

Deep Hybrid Learning Prediction of Patient-Specific Quality Assurance in Radiotherapy: Implementation in Clinical Routine
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohorts
2.2. Radiotherapy Plan
2.3. Patient Specific Quality Assurance
- x: gamma mean value
- σ: standard deviation
2.4. Artificial Intelligence Algorithms
2.4.1. Machine Learning (ML)
2.4.2. Deep Hybrid Learning (DHL)
2.5. Statistical Analysis
3. Results
3.1. Prediction Models for All Tumor Location
3.2. Prediction for Brain and Thorax Tumor Location: Machine Learning Models
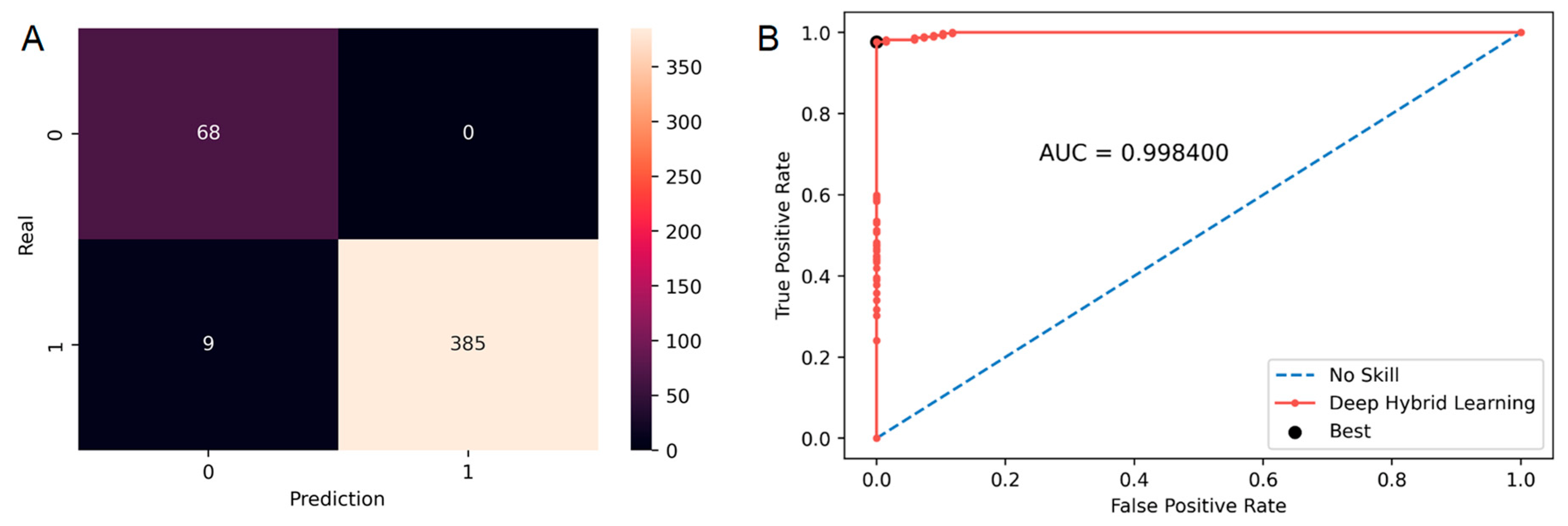
3.3. Prediction for Pelvis, Breast and H&N Tumor Location: Deep Hybrid Learning Models
3.4. Application of the Solution in Clinical Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Otto, K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med. Phys. 2007, 35, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Antoine, M.; Ralite, F.; Soustiel, C.; Marsac, T.; Sargos, P.; Cugny, A.; Caron, J. Use of metrics to quantify IMRT and VMAT treatment plan complexity: A systematic review and perspectives. Phys. Med. 2019, 64, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Low, D.A.; Harms, W.B.; Mutic, S.; Purdy, J.A. A technique for the quantitative evaluation of dose distributions. Med. Phys. 1998, 25, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Wu, Q.J. Knowledge-based planning for intensity-modulated radiation therapy: A review of data-driven approaches. Med. Phys. 2019, 46, 2760–2775. [Google Scholar] [CrossRef] [PubMed]
- Chiavassa, S.; Bessieres, I.; Edouard, M.; Mathot, M.; Moignier, A. Complexity metrics for IMRT and VMAT plans: A review of current literature and applications. Br. J. Radiol. 2019, 92, 20190270. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Chen, L.; Zhong, X.; Gonzalez, Y.; Visak, J.; Meng, B.; Inam, E.; Parsons, D.; Godley, A.; Jiang, S.; et al. Clinical experience on patient-specific quality assurance for CBCT-based online adaptive treatment plan. J. Appl. Clin. Med. Phys. 2023, e13918. [Google Scholar] [CrossRef]
- Savjani, R.R.; Salamon, N.; Deng, J.; Ma, M.; Tenn, S.; Agazaryan, N.; Hegde, J.; Kaprealian, T. A Framework for Sharing Radiation Dose Distribution Maps in the Electronic Medical Record for Improving Multidisciplinary Patient Management. Radiol. Imaging Cancer 2021, 3, e200075. [Google Scholar] [CrossRef]
- Sadowski, B.; Milewska, K.; Ginter, J. Machine Learning Based Prediction of Gamma Passing Rate for VMAT Radiotherapy Plans. J. Pers. Med. 2022, 12, 2071. [Google Scholar] [CrossRef]
- Jazouli, Z.; Muraro, S.; Julian, D. Patient-QA prediction: A new approach of complexity indexes. Phys. Med. 2021, 92, S87. [Google Scholar] [CrossRef]
- Kubben, P.; Dumontier, M.; Dekker, A. Fundamentals of Clinical Data Science; Springer International Publishing: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Chan, M.F.; Witztum, A.; Valdes, G. Integration of AI and Machine Learning in Radiotherapy QA. Front. Artif. Intell. 2020, 3, 577620. [Google Scholar] [CrossRef]
- Granville, D.A.; Sutherland, J.G.; Belec, J.G.; La Russa, D.J. Predicting VMAT patient-specific QA results using a support vector classifier trained on treatment plan characteristics and linac QC metrics. Phys. Med. Biol. 2019, 64, 095017. [Google Scholar] [CrossRef] [PubMed]
