
Fatty Acid Profile and Genetic Variants of Proteins Involved in Fatty Acid Metabolism Could Be Considered as Disease Predictor
 ,
,  ,
,
Abstract
1. Introduction
1.1. Different Fatty Acids in Plasma and Erythrocytes
1.2. Functions of Fatty Acids
2. Materials and Methods
3. Results and Discussion
3.1. Fatty Acids and Diseases
3.1.1. Fatty Acids and Cardiovascular Disease (CVD)
3.1.2. Fatty Acids and Diabetes (Table 2)
3.1.3. Fatty Acids and Cancer (Table 2)
3.1.4. Fatty Acids and Other Diseases (Table 2)

{kind=link}
{kind=link}
| Disease | Sample | Specific Fatty Acids | References |
|---|---|---|---|
| Cardiovascular diseases | Blood | Decreased n-6 PUFA | [35] |
| Cardiovascular disease | Blood | Increased SFA and trans FA | [36] |
| Cardiovascular risk | Serum | Increased MUFA Decreased n-6 PUFA and C22:6 n-3 (DHA) | [37] |
| Coronary artery disease | Red blood cells | Increased C26:0, C24:0, C22:0, C20:5 n-3 (EPA), C20:4 n-6 (AA) Decreased DHA, EPA/AA | [9] |
| Coronary artery disease | Plasma | Low levels of ALA, EPA, eicosatetraenoic (C20:4 n-3) and DHA | [38] |
| Coronary heart disease | Red blood cells | Increased Trans fatty acids | [26] |
| Coronary artery disease severity | Red Blood Cells and plasma | Increased Trans fatty acids | [30] |
| Heart Failure | Plasma | Decreased very long-chain saturated fatty acids arachidic acid (20:0), behenic acid (22:0) and lignoceric acid (24:0) | [29] |
| Acute myocardial infarction | Plasma | Decreased short-chain FA Increased long-chain FA | [31] |
| Acute coronary syndrome | Serum | Low DHA/AA | [32] |
| Early onset coronary atherosclerosis | RBC | Low EPA and DHA | [33] |
| Risk of atherosclerotic plaque rupture | serum | Increased AA/DHA | [34] |
| Type 2 diabetes | RBC | Elevated linolenic acid | [57] |
| Type 2 diabetes | Plasma | Increased palmitic, stearic and oleic acid | [55] |
| Type 2 diabetes | Plasma | Increased c9t11-CLA | [61] |
| Type 2 diabetes | Serum | Increased C22:6 | [50] |
| Type 2 diabetes | Plasma | Increased n-6/n-3 | [51] |
| Type 2 diabetes | Serum | EPA, C22:5 n-3 and DHA (inverse) | [59] |
| Cancer | RBC | Decreased SFA (C16:0 et C18:0) Increased MUFA (C18:1) Increased PUFA (LA and C20:3 n-6) | [65] |
| Oral cancer | RBC | Decreased EPA, DHA | [67] |
| Breast cancer | Plasma | Decreased linoleic acid (C18:2 n-6) | [72] |
| Pancreatic cancer | Plasma | Decreased n-3 PUFA and MUFA Increased AA | [68] |
| Hepatocellular carcinoma | Plasma | Very long-chain SFAs and very long-chain n-3 PUFAs (inverse) | [66] |
| Multiple myeloma | Red blood cell | Low n-3/n-6 PUFA ratio | [74] |
| Dementia | Red blood cells and plasma | Increased Hexacosanoic Acid (C26:0) | [7] |
| Dementia | Serum | ALA (inverse) | [78] |
| Alzheimer’s disease | Plasma and erythrocyte | Increased AA | [79] |
| Plasma | Decreased DHA | ||
| The indexes AA/Dihomo-gamma-linolenic acid and C24:4 n-6/Adrenic acid (AdA) were both higher | |||
| Alzheimer’s disease | Red blood cell | DHA (inverse) | [80] |
| Obesity | Serum | Increased γ-linolenic acid | [75] |
| Obesity | Serum | Increased C9:0 and C19:0 | [76] |
| Drug-induced liver injury | Serum | Altered PUFA | [83] |
| Hepatic steatosis | Serum | Increased dihomo-γ-linolenic acid | [84] |
| Severe traumatic brain injury | Plasma | Increased decanoic and octanoic acids | [82] |
| Neonatal morbidities and mortality | Red blood cell | Low AA and DHA | [88] |
| Autoimmune diseases | Serum | decreased n-6/n-3 ratio | [85] |
| Autoimmunity | Red blood cell | Decreased levels of n-3 fatty acid and docosapentaenoic acid | [86] |
| Allergy in children | Blood | Increased C22:5 n-3 and decreased C18:1 n-9 | [87] |
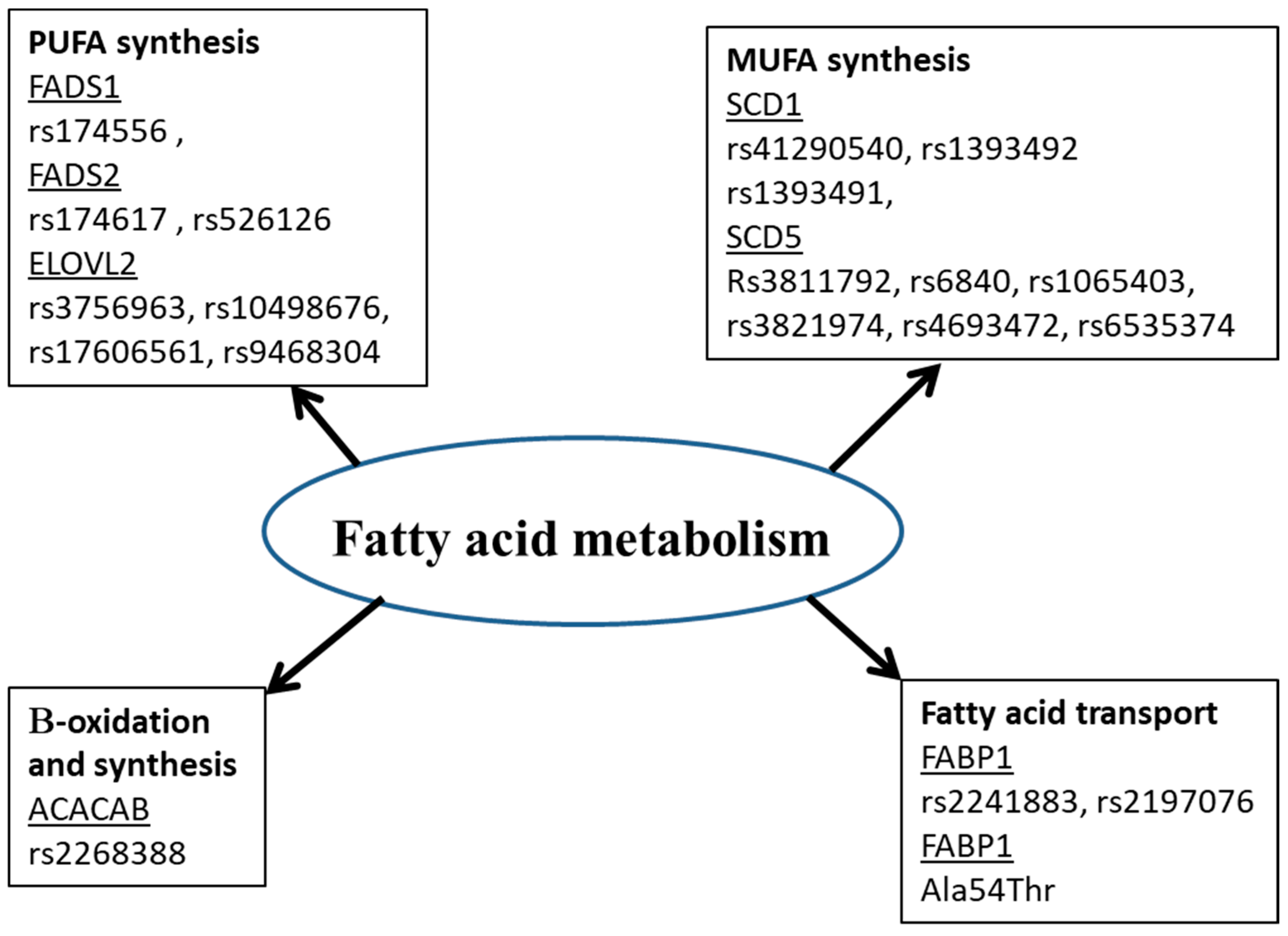
3.2. Polymorphisms of Gene Implicated in Fatty Acid Metabolism and Diseases
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holman, R.T.; Johnson, S.B.; Hatch, T.F. A case of human linolenic acid deficiency involving neurological abnormalities. Am. J. Clin. Nutr. 1982, 35, 617–623. [Google Scholar] [CrossRef]
- Hansen, A.E.; Haggard, M.E.; Boelsche, A.N.; Adam, D.J.; Wiese, H.F. Essential fatty acids in infant nutrition: III. Clinical manifestations of linoleic acid deficiency. J. Nutr. 1958, 66, 565–576. [Google Scholar] [CrossRef]
- Guesnet, P.; Alessandri, J.-M.; Astorg, P.; Pifferi, F.; Lavialle, M. Les rôles physiologiques majeurs exercés par les acides gras polyinsaturés (AGPI). Oléagineux Corps Gras Lipides 2005, 12, 333–343. [Google Scholar] [CrossRef]
- Parsons, H.G.; Hill, R.; Pencharz, P.; Kuksis, A. Modulation of human erythrocyte shape and fatty acids by diet. Biochim. Et Biophys. Acta (BBA)—Biomembr. 1986, 860, 420–427. [Google Scholar] [CrossRef]
- Lankinen, M.; Uusitupa, M.; Schwab, U. Genes and Dietary Fatty Acids in Regulation of Fatty Acid Composition of Plasma and Erythrocyte Membranes. Nutrients 2018, 10, 1785. [Google Scholar] [CrossRef] [PubMed]
- Chamorro, R.; Gonzalez, M.F.; Aliaga, R.; Gengler, V.; Balladares, C.; Barrera, C.; Bascuñan, K.A.; Bazinet, R.P.; Valenzuela, R. Diet, Plasma, Erythrocytes, and Spermatozoa Fatty Acid Composition Changes in Young Vegan Men. Lipids 2020, 55, 639–648. [Google Scholar] [CrossRef]
