

CT Perfusion in Lacunar Stroke: A Systematic Review

 , , ,
, , ,
Abstract
1. Introduction
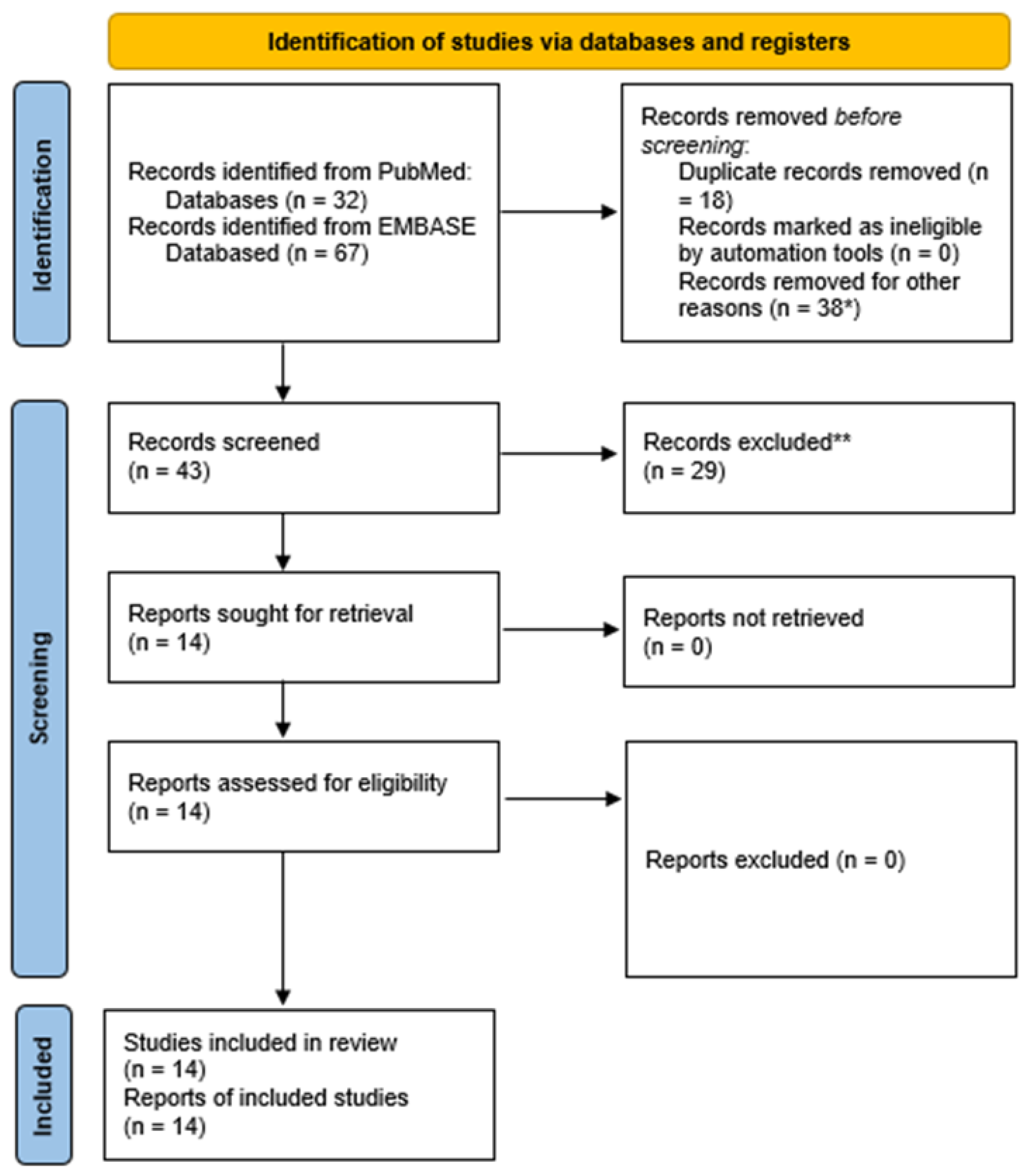
2. Materials and Methods
2.1. Sources
2.2. Eligibility Criteria
2.3. Data Extraction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Ma, H.; Campbell, B.C.; Parsons, M.W.; Churilov, L.; Levi, C.R.; Hsu, C.; Kleinig, T.J.; Wijeratne, T.; Curtze, S.; Dewey, H.M.; et al. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. N. Engl. J. Med. 2019, 380, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.V.; Ma, H.; A Ringleb, P.; Parsons, M.W.; Churilov, L.; Bendszus, M.; Levi, C.R.; Hsu, C.; Kleinig, T.J.; Fatar, M.; et al. Extending thrombolysis to 4·5–9 h and wake-up stroke using perfusion imaging: A systematic review and meta-analysis of individual patient data. Lancet 2019, 394, 139–147. [Google Scholar] [CrossRef]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, I–LXII. [Google Scholar] [CrossRef]
- Thomalla, G.; Boutitie, F.; Ma, H.; Koga, M.; Ringleb, P.; Schwamm, L.H.; Wu, O.; Bendszus, M.; Bladin, C.F.; Campbell, B.C.V.; et al. Intravenous alteplase for stroke with unknown time of onset guided by advanced imaging: Systematic review and meta-analysis of individual patient data. Lancet 2020, 396, 1574–1584. [Google Scholar] [CrossRef] [PubMed]
- Benson, J.; Payabvash, S.; Mortazavi, S.; Zhang, L.; Salazar, P.; Hoffman, B.; Oswood, M.; McKinney, A. CT Perfusion in Acute Lacunar Stroke: Detection Capabilities Based on Infarct Location. Am. J. Neuroradiol. 2016, 37, 2239–2244. [Google Scholar] [CrossRef]
- Rudilosso, S.; Urra, X.; Román, L.S.; Laredo, C.; Lopez-Rueda, A.; Amaro, S.; Oleaga, L.; Chamorro, Á. Perfusion Deficits and Mismatch in Patients with Acute Lacunar Infarcts Studied with Whole-Brain CT Perfusion. Am. J. Neuroradiol. 2015, 36, 1407–1412. [Google Scholar] [CrossRef]
- Tan, M.Y.Q.; Singhal, S.; Ma, H.; Chandra, R.V.; Cheong, J.; Clissold, B.B.; Ly, J.; Srikanth, V.; Phan, T.G. Examining Subcortical Infarcts in the Era of Acute Multimodality CT Imaging. Front. Neurol. 2016, 7, 220. [Google Scholar] [CrossRef]
- Lin, K.; Do, K.G.; Ong, P.; Shapiro, M.; Babb, J.S.; Siller, K.A.; Pramanik, B.K. Perfusion CT Improves Diagnostic Accuracy for Hyperacute Ischemic Stroke in the 3-Hour Window: Study of 100 Patients with Diffusion MRI Confirmation. Cerebrovasc. Dis. 2009, 28, 72–79. [Google Scholar] [CrossRef]
- Campbell, B.C.V.; Weir, L.; Desmond, P.M.; Tu, H.T.H.; Hand, P.J.; Yan, B.; Donnan, G.; Parsons, M.W.; Davis, S.M. CT perfusion improves diagnostic accuracy and confidence in acute ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2013, 84, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Zhu, C.; Qin, W. Perfusion Deficits in Different Mechanisms of Two Subtypes of Acute Stroke with Diffusion MRI confirmation. Curr. Neurovasc. Res. 2022. preprint. