
Diagnostic Usefulness of Diffusion-Weighted MRI for Axillary Lymph Node Evaluation in Patients with Breast Cancer
 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. MRI Technique
2.3. Imaging Analysis
2.4. Statistical Analysis
3. Results
3.1. Continuous Variables
3.2. Categorical Variables
3.3. Diagnostic Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carter, C.L.; Allen, C.; Henson, D.E. Relation of tumor size, lymph node status, and survival in 24,740 breast cancer cases. Cancer 1989, 63, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Surveillance, Epidemiology, and End RESULTS Program (SEER). Table 4.13: Cancer of the Female Breast (Invasive)—5 Year Relative and Period Survival by Race, Diagnosis Year, Ange and Stage at Diagnosis. In: SEER Cancer Statistics Review (CSR) 1975–2016. SEER Website. Available online: https://seer.cancer.gov/csr/1975_2016/browse_csr.php?sectionSEL=4&pageSEL=sect_04_table.13 (accessed on 29 October 2019).
- Ahmed, M.; Douek, M. What is the future of axillary surgery for breast cancer? Ecancermedicalscience 2013, 7, 319. [Google Scholar] [PubMed]
- De Cataldo, C.; Bruno, F.; Palumbo, P.; Di Sibio, A.; Arrigoni, F.; Clemente, A.; Di Cesare, E.; Barile, A.; Splendiani, A.; Masciocchi, C.; et al. Apparent diffusion coefficient magnetic resonance imaging (adc-mri) in the axillary breast cancer lymph node metastasis detection: A narrative review. Gland Surg. 2020, 9, 2225–2234. [Google Scholar] [CrossRef]
- Schijven, M.P.; Vingerhoets, A.J.; Rutten, H.J.; Nieuwenhuijzen, G.A.; Roumen, R.M.; van Bussel, M.E.; Voogd, A.C. Comparison of morbidity between axillary lymph node dissection and sentinel node biopsy. Eur. J. Surg. Oncol. 2003, 29, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Valente, S.A.; Levine, G.M.; Silverstein, M.J.; Rayhanabad, J.A.; Weng-Grumley, J.G.; Ji, L.; Holmes, D.R.; Sposto, R.; Sener, S.F. Accuracy of predicting axillary lymph node positivity by physical examination, mammography, ultrasonography, and magnetic resonance imaging. Ann. Surg. Oncol. 2012, 19, 1825–1830. [Google Scholar] [CrossRef]
- Madej, B.; Maciejewski, R.; Wójtowicz, Z.; Burdan, F.; Torres, K.; Kadej, A.; Furtak, P. Axillary lymph node and early breast cancer diagnostics. A case report. Folia Morphol. 2003, 62, 523–525. [Google Scholar]
- Khan, A.; Masroor, I.; Khandwala, K.; Abbasi, S.U.; Tariq, M.U. Utility of ultrasound and mammography in detection of negative axillary nodal metastasis in breast cancer. Cureus 2020, 12, e6691. [Google Scholar] [CrossRef]