- Zarrouk, A.; Riedinger, J.-M.; Ahmed, S.H.; Hammami, S.; Chaabane, W.; Debbabi, M.; Ben Ammou, S.; Rouaud, O.; Frih, M.; Lizard, G.; et al. Fatty Acid Profiles in Demented Patients: Identification of Hexacosanoic Acid (C26:0) as a Blood Lipid Biomarker of Dementia. J. Alzheimer’s Dis. 2015, 44, 1349–1359. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Ma, J.; Campos, H.; Hankinson, S.E.; Hu, F.B. Comparison between plasma and erythrocyte fatty acid content as biomarkers of fatty acid intake in US women. Am. J. Clin. Nutr. 2007, 86, 74–81. [Google Scholar] [CrossRef]
- Ahmed, S.H.; Koubaa, N.; Kharroubi, W.; Zarrouk, A.; Mnari, A.; Batbout, F.; Gamra, H.; Hammami, S.; Lizard, G.; Hammami, M. Identification of long and very long chain fatty acids, plasmalogen-C16: 0 and phytanic acid as new lipid biomarkers in Tunisian coronary artery disease patients. Prostaglandins Other Lipid Mediat. 2017, 131, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Hodson, L.; Skeaff, C.M.; Fielding, B.A. Fatty acid composition of adipose tissue and blood in humans and its use as a biomarker of dietary intake. Prog. Lipid Res. 2008, 47, 348–380. [Google Scholar] [CrossRef]
- Maulucci, G.; Cohen, O.; Daniel, B.; Sansone, A.; Petropoulou, P.I.; Filou, S.; Spyridonidis, A.; Pani, G.; De Spirito, M.; Chatgilialoglu, C.; et al. Fatty acid-related modulations of membrane fluidity in cells: Detection and implications. Free. Radic. Res. 2016, 50, S40–S50. [Google Scholar] [CrossRef]
- Stillwell, W.; Shaikh, S.R.; Zerouga, M.; Siddiqui, R.; Wassall, S.R. Docosahexaenoic acid affects cell signaling by altering lipid rafts. Reprod. Nutr. Dev. 2005, 45, 559–579. [Google Scholar] [CrossRef]
- Ghosh, A.; Gao, L.; Thakur, A.; Siu, P.M.; Lai, C.W.K. Role of free fatty acids in endothelial dysfunction. J. Biomed. Sci. 2017, 24, 50. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.S.; Nassar, Z.D.; Swinnen, J.V.; Butler, L.M. Monounsaturated Fatty Acids: Key Regulators of Cell Viability and Intracellular Signaling in Cancer. Mol. Cancer Res. 2022, 20, 1354–1364. [Google Scholar] [CrossRef] [PubMed]
- Wahle, K.W.J.; Rotondo, D.; Heys, S.D. Polyunsaturated fatty acids and gene expression in mammalian systems. Proc. Nutr. Soc. 2003, 62, 349–360. [Google Scholar] [CrossRef]
- Miles, E.; Childs, C.; Calder, P. Long-Chain Polyunsaturated Fatty Acids (LCPUFAs) and the Developing Immune System: A Narrative Review. Nutrients 2021, 13, 247. [Google Scholar] [CrossRef] [PubMed]
- Innes, J.K.; Calder, P.C. Omega-6 fatty acids and inflammation. Prostaglandins Leukot. Essent. Fat. Acids 2018, 132, 41–48. [Google Scholar] [CrossRef]
- Rogero, M.M.; Calder, P.C. Obesity, Inflammation, Toll-Like Receptor 4 and Fatty Acids. Nutrients 2018, 10, 432. [Google Scholar] [CrossRef]
- MacDonald-Ramos, K.; Martínez-Ibarra, A.; Monroy, A.; Miranda-Ríos, J.; Cerbón, M. Effect of Dietary Fatty Acids on MicroRNA Expression Related to Metabolic Disorders and Inflammation in Human and Animal Trials. Nutrients 2021, 13, 1830. [Google Scholar] [CrossRef] [PubMed]
- Krümmel, B.; von Hanstein, A.-S.; Plötz, T.; Lenzen, S.; Mehmeti, I. Differential effects of saturated and unsaturated free fatty acids on ferroptosis in rat β-cells. J. Nutr. Biochem. 2022, 106, 109013. [Google Scholar] [CrossRef] [PubMed]
- Sherratt, S.C.; Juliano, R.A.; Mason, R.P. Eicosapentaenoic acid (EPA) has optimal chain length and degree of unsaturation to inhibit oxidation of small dense LDL and membrane cholesterol domains as compared to related fatty acids in vitro. Biochim. et Biophys. Acta (BBA)—Biomembr. 2020, 1862, 183254. [Google Scholar] [CrossRef] [PubMed]
- Mitrovic, M.; Turnic, T.N.; Zivkovic, V.; Pavic, Z.; Vranic, A.; Srejovic, I.; Sretenovic, J.; Bolevich, S.; Jakovljevic, V.L. High-protein diet and omega-3 fatty acids improve redox status in olanzapine-treated rats. Mol. Cell. Biochem. 2020, 468, 143–152. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Rosenberg, I.; Uauy, R. History of modern nutrition science—Implications for current research, dietary guidelines, and food policy. BMJ 2018, 361, k2392. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef]
- Wilczek, M.M.; Olszewski, R.; Krupienicz, A. Trans-Fatty Acids and Cardiovascular Disease: Urgent Need for Legislation. Cardiology 2017, 138, 254–258. [Google Scholar] [CrossRef]
- Sun, Q.; Ma, J.; Campos, H.; Hankinson, S.E.; Manson, J.E.; Stampfer, M.J.; Rexrode, K.M.; Willett, W.C.; Hu, F.B. A Prospective Study of Trans Fatty Acids in Erythrocytes and Risk of Coronary Heart Disease. Circulation 2007, 115, 1858–1865. [Google Scholar] [CrossRef]
- Mallick, R.; Duttaroy, A.K. Modulation of endothelium function by fatty acids. Mol. Cell. Biochem. 2021, 477, 15–38. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.X.; Parker, R.; Parpia, B.; Qu, Y.S.; Cassano, P.; Crawford, M.; Leyton, J.; Tian, J.; Li, J.Y.; Chen, J.S. Erythrocyte fatty acids, plasma lipids, and cardiovascular disease in rural China. Am. J. Clin. Nutr. 1990, 52, 1027–1036. [Google Scholar] [CrossRef]
- Lemaitre, R.N.; McKnight, B.; Sotoodehnia, N.; Fretts, A.M.; Qureshi, W.T.; Song, X.; King, I.B.; Sitlani, C.M.; Siscovick, D.S.; Psaty, B.M.; et al. Circulating Very Long-Chain Saturated Fatty Acids and Heart Failure: The Cardiovascular Health Study. J. Am. Heart Assoc. 2018, 7, e010019. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.H.; Kharroubi, W.; Kaoubaa, N.; Zarrouk, A.; Batbout, F.; Gamra, H.; Najjar, M.F.; Lizard, G.; Hininger-Favier, I.; Hammami, M. Correlation of trans fatty acids with the severity of coronary artery disease lesions. Lipids Health Dis. 2018, 17, 52. [Google Scholar] [CrossRef]