- Hirashima, H.; Ono, T.; Nakamura, M.; Miyabe, Y.; Mukumoto, N.; Iramina, H.; Mizowaki, T. Improvement of prediction and classification performance for gamma passing rate by using plan complexity and dosiomics features. Radiother. Oncol. 2020, 153, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, J.; Zhang, S.; Zhang, X.; Zhang, Q.; Chan, M.F.; Yang, R.; Sui, J. Multi-task autoencoder based classification-regression model for patient-specific VMAT QA. Phys. Med. Biol. 2020, 65, 235023. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.H.; Sohail, A.; Khan, A.; Hassan, M.; Lee, Y.S.; Alam, J.; Basit, A.; Zubair, S. COVID-19 detection in chest X-ray images using deep boosted hybrid learning. Comput. Biol. Med. 2021, 137, 104816. [Google Scholar] [CrossRef]
- Corroyer-Dulmont, A. DeepHybridLearning_RadiotherapyQA. 2022. Available online: https://github.com/AurelienCD/DeepHybridLearning_RadiotherapyQA_Depository_ManuscriptID_22-1397 (accessed on 27 February 2023).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhof, P.; Weiss, R.; Dubour, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Chollet, F. Keras. 2015. Available online: https://docs.anaconda.com (accessed on 27 February 2023).
- Lemaitre, G.; Fernando, N.; Aridas, C. Imbalanced-learn: A Python Toolbox to Tackle the Curse of Imbalanced Datasets in Machine Learning. J. Mach. Learn. Res. 2017, 18, 559–563. [Google Scholar] [CrossRef]
- Anaconda Software Distribution; Anaconda Inc.: Austin, TX, USA, 2020.
- Waskom, M.L. seaborn: Statistical data visualization. J. Open Source Softw. 2021, 6, 3021. [Google Scholar] [CrossRef]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Agazaryan, N.; Solberg, T.D.; Demarco, J.J. Patient specific quality assurance for the delivery of intensity modulated radiotherapy. J. Appl. Clin. Med. Phys. 2003, 4, 40–50. [Google Scholar] [CrossRef]
- Valdes, G.; Scheuermann, R.; Hung, C.Y.; Olszanski, A.; Bellerive, M.; Solberg, T.D. A mathematical framework for virtual IMRT QA using machine learning. Med. Phys. 2016, 43, 4323–4334. [Google Scholar] [CrossRef]
- Simon, L.; Robert, C.; Meyer, P. Artificial intelligence for quality assurance in radiotherapy. Cancer 2021, 25, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Kadoya, N.; Tomori, S.; Oku, Y.; Jingu, K. Error detection using a convolutional neural network with dose difference maps in patient-specific quality assurance for volumetric modulated arc therapy. Phys. Med. 2020, 73, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Interian, Y.; Rideout, V.; Kearney, V.P.; Gennatas, E.; Morin, O.; Cheung, J.; Solberg, T.; Valdes, G. Deep nets vs expert designed features in medical physics: An IMRT QA case study. Med. Phys. 2018, 45, 2672–2680. [Google Scholar] [CrossRef] [PubMed]
- Miften, M.; Olch, A.; Mihailidis, D.; Moran, J.; Pawlicki, T.; Molineu, A.; Li, H.; Wijesooriya, K.; Shi, J.; Xia, P.; et al. Tolerance limits and methodologies for IMRT measurement-based verification QA: Recommendations of AAPM Task Group No. 218. Med. Phys. 2018, 45, e53–e83. [Google Scholar] [CrossRef] [PubMed]
- Legrand, C. 49. Current uses of log files in the radiotherapy quality assurance workflow for IMRT and VMAT techniques. Phys. Med. 2017, 44, 24. [Google Scholar] [CrossRef]