- Ecanow, J.S.; Abe, H.; Newstead, G.M.; Ecanow, D.B.; Jeske, J.M. Axillary staging of breast cancer: What the radiologist should know. Radiographics 2013, 33, 1589–1612. [Google Scholar] [CrossRef]
- Jang, J.M.; Leung, J.W.T.; Moy, L.; Ha, S.M.; Moon, W.K. Axillary nodal evaluation in breast cancer: State of the Art. Radiology 2020, 295, 500–515. [Google Scholar]
- Solomon, E.; Liberman, G.; Nissan, N.; Furman-Haran, E.; Sklair-Levy, M.; Frydman, L. Diffusion-weighted breast MRI of malignancies with submillimeter resolution and immunity to artifacts by spatiotemporal encoding at 3T. Magn. Reason. Med. 2020, 84, 1391–1403. [Google Scholar] [CrossRef]
- Scaranelo, A.M.; Eiada, R.; Jacks, L.M.; Kulkarni, S.R.; Crystal, P. Accuracy of unenhanced mr imaging in the detection of axillary lymph node metastasis: Study of reproducibility and reliability. Radiology 2012, 262, 425–434. [Google Scholar] [CrossRef]
- Chung, J.; Youk, J.H.; Kim, J.-A.; Gweon, H.M.; Kim, E.-K.; Ryu, Y.H.; Son, E.J. Role of diffusion-weighted MRI: Predicting axillary lymph node metastases in breast cancer. Acta Radiol. 2014, 55, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, G.; Sakurai, T.; Oura, S.; Suzuma, T.; Tamaki, T.; Umemura, T.; Kokawa, Y.; Yang, Q. Evaluation of axillary lymph node status in breast cancer with MRI. Breast Cancer 1999, 6, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Mortellaro, V.E.; Marshall, J.; Singer, L.; Hochwald, S.N.; Chang, M.; Copeland, E.M.; Grobmyer, S.R. Magnetic resonance imaging for axillary staging in patients with breast cancer. J. Magn. Reason. Imaging 2009, 30, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Baltzer, P.A.; Dietzel, M.; Burmeister, H.P.; Zoubi, R.; Gajda, M.; Camara, O.; Kaiser, W.A. Application of MR mammography beyond local staging: Is there a potential to accurately assess axillary lymph nodes? Evaluation of an extended protocol in an initial prospective study. AJR Am. J. Roentgenol. 2011, 196, W641–W647. [Google Scholar] [CrossRef]