- Guo, M.; Fan, X.; Tuerhongjiang, G.; Wang, C.; Wu, H.; Lou, B.; Wu, Y.; Yuan, Z.; She, J. Targeted metabolomic analysis of plasma fatty acids in acute myocardial infarction in young adults. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 3131–3141. [Google Scholar] [CrossRef]
- Nishizaki, Y.; Shimada, K.; Tani, S.; Ogawa, T.; Ando, J.; Takahashi, M.; Yamamoto, M.; Shinozaki, T.; Miyazaki, T.; Miyauchi, K.; et al. Association between the ratio of serum n-3 to n-6 polyunsaturated fatty acids and acute coronary syndrome in non-obese patients with coronary risk factor: A multicenter cross-sectional study. BMC Cardiovasc. Disord. 2020, 20, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Bittner, D.O.; Goeller, M.; Zopf, Y.; Achenbach, S.; Marwan, M. Early-onset coronary atherosclerosis in patients with low levels of omega-3 fatty acids. Eur. J. Clin. Nutr. 2020, 74, 651–656. [Google Scholar] [CrossRef]
- Bazan, H.A.; Lu, Y.; Jun, B.; Fang, Z.; Woods, T.C.; Hong, S. Circulating inflammation-resolving lipid mediators RvD1 and DHA are decreased in patients with acutely symptomatic carotid disease. Prostaglandins Leukot. Essent. Fat. Acids 2017, 125, 43–47. [Google Scholar] [CrossRef]
- Yang, W.-S.; Chen, Y.-Y.; Chen, P.-C.; Hsu, H.-C.; Su, T.-C.; Lin, H.-J.; Chen, M.-F.; Lee, Y.-T.; Chien, K.-L. Association between Plasma N-6 Polyunsaturated Fatty Acids Levels and the Risk of Cardiovascular Disease in a Community-based Cohort Study. Sci. Rep. 2019, 9, 19298. [Google Scholar] [CrossRef] [PubMed]
- Chien, K.-L.; Lin, H.-J.; Hsu, H.-C.; Chen, P.-C.; Su, T.-C.; Chen, M.-F.; Lee, Y.-T. Comparison of predictive performance of various fatty acids for the risk of cardiovascular disease events and all-cause deaths in a community-based cohort. Atherosclerosis 2013, 230, 140–147. [Google Scholar] [CrossRef]
- Würtz, P.; Havulinna, A.S.; Soininen, P.; Tynkkynen, T.; Prieto-Merino, D.; Tillin, T.; Ghorbani, A.; Artati, A.; Wang, Q.; Tiainen, M.; et al. Metabolite profiling and cardiovascular event risk: A prospective study of 3 population-based cohorts. Circulation 2015, 131, 774–785. [Google Scholar] [CrossRef]
- Dozio, E.; Vianello, E.; Grossi, E.; Menicanti, L.; Schmitz, G.; Romanelli, M.M.C. Plasma fatty acid profile as biomarker of coronary artery disease: A pilot study using fourth generation artificial neural networks. J. Biol. Regul. Homeost. Agents 2018, 32, 1007–1013. [Google Scholar]
- Muldoon, M.F.; Erickson, K.I.; Goodpaster, B.H.; Jakicic, J.M.; Conklin, S.M.; Sekikawa, A.; Yao, J.K.; Manuck, S.B. Concurrent Physical Activity Modifies the Association between n3 Long-Chain Fatty Acids and Cardiometabolic Risk in Midlife Adults. J. Nutr. 2013, 143, 1414–1420. [Google Scholar] [CrossRef]
- Harris, K.; Oshima, M.; Sattar, N.; Würtz, P.; Jun, M.; Welsh, P.; Hamet, P.; Harrap, S.; Poulter, N.; Chalmers, J.; et al. Plasma fatty acids and the risk of vascular disease and mortality outcomes in individuals with type 2 diabetes: Results from the ADVANCE study. Diabetologia 2020, 63, 1637–1647. [Google Scholar] [CrossRef]
- Shoji, T.; Kakiya, R.; Hayashi, T.; Tsujimoto, Y.; Sonoda, M.; Shima, H.; Mori, K.; Fukumoto, S.; Tahara, H.; Shioi, A.; et al. Serum n-3 and n-6 Polyunsaturated Fatty Acid Profile as an Independent Predictor of Cardiovascular Events in Hemodialysis Patients. Am. J. Kidney Dis. 2013, 62, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, H.; Okubo, R.; Hamazaki, K.; Yamashita, A.; Narisawa, T.; Matsuoka, Y.J. Serum polyunsaturated fatty acids and risk of psychiatric disorder at 6 months after acute coronary syndrome: A prospective cohort study. Prostaglandins Leukot. Essent. Fat. Acids 2019, 149, 18–23. [Google Scholar] [CrossRef]
- Ouchi, S.; Miyazaki, T.; Shimada, K.; Sugita, Y.; Shimizu, M.; Murata, A.; Kato, T.; Aikawa, T.; Suda, S.; Shiozawa, T.; et al. Decreased circulating dihomo-gamma-linolenic acid levels are associated with total mortality in patients with acute cardiovascular disease and acute decompensated heart failure. Lipids Health Dis. 2017, 16, 150. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, Y.; Su, D.; Lv, X.; Wang, M.; Ding, D.; Ma, J.; Xia, M.; Wang, D.; Yang, Y.; et al. The opposite associations of long-chain versus very long-chain monounsaturated fatty acids with mortality among patients with coronary artery disease. Heart 2014, 100, 1597–1605. [Google Scholar] [CrossRef]
- Harris, W.S.; Kennedy, K.F.; O’Keefe, J.H.; Spertus, J.A. Red blood cell fatty acid levels improve GRACE score prediction of 2-yr mortality in patients with myocardial infarction. Int. J. Cardiol. 2013, 168, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Salgin, B.; Ong, K.K.; Thankamony, A.; Emmett, P.; Wareham, N.J.; Dunger, D.B. Higher Fasting Plasma Free Fatty Acid Levels Are Associated with Lower Insulin Secretion in Children and Adults and a Higher Incidence of Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2012, 97, 3302–3309. [Google Scholar] [CrossRef]
- Clore, J.N.; Allred, J.; White, D.; Li, J.; Stillman, J. The role of plasma fatty acid composition in endogenous glucose production in patients with type 2 diabetes mellitus. Metabolism 2002, 51, 1471–1477. [Google Scholar] [CrossRef]
- Liu, L.; Li, Y.; Guan, C.; Li, K.; Wang, C.; Feng, R.; Sun, C. Free fatty acid metabolic profile and biomarkers of isolated post-challenge diabetes and type 2 diabetes mellitus based on GC–MS and multivariate statistical analysis. J. Chromatogr. B 2010, 878, 2817–2825. [Google Scholar] [CrossRef]