- Defoor, D.L.; Vazquez-Quino, L.A.; Mavroidis, P.; Papanikolaou, N.; Stathakis, S. Anatomy-based, patient-specific VMAT QA using EPID or MLC log files. J. Appl. Clin. Med. Phys. 2015, 16, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Chow, V.U.Y.; Kan, M.W.K.; Chan, A.T.C. Patient-specific quality assurance using machine log files analysis for stereotactic body radiation therapy (SBRT). J. Appl. Clin. Med. Phys. 2020, 21, 179–187. [Google Scholar] [CrossRef]
- Yang, R.; Yang, X.; Wang, L.; Li, D.; Guo, Y.; Li, Y.; Guan, Y.; Wu, X.; Xu, S.; Zhang, S.; et al. Commissioning and clinical implementation of an Autoencoder based Classification-Regression model for VMAT patient-specific QA in a multi-institution scenario. Radiother. Oncol. 2021, 161, 230–240. [Google Scholar] [CrossRef]
- Darzidehkalani, E.; Ghasemi-Rad, M.; van Ooijen, P. Federated Learning in Medical Imaging: Part I: Toward Multicentral Health Care Ecosystems. J. Am. Coll. Radiol. 2022, 19, 969–974. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor Location | Number of VMAT Plans |
|---|---|
| Pelvis | 576 |
| Breast | 462 |
| H&N | 204 |
| Brain | 156 |
| Thorax | 99 |
| Digestive | 49 |
| Rachis | 30 |
| Other | 25 |
| Member | 17 |
| Skin | 14 |
| All | 1632 |
| TP | TN | FP | FN | Sensitivity | Specificity |
|---|---|---|---|---|---|
| 90.56% | 7.05% | 1.10% | 1.29% | 98.6% | 86.47% |
| TP | TN | FP | FN | Sensitivity | Specificity |
|---|---|---|---|---|---|
| 83.33% | 14.72% | 0% | 1.95% | 97.7% | 100% |
| Locations | AUC | Sensitivity | Specificity | Accuracy | TP | TN | FP | FN | Architecture |
|---|---|---|---|---|---|---|---|---|---|
| Brain | 1 | 100% | 100% | 100% | 94.87% | 5.13% | 0% | 0% | ML |
| Thorax | 0.9986 | 98.90% | 100% | 98.99% | 90.91% | 8.08% | 0% | 1.01% | ML |
| Pelvis | 0.9869 | 100% | 90% | 99.65% | 96.53% | 3.13% | 0.35% | 0% | DHL |
| Breast | 0.9984 | 97.72% | 100% | 98.05% | 83.33% | 14.72% | 0% | 1.95% | DHL |
| H&N | 0.9589 | 98.32% | 84% | 96.57% | 86.27% | 10.29% | 1.96% | 1.47% | DHL |
| All | 0.9891 | 99.33% | 98.50% | 97.43% | 91.24% | 8.03% | 0.12% | 0.61% | DHL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreau, N.; Bonnor, L.; Jaudet, C.; Lechippey, L.; Falzone, N.; Batalla, A.; Bertaut, C.; Corroyer-Dulmont, A. Deep Hybrid Learning Prediction of Patient-Specific Quality Assurance in Radiotherapy: Implementation in Clinical Routine. Diagnostics 2023, 13, 943. https://doi.org/10.3390/diagnostics13050943
Moreau N, Bonnor L, Jaudet C, Lechippey L, Falzone N, Batalla A, Bertaut C, Corroyer-Dulmont A. Deep Hybrid Learning Prediction of Patient-Specific Quality Assurance in Radiotherapy: Implementation in Clinical Routine. Diagnostics. 2023; 13(5):943. https://doi.org/10.3390/diagnostics13050943
Chicago/Turabian StyleMoreau, Noémie, Laurine Bonnor, Cyril Jaudet, Laetitia Lechippey, Nadia Falzone, Alain Batalla, Cindy Bertaut, and Aurélien Corroyer-Dulmont. 2023. "Deep Hybrid Learning Prediction of Patient-Specific Quality Assurance in Radiotherapy: Implementation in Clinical Routine" Diagnostics 13, no. 5: 943. https://doi.org/10.3390/diagnostics13050943
APA StyleMoreau, N., Bonnor, L., Jaudet, C., Lechippey, L., Falzone, N., Batalla, A., Bertaut, C., & Corroyer-Dulmont, A. (2023). Deep Hybrid Learning Prediction of Patient-Specific Quality Assurance in Radiotherapy: Implementation in Clinical Routine. Diagnostics, 13(5), 943. https://doi.org/10.3390/diagnostics13050943