


Differentiating Multiple Myeloma and Osteolytic Bone Metastases on Contrast-Enhanced Computed Tomography Scans: The Feasibility of Radiomics Analysis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. CT Data Acquisition
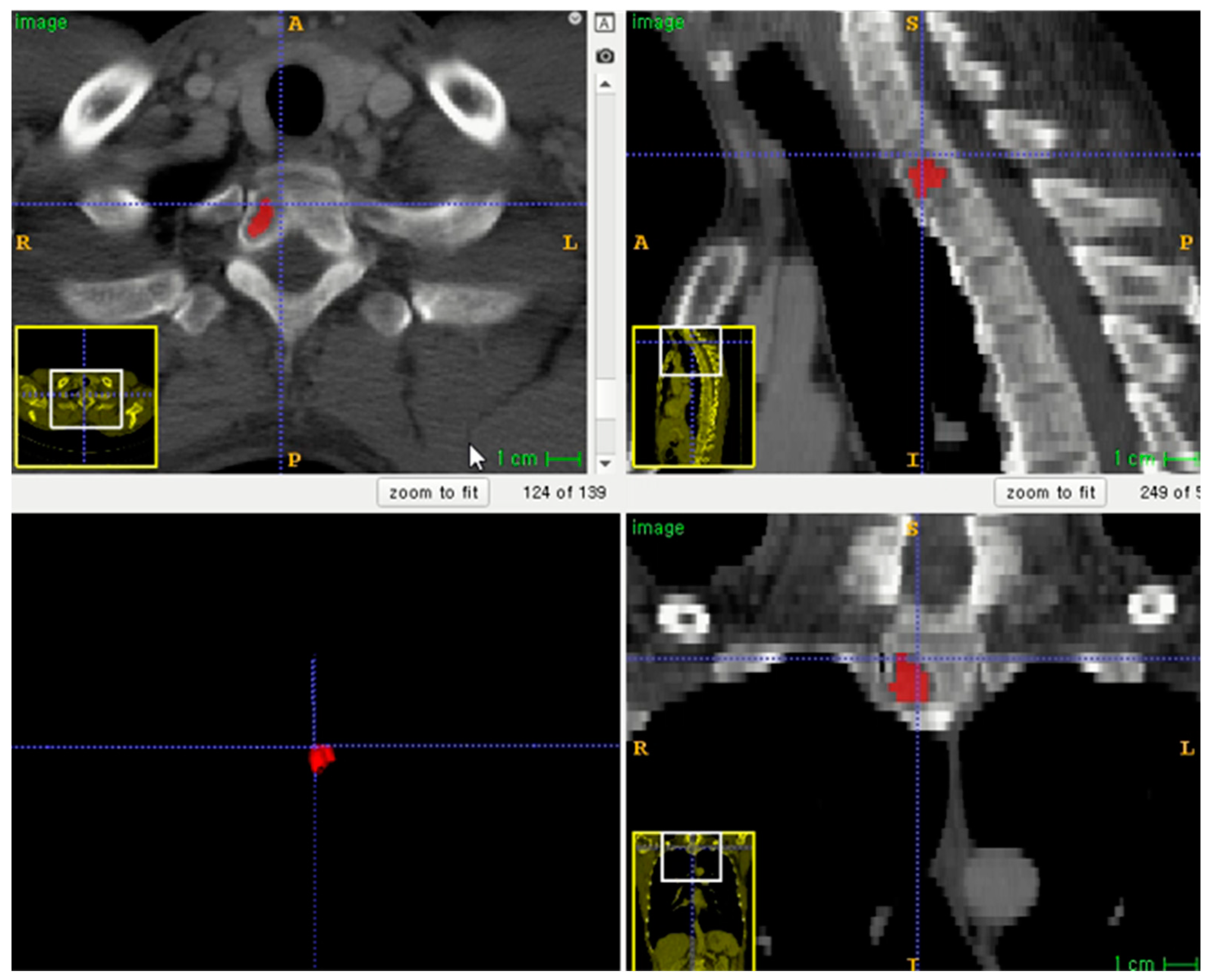
2.3. Volume of Interest (VOI) Segmentation and Radiomics Feature Extraction
2.4. Radiomics Feature Reduction and Selection
2.5. Radiomics Model Development
2.6. External Validation of Constructed Radiomics Model
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Radiomics Feature Selection and Model Development
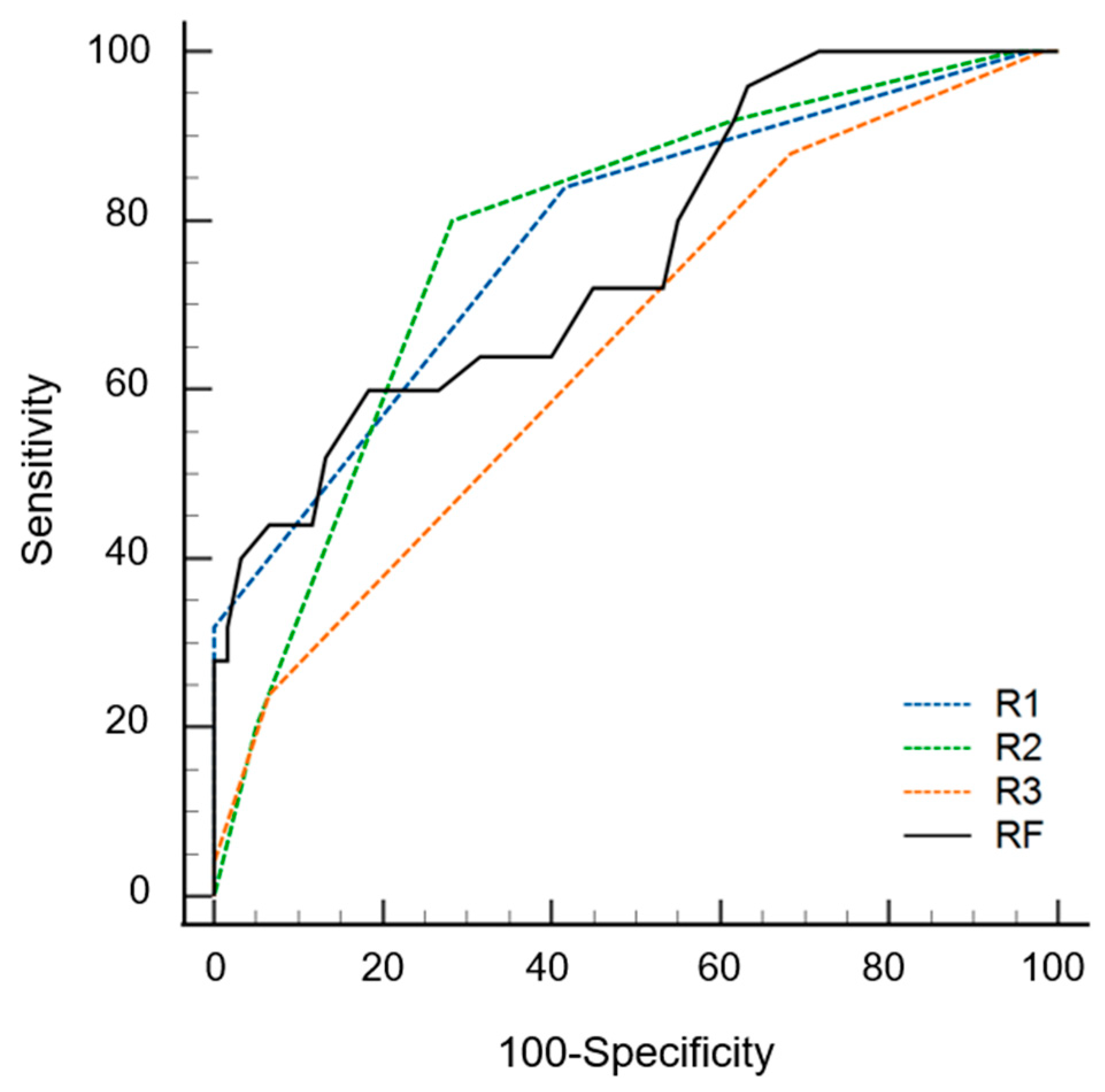
3.3. Diagnostic Performance of Radiomics Model on External Test Set
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Sullivan, G.J.; Carty, F.L.; Cronin, C.G. Imaging of bone metastasis: An update. World J. Radiol. 2015, 7, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Ulmert, D.; Solnes, L.; Thorek, D.L.J. Contemporary approaches for imaging skeletal metastasis. Bone Res. 2015, 3, 15024. [Google Scholar] [CrossRef] [PubMed]
- Padhani, A.R.; Makris, A.; Gall, P.; Collins, D.J.; Tunariu, N.; de Bono, J.S. Therapy monitoring of skeletal metastases with whole-body diffusion MRI. J. Magn. Reson. Imaging 2014, 39, 1049–1078. [Google Scholar] [CrossRef]
- Ormond Filho, A.G.; Carneiro, B.C.; Pastore, D.; Silva, I.P.; Yamashita, S.R.; Consolo, F.D.; Hungria, V.T.M.; Sandes, A.F.; Rizzatti, E.G.; Nico, M.A.C. Whole-Body Imaging of Multiple Myeloma: Diagnostic Criteria. Radiographics 2019, 39, 1077–1097. [Google Scholar] [CrossRef]
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Hillengass, J.; Usmani, S.; Rajkumar, S.V.; Durie, B.G.M.; Mateos, M.V.; Lonial, S.; Joao, C.; Anderson, K.C.; García-Sanz, R.; Riva, E.; et al. International myeloma working group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019, 20, e302–e312. [Google Scholar] [CrossRef]
