
Post-Dilatation of New-Generation Self-Expandable Transcatheter Aortic Valves Does Not Increase Atrioventricular Conduction Abnormalities
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
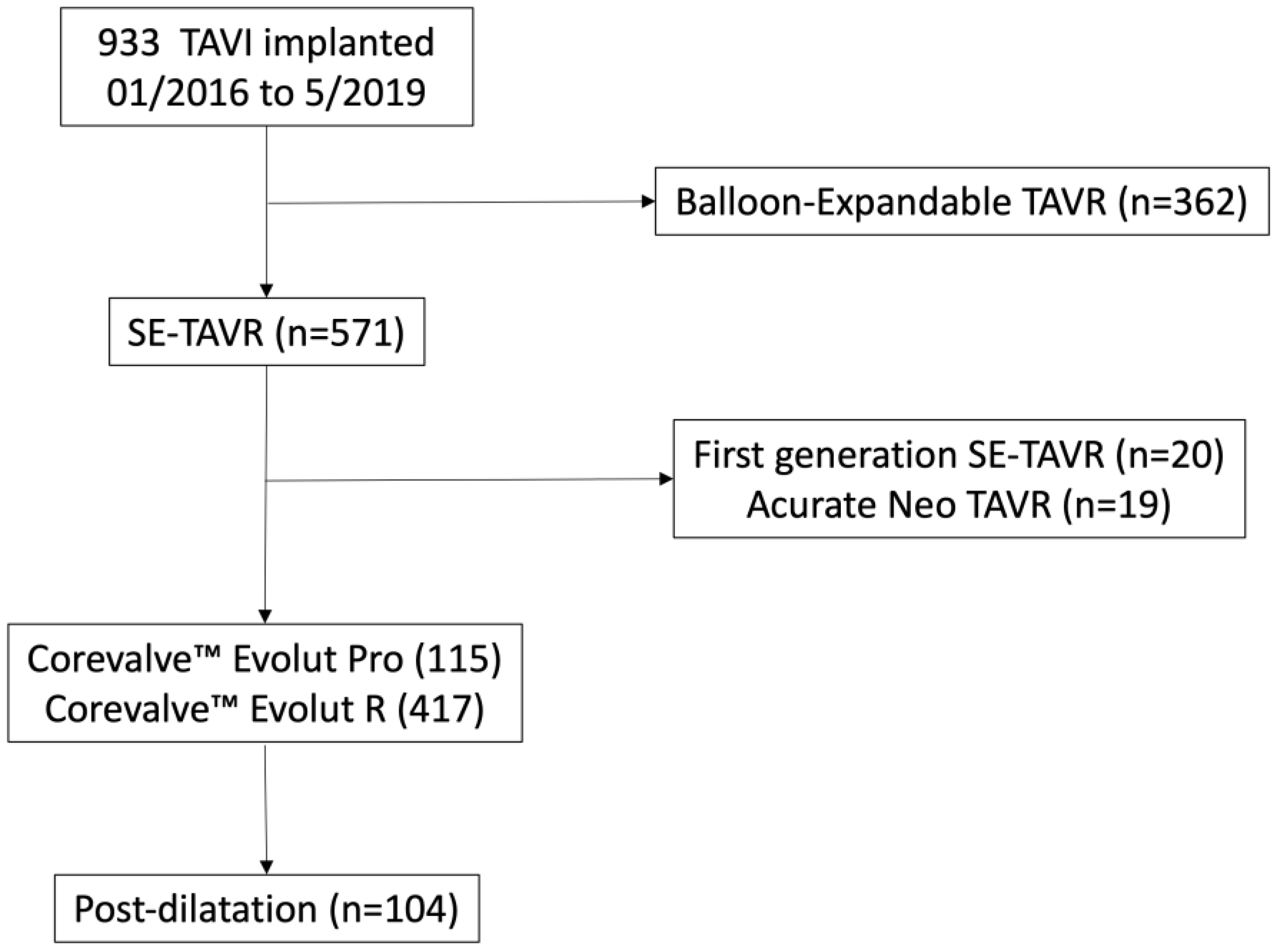
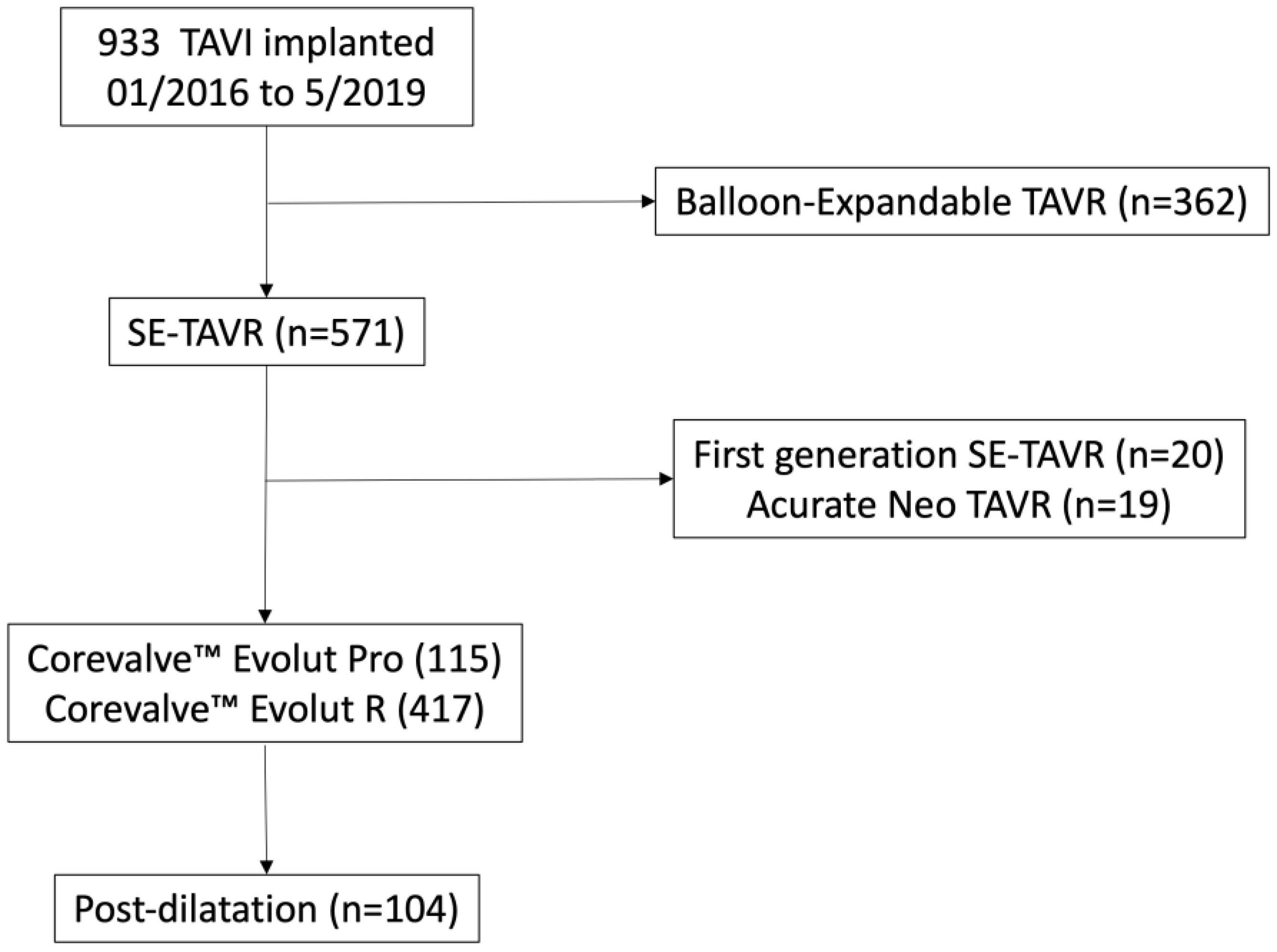
2.1. Study Population
2.2. TAVR Procedure and Data Collection
2.3. Outcomes: Electrical Conduction Disorders, Clinical Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Procedural Characteristics (Supplementary Table S1)
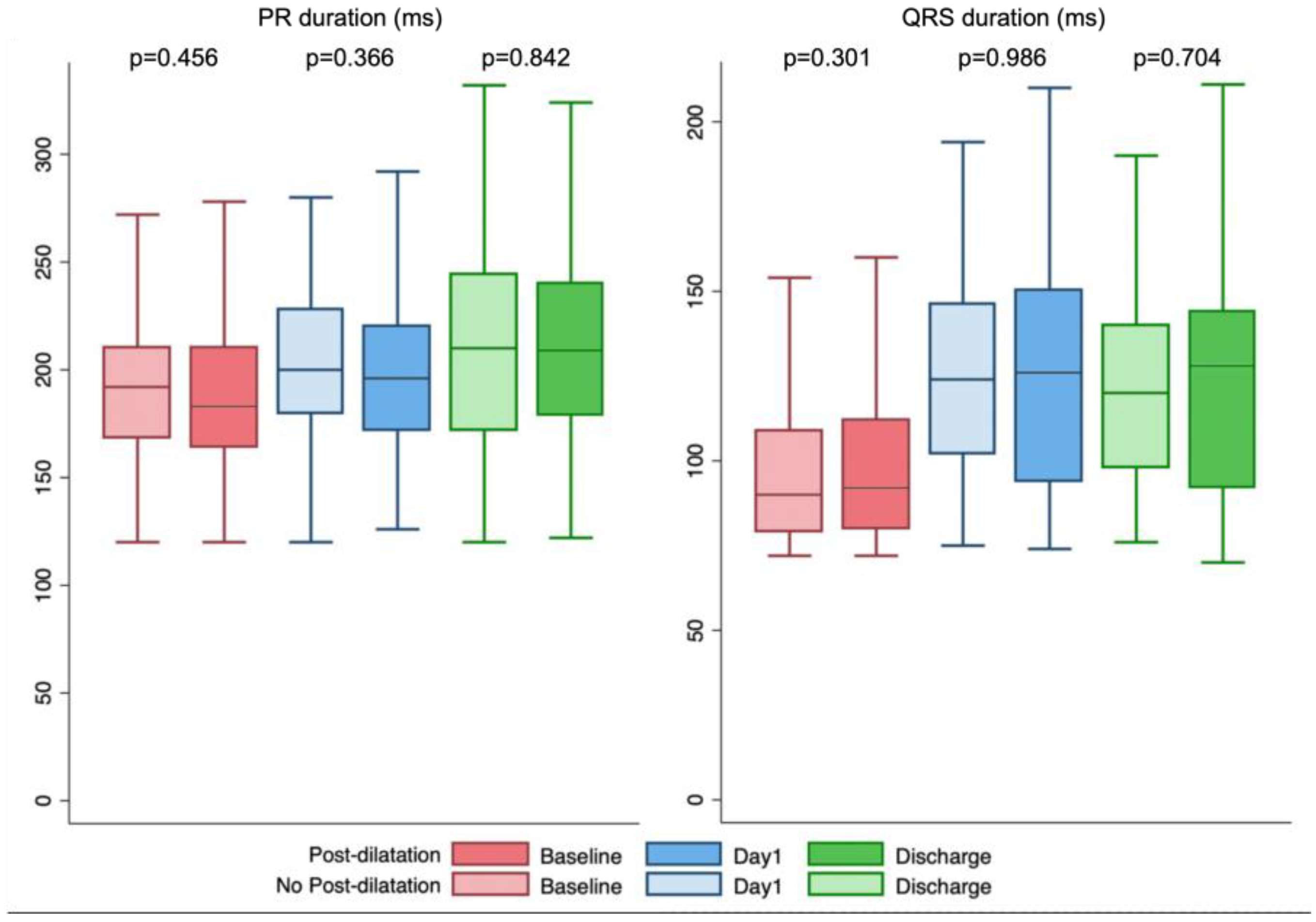
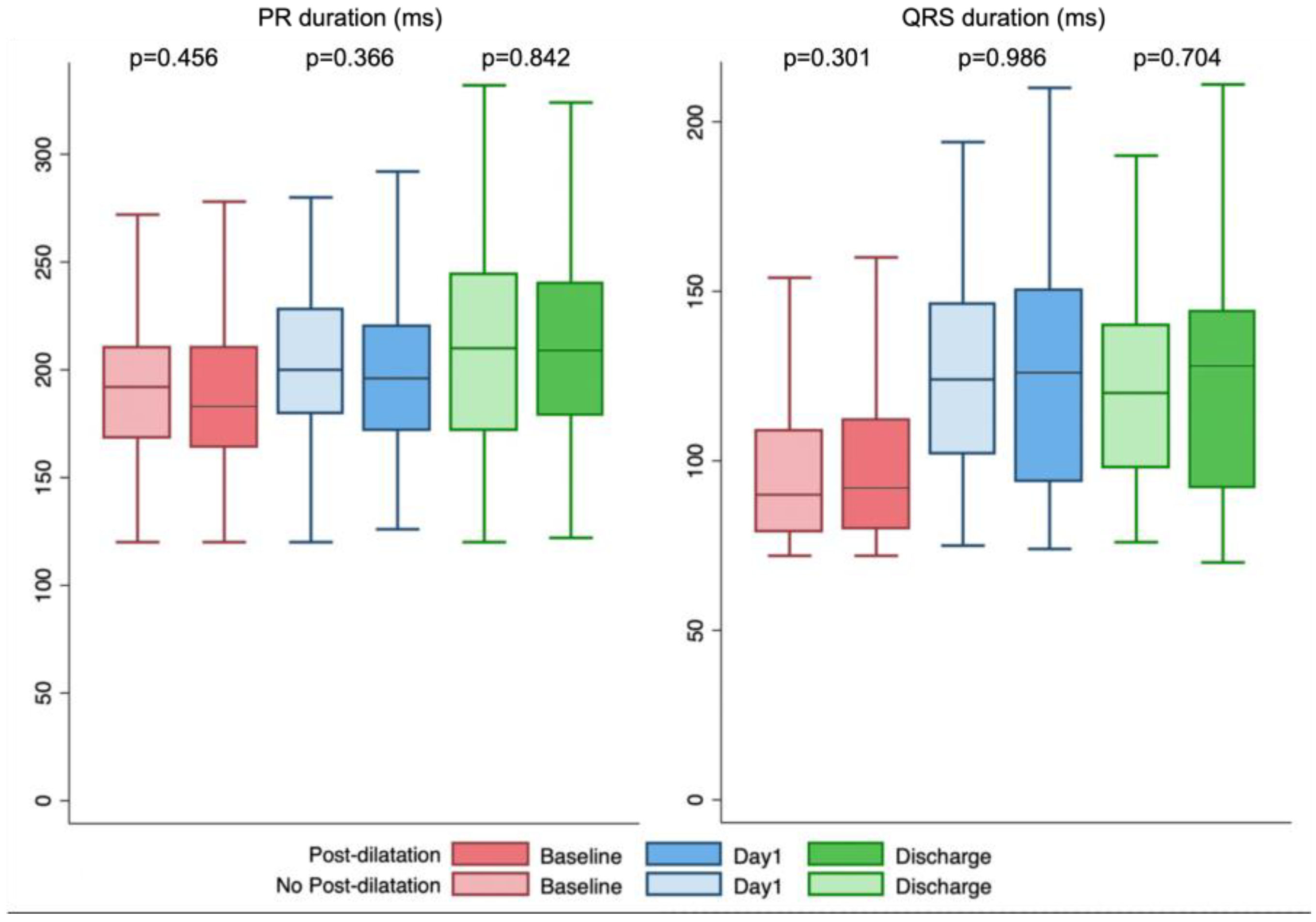
3.3. Conduction Abnormalities and Permanent Pacemaker Implantation (Table 2 and Table 3, Figure 2)

{kind=link}
{kind=link}
{kind=link}
| Total (n = 532) | No Post-Dilatation Group (n = 428) | Post-Dilatation Group (n = 104) | p-Value | |
|---|---|---|---|---|
| PR interval # (ms) | ||||
| Before TAVR | 191 ± 38 | 191 ± 37 | 195 ± 40 | 0.456 |
| Day 1 | 201 ± 41 | 200 ± 40 | 205 ± 44 | 0.366 |
| Discharge | 212 ± 48 | 212 ± 47 | 211 ± 50 | 0.842 |
| QRS length # (ms) | ||||
| Before TAVR | 100 ± 25 | 100 ± 25 | 97 ± 23 | 0.301 |
| Day 1 | 123 ± 30 | 123 ± 27 | 123 ± 31 | 0.986 |
| Discharge | 121 ± 30 | 121 ± 30 | 120 ± 26 | 0.704 |
| New permanent pacemaker implantation | 149 (28.0%) | 123 (28.7%) | 26 (25.0%) | 0.446 |
| Etiologies of pacemaker implantation | 0.294 | |||
| Sinus bradycardia | 5 (3.4%) | 3 (2.4%) | 2 (7.7%) | |
| Complete AV block or Mobitz 2 AV block | 107 (71.8%) | 87 (70.7%) | 20 (76.9%) | |
| LBBB and HV ≥ 70 ms | 30 (20.1%) | 26 (21.1%) | 4 (15.4%) | |
| Other abnormalities | 7 (4.7%) | 7 (5.7%) | 0 (0.0%) | |
| Timing of conduction abnormalities | 0.468 | |||
| During procedure | 53 (35.6%) | 44 (37.7%) | 9 (34.6%) | |
| ≤24 h | 35 (23.5%) | 14 (25.2%) | 4 (15.4%) | |
| >24 h | 61 (41.0%) | 48 (39.0%) | 13 (50.0%) |
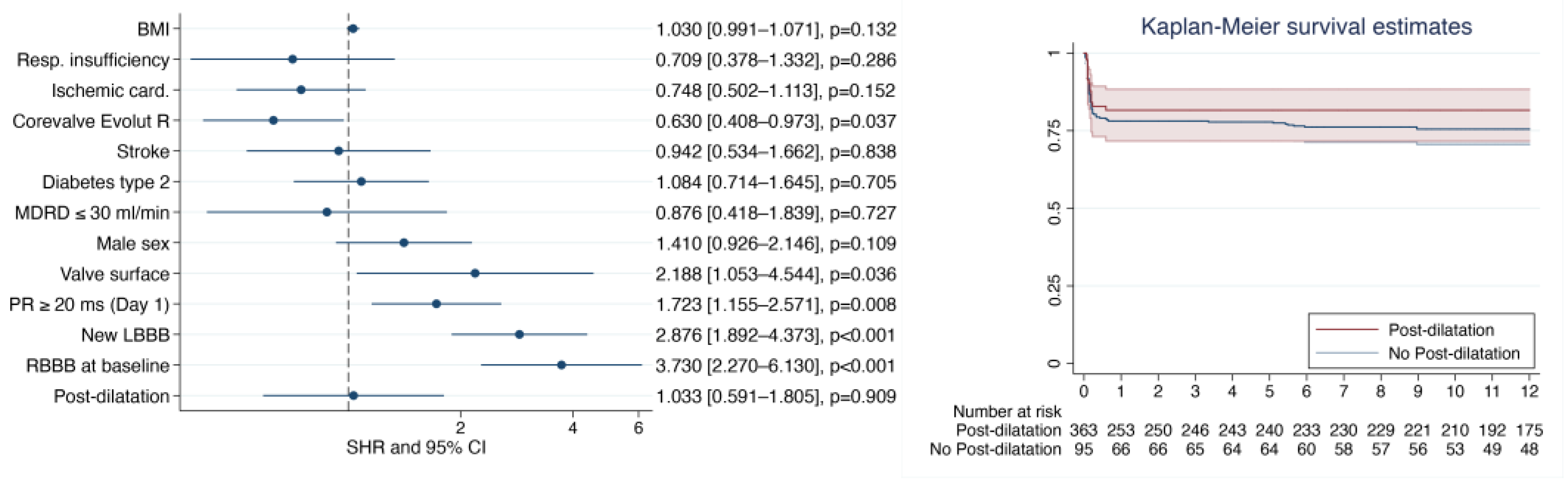
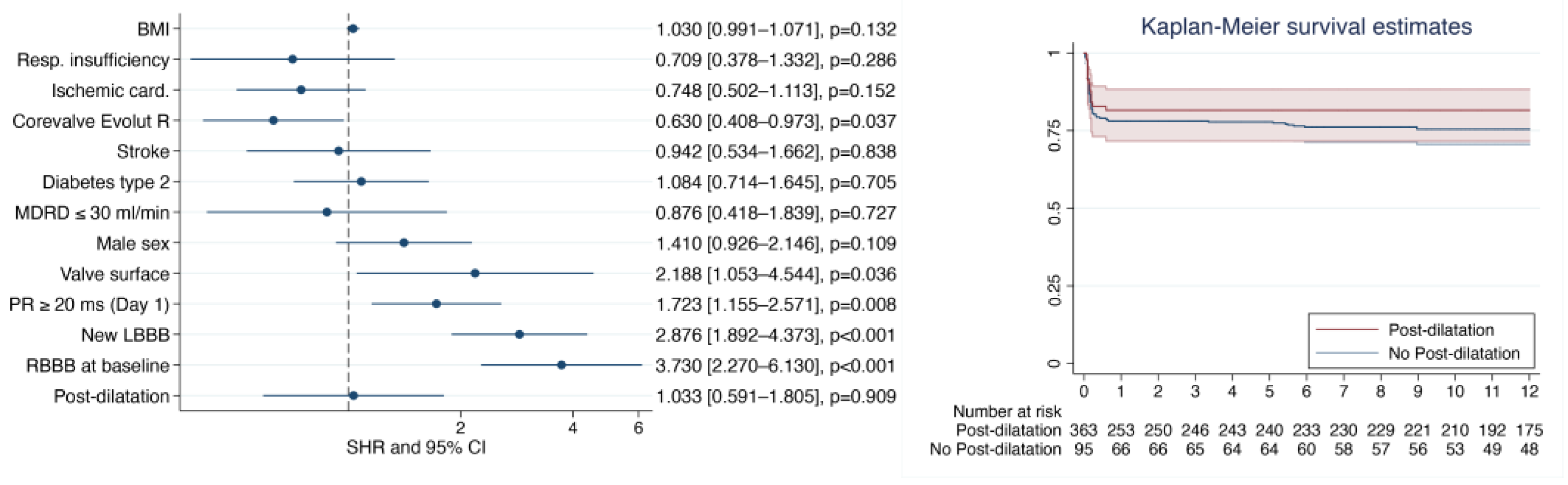
3.4. TAVR Clinical Outcomes (Supplementary Table S2)