- Jo, S.; An, W.-S.; Park, Y. Erythrocyte n-3 Polyunsaturated Fatty Acids and the Risk of Type 2 Diabetes in Koreans: A Case-Control Study. Ann. Nutr. Metab. 2013, 63, 283–290. [Google Scholar] [CrossRef]
- Ma, Y.; Xiong, J.; Zhang, X.; Qiu, T.; Pang, H.; Li, X.; Zhu, J.; Wang, J.; Pan, C.; Yang, X.; et al. Potential biomarker in serum for predicting susceptibility to type 2 diabetes mellitus: Free fatty acid 22:6. J. Diabetes Investig. 2020, 12, 950–962. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.S.; N., S.K.; Shetty, P.K. ω-6/ω-3 fatty acid ratio as an essential predictive biomarker in the management of type 2 diabetes mellitus. Nutrition 2020, 79-80, 110968. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wang, Y.; Ong, C.-N.; Subramaniam, T.; Choi, H.W.; Yuan, J.-M.; Koh, W.-P.; Pan, A. Metabolic signatures and risk of type 2 diabetes in a Chinese population: An untargeted metabolomics study using both LC-MS and GC-MS. Diabetologia 2016, 59, 2349–2359. [Google Scholar] [CrossRef] [PubMed]
- Grapov, D.; Adams, S.H.; Pedersen, T.L.; Garvey, W.T.; Newman, J.W. Type 2 Diabetes Associated Changes in the Plasma Non-Esterified Fatty Acids, Oxylipins and Endocannabinoids. PLoS ONE 2012, 7, e48852. [Google Scholar] [CrossRef]
- Yi, L.; He, J.; Liang, Y.; Yuan, D.; Gao, H.; Zhou, H. Simultaneously quantitative measurement of comprehensive profiles of esterified and non-esterified fatty acid in plasma of type 2 diabetic patients. Chem. Phys. Lipids 2007, 150, 204–216. [Google Scholar] [CrossRef]
- Sobczak, A.I.S.; Blindauer, C.A.; Stewart, A.J. Changes in Plasma Free Fatty Acids Associated with Type-2 Diabetes. Nutrients 2019, 11, 2022. [Google Scholar] [CrossRef]
- Ruddock, M.W.; Stein, A.; Landaker, E.; Park, J.; Cooksey, R.C.; McClain, D.; Patti, M.-E. Saturated Fatty Acids Inhibit Hepatic Insulin Action by Modulating Insulin Receptor Expression and Post-receptor Signalling. J. Biochem. 2008, 144, 599–607. [Google Scholar] [CrossRef]
- Miao, Z.; Lin, J.-S.; Mao, Y.; Chen, G.-D.; Zeng, F.-F.; Dong, H.-L.; Jiang, Z.; Wang, J.; Xiao, C.; Shuai, M.; et al. Erythrocyte n-6 Polyunsaturated Fatty Acids, Gut Microbiota, and Incident Type 2 Diabetes: A Prospective Cohort Study. Diabetes Care 2020, 43, 2435–2443. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.S.; Sharp, S.J.; Jansen, E.; Luben, R.N.; Khaw, K.-T.; Wareham, N.J.; Forouhi, N.G. Fatty acids measured in plasma and erythrocyte-membrane phospholipids and derived by food-frequency questionnaire and the risk of new-onset type 2 diabetes: A pilot study in the European Prospective Investigation into Cancer and Nutrition (EPIC)—Norfolk cohort. Am. J. Clin. Nutr. 2010, 92, 1214–1222. [Google Scholar] [CrossRef]
- Takkunen, M.J.; the DPS Study Group; Schwab, U.S.; de Mello, V.D.; Eriksson, J.G.; Lindstroöm, J.; Tuomilehto, J.; Uusitupa, M.I.J. Longitudinal associations of serum fatty acid composition with type 2 diabetes risk and markers of insulin secretion and sensitivity in the Finnish Diabetes Prevention Study. Eur. J. Nutr. 2015, 55, 967–979. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Sun, Y.; Snetselaar, L.G.; Sun, Q.; Yang, Q.; Zhang, Z.; Liu, L.; Hu, F.B.; Bao, W. Association between plasma trans-fatty acid concentrations and diabetes in a nationally representative sample of US adults. J. Diabetes 2018, 10, 653–664. [Google Scholar] [CrossRef]
- Prada, M.; Wittenbecher, C.; Eichelmann, F.; Wernitz, A.; Kuxhaus, O.; Kröger, J.; Weikert, C.; Schulze, M.B. Plasma Industrial and Ruminant Trans Fatty Acids and Incident Type 2 Diabetes in the EPIC-Potsdam Cohort. Diabetes Care 2022, 45, 845–853. [Google Scholar] [CrossRef]
- Luo, C.; Liu, H.; Wang, X.; Xia, L.; Huang, H.; Peng, X.; Xia, C.; Liu, L. The associations between individual plasma SFAs, serine palmitoyl-transferase long-chain base subunit 3 gene rs680379 polymorphism, and type 2 diabetes among Chinese adults. Am. J. Clin. Nutr. 2021, 114, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Jin, D.; Wang, S.; Xu, Y.; Li, H.; Chang, Y.; Ma, Y.; Xu, Y.; Guo, C.; Peng, F.; et al. Serum ω-6/ω-3 polyunsaturated fatty acids ratio and diabetic retinopathy: A propensity score matching based case-control study in China. eClinicalMedicine 2021, 39, 101089. [Google Scholar] [CrossRef]
- Afshinnia, F.; Rajendiran, T.M.; He, C.; Byun, J.; Montemayor, D.; Darshi, M.; Tumova, J.; Kim, J.; Limonte, C.P.; Miller, R.G.; et al. Circulating Free Fatty Acid and Phospholipid Signature Predicts Early Rapid Kidney Function Decline in Patients with Type 1 Diabetes. Diabetes Care 2021, 44, 2098–2106. [Google Scholar] [CrossRef]
- Amézaga, J.; Arranz, S.; Urruticoechea, A.; Ugartemendia, G.; Larraioz, A.; Louka, M.; Uriarte, M.; Ferreri, C.; Tueros, I. Altered Red Blood Cell Membrane Fatty Acid Profile in Cancer Patients. Nutrients 2018, 10, 1853. [Google Scholar] [CrossRef]
- Jiao, J.; Kwan, S.-Y.; Sabotta, C.M.; Tanaka, H.; Veillon, L.; Warmoes, M.O.; Lorenzi, P.L.; Wang, Y.; Wei, P.; Hawk, E.T.; et al. Circulating Fatty Acids Associated with Advanced Liver Fibrosis and Hepatocellular Carcinoma in South Texas Hispanics. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1643–1651. [Google Scholar] [CrossRef]
- Chen, Q.; Wang, J.; Lin, J.; Chen, L.; Lin, L.-S.; Pan, L.-Z.; Shi, B.; Qiu, Y.; Zheng, X.-Y.; Chen, F.; et al. Erythrocyte ω-3 polyunsaturated fatty acids are inversely associated with the risk of oral cancer: A case-control study. Nutr. Diabetes 2020, 10, 35. [Google Scholar] [CrossRef]