- Mahnken, A.H.; Wildberger, J.E.; Gehbauer, G.; Schmitz-Rode, T.; Blaum, M.; Fabry, U.; Günther, R.W. Multidetector CT of the spine in multiple myeloma: Comparison with MR imaging and radiography. AJR Am. J. Roentgenol. 2002, 178, 1429–1436. [Google Scholar] [CrossRef]
- Huh, Y.J.; Lee, S.Y.; Kim, S.; Lee, S.E.; Jung, J.Y. Differentiation of multiple myelomas from osteolytic bone metastases: Diagnostic value of tumor homogeneity on Contrast-Enhanced CT. Br. J. Radiol. 2022, 95, 20220009. [Google Scholar] [CrossRef]
- Park, G.E.; Jee, W.-H.; Lee, S.-Y.; Sung, J.-K.; Jung, J.-Y.; Grimm, R.; Son, Y.; Paek, M.Y.; Min, C.-K.; Ha, K.-Y. Differentiation of multiple myeloma and metastases: Use of axial diffusion-weighted MR imaging in addition to standard MR imaging at 3T. PLoS ONE 2018, 13, e0208860. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, U.; Balci, A.; Özsan, G.H.; Özkal, S.; Şeyhanli, A.; Özgül, H.A. Computed tomography characteristics of multiple myeloma and other osteolytic metastatic bone lesions. Acta Radiol. 2021, 62, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, M.R.; Gillies, R.J. The Biological Meaning of Radiomic Features. Radiology 2021, 298, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Wang, J.; Hu, S.; Dai, Y.; Zhang, Y.; Hu, C. Differentiating Between Multiple Myeloma and Metastasis Subtypes of Lumbar Vertebra Lesions Using Machine Learning–Based Radiomics. Front. Oncol. 2021, 11, 601699. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Wang, Y.; Wang, Y.; Mao, Y.; Zhang, F.; Yu, J. Application of 18F-FDG PET-CT Images Based Radiomics in Identifying Vertebral Multiple Myeloma and Bone Metastases. Front. Med. 2022, 9, 969. [Google Scholar] [CrossRef] [PubMed]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef]
