
Biophysical Changes of Leukocyte Activation (and NETosis) in the Cellular Host Response to Sepsis
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. In Vitro Experiments
2.1.1. Reagents and Solutions
2.1.2. PMA Assays
2.2. Clinical Studies
Study Population
2.3. IntelliSep Test and Results
2.4. Quantification of NET Content
2.5. Statistical Analysis
3. Results
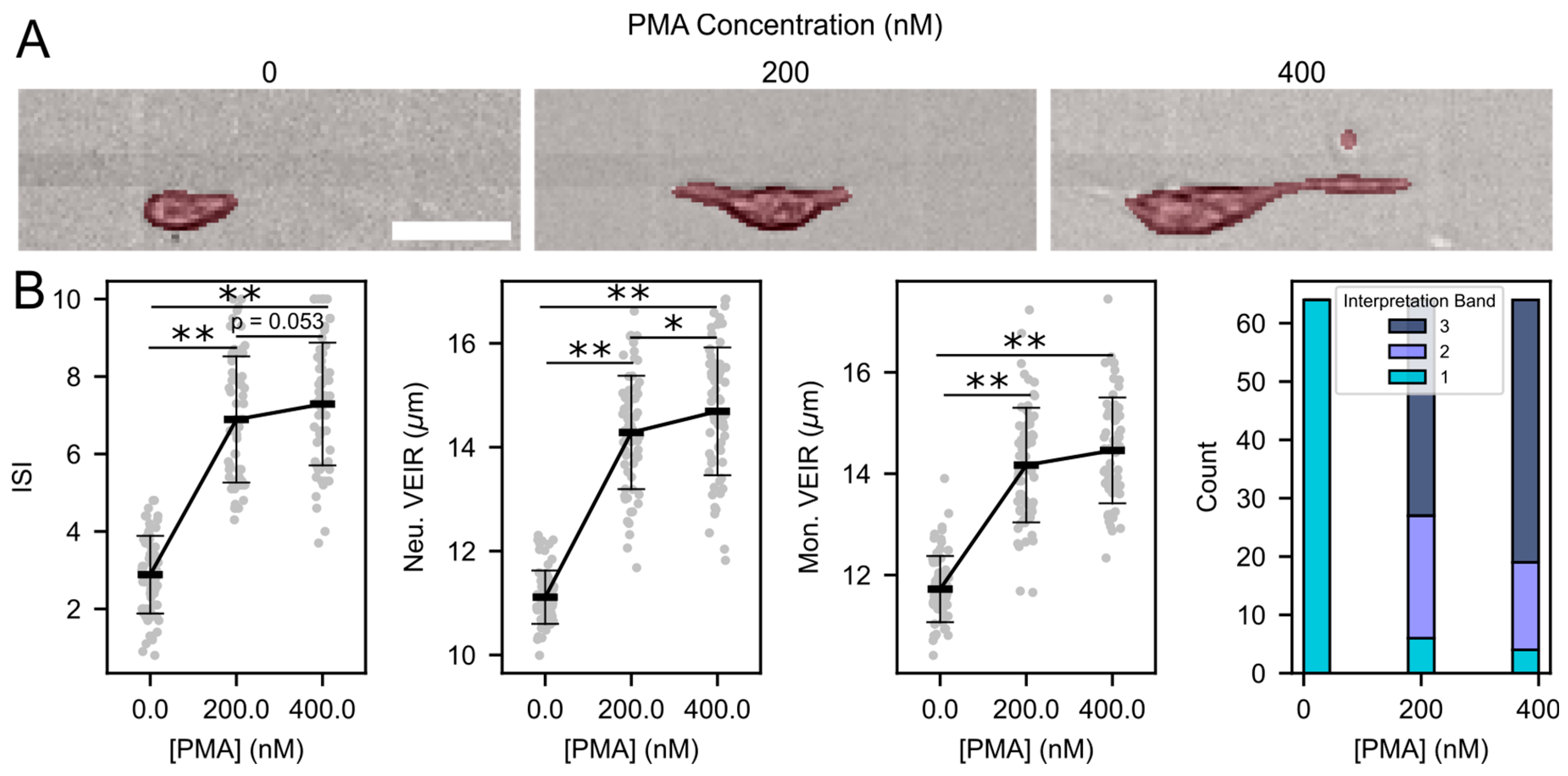
3.1. Activation of Neutrophil and Monocytes through PMA Is Detected through IntelliSep Measurements
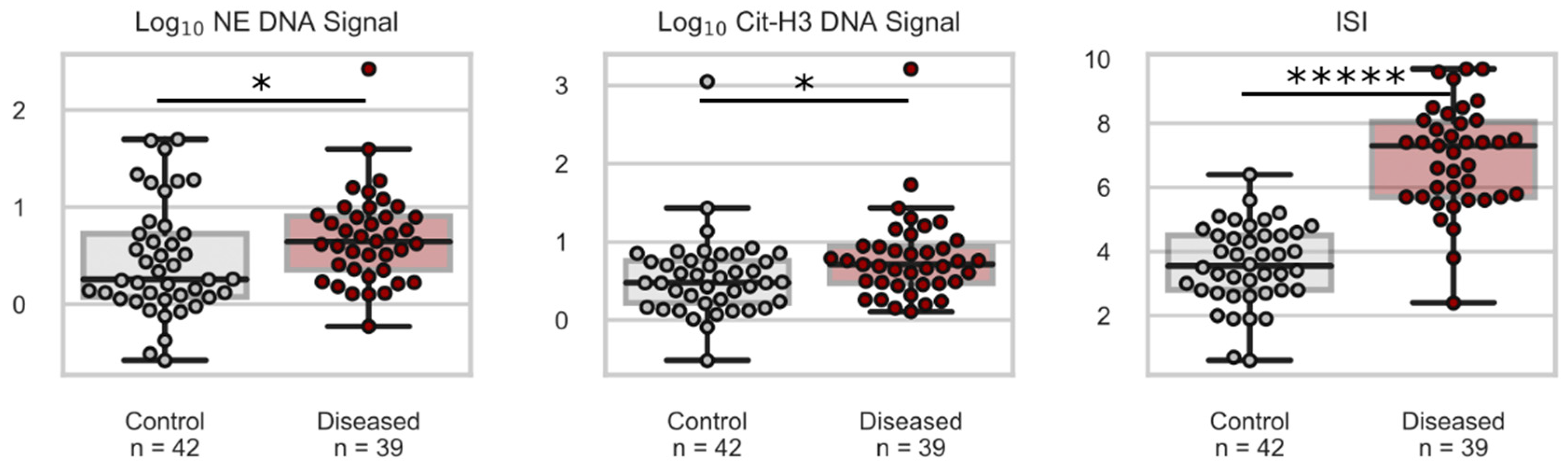
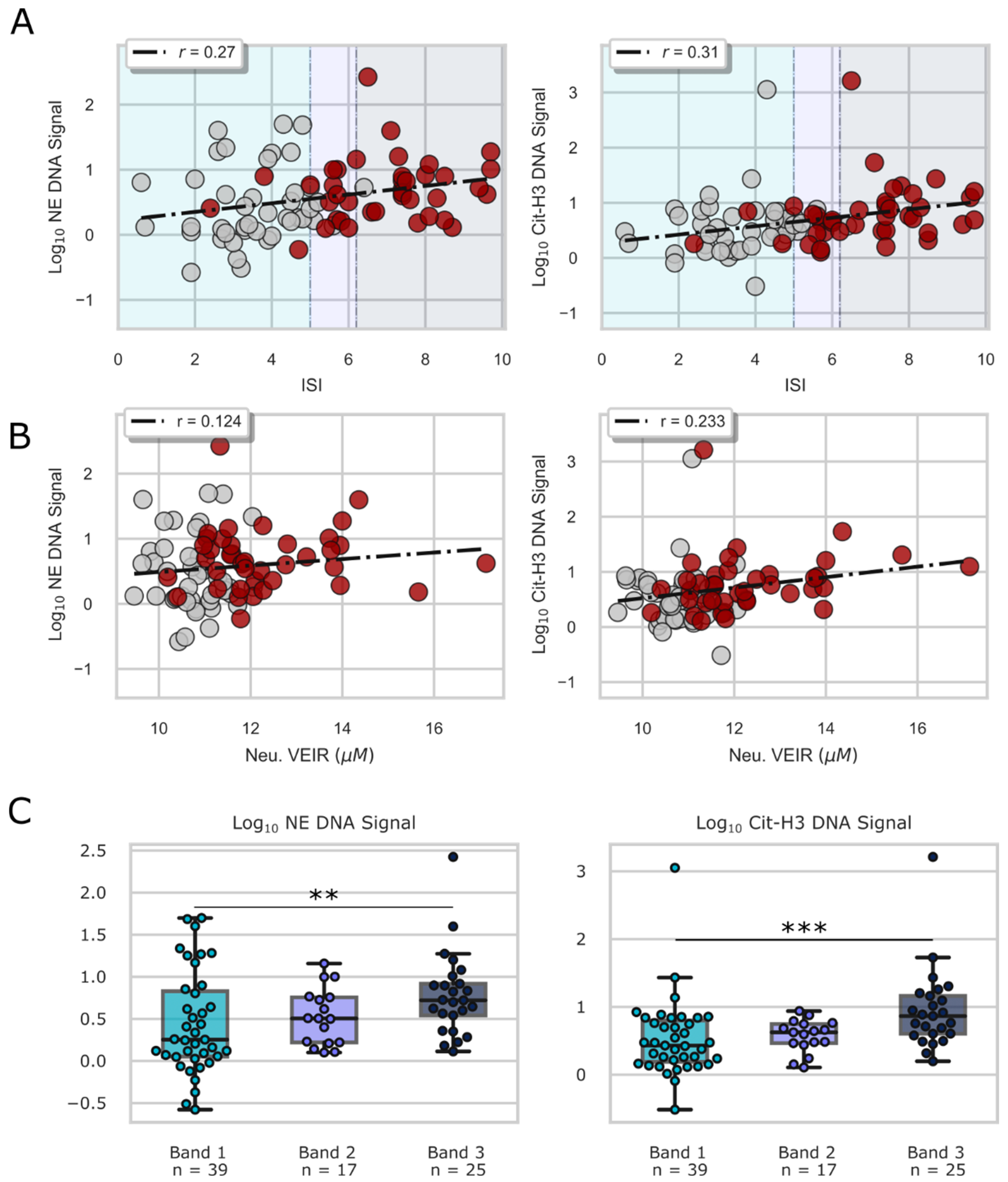
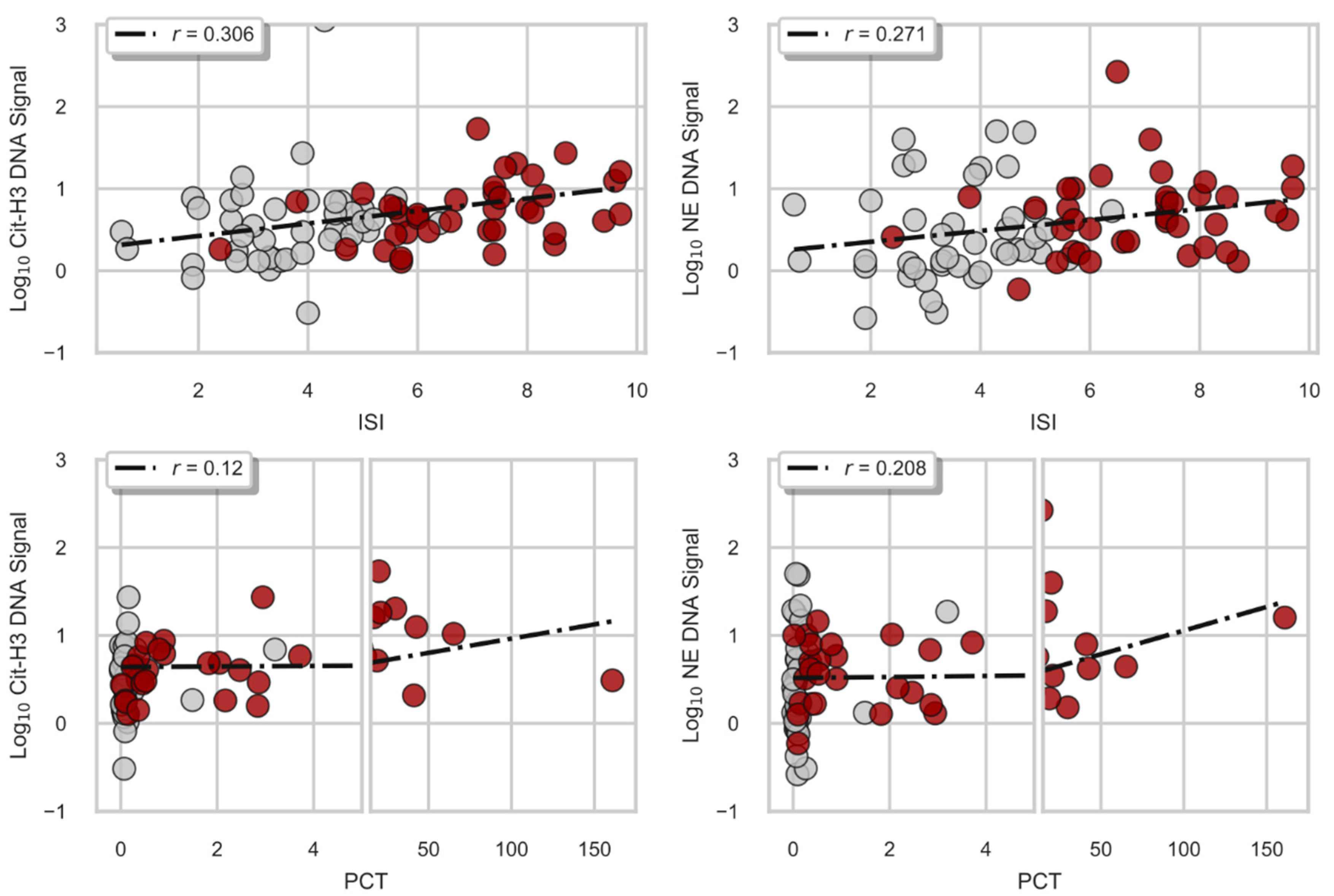
3.2. Quantity of NETs in Patient Samples Is Correlated with Sepsis and IntelliSep Index Measurements
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tavaré, A.; O’Flynn, N. Recognition, diagnosis, and early management of sepsis: NICE guideline. Br. J. Gen. Pr. 2017, 67, 185–186. [Google Scholar] [CrossRef]
- Paoli, C.J.; Reynolds, M.A.; Sinha, M.; Gitlin, M.; Crouser, E. Epidemiology and Costs of Sepsis in the United States—An Analysis Based on Timing of Diagnosis and Severity Level*. Crit. Care Med. 2018, 46, 1889–1897. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration C for DE and R. IntelliSep Test 21 CFR 866.3215 Approval Letter. 2022. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf22/K220991.pdf (accessed on 14 March 2023).
