
Diagnostic and Prognostic Nomograms for Hepatocellular Carcinoma Based on PIVKA-II and Serum Biomarkers

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Laboratory Methods
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients
3.2. AFP and PIVKA-II Distribution among Disease Groups
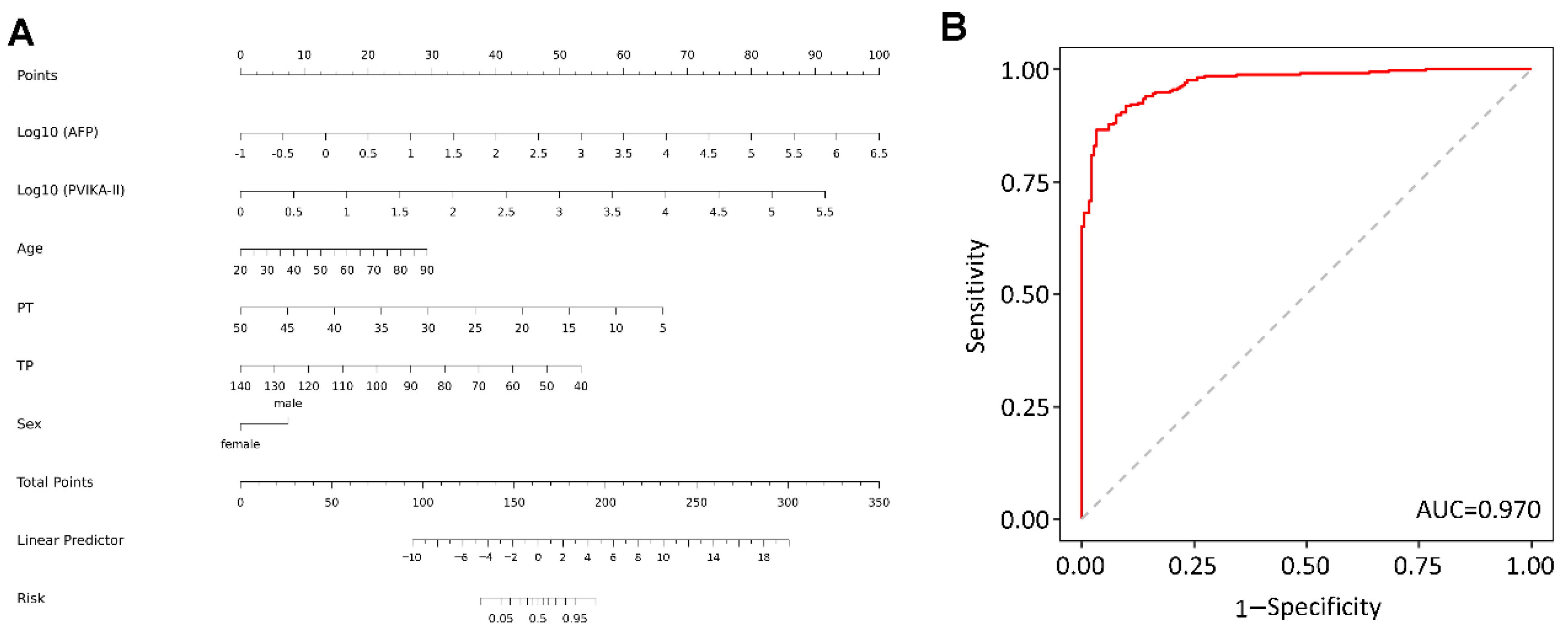
3.3. Diagnostic Factors of HCC Based on Logistic Regression
3.4. Clinical Characteristics of HCC Patients Enrolled in Survival Analysis
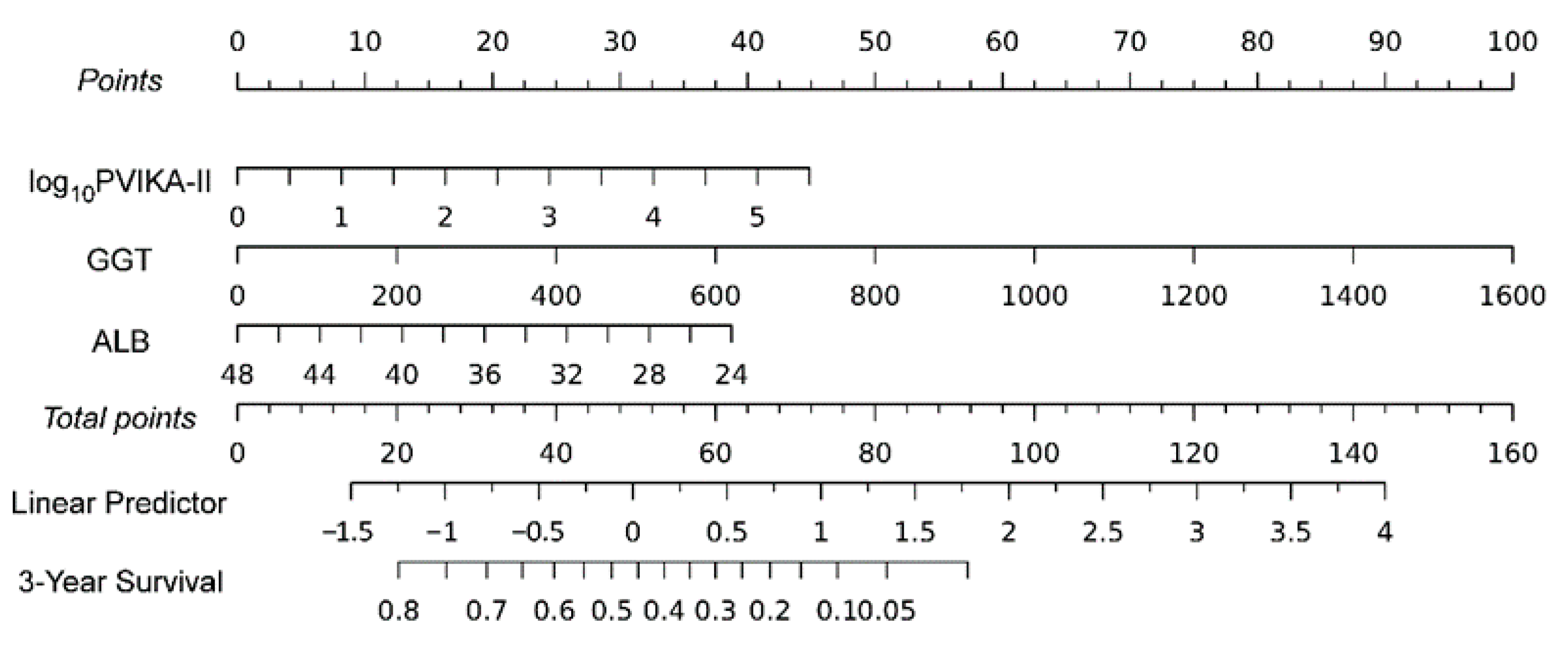
3.5. Predictive Potentials of Prognostic Nomogram
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Komuta, M. Histological Heterogeneity of Primary Liver Cancers: Clinical Relevance, Diagnostic Pitfalls and the Pathologist’s Role. Cancers 2021, 13, 2871. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Jiang, X.; Li, M.; Luo, Y. Hepatitis Virus and Hepatocellular Carcinoma: Recent Advances. Cancers 2023, 15, 533. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Huang, J.L.W.; George, J.; Huang, J.; Leung, C.; Eslam, M.; Chan, H.L.Y.; Ng, S.C. The changing epidemiology of liver diseases in the Asia-Pacific region. Nat. Rev. Gastroenterol. Hepatol 2019, 16, 57–73. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Lee, Y.T.; Fujiwara, N.; Yang, J.D.; Hoshida, Y. Risk stratification and early detection biomarkers for precision HCC screening. Hepatology 2022. [Google Scholar] [CrossRef]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 17–370. [Google Scholar] [CrossRef] [PubMed]
- Tzartzeva, K.; Obi, J.; Rich, N.E.; Parikh, N.D.; Marrero, J.A.; Yopp, A.; Waljee, A.K.; Singal, A.G. Surveillance Imaging and Alpha Fetoprotein for Early Detection of Hepatocellular Carcinoma in Patients With Cirrhosis: A Meta-analysis. Gastroenterology 2018, 154, 1706–1718.e1. [Google Scholar] [CrossRef]
- Goldberg, D.S.; Taddei, T.H.; Serper, M.; Mehta, R.; Dieperink, E.; Aytaman, A.; Baytarian, M.; Fox, R.; Hunt, K.; Pedrosa, M.; et al. Identifying barriers to hepatocellular carcinoma surveillance in a national sample of patients with cirrhosis. Hepatology 2017, 65, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.A.; Seock, C.H.; Park, J.W.; An, J.; Lee, K.S.; Yang, J.E.; Lim, Y.S.; Kim, K.M.; Shim, J.H.; Lee, D.; et al. Reappraisal of serum alpha-foetoprotein as a surveillance test for hepatocellular carcinoma during entecavir treatment. Liver Int. 2015, 35, 232–239. [Google Scholar] [CrossRef]