- Shishavan, N.G.; Mohamadkhani, A.; Sepanlou, S.G.; Masoudi, S.; Sharafkhah, M.; Poustchi, H.; Hekmatdoost, A.; Pourshams, A. Circulating plasma fatty acids and risk of pancreatic cancer: Results from the Golestan Cohort Study. Clin. Nutr. 2020, 40, 1897–1904. [Google Scholar] [CrossRef] [PubMed]
- Zaridze, D.G.; Chevchenko, V.E.; Levtshuk, A.A.; Lifanova, Y.E.; Maximovitch, D.M. Fatty acid composition of phospholipids in erythrocyte membranes and risk of breast cancer. Int. J. Cancer 1990, 45, 807–810. [Google Scholar] [CrossRef]
- Hirko, K.A.; Chai, B.; Spiegelman, D.; Campos, H.; Farvid, M.S.; Hankinson, S.E.; Willett, W.C.; Eliassen, A.H. Erythrocyte membrane fatty acids and breast cancer risk: A prospective analysis in the nurses’ health study II. Int. J. Cancer 2017, 142, 1116–1129. [Google Scholar] [CrossRef] [PubMed]
- McGee, E.E.; Kim, C.H.; Wang, M.; Spiegelman, D.; Stover, D.G.; Heng, Y.J.; Collins, L.C.; Baker, G.M.; Farvid, M.S.; Schedin, P.; et al. Erythrocyte membrane fatty acids and breast cancer risk by tumor tissue expression of immuno-inflammatory markers and fatty acid synthase: A nested case-control study. Breast Cancer Res. 2020, 22, 78. [Google Scholar] [CrossRef] [PubMed]
- Ruan, X.; Wang, Y.; Zhou, L.; Zheng, Q.; Hao, H.; He, D. Evaluation of Untargeted Metabolomic Strategy for the Discovery of Biomarker of Breast Cancer. Front. Pharmacol. 2022, 13, 894099. [Google Scholar] [CrossRef]
- Komi, D.E.A.; Shekari, N.; Soofian-Kordkandi, P.; Javadian, M.; Shanehbandi, D.; Baradaran, B.; Kazemi, T. Docosahexaenoic acid (DHA) and linoleic acid (LA) modulate the expression of breast cancer involved miRNAs in MDA-MB-231 cell line. Clin. Nutr. ESPEN 2021, 46, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Jurczyszyn, A.; Czepiel, J.; Gdula-Argasińska, J.; Czapkiewicz, A.; Biesiada, G.; Dróżdż, M.; Perucki, W.; Castillo, J.J. Erythrocyte membrane fatty acids in multiple myeloma patients. Leuk. Res. 2014, 38, 1260–1265. [Google Scholar] [CrossRef]
- Kaikkonen, J.E.; Jula, A.; Viikari, J.S.A.; Juonala, M.; Hutri-Kähönen, N.; Kähönen, M.; Lehtimäki, T.; Raitakari, O.T. Associations of Serum Fatty Acid Proportions with Obesity, Insulin Resistance, Blood Pressure, and Fatty Liver: The Cardiovascular Risk in Young Finns Study. J. Nutr. 2021, 151, 970–978. [Google Scholar] [CrossRef]
- Ma, Y.; Qiu, T.; Zhu, J.; Wang, J.; Li, X.; Deng, Y.; Zhang, X.; Feng, J.; Chen, K.; Wang, C.; et al. Serum FFAs profile analysis of Normal weight and obesity individuals of Han and Uygur nationalities in China. Lipids Health Dis. 2020, 19, 13. [Google Scholar] [CrossRef]
- Ni, Y.; Zhao, L.; Yu, H.; Ma, X.; Bao, Y.; Rajani, C.; Loo, L.W.; Shvetsov, Y.B.; Yu, H.; Chen, T.; et al. Circulating Unsaturated Fatty Acids Delineate the Metabolic Status of Obese Individuals. eBioMedicine 2015, 2, 1513–1522. [Google Scholar] [CrossRef]
- Yamagishi, K.; Ikeda, A.; Chei, C.-L.; Noda, H.; Umesawa, M.; Cui, R.; Muraki, I.; Ohira, T.; Imano, H.; Sankai, T.; et al. Serum α-linolenic and other ω-3 fatty acids, and risk of disabling dementia: Community-based nested case–control study. Clin. Nutr. 2016, 36, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Hammouda, S.; Ghzaiel, I.; Khamlaoui, W.; Hammami, S.; Mhenni, S.Y.; Samet, S.; Hammami, M.; Zarrouk, A. Genetic variants in FADS1 and ELOVL2 increase level of arachidonic acid and the risk of Alzheimer’s disease in the Tunisian population. Prostaglandins Leukot. Essent. Fat. Acids 2020, 160, 102159. [Google Scholar] [CrossRef]
- Sala-Vila, A.; Satizabal, C.L.; Tintle, N.; van Lent, D.M.; Vasan, R.S.; Beiser, A.S.; Seshadri, S.; Harris, W.S. Red Blood Cell DHA Is Inversely Associated with Risk of Incident Alzheimer’s Disease and All-Cause Dementia: Framingham Offspring Study. Nutrients 2022, 14, 2408. [Google Scholar] [CrossRef]
- Tomata, Y.; Larsson, S.C.; Hägg, S. Polyunsaturated fatty acids and risk of Alzheimer’s disease: A Mendelian randomization study. Eur. J. Nutr. 2019, 59, 1763–1766. [Google Scholar] [CrossRef]
- Orešič, M.; Posti, J.; Kamstrup-Nielsen, M.H.; Takala, R.S.; Lingsma, H.F.; Mattila, I.; Jäntti, S.; Katila, A.J.; Carpenter, K.; Ala-Seppälä, H.; et al. Human Serum Metabolites Associate With Severity and Patient Outcomes in Traumatic Brain Injury. eBioMedicine 2016, 12, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Fu, H.; Zhou, T.; Cai, M.; Huang, Y.; Gan, Q.; Zhang, C.; Qian, C.; Wang, J.; Zhang, Z.; et al. Alteration of Bile Acids and Omega-6 PUFAs Are Correlated With the Progression and Prognosis of Drug-Induced Liver Injury. Front. Immunol. 2022, 13, 772368. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Kawamoto, T.; Tamura, R. Predictive value of serum dihomo-γ-linolenic acid level and estimated Δ-5 desaturase activity in patients with hepatic steatosis. Obes. Res. Clin. Pract. 2017, 11, 34–43. [Google Scholar] [CrossRef]
- Tsoukalas, D.; Fragoulakis, V.; Sarandi, E.; Docea, A.O.; Papakonstaninou, E.; Tsilimidos, G.; Anamaterou, C.; Fragkiadaki, P.; Aschner, M.; Tsatsakis, A.; et al. Targeted Metabolomic Analysis of Serum Fatty Acids for the Prediction of Autoimmune Diseases. Front. Mol. Biosci. 2019, 6, 120. [Google Scholar] [CrossRef] [PubMed]