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Cinel, I.; Opal, S.M. Molecular biology of inflammation and sepsis: A primer. Crit. Care Med. 2009, 37, 291–304. [Google Scholar] [CrossRef]
- O’Brien, J.M.; Ali, N.A.; Aberegg, S.K.; Abraham, E. Sepsis. Am. J. Med. 2007, 120, 1012–1022. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Moldawer, L.L.; Opal, S.M.; Reinhart, K.; Turnbull, I.R.; Vincent, J.-L. Sepsis and septic shock. Nat. Rev. Dis. Prim. 2016, 2, 16045. [Google Scholar] [CrossRef] [PubMed]
- SSeymour, C.W.; Liu, V.X.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; Deutschman, C.S.; Escobar, G.J.; Angus, D.C.; Iwashyna, T.J.; Brunkhorst, F.M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef]
- Hidalgo, A.; Chilvers, E.R.; Summers, C.; Koenderman, L. The Neutrophil Life Cycle. Trends Immunol. 2019, 40, 584–597. [Google Scholar] [CrossRef]
- Lambert, J.; Fernandez, N.; Roy, M. Association of Presence of Band Cells and Toxic Neutrophils with Systemic Inflammatory Response Syndrome and Outcome in Horses with Acute Disease. J. Veter- Intern. Med. 2016, 30, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Silvestre-Roig, C.; Hidalgo, A.; Soehnlein, O. Neutrophil heterogeneity: Implications for homeostasis and pathogenesis. Blood 2016, 127, 2173–2181. [Google Scholar] [CrossRef] [PubMed]
- HHirsh, M.; Mahamid, E.; Bashenko, Y.; Hirsh, I.; Krausz, M.M. Overexpression of the High-affinity Fcγ Receptor (cd64) is Associated with Leukocyte Dysfunction in Sepsis. Shock 2001, 16, 102–108. [Google Scholar] [CrossRef]
- Lakschevitz, F.S.; Hassanpour, S.; Rubin, A.; Fine, N.; Sun, C.; Glogauer, M. Identification of neutrophil surface marker changes in health and inflammation using high-throughput screening flow cytometry. Exp. Cell Res. 2016, 342, 200–209. [Google Scholar] [CrossRef]
- Jundi, B.; Ryu, H.; Lee, D.-H.; Abdulnour, R.-E.E.; Engstrom, B.D.; Duvall, M.G.; Higuera, A.; Pinilla-Vera, M.; Benson, M.E.; Lee, J.; et al. Leukocyte function assessed via serial microlitre sampling of peripheral blood from sepsis patients correlates with disease severity. Nat. Biomed. Eng. 2019, 3, 961–973. [Google Scholar] [CrossRef]
- Sweeney, T.E.; Shidham, A.; Wong, H.R.; Khatri, P. A comprehensive time-course–based multicohort analysis of sepsis and sterile inflammation reveals a robust diagnostic gene set. Sci. Transl. Med. 2015, 7, 287ra71. [Google Scholar] [CrossRef]
- McHugh, L.; Seldon, T.A.; Brandon, R.A.; Kirk, J.T.; Rapisarda, A.; Sutherland, A.J.; Presneill, J.J.; Venter, D.J.; Lipman, J.; Thomas, M.R.; et al. A Molecular Host Response Assay to Discriminate Between Sepsis and Infection-Negative Systemic Inflammation in Critically Ill Patients: Discovery and Validation in Independent Cohorts. PLOS Med. 2015, 12, e1001916. [Google Scholar] [CrossRef]
- Mayadas, T.N.; Cullere, X.; Lowell, C.A. The Multifaceted Functions of Neutrophils. Annu. Rev. Pathol. Mech. Dis. 2014, 9, 181–218. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil extracellular traps kill bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef]