- Asrih, M.; Lenglet, S.; Mach, F.; Montecucco, F. Alpha-fetoprotein: A controversial prognostic biomarker for small hepatocellular carcinoma. World J. Gastroenterol. 2013, 19, 328–330. [Google Scholar] [CrossRef] [PubMed]
- Agopian, V.G.; Harlander-Locke, M.P.; Markovic, D.; Zarrinpar, A.; Kaldas, F.M.; Cheng, E.Y.; Yersiz, H.; Farmer, D.G.; Hiatt, J.R.; Busuttil, R.W. Evaluation of Patients With Hepatocellular Carcinomas That Do Not Produce alpha-Fetoprotein. JAMA Surg. 2017, 152, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, N.; Sawada, Y.; Endo, I.; Saito, K.; Uemura, Y.; Nakatsura, T. Biomarkers for the early diagnosis of hepatocellular carcinoma. World J. Gastroenterol. 2015, 21, 10573–10583. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Toan, B.N.; Tan, C.K.; Hasan, I.; Setiawan, L.; Yu, M.L.; Izumi, N.; Huyen, N.N.; Chow, P.K.; Mohamed, R.; et al. Utility of Combining PIVKA-II and AFP in the Surveillance and Monitoring of Hepatocellular Carcinoma in the Asia-Pacific Region. Clin. Mol. Hepatol. 2023, 29, 277–292. [Google Scholar] [CrossRef]
- Trevisani, F.; Garuti, F.; Neri, A. Alpha-fetoprotein for Diagnosis, Prognosis, and Transplant Selection. Semin Liver. Dis. 2019, 39, 163–177. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.L.; Tan, Q.W.; Gao, X.H.; Wu, J.; Guo, W. Elevated PIVKA-II is associated with early recurrence and poor prognosis in BCLC 0-A hepatocellular carcinomas. Asian Pac. J. Cancer Prev. 2014, 15, 6673–6678. [Google Scholar] [CrossRef]
- Pote, N.; Cauchy, F.; Albuquerque, M.; Voitot, H.; Belghiti, J.; Castera, L.; Puy, H.; Bedossa, P.; Paradis, V. Performance of PIVKA-II for early hepatocellular carcinoma diagnosis and prediction of microvascular invasion. J. Hepatol. 2015, 62, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Xiang, Z.; Bai, L.; He, L.; Tan, L.; Hu, M.; Ren, Y. Diagnostic value of serum PIVKA-II levels for BCLC early hepatocellular carcinoma and correlation with HBV DNA. Cancer Biomark. 2018, 23, 235–242. [Google Scholar] [CrossRef]
- Yang, Y.; Li, G.; Lu, Z.; Liu, Y.; Kong, J.; Liu, J. Progression of Prothrombin Induced by Vitamin K Absence-II in Hepatocellular Carcinoma. Front Oncol. 2021, 11, 726213. [Google Scholar] [CrossRef]
- Si, Y.Q.; Wang, X.Q.; Fan, G.; Wang, C.Y.; Zheng, Y.W.; Song, X.; Pan, C.C.; Chu, F.L.; Liu, Z.F.; Lu, B.R.; et al. Value of AFP and PIVKA-II in diagnosis of HBV-related hepatocellular carcinoma and prediction of vascular invasion and tumor differentiation. Infect. Agents Cancer 2020, 15, 70. [Google Scholar] [CrossRef]