- Ligero, M.; Jordi-Ollero, O.; Bernatowicz, K.; Garcia-Ruiz, A.; Delgado-Muñoz, E.; Leiva, D.; Mast, R.; Suarez, C.; Sala-Llonch, R.; Calvo, N.; et al. Minimizing acquisition-related radiomics variability by image resampling and batch effect correction to allow for large-scale data analysis. Eur. Radiol. 2021, 31, 1460–1470. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Park, J.E.; Park, S.Y.; Kim, H.J.; Kim, H.S. Reproducibility and Generalizability in Radiomics Modeling: Possible Strategies in Radiologic and Statistical Perspectives. Korean J. Radiol. 2019, 20, 1124–1137. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, T.W.; Wu, C.Q.; Lin, Q.; Hu, R.; Xie, C.L.; Zuo, H.D.; Wu, J.L.; Mu, Q.W.; Fu, Q.S.; et al. Radiomics model of contrast-enhanced computed tomography for predicting the recurrence of acute pancreatitis. Eur. Radiol. 2019, 29, 4408–4417. [Google Scholar] [CrossRef]
- Zou, H.; Hastie, T. Regularization and variable selection via the elastic net. J. R. Stat. Soc. Ser. B Stat. Methodol. 2005, 67, 301–320. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Naseri, H.; Skamene, S.; Tolba, M.; Faye, M.D.; Ramia, P.; Khriguian, J.; Patrick, H.; Andrade Hernandez, A.X.; David, M.; Kildea, J. Radiomics-based machine learning models to distinguish between metastatic and healthy bone using lesion-center-based geometric regions of interest. Sci. Rep. 2022, 12, 9866. [Google Scholar] [CrossRef]
- Sun, W.; Liu, S.; Guo, J.; Liu, S.; Hao, D.; Hou, F.; Wang, H.; Xu, W. A CT-based radiomics nomogram for distinguishing between benign and malignant bone tumours. Cancer Imaging 2021, 21, 20. [Google Scholar] [CrossRef]
- Gitto, S.; Cuocolo, R.; Annovazzi, A.; Anelli, V.; Acquasanta, M.; Cincotta, A.; Albano, D.; Chianca, V.; Ferraresi, V.; Messina, C.; et al. CT radiomics-based machine learning classification of atypical cartilaginous tumours and appendicular chondrosarcomas. EBioMedicine 2021, 68, 103407. [Google Scholar] [CrossRef]
- Meyer, M.; Ronald, J.; Vernuccio, F.; Nelson, R.C.; Ramirez-Giraldo, J.C.; Solomon, J.; Patel, B.N.; Samei, E.; Marin, D. Reproducibility of CT Radiomic Fea tures within the Same Patient: Influence of Radiation Dose and CT Recon struction Settings. Radiology 2019, 293, 583–591. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Set | External Test Set | |||