- Kang, B.; Lipson, J.A.; Planey, K.R.; Zackrisson, S.; Ikeda, D.M.; Kao, J.; Pal, S.; Moran, C.J.; Daniel, B.L. Rim sign in breast lesions on diffusion-weighted magnetic resonance imaging: Diagnostic accuracy and clinical usefulness. J. Magn. Reason. Imaging 2015, 41, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, H.; Partridge, S.C.; Eby, P.R.; Demartini, W.B.; Gutierrez, R.L.; Peacock, S.; Lehman, C.D. Characterization of ductal carcinoma in situ on diffusion weighted breast MRI. Eur. Radiol. 2011, 21, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Isomoto, I.; Sueyoshi, E.; Yano, H.; Uga, T.; Abe, K.; Hayashi, T.; Honda, S.; Yamaguchi, T.; Uetani, M. Diagnostic performance of ADC for Non-mass-like breast lesions on MR imaging. Magn. Reason. Med. Sci. 2010, 9, 217–225. [Google Scholar] [CrossRef]
- Jeh, S.K.; Kim, S.H.; Kim, H.S.; Kang, B.J.; Jeong, S.H.; Yim, H.W.; Song, B.J. Correlation of the apparent diffusion coefficient value and dynamic magnetic resonance imaging findings with prognostic factors in invasive ductal carcinoma. J. Magn. Reason. Imaging 2011, 33, 102–109. [Google Scholar] [CrossRef]
- Kul, S.; Cansu, A.; Alhan, E.; Dinc, H.; Gunes, G.; Reis, A. Contribution of diffusion-weighted imaging to dynamic contrast-enhanced MRI in the characterization of breast tumor. AJR Am. J. Roentgenol. 2011, 196, 210–217. [Google Scholar] [CrossRef]
- Fornasa, F.; Nesoti, M.V.; Bovo, C.; Bonavina, M.G. Diffusion-weighted magnetic resonance imaging in the characterization of axillary lymph nodes in patients with breast cancer. J. Magn. Reason. Imaging 2012, 36, 858–864. [Google Scholar] [CrossRef] [PubMed]
- He, N.; Xie, C.; Wei, W.; Pan, C.; Wang, W.; Lv, N.; Wu, P. A new, preoperative, mri-based scoring system for diagnosing malignant axillary lymph nodes in women evaluated for breast cancer. Eur. J. Radiol. 2012, 81, 2602–2612. [Google Scholar] [CrossRef] [PubMed]
- Luo, N.; Su, D.; Jin, G.; Liu, L.; Zhu, X.; Xie, D.; Liu, Y. Apparent diffusion coefficient ratio between axillary lymph node with primary tumor to detect nodal metastasis in breast cancer patients. J. Magn. Reason. Imaging 2013, 38, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Kim, S.H.; Kang, B.J.; Choi, B.G.; Song, B.J.; Choi, J.J. Diagnostic value of breast mri for predicting metastatic axillary lymph nodes in breast cancer patients: Diffusion-weighted mri and conventional mri. Magn. Reason. Imaging 2014, 32, 1230–1236. [Google Scholar] [CrossRef]
- Ei Khouli, R.H.; Jacobs, M.A.; Mezban, S.D.; Huang, P.; Kamel, I.R.; Macura, K.J.; Bluemke, D.A. Diffusion-weighted imaging improves the diagnostic accuracy of conventional 3.0 T breast MR imaging. Radiology 2010, 256, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Patridge, S.C.; Nissan, N.; Rahbar, H.; Kitsch, A.E.; Sigmund, E.E. Diffusion-weighted breast MRI: Clinical application and emerging techniques. J. Magn. Reason. Imaging 2017, 45, 337–355. [Google Scholar] [CrossRef]