- Seo, S.I.; Kim, H.S.; Kim, W.J.; Shin, W.G.; Kim, D.J.; Kim, K.H.; Jang, M.K.; Lee, J.H.; Kim, J.S.; Kim, H.Y.; et al. Diagnostic value of PIVKA-II and alpha-fetoprotein in hepatitis B virus-associated hepatocellular carcinoma. World J. Gastroenterol. 2015, 21, 3928–3935. [Google Scholar] [CrossRef] [PubMed]
- Strople, J.; Lovell, G.; Heubi, J. Prevalence of subclinical vitamin K deficiency in cholestatic liver disease. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 78–84. [Google Scholar] [CrossRef]
- Chen, J.; Wu, G.; Li, Y. Evaluation of Serum Des-Gamma-Carboxy Prothrombin for the Diagnosis of Hepatitis B Virus-Related Hepatocellular Carcinoma: A Meta-Analysis. Dis. Markers 2018, 2018, 8906023. [Google Scholar] [CrossRef]
- Yang, J.G.; He, X.F.; Huang, B.; Zhang, H.A.; He, Y.K. Rule of changes in serum GGT levels and GGT/ALT and AST/ALT ratios in primary hepatic carcinoma patients with different AFP levels. Cancer Biomark 2018, 21, 743–746. [Google Scholar] [CrossRef]
- Zhang, C.H.; Ni, X.C.; Chen, B.Y.; Qiu, S.J.; Zhu, Y.M.; Luo, M. Combined preoperative albumin-bilirubin (ALBI) and serum gamma-glutamyl transpeptidase (GGT) predicts the outcome of hepatocellular carcinoma patients following hepatic resection. J. Cancer 2019, 10, 4836–4845. [Google Scholar] [CrossRef] [PubMed]
- Bagirsakci, E.; Sahin, E.; Atabey, N.; Erdal, E.; Guerra, V.; Carr, B.I. Role of Albumin in Growth Inhibition in Hepatocellular Carcinoma. Oncology 2017, 93, 136–142. [Google Scholar] [CrossRef]
- Xia, F.; Ndhlovu, E.; Liu, Z.; Chen, X.; Zhang, B.; Zhu, P. Alpha-Fetoprotein+Alkaline Phosphatase (A-A) Score Can Predict the Prognosis of Patients with Ruptured Hepatocellular Carcinoma Underwent Hepatectomy. Dis. Markers 2022, 2022, 9934189. [Google Scholar] [CrossRef] [PubMed]
- Mao, M.; Wang, X.; Song, Y.; Sheng, H.; Han, R.; Lin, W.; Dai, S. Novel Prognostic Scores Based on Plasma Prothrombin Time and Fibrinogen Levels in Patients With AFP-Negative Hepatocellular Carcinoma. Cancer Control 2020, 27, 1073274820915520. [Google Scholar] [CrossRef]
- Haruki, K.; Shiba, H.; Saito, N.; Horiuchi, T.; Shirai, Y.; Fujiwara, Y.; Furukawa, K.; Sakamoto, T.; Yanaga, K. Risk stratification using a novel liver functional reserve score of combination prothrombin time-international normalized ratio to albumin ratio and albumin in patients with hepatocellular carcinoma. Surgery 2018, 164, 404–410. [Google Scholar] [CrossRef]