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kodali, S.K.; Williams, M.R.; Smith, C.R.; Svensson, L.G.; Webb, J.G.; Makkar, R.R.; Fontana, G.P.; Dewey, T.M.; Thourani, V.H.; Pichard, A.D.; et al. Two-Year Outcomes after Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2012, 366, 1686–1695. [Google Scholar] [CrossRef] [Green Version]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Thourani, V.H.; Mack, M.J.; Kodali, S.K.; Kapadia, S.; Webb, J.G.; Yoon, S.-H.; Trento, A.; Svensson, L.G.; Herrmann, H.C.; et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 799–809. [Google Scholar] [CrossRef]
- Kodali, S.; Pibarot, P.; Douglas, P.S.; Williams, M.; Xu, K.; Thourani, V.; Rihal, C.S.; Zajarias, A.; Doshi, D.; Davidson, M.; et al. Paravalvular Regurgitation after Transcatheter Aortic Valve Replacement with the Edwards Sapien Valve in the PARTNER Trial: Characterizing Patients and Impact on Outcomes. Eur. Heart J. 2015, 36, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Forrest, J.K.; Kaple, R.K.; Tang, G.H.L.; Yakubov, S.J.; Nazif, T.M.; Williams, M.R.; Zhang, A.; Popma, J.J.; Reardon, M.J. Three Generations of Self-Expanding Transcatheter Aortic Valves: A Report From the STS/ACC TVT Registry. JACC Cardiovasc. Interv. 2020, 13, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Hellhammer, K.; Piayda, K.; Afzal, S.; Kleinebrecht, L.; Makosch, M.; Hennig, I.; Quast, C.; Jung, C.; Polzin, A.; Westenfeld, R.; et al. The Latest Evolution of the Medtronic CoreValve System in the Era of Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2018, 11, 2314–2322. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Adams, D.H.; Reardon, M.J.; Yakubov, S.J.; Kleiman, N.S.; Heimansohn, D.; Hermiller, J.; Hughes, G.C.; Harrison, J.K.; Coselli, J.; et al. Transcatheter Aortic Valve Replacement Using a Self-Expanding Bioprosthesis in Patients With Severe Aortic Stenosis at Extreme Risk for Surgery. J. Am. Coll. Cardiol. 2014, 63, 1972–1981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toutouzas, K.; Benetos, G.; Voudris, V.; Drakopoulou, M.; Stathogiannis, K.; Latsios, G.; Synetos, A.; Antonopoulos, A.; Kosmas, E.; Iakovou, I.; et al. Pre-Dilatation Versus No Pre-Dilatation for Implantation of a Self-Expanding Valve in All Comers Undergoing TAVR: The DIRECT Trial. JACC Cardiovasc. Interv. 