- Granger, V.; Faille, D.; Marani, V.; Noël, B.; Gallais, Y.; Szely, N.; Flament, H.; Pallardy, M.; Chollet-Martin, S.; de Chaisemartin, L. Human blood monocytes are able to form extracellular traps. J. Leukoc. Biol. 2017, 102, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Camicia, G.; Pozner, R.; de Larrañaga, G. Neutrophil Extracellular Traps in Sepsis. Shock 2014, 42, 286–294. [Google Scholar] [CrossRef]
- Allison, S.J. NET-induced coagulation induces organ damage in sepsis. Nat. Rev. Nephrol. 2017, 13, 133. [Google Scholar] [CrossRef]
- Denning, N.-L.; Aziz, M.; Gurien, S.D.; Wang, P. DAMPs and NETs in Sepsis. Front. Immunol. 2019, 10, 2536. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, X.; Pelayo, R.; Monestier, M.; Ammollo, C.T.; Semeraro, F.; Taylor, F.B.; Esmon, N.L.; Lupu, F.; Esmon, C.T. Extracellular histones are major mediators of death in sepsis. Nat. Med. 2009, 15, 1318–1321. [Google Scholar] [CrossRef]
- Li, Y.; Liu, B.; Fukudome, E.Y.; Lu, J.; Chong, W.; Jin, G.; Liu, Z.; Velmahos, G.C.; Demoya, M.; King, D.R.; et al. Identification of citrullinated histone H3 as a potential serum protein biomarker in a lethal model of lipopolysaccharide-induced shock. Surgery 2011, 150, 442–451. [Google Scholar] [CrossRef]
- Margraf, S.; Lögters, T.; Reipen, J.; Altrichter, J.; Scholz, M.; Windolf, J. Neutrophil-Derived Circulating Free DNA (cf-DNA/NETs): A Potential Prognostic Marker for Posttraumatic Development of Inflammatory Second Hit and sepsis. Shock 2008, 30, 352–358. [Google Scholar] [CrossRef]
- Manley, H.; Keightley, M.-C.; Lieschke, G.J. The Neutrophil Nucleus: An Important Influence on Neutrophil Migration and Function. Front. Immunol. 2018, 9, 2867. [Google Scholar] [CrossRef]
- TThiam, H.R.; Wong, S.L.; Wagner, D.D.; Waterman, C.M. Cellular Mechanisms of NETosis. Annu. Rev. Cell Dev. Biol. 2020, 36, 191–218. [Google Scholar] [CrossRef] [PubMed]
- Crawford, K.; DeWitt, A.; Brierre, S.; Caffery, T.; Jagneaux, T.; Thomas, C.; Macdonald, M.; Tse, H.; Shah, A.; Di Carlo, D.; et al. Rapid Biophysical Analysis of Host Immune Cell Variations Associated with Sepsis. Am. J. Respir. Crit. Care Med. 2018, 198, 280–282. [Google Scholar] [CrossRef]
- Guillou, L.; Sheybani, R.; Jensen, A.E.; Di Carlo, D.; Caffery, T.S.; Thomas, C.B.; Shah, A.M.; Tse, H.T.K.; Hollis, R.O., Jr. Development and validation of a cellular host response test as an early diagnostic for sepsis. PLoS ONE 2021, 16, e0246980. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, H.R.J.; Sheybani, R.; Caffery, T.S.; Musso, M.W.; Hamer, D.; Alwood, S.M.; Berlinger, M.S.; Jagneaux, T.; LaVie, K.W.; O’Neal, C.S.; et al. Assessment of a Cellular Host Response Test as a Sepsis Diagnostic for Those With Suspected Infection in the Emergency Department. Crit. Care Explor. 2021, 3, e0460. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, H.R., Jr.; Sheybani, R.; Caffery, T.S.; Hamer, D.; Laperouse, L.M.; Musso, M.W.; O’Neal, C.S.; Tse, H.T.K.; Shah, A.M.; Thomas, C.B. Assessment of a cellular host response test to risk-stratify suspected COVID-19 patients in the Emergency Department setting. PLoS ONE 2022, 17, e0264220. [Google Scholar] [CrossRef]