- Schuppan, D.; Afdhal, N.H. Liver cirrhosis. Lancet 2008, 371, 838–851. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Xing, H.; Wang, G.; Wang, N.; Liu, M.; Yan, C.; Li, H.; Wei, L.; Li, S.; Fan, Z.; et al. A Novel Online Calculator Based on Serum Biomarkers to Detect Hepatocellular Carcinoma among Patients with Hepatitis B. Clin Chem. 2019, 65, 1543–1553. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]
- Park, H.; Park, J.Y. Clinical significance of AFP and PIVKA-II responses for monitoring treatment outcomes and predicting prognosis in patients with hepatocellular carcinoma. Biomed Res. Int. 2013, 2013, 310427. [Google Scholar] [CrossRef] [PubMed]
- Viggiani, V.; Palombi, S.; Gennarini, G.; D’Ettorre, G.; De Vito, C.; Angeloni, A.; Frati, L.; Anastasi, E. Protein induced by vitamin K absence or antagonist-II (PIVKA-II) specifically increased in Italian hepatocellular carcinoma patients. Scand. J. Gastroenterol. 2016, 51, 1257–1262. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers. 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.; Li, B.; Li, Z.; Wei, Q.; Ren, L. PIVKA-II serves as a potential biomarker that complements AFP for the diagnosis of hepatocellular carcinoma. BMC Cancer 2021, 21, 401. [Google Scholar] [CrossRef]
- Shahini, E.; Pasculli, G.; Solimando, A.G.; Tiribelli, C.; Cozzolongo, R.; Giannelli, G. Updating the Clinical Application of Blood Biomarkers and Their Algorithms in the Diagnosis and Surveillance of Hepatocellular Carcinoma: A Critical Review. Int. J. Mol. Sci. 2023, 24, 4286. [Google Scholar] [CrossRef]
- Tas, F.; Kilic, L.; Serilmez, M.; Keskin, S.; Sen, F.; Duranyildiz, D. Clinical and prognostic significance of coagulation assays in lung cancer. Respir. Med. 2013, 107, 451–457. [Google Scholar] [CrossRef]
- Wang, X.P.; Mao, M.J.; He, Z.L.; Zhang, L.; Chi, P.D.; Su, J.R.; Dai, S.Q.; Liu, W.L. A retrospective discussion of the prognostic value of combining prothrombin time(PT) and fibrinogen(Fbg) in patients with Hepatocellular carcinoma. J. Cancer 2017, 8, 2079–2087. [Google Scholar] [CrossRef]
- Bian, Z.; Meng, J.; Niu, Q.; Jin, X.; Wang, J.; Feng, X.; Che, H.; Zhou, J.; Zhang, L.; Zhang, M.; et al. Prognostic Role of Prothrombin Time Activity, Prothrombin Time, Albumin/Globulin Ratio, Platelets, Sex, and Fibrinogen in Predicting Recurrence-Free Survival Time of Renal Cancer. Cancer Manag. Res. 2020, 12, 8481–8490. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fabrega, J.; Burrel, M.; Garcia-Criado, A.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Toyoda, H.; Tada, T.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2016, 31, 1031–1036. [Google Scholar] [CrossRef]