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Yassi, N.; Sharma, G.; Yan, B.; Desmond, P.M.; Davis, S.M.; Campbell, B.C. Diagnosing acute lacunar infarction using CT perfusion. J. Clin. Neurosci. 2016, 29, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Esperon, C.; Visser, M.; Churilov, L.; Miteff, F.; Bivard, A.; Lillicrap, T.; Levi, C.R.; Spratt, N.J.; Parsons, M.W. Role of Computed Tomography Perfusion in Identification of Acute Lacunar Stroke Syndromes. Stroke 2021, 52, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Das, T.; Settecase, F.; Boulos, M.; Huynh, T.; d’Esterre, C.D.; Symons, S.P.; Zhang, L.; Aviv, R.I. Multimodal CT provides improved per-formance for lacunar infarct detection. Am. J. Neuroradiol. 2015, 36, 1069–1075. [Google Scholar] [CrossRef]
- Eckert, B.; Küsel, T.; Leppien, A.; Michels, P.; Müller-Jensen, A.; Fiehler, J. Clinical outcome and imaging follow-up in acute stroke patients with normal perfusion CT and normal CT angiography. Neuroradiology 2010, 53, 79–88. [Google Scholar] [CrossRef]
- Hana, T.; Iwama, J.; Yokosako, S.; Yoshimura, C.; Arai, N.; Kuroi, Y.; Koseki, H.; Akiyama, M.; Hirota, K.; Ohbuchi, H.; et al. Sensitivity of CT perfusion for the diagnosis of cerebral infarction. J. Med. Investig. 2014, 61, 41–45. [Google Scholar] [CrossRef]
- Rudilosso, S.; Laredo, C.; Mancosu, M.; Moya-Planas, N.; Zhao, Y.; Chirife, O.; Chamorro, Á.; Urra, X. Cerebral Perfusion and Compensatory Blood Supply in Patients with Recent Small Subcortical Infarcts. J. Cereb. Blood Flow Metab. 2019, 39, 1326–1335. [Google Scholar] [CrossRef]
- Akhtar, N.; Kamran, S.; Elkhider, H.; Al-Makki, S.; Mhjob, N.; ElShiekh, L.; AlHussain, H.; Ali, M.; Khodair, R.; Wadiwala, F.; et al. Progression of stroke deficits in patients presenting with mild symptoms: The underlying etiology determines outcome. PLoS ONE 2020, 15, e0231448. [Google Scholar] [CrossRef]
- Nagaraja, N.; Farooqui, A.; Albayram, M.S.; Reddy, V.B.N. Neurological deterioration and computed tomography perfusion changes with increased time to peak in lacunar stroke. Brain Circ. 2022, 8, 17–23. [Google Scholar] [CrossRef]
- Oppenheim, C.; Lamy, C.; Touze, E.; Calvet, D.; Hamon, M.; Mas, J.L.; Méder, J.F. Do transient ischemic attacks with diffusion-weighted imaging abnormalities corre-spond to brain infarctions? Am. J. Neuroradiol. 2006, 27, 1782–1787. [Google Scholar] [PubMed]
- McVerry, F.; Dani, K.A.; MacDougall, N.J.; MacLeod, M.J.; Wardlaw, J.; Muir, K.W. Derivation and Evaluation of Thresholds for Core and Tissue at Risk of Infarction Using CT Perfusion. J. Neuroimaging 2014, 24, 562–568. [Google Scholar] [CrossRef]
- Jiang, S.; Cui, J.-Y.; Yan, Y.-Y.; Yang, T.; Tao, W.-D.; Wu, B. Association of compromised cerebral perfusion with lenticulostriate artery impairments in the subacute phase of branch atheromatous disease. Ther. Adv. Neurol. Disord. 2022, 15, 17562864221109746. [Google Scholar] [CrossRef] [PubMed]