- Hedley, D.W.; Chow, S.; Shankey, T.V. Cytometry of Intracellular Signaling: From Laboratory Bench to Clinical Application. Methods in cell biol. 2011, 103, 203–220. [Google Scholar] [CrossRef]
- Hakkim, A.; Fuchs, T.A.; Martinez, N.E.; Hess, S.; Prinz, H.; Zychlinsky, A.; Waldmann, H. Activation of the Raf-MEK-ERK pathway is required for neutrophil extracellular trap formation. Nat. Chem. Biol. 2011, 7, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Lefrancais, E.; Mallavia, B.; Zhuo, H.; Calfee, C.S.; Looney, M.R. Maladaptive role of neutrophil extracellular traps in pathogen-induced lung injury. J. Clin. Investig. 2018, 3, e98178. [Google Scholar] [CrossRef] [PubMed]
- Meisner, M. Update on Procalcitonin Measurements. Ann. Lab. Med. 2014, 34, 263–273. [Google Scholar] [CrossRef]
- Sayah, D.M.; Mallavia, B.; Liu, F.; Ortiz-Muñoz, G.; Caudrillier, A.; DerHovanessian, A.; Ross, D.J.; Iii, J.P.L.; Saggar, R.; Ardehali, A.; et al. Neutrophil Extracellular Traps Are Pathogenic in Primary Graft Dysfunction after Lung Transplantation. Am. J. Respir. Crit. Care Med. 2015, 191, 455–463. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Abed, U.; Goosmann, C.; Hurwitz, R.; Schulze, I.; Wahn, V.; Weinrauch, Y.; Brinkmann, V.; Zychlinsky, A. Novel cell death program leads to neutrophil extracellular traps. J. Cell Biol. 2007, 176, 231–241. [Google Scholar] [CrossRef]
- Kibe, S.; Adams, K.; Barlow, G. Diagnostic and prognostic biomarkers of sepsis in critical care. J. Antimicrob. Chemother. 2011, 66, ii33–ii40. [Google Scholar] [CrossRef]
- Remijsen, Q.; Berghe, T.V.; Wirawan, E.; Asselbergh, B.; Parthoens, E.; De Rycke, R.; Noppen, S.; Delforge, M.; Willems, J.; Vandenabeele, P. Neutrophil extracellular trap cell death requires both autophagy and superoxide generation. Cell Res. 2011, 21, 290–304. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Total N = 81 | Control N = 42 | Diseased N = 39 | p Value | |
|---|---|---|---|---|---|
| Age | Median (Q1–Q3) | 58.00 (43.75–69.00) | 52.50 (34.00–66.25) | 62.00 (53.00–72.50) | p < 0.01 |
| Subjects ≥ 65 N (%) | 28 (34.57) | 11 (26.19) | 17 (43.59) | ns | |
| Biological Sex N (%) | Male | 39 (48.15) | 18 (42.86) | 21 (53.85) | ns |
| Female | 42 (51.85) | 24 (57.14) | 18 (46.15) | ns | |
| Race N (%) | Black | 28 (34.57) | 18 (42.86) | 10 (25.64) | ns |
| White | 50 (61.73) | 23 (54.76) | 27 (69.23) | ns | |
| Other | 3 (3.7) | 1 (2.38) | 2 (5.13) | ns | |
| Comorbidities N (%) | Hypertension | 18 (22.22) | 11 (26.19) | 7 (17.95) | ns |
| Diabetes | 7 (8.64) | 4 (9.52) | 3 (7.69) | ns | |
| Obesity | 9 (11.11) | 6 (14.29) | 3 (7.69) | ns | |
| Cancer | 4 (4.94) | 2 (4.76) | 2 (5.13) | ns | |