- Demirtas, C.O.; D’Alessio, A.; Rimassa, L.; Sharma, R.; Pinato, D.J. ALBI grade: Evidence for an improved model for liver functional estimation in patients with hepatocellular carcinoma. JHEP Rep. 2021, 3, 100347. [Google Scholar] [CrossRef]
- Zhang, J.; Zhao, L.; Zhou, Y.; Ding, J.; Zhang, Q.; Jing, X. The comparison between albumin-bilirubin grade and Child-Pugh grade for assessing the prognosis of hepatocellular carcinoma after thermal ablation: A propensity score-matched analysis. Transl. Cancer Res. 2022, 11, 2523–2535. [Google Scholar] [CrossRef]
- Huang, F.; Gao, J. Modified Child-Pugh grade vs albumin-bilirubin grade for predicting prognosis of hepatocellular carcinoma patients after hepatectomy. World J. Gastroenterol. 2020, 26, 749–758. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.H.; Kim, J.H.; Kang, S.H.; Lee, B.J.; Seo, Y.S.; Yim, H.J.; Yeon, J.E.; Park, J.J.; Kim, J.S.; Bak, Y.T.; et al. The influence of alcoholic liver disease on serum PIVKA-II levels in patients without hepatocellular carcinoma. Gut. Liver 2015, 9, 224–230. [Google Scholar] [CrossRef]
- Wang, X.; Mao, M.; He, Z.; Zhang, L.; Li, H.; Lin, J.; He, Y.; Dai, S.; Hu, W.; Liu, W. Development and Validation of a Prognostic Nomogram in AFP-negative hepatocellular carcinoma. Int. J. Biol. Sci. 2019, 15, 221–228. [Google Scholar] [CrossRef]
- Li, S.; Xu, W.; Liao, M.; Zhou, Y.; Weng, J.; Ren, L.; Yu, J.; Liao, W.; Huang, Z. The Significance of Gamma-Glutamyl Transpeptidase to Lymphocyte Count Ratio in the Early Postoperative Recurrence Monitoring and Prognosis Prediction of AFP-Negative Hepatocellular Carcinoma. J. Hepatocell Carcinoma. 2021, 8, 23–33. [Google Scholar] [CrossRef]
- Wu, S.J.; Lin, Y.X.; Ye, H.; Xiong, X.Z.; Li, F.Y.; Cheng, N.S. Prognostic value of alkaline phosphatase, gamma-glutamyl transpeptidase and lactate dehydrogenase in hepatocellular carcinoma patients treated with liver resection. Int. J. Surg. 2016, 36, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.S.; Wan, Y.; Song, S.D.; Chen, W.; Miao, R.C.; Zhou, Y.Y.; Zhang, L.Q.; Qu, K.; Liu, S.N.; Zhang, Y.L.; et al. Model based on gamma-glutamyltransferase and alkaline phosphatase for hepatocellular carcinoma prognosis. World J. Gastroenterol. 