|---|---|---|---|---|
| Characteristics | MM | Osteolytic Metastases | MM | Osteolytic Metastases |
| Number of patients | 49 | 126 | 15 | 35 |
| Number of lesions | 108 | 317 | 25 | 60 |
| Age (mean ± SD; years) | 60.7 ± 12.4 | 62.8 ± 13.1 | 74.8 ± 13.8 | 64.3 ± 11.4 |
| Sex (M:F) | 26:23 | 82:44 | 8:7 | 21:14 |
| Primary origin (numbers of patients) | n/a | Breast cancer (15) Cervical cancer (3) Cholangiocarcinoma (4) Colorectal cancer (5) Endometrial cancer (1) Gallbladder cancer (2) Hepatocellular carcinoma (17) Lung cancer (50) Melanoma (1) Neuroendocrine tumor (2) Ovarian cancer (1) Pancreatic cancer (1) Prostate cancer (3) Renal cell carcinoma (10) Stomach cancer (5) Thyroid cancer (3) Undifferentiated spindle cell sarcoma (1) Urothelial cell carcinoma (1) | n/a | Breast cancer (4) Colorectal cancer (1) Endometrial cancer (1) Gallbladder cancer (1) Hepatocellular carcinoma (2) Lung cancer (9) |
| Radiomics Features | Importance |
|---|---|
| wavelet.LLL_gldm_DependenceNonUniformityNormalized | 5.643140 |
| wavelet.HLL_firstorder_Maximum | 4.512872 |
| wavelet.LLL_gldm_DependenceVariance | 4.321726 |
| wavelet.LHL_gldm_LargeDependenceEmphasis | 3.974077 |
| original_glcm_SumEntropy | 3.792728 |
| wavelet.LHL_glszm_SmallAreaEmphasis | 3.693439 |
| wavelet.LLL_firstorder_10Percentile | 3.663920 |
| original_gldm_DependenceVariance | 3.499032 |
| wavelet.LHH_firstorder_Kurtosis | 3.353556 |
| original_glcm_Imc2 | 3.305649 |
| Diagnostic Performance (AUC) | Radiomics Model without Class Imbalance Correction | Radiomics Model with Class Imbalance Correction |
|---|---|---|
| Training set | 0.807 (0.759–0.854) | 0.821 (0.775–0.868) |
| External test set | 0.762 (0.648–0.876) | 0.842 (0.752–0.932) |
| Diagnostic Performance | Sensitivity | Specificity | Accuracy | AUC |
|---|---|---|---|---|
| Radiomics model (A) † | 60.0% (15/25) | 81.7% (49/60) | 75.3% (64/85) | 0.762 (0.648–0.876) |