- Norris, J.M.; Kroehl, M.; Fingerlin, T.E.; Frederiksen, B.N.; Seifert, J.; Wong, R.; Clare-Salzler, M.; Rewers, M. Erythrocyte membrane docosapentaenoic acid levels are associated with islet autoimmunity: The Diabetes Autoimmunity Study in the Young. Diabetologia 2013, 57, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, A.; Galli, C.; Eiben, G.; Ahrens, W.; Iacoviello, L.; Molnár, D.; Pala, V.; Risé, P.; Rodriguez, G.; Russo, P.; et al. Blood fatty acid composition in relation to allergy in children aged 2–9 years: Results from the European IDEFICS study. Eur. J. Clin. Nutr. 2016, 71, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Fares, S.; Sethom, M.; Hammami, M.; Cheour, M.; Feki, M.; Hadj-Taieb, S.; Kacem, S. Postnatal RBC arachidonic and docosahexaenoic acids deficiencies are associated with higher risk of neonatal morbidities and mortality in preterm infants. Prostaglandins Leukot. Essent. Fat. Acids 2017, 126, 112–116. [Google Scholar] [CrossRef]
- Jaček, M.; Hrnčířová, D.; Rambousková, J.; Dlouhý, P.; Tůma, P. Effect of Food with Low Enrichment of N-3 Fatty Acids in a Two-Month Diet on the Fatty Acid Content in the Plasma and Erythrocytes and on Cardiovascular Risk Markers in Healthy Young Men. Nutrients 2020, 12, 2207. [Google Scholar] [CrossRef]
- Seethaler, B.; Basrai, M.; Vetter, W.; Lehnert, K.; Engel, C.; Siniatchkin, M.; Halle, M.; Kiechle, M.; Bischoff, S.C. Fatty acid profiles in erythrocyte membranes following the Mediterranean diet—Data from a multicenter lifestyle intervention study in women with hereditary breast cancer (LIBRE). Clin. Nutr. 2019, 39, 2389–2398. [Google Scholar] [CrossRef]
- Raeisi, M.; Hassanbeigi, L.; Khalili, F.; Kharrati-Shishavan, H.; Yousefi, M.; Mehdizadeh, A. Stearoyl-CoA desaturase 1 as a therapeutic target for cancer: A focus on hepatocellular carcinoma. Mol. Biol. Rep. 2022, 49, 8871–8882. [Google Scholar] [CrossRef]
- Stearoyl-CoA desaturase 1: A potential target for non-alcoholic fatty liver disease?-perspective on emerging experimental evidence. World J. Hepatol. 2022, 14, 168–179. [CrossRef] [PubMed]
- Iida, T.; Ubukata, M.; Mitani, I.; Nakagawa, Y.; Maeda, K.; Imai, H.; Ogoshi, Y.; Hotta, T.; Sakata, S.; Sano, R.; et al. Discovery of potent liver-selective stearoyl-CoA desaturase-1 (SCD1) inhibitors, thiazole-4-acetic acid derivatives, for the treatment of diabetes, hepatic steatosis, and obesity. Eur. J. Med. Chem. 2018, 158, 832–852. [Google Scholar] [CrossRef]
- Liu, Z.; Yin, X.; Mai, H.; Li, G.; Lin, Z.; Jie, W.; Li, K.; Zhou, H.; Wei, S.; Hu, L.; et al. SCD rs41290540 single-nucleotide polymorphism modifies miR-498 binding and is associated with a decreased risk of coronary artery disease. Mol. Genet. Genom. Med. 2020, 8, e1136. [Google Scholar] [CrossRef]
- Guo, Y.; Xiong, Z.; Su, M.; Huang, L.; Liao, J.; Xiao, H.; Huang, X.; Xiong, Z. Positive association of SCD1 genetic variation and metabolic syndrome in dialysis patients in China. Pers. Med. 2020, 17, 111–119. [Google Scholar] [CrossRef]
- Planck, T.; Shahida, B.; Sjögren, M.; Groop, L.; Hallengren, B.; Lantz, M. Association of BTG2, CYR61, ZFP36, and SCD Gene Polymorphisms with Graves’ Disease and Ophthalmopathy. Thyroid 2014, 24, 1156–1161. [Google Scholar] [CrossRef] [PubMed]
- Martín-Núñez, G.M.; Cabrera-Mulero, R.; Rojo-Martínez, G.; Gómez-Zumaquero, J.M.; Chaves, F.J.; de Marco, G.; Soriguer, F.; Castaño, L.; Morcillo, S. Polymorphisms in the SCD1 gene are associated with indices of stearoyl CoA desaturase activity and obesity: A prospective study. Mol. Nutr. Food Res. 2013, 57, 2177–2184. [Google Scholar] [CrossRef] [PubMed]
- Byberg, L.; Kilander, L.; Lemming, E.W.; Michaëlsson, K.; Vessby, B. Cancer death is related to high palmitoleic acid in serum and to polymorphisms in the SCD-1 gene in healthy Swedish men. Am. J. Clin. Nutr. 2014, 99, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Tibori, K.; Orosz, G.; Zámbó, V.; Szelényi, P.; Sarnyai, F.; Tamási, V.; Rónai, Z.; Mátyási, J.; Tóth, B.; Csala, M.; et al. Molecular Mechanisms Underlying the Elevated Expression of a Potentially Type 2 Diabetes Mellitus Associated SCD1 Variant. Int. J. Mol. Sci. 2022, 23, 6221. [Google Scholar] [CrossRef]
- Zámbó, V.; Orosz, G.; Szabó, L.; Tibori, K.; Sipeki, S.; Molnár, K.; Csala, M.; Kereszturi, É. A Single Nucleotide Polymorphism (rs3811792) Affecting Human SCD5 Promoter Activity Is Associated with Diabetes Mellitus. Genes 2022, 13, 1784. [Google Scholar] [CrossRef]
- Yu, G.I.; Mun, K.H.; Yang, S.H.; Shin, D.H.; Hwang, J.S. Polymorphisms in the 3′-UTR of SCD5 gene are associated with hepatocellular carcinoma in Korean population. Mol. Biol. Rep. 2018, 45, 1705–1714. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Cao, H.; Qin, L.; Jiang, Y. A Case-Control Study between Gene Polymorphisms of Polyunsaturated Fatty Acid Metabolic Rate-Limiting Enzymes and Acute Coronary Syndrome in Chinese Han Population. BioMed Res. Int. 2013, 2013, 928178. [Google Scholar] [CrossRef]
- Khamlaoui, W.; Mehri, S.; Hammami, S.; Hammouda, S.; Chraeif, I.; Elosua, R.; Hammami, M. Association Between Genetic Variants in FADS1-FADS2 and ELOVL2 and Obesity, Lipid Traits, and Fatty Acids in Tunisian Population. Clin. Appl. Thromb. 2020, 26. [Google Scholar] [CrossRef]
- Sun, C.; Zou, M.; Wang, X.; Xia, W.; Ma, Y.; Liang, S.; Hao, Y.; Wu, L.; Fu, S. FADS1-FADS2 and ELOVL2 gene polymorphisms in susceptibility to autism spectrum disorders in Chinese children. BMC Psychiatry 2018, 18, 283. [Google Scholar] [CrossRef] [PubMed]