- Chayakulkheeree, J.; Pungrassami, D.; Prueksadee, J. Performance of breast magnetic resonance imaging in axillary nodal staging in newly diagnosed breast cancer patients. Pol. J. Radiol. 2019, 84, e413–e418. [Google Scholar] [CrossRef] [PubMed]
- Kwee, T.C.; Takahara, T.; Luijten, P.R.; Nievelstein, R.A. ADC measurements of lymph nodes: Inter- and intra-obsever reproducibility study and an overview of the literature. Eur. J. Radiol. 2010, 75, 215–220. [Google Scholar] [CrossRef]
- Hoehn-Berlage, M.; Eis, M.; Schmitx, B. Regional and directional anissotrpy of apparent diffusion coefficient in rat brain. NMR Biomed. 1999, 12, 45–50. [Google Scholar] [CrossRef]
- Wang, J.; Liao, Q.; Zhang, Y.; Yu, C.; Bai, R.; Sun, H. Differential diagnosis of axillary inflammatory and metastatic lymph nodes in rabbit models by using diffusion-weighted imaging: Compared with conventional magnetic resonance imaging. Korean J. Radiol. 2012, 13, 458–466. [Google Scholar] [CrossRef]
- DeLano, M.C.; Cooper, T.G.; Siebert, J.E.; Potchen, M.J.; Kuppusamy, K. High-b-balue diffusion-weighted MR imaging of adult brain: Image contrast and appraent diffusion coefficient map features. AJNR Am. J. Neuroradiol. 2000, 21, 1830–1836. [Google Scholar] [PubMed]
- Mulkern, R.V.; Barnes, A.S.; Haker, S.J.; Hung, Y.P.; Rybicki, F.J.; Maier, S.E.; Tempany, C.M. Biexponential characterization of prostate tissue water diffusion decay curves over an extended b-factor range. Magn. Reason. Imaging 2006, 24, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Rogers, W.; Thulasi Seetha, S.; Refaee, T.A.G.; Lieverse, R.I.Y.; Granzier, R.W.Y.; Ibrahim, A.; Keek, S.; Sanduleanu, S.; Primakov, S.; Beuque, M.; et al. Radiomics: From qualitative to quantitative imaging. Br. J. Radiol. 2020, 93, 20190948. [Google Scholar] [CrossRef] [PubMed]
- Ye, D.-M.; Wang, H.-T.; Yu, T. The application of radiomics in breast MRI: A Review. Technol. Cancer Res. Treat. 2020, 19, 1533033820916191. [Google Scholar] [CrossRef] [PubMed]
- Bickelhaupt, S.; Paech, D.; Kickingereder, P.; Steudle, F.; Lederer, W.; Daniel, H.; Götz, M.; Gählert, N.; Tichy, D.; Wiesenfarth, M.; et al. Prediction of malignancy by a radiomics signature from contrast agent-free diffusion MRI in suspicious breast lesions found on screening mammography. J. Magn. Reason. Imaging 2017, 46, 604–616. [Google Scholar] [CrossRef]