2014, 20, 10944–10952. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Chon, C.Y.; Han, K.H.; Seong, J. Clinical usefulness of double biomarkers AFP and PIVKA-II for subdividing prognostic groups in locally advanced hepatocellular carcinoma. Liver Int. 2014, 34, 313–321. [Google Scholar] [CrossRef]
- Wang, J.C.; Hou, J.Y.; Chen, J.C.; Xiang, C.L.; Mao, X.H.; Yang, B.; Li, Q.; Liu, Q.B.; Chen, J.; Ye, Z.W.; et al. Development and validation of prognostic nomograms for single large and huge hepatocellular carcinoma after curative resection. Eur. J. Cancer 2021, 155, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.H.; Liu, Q.B.; Xiang, C.L.; Mao, X.H.; Yang, B.; Li, Q.; Zhou, Q.F.; Li, S.Q.; Zhou, Z.G.; Chen, M.S. Multi-institutional validation of novel models for predicting the prognosis of patients with huge hepatocellular carcinoma. Int. J. Cancer 2021, 149, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.W.; Li, Q.F.; Chen, Y.Y.; Wang, K.; Pu, D.; Chen, X.R.; Li, C.H.; Jiang, L.; Wang, Y.; Li, Q.; et al. Clinicopathologic features, treatment, survival, and prognostic factors of combined hepatocellular and cholangiocarcinoma: A nomogram development based on SEER database and validation in multicenter study. Eur. J. Surg. Oncol. 2022, 48, 1559–1566. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | HCC (N = 352) | Liver Cirrhosis (N = 102) | HBV (N = 124) | Healthy Subjects (N = 127) |
|---|---|---|---|---|
| Age, years mean (SD) | 54 (11.8) | 55.7 (12.7) | 36.3 (10.8) | 50.1 (10.7) |
| Gender, n (%) | ||||
| Male | 309 (87.8%) | 67 (65.7%) | 83 (66.9%) | 69 (54.3%) |
| Female | 43 (12.2%) | 35 (34.3%) | 41 (33.1%) | 58 (45.7%) |
| AST (U/L) mean (SD) | 92.2 (135.2) | 79.2 (91.9) | 40.0 (59.5) | 24.1 (6.1) |
| ALT (U/L) mean (SD) | 79.4 (190.2) | 52.1 (56.5) | 45.5 (120.8) | 24.0 (13.6) |
| TBIL, μmol/L mean (SD) | 32.5 (57.0) | 60.7 (96.2) | 17.0 (14.5) | 12.4 (3.9) |
| ALB (g/L) mean (SD) | 36.3 (5.4) | 32.7 (6.6) | 45.6 (3.0) | 44.5 (3.8) |
| TP (g/L) mean (SD) | 66.5 (8.5) | 66.2 (9.0) | 75.4 (4.7) | 73.1 (4.8) |
| PLT (×109/L) mean (SD) | 174.3 (90.3) | 124.2 (87.8) | 214.5 (47.9) | 244.6 (53.8) |
| Hb (g/L) mean (SD) | 129.5 (23.6) | 106.7 (27.4) | 145.2 (16.7) | 146.1 (14.8) |
| PT, s mean (SD) | 13.2 (2.8) | 15.7 (4.5) | 12.8 (2.0) | 13.0 (1.1) |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age | 1.052 (1.037–1.066) | <0.001 | 1.082 (1.05–1.116) | <0.001 |