2019, 12, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Seiffert, M.; Fujita, B.; Avanesov, M.; Lunau, C.; Schön, G.; Conradi, L.; Prashovikj, E.; Scholtz, S.; Börgermann, J.; Scholtz, W.; et al. Device Landing Zone Calcification and Its Impact on Residual Regurgitation after Transcatheter Aortic Valve Implantation with Different Devices. Eur. Heart J. – Cardiovasc. Imaging 2016, 17, 576–584. [Google Scholar] [CrossRef] [Green Version]
- Pollari, F.; Dell’Aquila, A.M.; Söhn, C.; Marianowicz, J.; Wiehofsky, P.; Schwab, J.; Pauschinger, M.; Hitzl, W.; Fischlein, T.; Pfeiffer, S. Risk Factors for Paravalvular Leak after Transcatheter Aortic Valve Replacement. J. Thorac. Cardiovasc. Surg. 2019, 157, 1406–1415.e3. [Google Scholar] [CrossRef] [Green Version]
- Nombela-Franco, L.; Barbosa Ribeiro, H.; Allende, R.; Urena, M.; Doyle, D.; Dumont, E.; Delarochellière, R.; Rodés-Cabau, J. Role of Balloon Postdilation Following Trancatheter Aortic Valve Implantation. Minerva Cardioangiol. 2013, 61, 499–512. [Google Scholar]
- Hahn, R.T.; Pibarot, P.; Webb, J.; Rodes-Cabau, J.; Herrmann, H.C.; Williams, M.; Makkar, R.; Szeto, W.Y.; Main, M.L.; Thourani, V.H.; et al. Outcomes with Post-Dilation Following Transcatheter Aortic Valve Replacement: The PARTNER I Trial (Placement of Aortic Transcatheter Valve). JACC Cardiovasc. Interv. 2014, 7, 781–789. [Google Scholar] [CrossRef] [Green Version]
- Auffret, V.; Puri, R.; Urena, M.; Chamandi, C.; Rodriguez-Gabella, T.; Philippon, F.; Rodés-Cabau, J. Conduction Disturbances After Transcatheter Aortic Valve Replacement: Current Status and Future Perspectives. Circulation 2017, 136, 1049–1069. [Google Scholar] [CrossRef]
- Barbanti, M.; Petronio, A.S.; Capodanno, D.; Ettori, F.; Colombo, A.; Bedogni, F.; De Marco, F.; De Carlo, M.; Fiorina, C.; Latib, A.; et al. Impact of Balloon Post-Dilation on Clinical Outcomes after Transcatheter Aortic Valve Replacement with the Self-Expanding CoreValve Prosthesis. JACC Cardiovasc. Interv. 2014, 7, 1014–1021. [Google Scholar] [CrossRef]