- Bollwein, C.; Plate, A.; Sommer, W.H.; Thierfelder, K.M.; Janssen, H.; Reiser, M.F.; Straube, A.; von Baumgarten, L. Diagnostic accuracy of whole-brain CT perfusion in the detection of acute infratentorial infarctions. Neuroradiology 2016, 58, 1077–1085. [Google Scholar] [CrossRef]
- Ay, H.; Buonanno, F.; Rordorf, G.; Schaefer, P.; Schwamm, L.; Wu, O.; Gonzalez, R.; Yamada, K.; Sorensen, G.; Koroshetz, W. Normal diffusion-weighted MRI during stroke-like deficits. Neurology 1999, 52, 1784. [Google Scholar] [CrossRef]
- González, R.G.; Schaefer, P.W.; Buonanno, F.S.; Schwamm, L.; Budzik, R.F.; Rordorf, G.; Wang, B.; Sorensen, A.G.; Koroshetz, W.J. Diffusion-weighted MR Imaging: Diagnostic Accuracy in Patients Imaged within 6 Hours of Stroke Symptom Onset. Radiology 1999, 210, 155–162. [Google Scholar] [CrossRef]
- Ghaznawi, R.; I Geerlings, M.; Jaarsma-Coes, M.; Zwartbol, M.H.; Kuijf, H.J.; Van Der Graaf, Y.; Witkamp, T.D.; Hendrikse, J.; De Bresser, J. The association between lacunes and white matter hyperintensity features on MRI: The SMART-MR study. J. Cereb. Blood Flow Metab. 2019, 39, 2486–2496. [Google Scholar] [CrossRef]
- Biesbroek, J.; Niesten, J.; Dankbaar, J.; Biessels, G.; Velthuis, B.; Reitsma, J.; van der Schaaf, I. Diagnostic Accuracy of CT Perfusion Imaging for Detecting Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Cerebrovasc. Dis. 2013, 35, 493–501. [Google Scholar] [CrossRef]
- Caplan, L.R. Lacunar Infarction and Small Vessel Disease: Pathology and Pathophysiology. J. Stroke 2015, 17, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Hernández, M.D.C.V.; Grimsley-Moore, T.; Sakka, E.; Thrippleton, M.J.; Chappell, F.M.; Armitage, P.A.; Makin, S.; Wardlaw, J.M. Lacunar Stroke Lesion Extent and Location and White Matter Hyperintensities Evolution 1 Year Post-lacunar Stroke. Front. Neurol. 2021, 12, 640498. [Google Scholar] [CrossRef]
- Förster, A.; Mürle, B.; Böhme, J.; Al-Zghloul, M.; Kerl, H.U.; Wenz, H.; Groden, C. Perfusion-weighted imaging and dynamic 4D angio-grams for the estimation of collateral blood flow in lacunar infarction. J. Cereb. Blood Flow Metab. 2016, 36, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Cheng, Y.; Guo, W.; Kwapong, W.R.; Ye, C.; Wu, B.; Zhang, S.; Liu, M. Clinical features and imaging markers of small vessel disease in symptomatic acute subcortical cerebral microinfarcts. BMC Neurol. 2022, 22, 311. [Google Scholar] [CrossRef]
- Chalela, J.A.; Ezzeddine, M.; Latour, L.; Warach, S. Reversal of perfusion and diffusion abnormalities after intravenous thrombo-lysis for a lacunar infarction. J. Neuroimaging 2003, 13, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Keir, S.L.; Wardlaw, J.M. Systematic review of diffusion and perfusion imaging in acute ischemic stroke. Stroke 2000, 31, 2723–2731. [Google Scholar] [CrossRef]
- Del Bene, A.; Makin, S.; Doubal, F.N.; Inzitari, D.; Wardlaw, J.M. Variation in Risk Factors for Recent Small Subcortical Infarcts with Infarct Size, Shape, and Location. Stroke 2013, 44, 3000–3006. [Google Scholar] [CrossRef] [PubMed]