- Militello, C.; Rundo, L.; Dimarco, M.; Orlando, A.; Woitek, R.; D’Angelo, I.; Russo, G.; Bartolotta, T.V. 3D DCE-MRI radiomic analysis for malignant lesion prediction in breast cancer patients. Acad. Radiol. 2022, 29, 830–840. [Google Scholar] [CrossRef]
- Dong, Y.; Feng, Q.; Yang, W.; Lu, Z.; Deng, C.; Zhang, L.; Lian, Z.; Liu, J.; Luo, X.; Pei, S.; et al. Preoperative prediction of sentinel lymph node metastasis in breast cancer based on radiomics of T2-weighted fat-suppression and diffusion-weighted MRI. Eur. Radiol. 2018, 28, 582–591. [Google Scholar] [CrossRef]
- Park, H.; Lim, Y.; Ko, E.S.; Cho, H.; Lee, J.E.; Han, B.; Choi, J.S.; Park, K.W. Radiomics signature on magnetic resonance imaging: Association with disease-free survival in patients with invasive breast cancer. Clin. Cancer Res. 2018, 24, 4705–4714. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T2WI | DWI | Pre- and Post-Contrast T1WI 3D VIBE | |
|---|---|---|---|
| TR (msec) | 4530 | 5200 | 2.7 |
| TE (msec) | 90 | 53 | 0.8 |
| FOV (mm) | 340 × 205 | 320 × 320 | |
| Matrix size | 576 × 403 | 192 × 116 | 256 × 192 |
| Slice thickness (mm) | 6 | 4 | 1.2 |
| Flip angle (°) | 80 | 2, 6, 9, 12, 15 | |
| Acquisition time (s) | 148 | 151 | 10, 70, 130, 190, 250, 310 |
| b-value | 0, 1000 or 1200 |
| Subtypes of Primary Breast Cancer | Metastatic ALN (n = 35) | Benign ALN (n = 95) |
|---|---|---|
| Invasive carcinoma, no special type | 29 | 90 |
| Invasive lobular carcinoma | 3 | 2 |
| Mixed invasive carcinoma | 3 | 2 |
| Mucinous carcinoma | 0 | 4 |
| Tubular carcinoma | 0 | 2 |
| Metaplastic carcinoma | 0 | 2 |
| Encapsulated papillary carcinoma | 0 | 2 |
| Solid papillary carcinoma | 0 | 1 |
| Variables | Benign | Malignancy | p |
|---|---|---|---|
| * Long diameter (mm) | 10.1 ± 4.1 | 14.8 ± 7.7 | <0.001 |
| * Short diameter (mm) | 5.1 ± 1.6 | 9.2 ± 6.4 | <0.001 |
| * L/S ratio | 2.1 ± 0.8 | 1.8 ± 0.6 | 0.059 |
| * Cortical thickness (mm) | 3.2 ± 1.0 | 7.6 ± 7.0 | <0.001 |
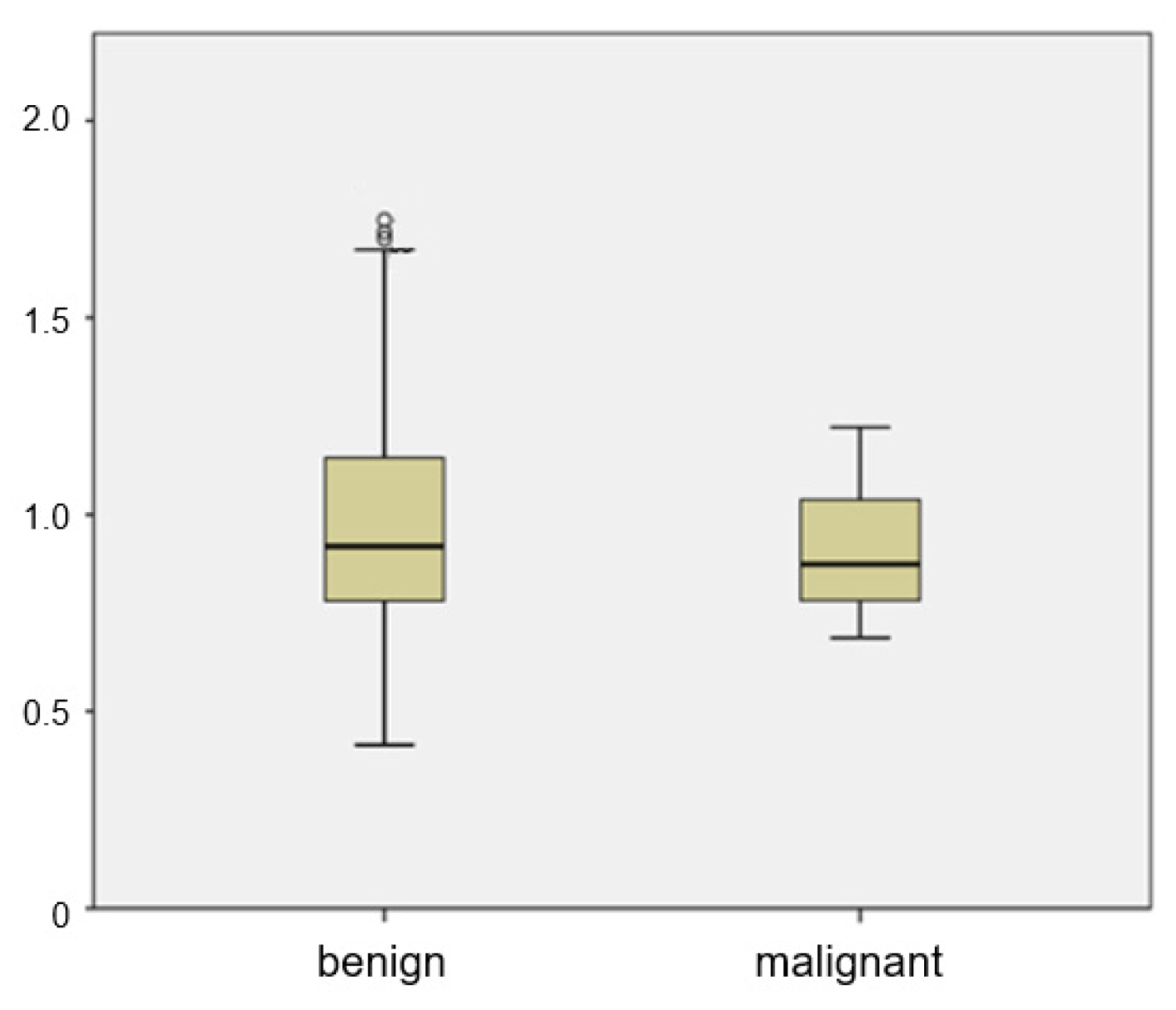
| * ADC value (×10−3 mm2/s) | 0.999 ± 0.283 | 0.905 ± 0.163 | 0.185 |
| Eccentricity | 0.001 | ||
| No | 68 (71.6) | 14 (40) | |
| Yes | 27 (28.4) | 21 (60) | |
| Loss of fatty hilum | <0.001 | ||
| No | 94 (98.9) | 20 (57.1) | |
| Yes | 1 (1.1) | 15 (42.9) | |
| Irregular margin | <0.001 | ||
| No | 93 (97.9) | 25 (71.4) | |
| Yes | 2 (2.1) | 10 (28.6) | |