- Nombela-Franco, L.; Rodés-Cabau, J.; DeLarochellière, R.; Larose, E.; Doyle, D.; Villeneuve, J.; Bergeron, S.; Bernier, M.; Amat-Santos, I.J.; Mok, M.; et al. Predictive Factors, Efficacy, and Safety of Balloon Post-Dilation After Transcatheter Aortic Valve Implantation With a Balloon-Expandable Valve. JACC Cardiovasc. Interv. 2012, 5, 499–512. [Google Scholar] [CrossRef] [Green Version]
- Harrison, J.K.; Hughes, G.C.; Reardon, M.J.; Stoler, R.; Grayburn, P.; Hebeler, R.; Liu, D.; Chang, Y.; Popma, J.J. Balloon Post-Dilation Following Implantation of a Self-Expanding Transcatheter Aortic Valve Bioprosthesis. JACC Cardiovasc. Interv. 2017, 10, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Lefevre, T.; Van Belle, E.; Eltchaninoff, H.; Iung, B.; Koning, R.; Motreff, P.; Leprince, P.; Verhoye, J.P.; Manigold, T.; et al. Temporal Trends in Transcatheter Aortic Valve Replacement in France: FRANCE 2 to FRANCE TAVI. J. Am. Coll. Cardiol. 2017, 70, 42–55. [Google Scholar] [CrossRef]
- Gilard, M.; Eltchaninoff, H.; Iung, B.; Donzeau-Gouge, P.; Chevreul, K.; Fajadet, J.; Leprince, P.; Leguerrier, A.; Lievre, M.; Prat, A.; et al. Registry of Transcatheter Aortic-Valve Implantation in High-Risk Patients. N. Engl. J. Med. 2012, 366, 1705–1715. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.-A.; et al. Updated Standardized Endpoint Definitions for Transcatheter Aortic Valve Implantation: The Valve Academic Research Consortium-2 Consensus Document (VARC-2). Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2012, 42, S45–S60. [Google Scholar] [CrossRef]
- Sellers, R.D.; Levy, M.J.; Amplatz, K.; Lillehei, C.W. Left Retrograde Cardioangiography in Acquired Cardiac Disease. Am. J. Cardiol. 1964, 14, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Sinning, J.-M.; Hammerstingl, C.; Vasa-Nicotera, M.; Adenauer, V.; Lema Cachiguango, S.J.; Scheer, A.-C.; Hausen, S.; Sedaghat, A.; Ghanem, A.; Müller, C.; et al. Aortic Regurgitation Index Defines Severity of Peri-Prosthetic Regurgitation and Predicts Outcome in Patients after Transcatheter Aortic Valve Implantation. J. Am. Coll. Cardiol. 