- Redgrave, J.N.; Coutts, S.B.; Schulz, U.G.; Briley, D.; Rothwell, P.M. Systematic Review of Associations Between the Presence of Acute Ischemic Lesions on Diffusion-Weighted Imaging and Clinical Predictors of Early Stroke Risk After Transient Ischemic Attack. Stroke 2007, 38, 1482–1488. [Google Scholar] [CrossRef]
- Schulz, U.G.; Briley, D.; Meagher, T.; Molyneux, A.; Rothwell, P.M. Diffusion-Weighted MRI in 300 Patients Presenting Late with Subacute Transient Ischemic Attack or Minor Stroke. Stroke 2004, 35, 2459–2465. [Google Scholar] [CrossRef]
- Kidwell, C.S.; Alger, J.R.; Di Salle, F.; Starkman, S.; Villablanca, P.; Bentson, J.; Saver, J. Diffusion MRI in Patients with Transient Ischemic Attacks. Stroke 1999, 30, 1174–1180. [Google Scholar] [CrossRef]
- Engelter, S.T.; Provenzale, J.M.; Petrella, J.R.; Alberts, M.J. Diffusion MR Imaging and Transient Ischemic Attacks. Stroke 1999, 30, 2759–2768. [Google Scholar] [CrossRef]
- Winbeck, K.; Bruckmaier, K.; Etgen, T.; Von Einsiedel, H.G.; Röttinger, M.; Sander, D. Transient Ischemic Attack and Stroke Can Be Differentiated by Analyzing Early Diffusion-Weighted Imaging Signal Intensity Changes. Stroke 2004, 35, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Engelter, S.T.; Wetzel, S.G.; Radue, E.W.; Rausch, M.; Steck, A.J.; Lyrer, P.A. The clinical significance of diffusion-weighted MR imaging in infratentorial strokes. Neurology 2004, 62, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Lövblad, K.O.; Laubach, H.J.; E Baird, A.; Curtin, F.; Schlaug, G.; Edelman, R.R.; Warach, S. Clinical experience with diffusion-weighted MR in patients with acute stroke. Am. J. Neuroradiol. 1998, 19, 1061–1066. [Google Scholar]
- van Everdingen, K.; van der Grond, J.; Kappelle, L.; Ramos, L.; Mali, W. Diffusion-Weighted Magnetic Resonance Imaging in Acute Stroke. Stroke 1998, 29, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Oppenheim, C.; Stanescu, R.; Dormont, D.; Crozier, S.; Marro, B.; Samson, Y.; Rancurel, G.; Marsault, C. False-negative Diffusion-weighted MR Findings in Acute Ischemic Stroke. Am. J. Neuroradiol. 2000, 21, 1434–1440. [Google Scholar] [PubMed]
- Wang, P.Y.-K.; Barker, P.B.; Wityk, R.J.; Uluğ, A.M.; Van Zijl, P.C.M.; Beauchamp, N.J. Diffusion-Negative Stroke: A Report of Two Cases. Am. J. Neuroradiol. 1999, 20, 1876–1880. [Google Scholar] [PubMed]
- Zuo, L.; Zhang, Y.; Xu, X.; Li, Y.; Bao, H.; Hao, J.; Wang, X.; Li, G. A retrospective analysis of negative diffusion-weighted image results in patients with acute cerebral infarction. Sci. Rep. 2015, 5, srep08910. [Google Scholar] [CrossRef] [PubMed]
- Sylaja, P.; Coutts, S.B.; Krol, A.; Hill, M.D.; Demchuk, A.M. When to Expect Negative Diffusion-Weighted Images in Stroke and Transient Ischemic Attack. Stroke 2008, 39, 1898–1900. [Google Scholar] [CrossRef]