- Valizadeh, M.; Aghasizadeh, M.; Nemati, M.; Hashemi, M.; Aghaee-Bakhtiari, S.H.; Zare-Feyzabadi, R.; Esmaily, H.; Ghazizdaeh, H.; Sahebi, R.; Ahangari, N.; et al. The association between a Fatty Acid Binding Protein 1 (FABP1) gene polymorphism and serum lipid abnormalities in the MASHAD cohort study. Prostaglandins Leukot. Essent. Fat. Acids 2021, 172, 102324. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Zhao, H.; Liu, X.; Zhao, Y.-R.; Chen, Z.-J.; Ma, J. Association of single-nucleotide polymorphisms rs2197076 and rs2241883 of FABP1 gene with polycystic ovary syndrome. J. Assist. Reprod. Genet. 2015, 33, 75–83. [Google Scholar] [CrossRef]
- Mansego, M.L.; Martínez, F.; Martínez-Larrad, M.T.; Zabena, C.; Rojo, G.; Morcillo, S.; Soriguer, F.; Martín-Escudero, J.C.; Serrano-Ríos, M.; Redon, J.; et al. Common Variants of the Liver Fatty Acid Binding Protein Gene Influence the Risk of Type 2 Diabetes and Insulin Resistance in Spanish Population. PLoS ONE 2012, 7, e31853. [Google Scholar] [CrossRef]
- Mozaffari, M.; Ghayour-Mobarhan, M.; Zare-Feyzabadi, R.; Valizadeh, M. FABP1 gene variant associated with risk of metabolic syndrome. Comb. Chem. High Throughput Screen. 2022, 25, 1355–1360. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.-E.; Wu, Y.-L.; Lu, Q.-Q.; Hu, Z.-J.; Lin, X. Two genetic variants in FABP1 and susceptibility to non-alcohol fatty liver disease in a Chinese population. Gene 2012, 500, 54–58. [Google Scholar] [CrossRef]
- Fisher, E.; Li, Y.; Burwinkel, B.; Kühr, V.; Hoffmann, K.; Möhlig, M.; Spranger, J.; Pfeiffer, A.; Boeing, H.; Schrezenmeir, J.; et al. Preliminary Evidence of FABP2 A54T Polymorphism Associated with Reduced Risk of Type 2 Diabetes and Obesity in Women from a German Cohort. Horm. Metab. Res. 2006, 38, 341–345. [Google Scholar] [CrossRef]
- Shabana; Hasnain, S. The fatty acid binding protein 2 (FABP2) polymorphism Ala54Thr and obesity in Pakistan: A population based study and a systematic meta-analysis. Gene 2015, 574, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wu, G.; Han, L.; Zhao, K.; Qu, Y.; Xu, A.; Huang, Q. Association of the FABP2 Ala54Thr polymorphism with type 2 diabetes, obesity, and metabolic syndrome: A population-based case-control study and a systematic meta-analysis. Genet. Mol. Res. 2015, 14, 1155–1168. [Google Scholar] [CrossRef]
- Peng, X.; Zhang, L.; Wang, Q.; Cui, X. Study on the relationship between FABP2 Ala54Thr polymorphism and the risk of non-alcoholic fatty liver diseases. Wei Sheng Yan Jiu 2009, 38, 401–404. [Google Scholar]
- Khattab, S.A.; Abo-Elmatty, D.; Ghattas, M.H.; Mesbah, N.; Mehanna, E.T. Intestinal fatty acid binding protein Ala54Thr polymorphism is associated with peripheral atherosclerosis combined with type 2 diabetes mellitus. J. Diabetes 2016, 9, 821–826. [Google Scholar] [CrossRef]
- Li, Z.; Ni, C.-L.; Niu, W.-Y.; Chang, B.-C.; Chen, L.-M. The intestinal fatty acid binding protein-2 Ala54Thr polymorphism is associated with diabetic retinopathy in Chinese population. Diabetol. Metab. Syndr. 2015, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Canani, L.H.; Capp, C.; Ng, D.P.; Choo, S.G.; Maia, A.L.; Nabinger, G.B.; Santos, K.; Crispim, D.; Roisemberg, I.; Krolewski, A.S.; et al. The Fatty Acid–Binding Protein-2 A54T Polymorphism Is Associated With Renal Disease in Patients With Type 2 Diabetes. Diabetes 2005, 54, 3326–3330. [Google Scholar] [CrossRef]
- Abbas, S.; Raza, S.T.; Chandra, A.; Rizvi, S.; Ahmed, F.; Eba, A.; Mahdi, F. Association of ACE, FABP2 and GST genes polymorphism with essential hypertension risk among a North Indian population. Ann. Hum. Biol. 2014, 42, 461–469. [Google Scholar] [CrossRef]
- Sikhayeva, N.; Iskakova, A.; Saigi-Morgui, N.; Zholdybaeva, E.; Eap, C.-B.; Ramanculov, E. Association between 28 single nucleotide polymorphisms and type 2 diabetes mellitus in the Kazakh population: A case-control study. BMC Med. Genet. 2017, 18, 76. [Google Scholar] [CrossRef] [PubMed]
- An, L.; Jiang, H.; Tang, R.-N. The ACACB gene rs2268388 polymorphism is associated with nephropathy in Caucasian patients with diabetes: A meta-analysis. Ren. Fail. 2015, 37, 925–928. [Google Scholar] [CrossRef]
- Tang, S.C.W.; Leung, V.T.M.; Chan, L.Y.Y.; Wong, S.S.H.; Chu, D.W.S.; Leung, J.C.K.; Ho, Y.W.; Lai, K.N.; Ma, L.; Elbein, S.C.; et al. The acetyl-coenzyme A carboxylase beta (ACACB) gene is associated with nephropathy in Chinese patients with type 2 diabetes. Nephrol. Dial. Transplant. 2010, 25, 3931–3934. [Google Scholar] [CrossRef]
- Shah, V.N.; Cheema, B.S.; Sharma, R.; Khullar, M.; Kohli, H.S.; Ahluwalia, T.S.; Mohan, V.; Bhansali, A. ACACβ gene (rs2268388) and AGTR1 gene (rs5186) polymorphism and the risk of nephropathy in Asian Indian patients with type 2 diabetes. Mol. Cell. Biochem. 2012, 372, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Chan, G.C.W.; Zhi, H.; Hicks, P.J.; Freedman, B.I.; Tang, S.C.W. Acetyl-coenzyme A carboxylase beta gene polymorphism does not predict cardiovascular risk susceptibility in Chinese type 2 diabetic individuals. Nephrology 2022, 27, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Riancho, J.; Vázquez, L.; García-Pérez, M.; Sainz, J.; Olmos, J.; Hernández, J.; Pérez-López, J.; Amado, J.; Zarrabeitia, M.; Cano, A.; et al. Association of ACACB polymorphisms with obesity and diabetes. Mol. Genet. Metab. 2011, 104, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.M.; Goumidi, L.; Bertrais, S.; Field, M.R.; Cupples, L.A.; Ordovas, J.M.; McMonagle, J.; Defoort, C.; Lovegrove, J.A.; Drevon, C.A.; et al. ACC2 gene polymorphisms, metabolic syndrome, and gene-nutrient interactions with dietary fat. J. Lipid Res. 2010, 51, 3500–3507. [Google Scholar] [CrossRef]