2012, 59, 1134–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massoullié, G.; Bordachar, P.; Irles, D.; Caussin, C.; Da Costa, A.; Defaye, P.; Jean, F.; Mechulan, A.; Mondoly, P.; Souteyrand, G.; et al. Prognosis Assessment of Persistent Left Bundle Branch Block after TAVI by an Electrophysiological and Remote Monitoring Risk-Adapted Algorithm: Rationale and Design of the Multicentre LBBB–TAVI Study. BMJ Open 2016, 6, e010485. [Google Scholar] [CrossRef] [Green Version]
- Mickey, R.M.; Greenland, S. The Impact of Confounder Selection Criteria on Effect Estimation. Am. J. Epidemiol. 1989, 129, 125–137. [Google Scholar] [CrossRef]
- Jilaihawi, H.; Zhao, Z.; Du, R.; Staniloae, C.; Saric, M.; Neuburger, P.J.; Querijero, M.; Vainrib, A.; Hisamoto, K.; Ibrahim, H.; et al. Minimizing Permanent Pacemaker Following Repositionable Self-Expanding Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 1796–1807. [Google Scholar] [CrossRef]
- Athappan, G.; Patvardhan, E.; Tuzcu, E.M.; Svensson, L.G.; Lemos, P.A.; Fraccaro, C.; Tarantini, G.; Sinning, J.-M.; Nickenig, G.; Capodanno, D.; et al. Incidence, Predictors, and Outcomes of Aortic Regurgitation after Transcatheter Aortic Valve Replacement: Meta-Analysis and Systematic Review of Literature. J. Am. Coll. Cardiol. 2013, 61, 1585–1595. [Google Scholar] [CrossRef]
- Tamburino, C.; Capodanno, D.; Ramondo, A.; Petronio, A.S.; Ettori, F.; Santoro, G.; Klugmann, S.; Bedogni, F.; Maisano, F.; Marzocchi, A.; et al. Incidence and Predictors of Early and Late Mortality after Transcatheter Aortic Valve Implantation in 663 Patients with Severe Aortic Stenosis. Circulation 2011, 123, 299–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giustino, G.; Van der Boon, R.; Molina-Martin de Nicolas, J.; Dumonteil, N.; Chieffo, A.; de Jaegere, P.; Tchetche, D.; Marcheix, B.; Millischer, D.; Cassagneau, R.; et al. Impact of Permanent Pacemaker on Mortality after Transcatheter Aortic Valve Implantation: The PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration) Pacemaker Substudy. EuroIntervention 2016, 12, 1185–1193. [Google Scholar] [CrossRef]