- Roberts, H.C.; Roberts, T.P.L.; Smith, W.S.; Lee, T.J.; Fischbein, N.J.; Dillon, W.P. Multisection Dynamic CT Perfusion for Acute Cerebral Ischemia: The “Toggling-table” Technique. Am. J. Neuroradiol. 2001, 22, 1077–1080. [Google Scholar] [PubMed]
- Youn, S.W.; Kim, J.H.; Weon, Y.-C.; Kim, S.H.; Han, M.-K.; Bae, H.-J. Perfusion CT of the Brain Using 40-mm-Wide Detector and Toggling Table Technique for Initial Imaging of Acute Stroke. Am. J. Roentgenol. 2008, 191, W120–W126. [Google Scholar] [CrossRef]
- Heit, J.J.; Wintermark, M. Perfusion computed tomography for the evaluation of acute ischemic stroke: Strengths and pitfalls. Stroke 2016, 47, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Wintermark, M.; Smith, W.S.; Ko, N.U.; Quist, M.; Schnyder, P.; Dillon, W.P. Dynamic perfusion CT: Optimizing the temporal resolu-tion and contrast volume for calculation of perfusion CT parameters in stroke patients. Am. J. Neuroradiol. 2004, 25, 720–729. [Google Scholar]
- Yi, F.; Cai, M.; Jacob, M.A.; Marques, J.; Norris, D.G.; Duering, M.; Tuladhar, A.M.; de Leeuw, F.-E. Spatial Relation Between White Matter Hyperintensities and Incident Lacunes of Presumed Vascular Origin: A 14-Year Follow-Up Study. Stroke 2022, 53, 3688–3695. [Google Scholar] [CrossRef]
- Huynh, T.; Murphy, B.; Pettersen, J.; Tu, H.; Sahlas, D.; Zhang, L.; Symons, S.; Black, S.; Lee, T.-Y.; Aviv, R. CT Perfusion Quantification of Small-Vessel Ischemic Severity. Am. J. Neuroradiol. 2008, 29, 1831–1836. [Google Scholar] [CrossRef]
- Ramli, N.; Ho, K.; Nawawi, O.; Chong, H.; Tan, C. CT perfusion as a useful tool in the evaluation of leuko-araiosis. Biomed. Imaging Interv. J. 2006, 2, e16. [Google Scholar] [CrossRef] [PubMed]
- Rudilosso, S.; Laredo, C.; Vivancos, C.; Urra, X.; Llull, L.; Renú, A.; Obach, V.; Zhao, Y.; Moreno, J.; Lopez-Rueda, A.; et al. Leukoaraiosis May Confound the Interpretation of CT Perfusion in Patients Treated with Mechanical Thrombectomy for Acute Ischemic Stroke. Am. J. Neuroradiol. 2019, 40, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.V.; Christensen, S.; Levi, C.; Desmond, P.M.; Donnan, G.; Davis, S.M.; Parsons, M.W. Comparison of Computed Tomography Perfusion and Magnetic Resonance Imaging Perfusion-Diffusion Mismatch in Ischemic Stroke. Stroke 2012, 43, 2648–2653. [Google Scholar] [CrossRef]
- Leiva-Salinas, C.; Provenzale, J.M.; Wintermark, M. Responses to the 10 Most Frequently Asked Questions About Perfusion CT. Am. J. Roentgenol. 2011, 196, 53–60. [Google Scholar] [CrossRef]
- Konstas, A.; Goldmakher, G.; Lee, T.-Y.; Lev, M. Theoretic Basis and Technical Implementations of CT Perfusion in Acute Ischemic Stroke, Part 2: Technical Implementations. Am. J. Neuroradiol. 2009, 30, 885–892. [Google Scholar] [CrossRef]
- Zedde, M.; Napoli, M.; Grisendi, I.; Assenza, I.; Moratti, C.; Valzania, F.; Pascarella, R. The perfusion status in lacunar stroke: A pathophysiological issue. In preparation.