| Chronic Kidney Disease | 3 (3.7) | 2 (4.76) | 1 (2.56) | ns | |
| Autoimmune Disease | 3 (3.7) | 2 (4.76) | 1 (2.56) | ns | |
| Infected by adjudication N (%) | Yes | 39 (48.15) | 0 (0.0) | 39 (100.0) | p < 0.0001 |
| Septic, by Sepsis-3 definition N (%) | Yes | 39 (48.15) | 0 (0.0) | 39 (100.0) | p < 0.0001 |
| All-Cause Cumulative In-Hospital Mortality N (%) | 3-day | 0 (0.0) | 0 (0.0) | 0 (0.0) | ns |
| 7-day | 3 (3.7) | 0 (0.0) | 3 (7.69) | ns | |
| 30-day | 3 (3.7) | 0 (0.0) | 3 (7.69) | ns | |
| Admitted to Hospital N (%) | 57 (70.37) | 19 (45.24) | 38 (97.44) | p < 0.0001 | |
| Admitted to ICU N (%) | 11 (13.58) | 2 (4.76) | 9 (23.08) | p < 0.05 | |
| SOFA, 3-day max (baseline subtracted) Median (Q1–Q3) | 2.00 (0.00–4.00) | 0.00 (0.00–1.00) | 4.00 (3.00–6.00) | p < 0.0001 | |
| WBC (103 cells/µL), Median (Q1–Q3) | 13.16 (7.85–19.35) | 9.65 (5.70–13.46) | 17.30 (12.62–22.98) | p < 0.0001 | |
| Triage Temperature, Median (Q1–Q3) | 98.30 (97.90–99.12) | 98.20 (97.90–98.40) | 98.90 (98.10–101.00) | p < 0.0001 | |
| Lactate Measured, N (%) | 51 (62.96) | 14 (33.33) | 37 (94.87) | p < 0.0001 | |
| Lactate, Median (Q1–Q3) | 2.10 (1.30–3.65) | 1.80 (0.68–2.10) | 2.90 (1.40–5.10) | p < 0.05 | |
| IntelliSep Index, Median (Q1–Q3) | 5.00 (3.40–7.10) | 3.55 (2.80–4.50) | 7.30 (5.70–8.05) | p < 0.0001 | |
| Log10 Cit-H3 DNA Signal, Median (Q1–Q3) | 0.61 (0.32–0.85) | 0.48 (0.22–0.76) | 0.71 (0.47–0.94) | p < 0.05 | |
| Log10 NE-DNA Signal, Median (Q1–Q3) | 0.51 (0.16–0.90) | 0.26 (0.08–0.73) | 0.65 (0.35–0.91) | p < 0.05 | |
| PCT, Median (Q1–Q3) | 0.24 (0.08–2.32) | 0.08 (0.06–0.11) | 2.32 (0.46–13.56) | p < 0.01 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorrells, M.G.; Seo, Y.; Magnen, M.; Broussard, B.; Sheybani, R.; Shah, A.M.; O’Neal, H.R.; Tse, H.T.K., Jr.; Looney, M.R.; Di Carlo, D. Biophysical Changes of Leukocyte Activation (and NETosis) in the Cellular Host Response to Sepsis. Diagnostics 2023, 13, 1435. https://doi.org/10.3390/diagnostics13081435
Sorrells MG, Seo Y, Magnen M, Broussard B, Sheybani R, Shah AM, O’Neal HR, Tse HTK Jr., Looney MR, Di Carlo D. Biophysical Changes of Leukocyte Activation (and NETosis) in the Cellular Host Response to Sepsis. Diagnostics. 2023; 13(8):1435. https://doi.org/10.3390/diagnostics13081435
Chicago/Turabian StyleSorrells, Matt G., Yurim Seo, Melia Magnen, Bliss Broussard, Roya Sheybani, Ajay M. Shah, Hollis R. O’Neal, Henry T. K. Tse, Jr., Mark R. Looney, and Dino Di Carlo. 2023. "Biophysical Changes of Leukocyte Activation (and NETosis) in the Cellular Host Response to Sepsis" Diagnostics 13, no. 8: 1435. https://doi.org/10.3390/diagnostics13081435
APA StyleSorrells, M. G., Seo, Y., Magnen, M., Broussard, B., Sheybani, R., Shah, A. M., O’Neal, H. R., Tse, H. T. K., Jr., Looney, M. R., & Di Carlo, D. (2023). Biophysical Changes of Leukocyte Activation (and NETosis) in the Cellular Host Response to Sepsis. Diagnostics, 13(8), 1435. https://doi.org/10.3390/diagnostics13081435