- Manoharan, G.; Walton, A.S.; Brecker, S.J.; Pasupati, S.; Blackman, D.J.; Qiao, H.; Meredith, I.T. Treatment of Symptomatic Severe Aortic Stenosis With a Novel Resheathable Supra-Annular Self-Expanding Transcatheter Aortic Valve System. JACC Cardiovasc. Interv. 2015, 8, 1359–1367. [Google Scholar] [CrossRef] [Green Version]
- Forrest, J.K.; Mangi, A.A.; Popma, J.J.; Khabbaz, K.; Reardon, M.J.; Kleiman, N.S.; Yakubov, S.J.; Watson, D.; Kodali, S.; George, I.; et al. Early Outcomes With the Evolut PRO Repositionable Self-Expanding Transcatheter Aortic Valve With Pericardial Wrap. JACC Cardiovasc. Interv. 2018, 11, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Grube, E.; Van Mieghem, N.M.; Bleiziffer, S.; Modine, T.; Bosmans, J.; Manoharan, G.; Linke, A.; Scholtz, W.; Tchétché, D.; Finkelstein, A.; et al. Clinical Outcomes With a Repositionable Self-Expanding Transcatheter Aortic Valve Prosthesis: The International FORWARD Study. J. Am. Coll. Cardiol. 2017, 70, 845–853. [Google Scholar] [CrossRef] [PubMed]
| Total (n = 532) | No Post-Dilatation Group (n = 428) | Post-Dilatation Group (n = 104) | p-Value | |
|---|---|---|---|---|
| Age, yrs | 82 ± 6 | 82 ± 6 | 83 ± 6 | 0.361 |
| Female, no. (%) | 260 (48.8%) | 212 (49.5%) | 48 (46.1%) | 0.536 |
| Logistic EuroSCORE | 13.8 ± 8.2 | 13.9 ± 8.5 | 13.6 ± 7.3 | 0.717 |
| Logistic EuroSCORE II | 4.2 ± 3.0 | 4.2 ± 3.2 | 4.0 ± 2.1 | 0.528 |
| BMI (kg/m2) | 27.1 ± 5.2 | 27.3 ± 5.3 | 25.7 ± 4.2 | 0.001 |
| COPD, no. (%) | 65 (12.2%) | 57 (13.3%) | 8 (7.7%) | 0.116 |
| NYHA (Status) | 2.3 ± 0.6 | 2.2 ± 0.6 | 2.3 ± 0.6 | 0.033 |
| AF, no. (%) | 114 (21.4%) | 97 (22.6%) | 17 (16.3%) | 0.159 |
| GFR median (ml/min/1.72 m2) | 52.2 ± 19.7 | 52.7 ± 20.5 | 48.6 ± 16.9 | 0.032 |
| Diabetes mellitus, no. (%) | 161 (30.2%) | 131 (30.6%) | 30 (28.9%) | 0.828 |
| Previous PPI, no. (%) | 45 (8.4%) | 42 (9.8%) | 3 (2.9%) | 0.023 |
| Stroke /TIA, no. (%) | 44 (8.3%) | 34 (7.9%) | 10 (9.6%) | 0.579 |
| Prior cardiac surgery, no. (%) | 48 (9.1%) | 40 (9.3%) | 8 (7.7%) | 0.469 |