| Rim sign | <0.001 | ||
| No | 93 (97.9) | 24 (68.6) | |
| Yes | 2 (2.1) | 11 (31.4) | |
| Asymmetry in either shape or number | <0.001 | ||
| No | 82 (86.3) | 8 (22.9) | |
| Yes | 13 (13.7) | 27 (77.1) |
| Variables | AUC (95% CI) | Cut off Value | p |
|---|---|---|---|
| Long diameter | 0.717 (0.631–0.792) | 10.65 (mm) | <0.001 |
| Short diameter | 0.786 (0.706–0.853) | 6.45 (mm) | <0.001 |
| Cortical thickness | 0.816 (0.739–0.879) | 4.35 (mm) | <0.001 |
| ADC value | 0.577 (0.487–0.663) | 1.193 (×10−3 mm2/s) | 0.147 |
| L/S ratio | 0.608 (0.519–0.692) | 2.15 | 0.045 |
| Variables | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Diagnostic Accuracy (%) | p |
|---|---|---|---|---|---|---|
| Long diameter | 71.4 | 62.1 | 85.5 | 41.0 | 64.6 | <0.001 |
| Short diameter | 65.7 | 84.2 | 60.5 | 87.0 | 79.2 | <0.001 |
| L/S ratio | 82.9 | 39.0 | 33.3 | 86.1 | 50.8 | |
| Cortical thickness | 60.0 | 89.5 | 67.7 | 85.9 | 81.5 | <0.001 |
| Eccentricity | 60.0 | 71.6 | 43.8 | 82.9 | 68.5 | <0.001 |
| Loss of fatty hilum | 42.9 | 99.0 | 93.8 | 82.5 | 83.9 | <0.001 |
| Irregular margin | 28.6 | 99.0 | 90.9 | 79.0 | 80.0 | <0.001 |
| Asymmetry in either shape or number | 80.0 | 76.8 | 56.0 | 91.3 | 83.9 | 0.012 |
| Rim sign | 31.4 | 97.9 | 84.6 | 79.5 | 80.0 | <0.001 |
| Final assessment | 77.1 | 93.3 | 79.4 | 92.5 | 86.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, P.; Park, C.S.; Park, G.E.; Kim, S.H.; Kim, H.S.; Oh, S.-J. Diagnostic Usefulness of Diffusion-Weighted MRI for Axillary Lymph Node Evaluation in Patients with Breast Cancer. Diagnostics 2023, 13, 513. https://doi.org/10.3390/diagnostics13030513
Cho P, Park CS, Park GE, Kim SH, Kim HS, Oh S-J. Diagnostic Usefulness of Diffusion-Weighted MRI for Axillary Lymph Node Evaluation in Patients with Breast Cancer. Diagnostics. 2023; 13(3):513. https://doi.org/10.3390/diagnostics13030513
Chicago/Turabian StyleCho, Pyeonghwa, Chang Suk Park, Ga Eun Park, Sung Hun Kim, Hyeon Sook Kim, and Se-Jeong Oh. 2023. "Diagnostic Usefulness of Diffusion-Weighted MRI for Axillary Lymph Node Evaluation in Patients with Breast Cancer" Diagnostics 13, no. 3: 513. https://doi.org/10.3390/diagnostics13030513
APA StyleCho, P., Park, C. S., Park, G. E., Kim, S. H., Kim, H. S., & Oh, S.-J. (2023). Diagnostic Usefulness of Diffusion-Weighted MRI for Axillary Lymph Node Evaluation in Patients with Breast Cancer. Diagnostics, 13(3), 513. https://doi.org/10.3390/diagnostics13030513