{kind=link}
| Reference | Country | Study Design | Study Period | Population | Lacunar Stroke Definition | Neuroimaging Comparator |
|---|---|---|---|---|---|---|
| Zhu 2022 [13] | China | Monocenter retrospective cohort | January–December 2021 | 599 CTP examinations in patients with acute stroke symptoms within 12 h and MRI within 7 days of symptom onset | Intracerebral lesions < 20 mm in diameter and fewer than 3 slices or a lesion within the pontine parenchyma on DWI-MRI | MRI |
| Tan 2016 [8] | Australia | Monocenter retrospective cohort | April 2009–March 2013 | 182 patients with ischemic stroke | Single subcortical infarct ≤ 20 mm on follow-up MRI | MRI (median time 15 days) |
| Cao 2016 [14] | Australia | Retrospective cohort | 2009–2013 | 63 patients (32 with RSSI and 30 without lesions on DWI) | Ovoid DWI hyperintensities with maximum diameter ≤ 25 mm in the territory of small penetrating arteries (thalamus, striatum, or corona radiata) | MRI (within 48 h) |
| García-Esperón 2021 [15] | Australia | Retrospective analysis | January 2010–June 2018 | 712 DWI-confirmed stroke patients | Combination of clinical lacunar syndromes, hyperintensity on DWI-MRI in a penetrating vessel territory and no visible vessel occlusion in that region | DWI-MRI |
| Rudilosso 2015 [7] | Spain | Retrospective analysis | January 2009–December 2012 | 33 patients with lacunar syndrome | Infarct volume < 1.767 cm3 (the volume of a sphere with a diameter 1.5 cm) on DWI | MRI; median delay 26 h (IQR 18–43 h) |
| Das, 2015 [16] | UK | Retrospective cohort | March 2011–February 2013 | 88 patients with lacunar syndrome RSSI: 59/88 (67%). | Solitary, subcortical lesions, ≤ 20 mm in greatest diameter | MRI (median time 2d, IQR 1–4.25 d) |
| Benson 2016 [6] | USA | Retrospective cohort | January 2006–July 2011 | 113 patients: 37 (32.7%) lacunar | Infarcts < 20 mm in maximum diameter on DWI (either cortical or subcortical) | MRI within 7 days |
| Lin 2009 [9] | Germany | Retrospective cohort | January 2004–May 2008 | 65 consecutive stroke patients < 3 h and receiving NCCT and CTP and follow-up DWI < 7 days | DWI < 15 mm | DWI-MRI within 7 days |
| Eckert 2011 [17] | Germany | Retrospective cohort | April 2007–April 2008 | 107 stroke patients within 6 h | Not stated | MRI within 2 to 5 days CT if contraindication to MRI |
| Campbell 2013 [10] | Australia | Retrospective cohort | January 2009–September 2011 | 277/475 (58%) ischemic stroke patients < 9 h/wake-up onset studied by CTP | Not stated | CT or MRI |
| Hana 2014 [18] | Japan | Retrospective cohort | October 2008–October 2011 | 87 patients with ischemic stroke with CTP at the admission and DWI-MRI post hospitalization | Not stated | DWI-MRI |
| Rudilosso 2019 [19] | Spain | Retrospective cohort | May 2011–September 2016 | Acute stroke patients undergoing CTA + CTP | RSSI according to the STRIVE definition (a symptomatic hyperintensity in the territory of one perforating arteriole measuring < 20 mm in its maximum diameter in the axial plane on DWI) | DWI-MRI |
| Akhtar 2020 [20] | Qatar | Retrospective cohort | January 2014–April 2017 | 506 acute stroke patients | Not stated | NA |
| Farooqui 2022 [21] | USA | Retrospective cohort | March 2015–June 2016 | Patients with lacunar stroke who had magnetic resonance imaging and CTP performed | Not stated | DWI-MRI |
| Reference | Lacunar Stroke Patients (N) | Women (%) | Mean Age (years) | CTP Technical Notes | CTP Findings |
|---|---|---|---|---|---|
| Zhu 2022 [13] | 29 | 37.9 | 66.9 ± 9.4 | Scanner: 64-section multidetector scanner (Revolution Frontier, GE Healthcare, Siemens) Post-processing software: d fast-processing of ischemic stroke (F-STROKE) software [22] Perfusion maps: TTP, CBF, CBV, MTT | 5/18 (27.8%) in the lacunar stroke group had perfusion deficits in the supratentorial region |