| Study 1 [6] | Study 2 [7] | Study 3 [8] | ||||
|---|---|---|---|---|---|---|
| Samples | Plasma | RBC | Plasma | RBC | Plasma | RBC |
| Total SFA | 29.9 ± 2.3 | 42.1 ± 4.6 | 34.22 ± 3.26 | 50.56 ± 6.82 | 28.71 ± 2.38 | 34.37 ± 1.60 |
| Lauric acid, 12:0 | 0.09 ± 0.02 | - | - | - | 0.02 ± 0.03 | 0.002 ±0.01 |
| Myristic acid, 14:0 | 0.95 ± 0.3 | 0.73 ± 0.2 | - | - | 0.58 ± 0.28 | 0.19 ± 0.10 |
| Palmitic acid, 16:0 | 21.1 ± 1.9 | 25.9 ± 3.0 | 26.24 ± 2.75 | 30.05 ± 4.71 | 19.31 ± 2.41 | 18.65 ± 1.86 |
| Stearic acid, 18:0 | 7.08 ± 0.8 | 13.2 ± 1.2 | 7.16 ± 1.52 | 16.51 ± 3.41 | 7.29 ± 0.78 | 13.14 ± 1.00 |
| Arachidic acid, 20:0 | 0.06 ± 0.05 | 0.14 ± 0.1 | 0.25 ± 0.35 | 0.62 ± 0.27 | - | - |
| Behenic acid, 22:0 | 0.19 ± 0.07 | 0.50 ± 0.2 | 0.30 ± 0.12 | 1.71 ± 0.62 | - | - |
| Lignoceric acid, 24:0 | 0.17 ± 0.08 | 1.71 ± 0.7 | 0.17 ± 0.05 | 0.79 ± 0.29 | - | - |
| Cerotic acid, 26:0 | - | - | 0.1 ± 0.05 | 0.88 ± 0.06 | - | - |
| Total MUFA | 25.0 ± 4.3 | 20.8 ± 2.9 | 28.2 ± 3.48 | 30.71 ± 5.13 | 22.86 ± 3.01 | 18.64 ± 1.24 |
| Myristoleic acid, 14:1 n-5 | 0.01 ± 0.01 | 0.03 ± 0.1 | 1.32 ± 1.21 | 1.52 ± 1.23 | - | - |
| Palmitoleic acid, 16:1 n-5 | - | - | 2.53 ± 0.9 | 1.53 ± 0.97 | - | - |
| Oleic acid, 18:1 n-9 | 22.7 ± 3.4 | 18.4 ± 2.4 | 21.01 ± 3.56 | 22.01 ± 4.62 | 18.60 ± 2.43 | 13.26 ± 1.17 |
| cis-Vaccenic acid, 18:1 n-7 | - | - | 1.93 ± 0.48 | 2.41 ± 0.68 | - | - |
| Eicosenoic acid, 20:1 n-9 | 0.25 ± 0.1 | 0.90 ± 0.2 | 0.64 ± 0.13 | 0.49 ± 0.29 | - | - |
| Erucic acid, 22:1 n-9 | - | - | 0.43 ± 0.16 | 1.33 ± 1.05 | - | - |
| Nervonic acid, 24:1 n-9 | - | - | 0.34 ± 0.02 | 1.42 ± 1.08 | - | - |
| Total PUFA | 45.1 ± 4.9 | 37.1 ± 6.7 | 37.58 ± 4.67 | 18.73 ± 4.97 | 44.87 ± 4.81 | 43.48 ± 1.77 |
| Alpha-linolenic acid, 18:3 n-3 | 0.69 ± 0.1 | 0.12 ± 0.01 | 0.71 ± 0.23 | 0.47 ± 0.47 | 0.50 ± 0.15 | 0.18 ± 0.05 |
| Eicosatrienoic acid, 20:3 n-3 | - | - | 1.75 ± 0.48 | 1.71 ± 0.98 | - | - |
| Eicosapentaenoic acid, 20:5 n-3 | 0.50 ± 0.2 | 0.32 ± 0.2 | 0.30 ± 0.31 | 0.61 ± 0.41 | 0.49 ± 0.21 | 1.15 ± 0.91 |
| Docosahexaenoic acid, 22:6 n-3 | - | - | 1.43 ± 0.27 | 0.73 ± 0.07 | 1.56 ± 0.60 | 3.71 ± 1.09 |
| Linoleic acid, 18:2 n-6 | 33.7 ± 4.5 | 14.8 ± 2.2 | 27.78 ± 5.26 | 9.49 ± 3.31 | 30.58 ± 4.33 | 13.66 ± 1.80 |
| linolenic acid, 18:3 n-6 | 0.36 ± 0.1 | 0.40 ± 0.2 | 0.59 ± 0.30 | 0.39 ± 0.45 | - | - |
| Dihomo-c-linolenic acid, 20:3 n-6 | 1.29 ± 0.3 | 1.50 ± 0.4 | 0.57 ± 0.37 | 2.01 ± 0.85 | - | - |
| Arachidonic acid, 20:4 n-6 | 6.27 ± 1.6 | 4.82 ± 1.52 | 4.45 ± 1.24 | 3.32 ± 2.06 | 7.80 ± 1.62 | 14.63 ± 1.29 |
| Genes | Polymorphisms | Diseases | References |
|---|---|---|---|
| SCD1 | rs41290540 | Decreased risk of coronary artery disease | [62] |
| rs1393492 | Metabolic syndrome | [63] | |
| rs1393491 | Graves’ Ophthalmopathy | [64] | |
| SCD5 | rs3811792 | Diabetes | [68] |
| rs6840, rs1065403, rs3821974, rs4693472, rs6535374 | Hepatocellular carcinoma | [69] | |
| FADS1 | rs174556 | Increase the risk of Alzheimer’s disease | [53] |
| Acute Coronary Syndrome | [70] | ||
| Obesity | [71] | ||
| FADS2 | rs174617 | No effect on the risk of Alzheimer’s disease | [53] |
| obesity | [71] | ||
| rs526126 | Autism spectrum disorder | [72] | |
| ELOVL2 | rs3756963 | Increase the risk of Alzheimer’s disease | [53] |
| obesity | [71] | ||
| rs10498676, rs17606561, rs3756963 and rs9468304 | Autism spectrum disorder | [72] | |
| FABP1 | rs2241883 | Dyslipidemia | [73] |
| rs2197076 and rs2241883 | Polycystic ovary syndrome | [74] | |
| rs2241883 and rs1545224 | Non-alcoholic fatty liver | [77] | |
| rs2197076 | Type 2 diabetes | [75] | |
| rs2241883 | Metabolic syndrome | [76] | |
| FABP2 | Ala54Thr | Diabetes, metabolic syndrome and obesity | [78] |
| Peripheral atherosclerosis combined with T2DM | [82] | ||
| Obesity | [79] | ||
| Diabetic retinopathy | [83] | ||
| Type 2 diabetes and metabolic syndrome | [80] | ||
| Renal disease in type 2 diabetic | [84] | ||
| Non-alcoholic fatty liver | [81] | ||
| rs1799883 | Essential hypertension | [85] | |
| Diabetes | [86] | ||
| ACACB | rs2268388 | Diabetes related nephropathy | [87,89] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaaba, R.; Bouaziz, A.; Ben Amor, A.; Mnif, W.; Hammami, M.; Mehri, S. Fatty Acid Profile and Genetic Variants of Proteins Involved in Fatty Acid Metabolism Could Be Considered as Disease Predictor. Diagnostics 2023, 13, 979. https://doi.org/10.3390/diagnostics13050979
Chaaba R, Bouaziz A, Ben Amor A, Mnif W, Hammami M, Mehri S. Fatty Acid Profile and Genetic Variants of Proteins Involved in Fatty Acid Metabolism Could Be Considered as Disease Predictor. Diagnostics. 2023; 13(5):979. https://doi.org/10.3390/diagnostics13050979
Chicago/Turabian StyleChaaba, Raja, Aicha Bouaziz, Asma Ben Amor, Wissem Mnif, Mohamed Hammami, and Sounira Mehri. 2023. "Fatty Acid Profile and Genetic Variants of Proteins Involved in Fatty Acid Metabolism Could Be Considered as Disease Predictor" Diagnostics 13, no. 5: 979. https://doi.org/10.3390/diagnostics13050979
APA StyleChaaba, R., Bouaziz, A., Ben Amor, A., Mnif, W., Hammami, M., & Mehri, S. (2023). Fatty Acid Profile and Genetic Variants of Proteins Involved in Fatty Acid Metabolism Could Be Considered as Disease Predictor. Diagnostics, 13(5), 979. https://doi.org/10.3390/diagnostics13050979