom assessment tool and health library. | Patients | Assessment |
| [113] | Cancer.Net Mobile | iOS 10.0 or Above Android 5.0 or Above | Free | Cancer-related resource with a tool for tracking symptoms, appointments, and medications. | Patients and Physicians | Information |
| [114] | ASCO Guidelines | iOS 12.0 or Above Android 5.0 or Above | Free | Tools for risk assessment, staging, and treatment-related decision-making based on the latest clinical evidence. | Physician | Guidance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jain, S.; Naicker, D.; Raj, R.; Patel, V.; Hu, Y.-C.; Srinivasan, K.; Jen, C.-P. Computational Intelligence in Cancer Diagnostics: A Contemporary Review of Smart Phone Apps, Current Problems, and Future Research Potentials. Diagnostics 2023, 13, 1563. https://doi.org/10.3390/diagnostics13091563
Jain S, Naicker D, Raj R, Patel V, Hu Y-C, Srinivasan K, Jen C-P. Computational Intelligence in Cancer Diagnostics: A Contemporary Review of Smart Phone Apps, Current Problems, and Future Research Potentials. Diagnostics. 2023; 13(9):1563. https://doi.org/10.3390/diagnostics13091563
Chicago/Turabian StyleJain, Somit, Dharmik Naicker, Ritu Raj, Vedanshu Patel, Yuh-Chung Hu, Kathiravan Srinivasan, and Chun-Ping Jen. 2023. "Computational Intelligence in Cancer Diagnostics: A Contemporary Review of Smart Phone Apps, Current Problems, and Future Research Potentials" Diagnostics 13, no. 9: 1563. https://doi.org/10.3390/diagnostics13091563
APA StyleJain, S., Naicker, D., Raj, R., Patel, V., Hu, Y.-C., Srinivasan, K., & Jen, C.-P. (2023). Computational Intelligence in Cancer Diagnostics: A Contemporary Review of Smart Phone Apps, Current Problems, and Future Research Potentials. Diagnostics, 13(9), 1563. https://doi.org/10.3390/diagnostics13091563