| Tan 2016 [8] | 31 | 44 | 66.4 ± 15.3 | Scanner: General Electric 750HD 64-slice CT scanner or a Philips 128-slice CT scanner Post-processing software: Advantage Windows (GE Medical Systems) and Extended Brilliance Workspace (Philips Healthcare, Best, Netherlands) Perfusion maps: MTT | 12/31 (39%) lacunar stroke patients had a perfusion deficit compared with those with any cortical infarction (120/142, 67%) |
| Cao 2016 [14] | 32 | 32 | 70 ([IQR] 56–79) | Scanner: Somatom 16-slice scanner, Siemens, Erlangen, Germany) Post-processing software: RAPID iSchemicView (Menlo Park, CA, USA) Perfusion maps: CBF, CBV, MTT, and Tmax | The sensitivity of CTP vs. DWI-MRI was 56% for MTT, and significantly lower for Tmax (25%, p < 0.001), CBV (9%, p = 0.021) and CBF (44%, p < 0.001). Using all four maps gained 56% sensitivity, 100% specificity, 100% PPV and 68% NPV. |
| García-Esperón 2021 [15] | 59/106 (55.7%) (59 RSSI, 33 cortical and 14 infratentorial strokes) | NA | 70 (59–79) | Scanner: Aquilion 320-slice CT scanner (Toshiba) Post-processing software: MIStar (Apollo Medical Imaging Technology, Melbourne, Australia) Perfusion maps: CBF, CBV, MTT, DT | 42% SE, 80% SP for RSSI. Visual inspection of CTP maps had higher sensitivity than the automated method (42% vs. 6%). |
| Rudilosso 2015 [7] | 16 | 37.5 | 62.6 | Scanner: Somatom definition Flash 128-slices dual-source CT system Post-processing software: visual assessment by using CT Neuro Perfusion Syngo.via (Siemens Healthcare GmbH); core/penumbra threshold analysis by using MIStar (Apollo Medical Imaging Technology, Melbourne, Australia) Perfusion maps: CBF, CBV, MTT, Tmax, TTP, TTD and MIP | The sensitivity and PPV of CTP were higher than NCCT (63% vs. 19%). The sensitivity of CTP was higher for supratentorial than for infratentorial (65% vs. 16%). Specificity was low (20%). TTD was the most informative map. |
| Das, 2015 [16] | 59 (14/59 pontine) | NA | 72 | Scanner: 64-section CT scanner Postprocessing software: CT Perfusion 4, GE Healthcare Perfusion maps: CBV, CBF and MTT | 36/59 (61%) with a concordant abnormal findings between DWI-MRI and CTP |
| Benson 2016 [6] | 37 (all supratentorial) | 53.1 | 59.8 ± 16.9 | Scanner: 64-section CT scanner Post-processing software: Vitrea workstation (Vital Imaged, Minnetonka, Minnesota) Perfusion maps: TTP, MTT, CBV and CBF | Sensitivity was highest for TTP (49%), and lowest for NCCT (3%). Specigicity mantained high with any map (all > 97%). |
| Lin 2009 [9] | 13/65 | NA | NA | Scanner: 16-slice scanners (Siemens Sensation, Siemens AG, Erlangen, Germany) Postprocessing software: Siemens Syngo Neuro Perfusion CT, Siemens AG Perfusion maps: CBF, CBV, TTP | CTP detected 2/13 (15.4%) LI that were within its coverage volume |
| Eckert 2011 [17] | 54 with no occlusion on CTA | NA | 68.4 | Scanner: 40-row multidetector CT scan, Brilliance 40 (Philips, Eindhoven, The Netherlands) Post-processing software: Philips Medical System, Best, The Netherlands Perfusion maps: MTT, CBF, CBV and TTP | 23/54 (42.59%) patients had normal MMCT and positive follow-up MRI 16/23 (69.56%) were lacunar infarcts within the CTP perfusion maps, 4 were infratentorial infarcts and 3 were territorial infarcts beyond the perfusion maps. |
| Campbell 2013 [10] | NA | NA | Scanner: Siemens Somatom 16-slice multidetector scanner (Siemens, Erlangen, Germany) Postprocessing software: Siemens Syngo NeuroPCT, Siemens Perfusion maps: TTP, CBF, CBV Visual assessment of unthresholded TTP and CBV/CBF maps | Non-diagnostic CTP was due to lacunar infarction (28 (10%)), infarct outside slab coverage (21 (8%)), technical failure (4 (1%)) and reperfusion (2 (0.7%)). | |
| Hana 2014 [18] | NA | NA | Scanner: 64 row detector CT scanner (LightSpeed VCT XT; GE) Post-processing software: CTP software developed by GE Health care Perfusion maps: MTT, CBV, CBF | 55/87 CTP deficit with highr sensitivity in infarcts < 3 cm; sensitivity 0% for lacunar infarction | |