| Prior PCI, no. (%) | 205 (38.6 %) | 170 (39.8%) | 35 (34.0%) | 0.405 |
| Echocardiographic assessment | ||||
| LVEF (%) | 60 ± 11 | 59 ± 11 | 60 ± 11 | 0.258 |
| Aortic valve area (cm2) | 0.73 ± 0.22 | 0.74 ± 0.22 | 0.64 ± 0.22 | <0.001 |
| Mean gradient (mmHg) | 45 ± 15 | 43 ± 13 | 55 ± 18 | <0.001 |
| Moderate Aortic regurgitation, no. (%) | 67 (12.6%) | 54 (12.6%) | 13 (12.5%) | 0.974 |
| Moderate Mitral regurgitation, no. (%) | 88 (16.5%) | 67 (15.5%) | 21 (20.4%) | 0.688 |
| Aortic annular diameter (mm, CT) | 23.8 ± 2.4 | 23.8 ± 2.4 | 23.8 ± 2.1 | 0.844 |
| ECG Pre-TAVI | ECG J1-TAVI | ECG Discharge-TAVI | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (523) | No Post-Dilatation (423) | Post-Dilatation (100) | p Value | Total (515) | No Post-Dilatation (417) | Post-Dilatation (98) | p Value | Total (498) | No Post-Dilatation (401) | Post-Dilatation (97) | p Value | |
| Sinus rhythm (%) | 410 (78.4%) | 328 (77.5%) | 82 (82%) | 0.631 | 371 (72%) | 297 (71.2%) | 74 (75.5%) | 0.726 | 363 (72.9%) | 290 (72.3%) | 73 (75.3%) | 0.632 |
| Heart rate (bpm) | 72 ± 14 | 72 ± 15 | 72 ± 14 | 0.647 | 77 ± 15 | 78 ± 16 | 74 ± 14 | 0.028 | 76 ± 14 | 76 ± 14 | 76 ± 15 | 0.897 |
| PR intervals (ms) | 192 ± 38 | 191 ± 37 | 195 ± 40 | 0.458 | 201 ± 41 | 200 ± 40 | 205 ± 44 | 0.367 | 212 ± 48 | 212 ± 47 | 211 ± 50 | 0.842 |
| Type 1 AVB (%) | 154 (29.4%) | 122 (28.8%) | 32 (32%) | 0.85 | 179 (34.8%) | 138 (33.1%) | 41 (41.8%) | 0.203 | 189 (38%) | 150 (37.4%) | 39 (40.2%) | 0.878 |
| QRS intervals (ms) * | 100 ± 25 | 100 ± 25 | 97 ± 23 | 0.302 | 123 ± 30 | 123 ± 31 | 123 ± 27 | 0.985 | 121 ± 30 | 121 ± 30 | 120 ± 27 | 0.704 |
| QTc (ms) | 423 ± 31 | 424 ± 32 | 421 ± 28 | 0.433 | 463 ± 47 | 464 ± 47 | 460 ± 46 | 0.524 | 437 ± 40 | 438 ± 39 | 433 ± 41 | 0.29 |
| Hemiblock | ||||||||||||
| HAFB (%) | 83 (15.9%) | 63 (14.9%) | 20 (20%) | 0.255 | 48 (9.3%) | 40 (9.3%) | 8 (1.6%) | 0.598 | 39 (7.8%) | 39 (9.7%) | 8 (8.2%) | 0.875 |
| HPFB (%) | 4 (0.8%) | 4 (0.9%) | 0 (0%) | 0.322 | 9 (1.7%) | 7 (1.7%) | 2 (0.4%) | 0.838 | 1 (0.2%) | 1 (0.2%) | 1 (1%) | 0.042 |
| QRS type | ||||||||||||
| Narrow QRS (%) | ||||||||||||