| First review (B) | ||||
| R1 | 84.0% (21/25) | 58.3% (35/60) | 65.9% (56/85) | 0.781 (0.681–0.881) |
| R2 | 92.0% (23/25) | 38.3% (23/60) | 54.1% (46/85) | 0.778 (0.677–0.880) |
| R3 | 88.0% (22/25) | 31.7% (19/60) | 48.2% (41/85) | 0.653 (0.545–0.762) |
| Second review (C) | ||||
| R1 | 92.0% (23/25) | 68.3% (41/60) | 75.3% (64/85) | 0.900 (0.815–0.954) |
| R2 | 96.0% (24/25) | 53.3% (32/60) | 65.9% (56/85) | 0.876 (0.786–0.937) |
| R3 | 92.0% (23/25) | 53.3% (32/60) | 64.7% (55/85) | 0.833 (0.736–0.905) |
| Comparison of B and C (p-values) | ||||
| R1 | 0.500 | 0.109 | 0.039 * | <0.001 * |
| R2 | 1.000 | 0.004 * | 0.002 * | <0.001 * |
| R3 | 1.000 | 0.001 * | 0.001 * | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Lee, S.-Y.; Kim, S.; Huh, Y.-J.; Lee, J.; Lee, K.-E.; Jung, J.-Y. Differentiating Multiple Myeloma and Osteolytic Bone Metastases on Contrast-Enhanced Computed Tomography Scans: The Feasibility of Radiomics Analysis. Diagnostics 2023, 13, 755. https://doi.org/10.3390/diagnostics13040755
Lee S, Lee S-Y, Kim S, Huh Y-J, Lee J, Lee K-E, Jung J-Y. Differentiating Multiple Myeloma and Osteolytic Bone Metastases on Contrast-Enhanced Computed Tomography Scans: The Feasibility of Radiomics Analysis. Diagnostics. 2023; 13(4):755. https://doi.org/10.3390/diagnostics13040755
Chicago/Turabian StyleLee, Seungeun, So-Yeon Lee, Sanghee Kim, Yeon-Jung Huh, Jooyeon Lee, Ko-Eun Lee, and Joon-Yong Jung. 2023. "Differentiating Multiple Myeloma and Osteolytic Bone Metastases on Contrast-Enhanced Computed Tomography Scans: The Feasibility of Radiomics Analysis" Diagnostics 13, no. 4: 755. https://doi.org/10.3390/diagnostics13040755
APA StyleLee, S., Lee, S.-Y., Kim, S., Huh, Y.-J., Lee, J., Lee, K.-E., & Jung, J.-Y. (2023). Differentiating Multiple Myeloma and Osteolytic Bone Metastases on Contrast-Enhanced Computed Tomography Scans: The Feasibility of Radiomics Analysis. Diagnostics, 13(4), 755. https://doi.org/10.3390/diagnostics13040755