| Rudilosso 2019 [19] | 74 RSSI | 40 | 66.3 (12.1) | Scanner: Somatom Definition Flash 128-section dual-source CT system (Siemens, Erlangen, Germany) Postprocessing software: Syngo CT Neuro Perfusion VA20 (Siemens) Perfusion maps: CBF, CBV, TTP and TTD | On visual inspection, hypoperfusion on CTP was identified in 51 patients (76%), perfusion was normal in 12 patients (18%) and hyperperfusion was observed in the remaining 4 patients (6%). |
| Akhtar 2020 [20] | 130 | NA | NA | Scanner: NA Postprocessing software: NA Perfusion maps: NA | The main reason for not doing CTP was a clinical diagnosis of small vessel (lacunar) stroke. |
| Farooqui 2022 [21] | 49 (19 ND + 30 no ND) | 25 (10 + 15)/49 51.02% | 65 ± 13 vs. 62 ± 15 | Scanner: 320–detector row scanner (Toshiba Aquilion One; Toshiba Medical Imaging, Tokyo Japan) Postprocessing software: Vitrea; Vital Images Minnetonka, Minnesota, USA Perfusion maps: CBF, CBV, MTT, TTP | 63% of patients had stroke diameters < 10 mm. ND patients have a trend for increased TTP in the stroke area compared to the no ND patients [12 (63%) vs. 11 (37%), p = 0.07]. 8 patients had a change in CBV without difference between the two groups. Increased TTP was a predictor of ND on multivariate analysis. MTT was not assessed, considering TTP more sensitive. |
| Reference | CBF | CBV | MTT | DT 1 | TMax | TTP | TTD | Vertical Coverage (mm) |
|---|---|---|---|---|---|---|---|---|
| Zhu 2022 [13] | Y | Y | Y | Y | NR | |||
| Tan 2016 [8] | Y | 80 2 | ||||||
| Cao 2016 [14] | Y | Y | Y | Y | ||||
| García-Esperón 2021 [15] | Y | Y | Y | Y | 160 | |||
| Rudilosso 2015 [7] | Y | Y | Y | Y | Y | Y | 98 | |
| Das, 2015 [16] | Y | Y | Y | NR | ||||
| Benson 2016 [6] | Y | Y | Y | Y | 80 4 | |||
| Lin 2009 [9] | Y | Y | Y | 24 | ||||
| Eckert 2011 [17] | Y | Y | Y | Y | 40 | |||
| Campbell 2013 [10] | Y | Y | Y | 24 4 | ||||
| Hana 2014 [18] | Y | Y | Y | 80 3 | ||||
| Rudilosso 2019 [19] | Y | Y | Y | Y | 98 | |||
| Akhtar 2020 [20] | NA | NA | NA | NA | NA | NA | NA | NR |
| Farooqui 2022 [21] | Y | Y | Y | Y | 160 |
| Reference | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|
| García-Esperón 2021 [15] | CTP core/pen: 5.9% | CTP core/pen: 93.6% | CTP core/pen: 53.8% | CTP core/pen: 44.2% |
| CBV 2.5% | CBV 97.9% | CBV 60% | CBV 44.4% | |
| CBF 5.1% | CBF 97.9% | CBF 75% | CBF 45.1% | |
| MTT 39.8% | MTT 90.4% | MTT 83.9% | MTT 54.5% | |
| DT 33.9% | DT 91.5% | DT 83.9% | DT 52.4% | |
| Any positive map: 42.4% | Any positive map: 89.4% | Any positive map 83.3% | Any positive map: 55.3% | |
| Rudilosso 2015 [7] | 62.5% | 20% | ||
| Das, 2015 [16] | 9.3–42.5% | 91.9–95.3% | ||
| Benson 2016 [6] | All sites: 18.9% (CBV), 48.7% (TTP) CSWM 65.2% PWM: 12.5–37.5% BGT: 0% | All sites: 97.4% (CBF-TTP), 98.7% (CBV-MTT) | 81.8% (CBF), 92.9% (MTT) | 71.4% (CBV), 80% (TTP) |
| Lin 2009 [9] | 15.4% | 100% | 100% | 82.5% |
| Eckert 2011 [17] | 0% | 100% | 0% | 100% |
| Hana 2014 [18] | 0% | 100% | 0% | 100% |
| Cao 2016 [14] | MTT 56% Tmax 25% CBV 9% CBF 44% All maps 56% | All maps 100% | All maps 100% | All maps: 68% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zedde, M.; Napoli, M.; Grisendi, I.; Assenza, F.; Moratti, C.; Valzania, F.; Pascarella, R. CT Perfusion in Lacunar Stroke: A Systematic Review. Diagnostics 2023, 13, 1564. https://doi.org/10.3390/diagnostics13091564
Zedde M, Napoli M, Grisendi I, Assenza F, Moratti C, Valzania F, Pascarella R. CT Perfusion in Lacunar Stroke: A Systematic Review. Diagnostics. 2023; 13(9):1564. https://doi.org/10.3390/diagnostics13091564
Chicago/Turabian StyleZedde, Marialuisa, Manuela Napoli, Ilaria Grisendi, Federica Assenza, Claudio Moratti, Franco Valzania, and Rosario Pascarella. 2023. "CT Perfusion in Lacunar Stroke: A Systematic Review" Diagnostics 13, no. 9: 1564. https://doi.org/10.3390/diagnostics13091564
APA StyleZedde, M., Napoli, M., Grisendi, I., Assenza, F., Moratti, C., Valzania, F., & Pascarella, R. (2023). CT Perfusion in Lacunar Stroke: A Systematic Review. Diagnostics, 13(9), 1564. https://doi.org/10.3390/diagnostics13091564