| Gender (male) | 3.641 (2.388–5.551) | <0.001 | 2.662 (1.159–6.117) | 0.021 |
| Log10AFP | 6.572 (4.515–9.566) | <0.001 | 8.291 (4.366–15.743) | <0.001 |
| Log10PVIKA-II | 17.056 (9.366–31.059) | <0.001 | 12.231 (5.853–25.559) | <0.001 |
| AST | 1.004 (1.002–1.007) | 0.001 | 0.996 (0.989–1.004) | 0.339 |
| ALT | 1.004 (1.001–1.006) | 0.01 | 1.009 (0.999–1.019) | 0.078 |
| TBIL | 0.999 (0.996–1.002) | 0.426 | ||
| ALB | 0.923 (0.899–0.948) | <0.001 | 1.073 (0.998–1.153) | 0.056 |
| TP | 0.933 (0.912–0.954) | <0.001 | 0.912 (0.871–0.954) | <0.001 |
| PLT | 1.00 (0.998–1.002) | 0.968 | ||
| Hb | 1.002 (0.996–1.009) | 0.487 | ||
| PT | 0.918 (0.862–0.977) | 0.007 | 0.839 (0.752–0.935) | 0.002 |
| Parameters | Survivor (n = 135) | Non-Survivor (n = 106) | p Value |
|---|---|---|---|
| Age (years) Median (IQR) | 55.0 (48.0–63.0) | 54.5 (48–65.0) | 0.730 a |
| Gender Male (%) | 117 (86.7%) | 93 (87.7%) | 0.806 b |
| Child-Pugh grade Number (%) | <0.001 b | ||
| A | 120 (88.9%) | 69 (65.1%) | |
| B | 15 (11.1%) | 37 (34.9%) | |
| BCLC stage Number (%) | 0.092 b | ||
| A | 26 (19.3%) | 19 (17.9%) | |
| B | 81 (60.0%) | 52 (49.1%) | |
| C | 28 (20.7%) | 35 (33.0%) | |
| HBsAg Positive (%) | 108 (80.0%) | 86 (81.1%) | 0.826 b |
| AFP (mg/mL) Median (IQR) | 49.8 (8.3–719.0) | 92.9 (8.5–8406.2) | 0.099 a |
| PVIKA-II (mAU/mL) Median (IQR) | 296.6 (61.0–1725.3) | 1626.3 (123.2–10833.8) | <0.001 a |
| CEA (mg/mL) Median (IQR) | 2.8 (1.5–4.2) | 2.6 (1.7–4.2) | 0.948 a |
| CA199 (mg/mL) Median (IQR) | 7.4 (4.1–14.0) | 12.5 (5.6–31.8) | 0.001 a |
| WBC (×109/L) Median (IQR) | 7.2 (5.1–10.2) | 7.7 (5.5–9.5) | 0.858 a |
| LY (×109/L) Median (IQR) | 1.1 (0.8–1.6) | 1.0 (0.7–1.5) | 0.240 a |
| NET (×109/L) Median (IQR) | 5.0 (3.4–7.9) | 5.0 (3.1–7.8) | 0.918 a |
| NLR Median (IQR) | 4.5 (2.7–8.4) | 4.6 (2.7–8.9) | 0.577 a |
| RBC (×109/L) Median (IQR) | 4.0 (3.4–4.4) | 4.1 (3.4–4.5) | 0.230 a |
| Hb (g/L) Median (IQR) | 131.0 (117.0–145.5) | 130.0 (113.3–142.0) | 0.460 a |
| RDW (%) Median (IQR) | 13.5 (13.0–14.0) | 14.0 (13.0–15.2) | 0.049 a |
| PLT (×109/L) Median (IQR) | 166.0 (113.0–223.0) | 163.5 (99.5–243.3) | 0.913 a |
| MPV (fL) Median (IQR) | 10.0 (9.2–11.1) | 10.0 (9.2–10.8) | 0.686 a |
| ALT (U/L) Median (IQR) | 39.0 (24.0–66.5) | 45.0 (32.0–65.8) | 0.109 a |
| AST (U/L) Median (IQR) | 39.0 (29.0–64.0) | 56.5 (37.5–98.5) | <0.001 a |
| GGT Median (IQR) | 64.5 (39.2–112.7) | 138.5 (72.7–242.7) | <0.001 a |
| LDH Median (IQR) | 228.5 (195.5–298.0) | 250.5 (206.2–345.5) | 0.072 a |
| TBIL (µmol/L) Median (IQR) | 16.4 (12.5–24.8) | 19.7 (14.1–34.9) | 0.004 a |
| DBIL (µmol/L) Median (IQR) | 3.8 (2.5–6.8) | 5.5 (3.2–12.9) | 0.002 a |
| ALB (g/L) Median (IQR) | 37.0 (34.8–40.7) | 35.2 (31.7–39.0) | 0.002 a |
| TP (g/L) Median (IQR) | 66.2 (61.3–71.2) | 66.9 (61.2–71.6) | 0.630 a |
| Cr (µmol/L) Median (IQR) | 71.0 (60.0–81.0) | 67.0 (56.0–79.0) | 0.114 a |
| PT (s) Median (IQR) | 12.4 (11.8–13.1) | 12.8 (12.1–14.2) | 0.004 a |
| INR Median (IQR) | 1.1 (1.1–1.2) | 1.1 (1.0–1.2) | 0.949 a |
| APTT (s) Median (IQR) | 29.2 (27.2–33.4) | 30.8 (27.6–35.6) | 0.066 a |
| TT (s) Median (IQR) | 18.3 (17.5–19.1) | 17.9 (17.2–19.1) | 0.316 a |
| FIB (g/L) Median (IQR) | 2.6 (2.1–3.4) | 3.1 (2.1–4.0) | 0.035 a |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Log10PVIKA-II | 1.573 (1.263–1.958) | <0.001 | 1.347 (1.053–1.724) | 0.018 |
| GGT | 1.005 (1.002–1.008) | <0.001 | 1.002 (1.001–1.003) | 0.002 |
| CA199 | 1.004 (1.002–1.006) | <0.001 | 1.001 (0.998–1.004) | 0.395 |
| AST | 1.001 (1.000–1.002) | 0.07 | ||
| TBIL | 1.007 (1.003–1.012) | 0.002 | 1.001 (0.994–1.009) | 0.763 |
| DBIL | 1.012 (1.005–1.018) | 0.001 | 1.007 (0.999–1.016) | 0.263 |
| ALB | 0.924 (0.884–0.966) | <0.001 | 0.932 (0.888–0.979) | 0.005 |
| PT | 1.082 (0.985–1.188) | 0.102 | ||
| FIB | 1.22 (1.032–1.443) | 0.02 | 1.121 (0.918–1.368) | 0.263 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
An, S.; Zhan, X.; Liu, M.; Li, L.; Wu, J. Diagnostic and Prognostic Nomograms for Hepatocellular Carcinoma Based on PIVKA-II and Serum Biomarkers. Diagnostics 2023, 13, 1442. https://doi.org/10.3390/diagnostics13081442
An S, Zhan X, Liu M, Li L, Wu J. Diagnostic and Prognostic Nomograms for Hepatocellular Carcinoma Based on PIVKA-II and Serum Biomarkers. Diagnostics. 2023; 13(8):1442. https://doi.org/10.3390/diagnostics13081442
Chicago/Turabian StyleAn, Shu, Xiaoxia Zhan, Min Liu, Laisheng Li, and Jian Wu. 2023. "Diagnostic and Prognostic Nomograms for Hepatocellular Carcinoma Based on PIVKA-II and Serum Biomarkers" Diagnostics 13, no. 8: 1442. https://doi.org/10.3390/diagnostics13081442
APA StyleAn, S., Zhan, X., Liu, M., Li, L., & Wu, J. (2023). Diagnostic and Prognostic Nomograms for Hepatocellular Carcinoma Based on PIVKA-II and Serum Biomarkers. Diagnostics, 13(8), 1442. https://doi.org/10.3390/diagnostics13081442