| RBBB (%) | 26 (5%) | 22 (5.2%) | 4 (4%) | 0.583 | 44 (8.5%) | 38 (9.1%) | 6 (6.1%) | 0.302 | 27 (5.4%) | 27 (6.7%) | 5 (5.2%) | 0.89 |
| LBBB (%) | 64 (12.2%) | 52 (12.3%) | 12 (12%) | 0.864 | 184 (35.7%) | 147 (35.3%) | 37 (37.7%) | 0.813 | 179 (35.9%) | 179 (44.6%) | 37 (38.1%) | 0.642 |
| NICD (%) | 17 (3.3%) | 16 (3.8%) | 1 (1%) | 0.149 | 12 (2.3%) | 10 (2.4%) | 2 (2.04%) | 0.799 | 14 (2.8%) | 14 (3.5%) | 3 (3.1%) | 0.857 |
| Paced (%) | 22 (4.2%) | 21 (5%) | 1 (1%) | 0.07 | 67 (13%) | 56 (13.4%) | 11 (11.2%) | 0.489 | 102 (20.5%) | 102 (25.4%) | 16 (16.5%) | 0.274 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massoullié, G.; Combaret, N.; Souteyrand, G.; Salazard, J.P.; Pereira, B.; Jean, F.; Motreff, P.; Taghli-Lamallem, O.; Clerfond, G.; Eschalier, R. Post-Dilatation of New-Generation Self-Expandable Transcatheter Aortic Valves Does Not Increase Atrioventricular Conduction Abnormalities. Diagnostics 2023, 13, 427. https://doi.org/10.3390/diagnostics13030427
Massoullié G, Combaret N, Souteyrand G, Salazard JP, Pereira B, Jean F, Motreff P, Taghli-Lamallem O, Clerfond G, Eschalier R. Post-Dilatation of New-Generation Self-Expandable Transcatheter Aortic Valves Does Not Increase Atrioventricular Conduction Abnormalities. Diagnostics. 2023; 13(3):427. https://doi.org/10.3390/diagnostics13030427
Chicago/Turabian StyleMassoullié, Grégoire, Nicolas Combaret, Géraud Souteyrand, Jean Pascal Salazard, Bruno Pereira, Frédéric Jean, Pascal Motreff, Ouarda Taghli-Lamallem, Guillaume Clerfond, and Romain Eschalier. 2023. "Post-Dilatation of New-Generation Self-Expandable Transcatheter Aortic Valves Does Not Increase Atrioventricular Conduction Abnormalities" Diagnostics 13, no. 3: 427. https://doi.org/10.3390/diagnostics13030427
APA StyleMassoullié, G., Combaret, N., Souteyrand, G., Salazard, J. P., Pereira, B., Jean, F., Motreff, P., Taghli-Lamallem, O., Clerfond, G., & Eschalier, R. (2023). Post-Dilatation of New-Generation Self-Expandable Transcatheter Aortic Valves Does Not Increase Atrioventricular Conduction Abnormalities. Diagnostics, 13(3), 427. https://doi.org/10.3390/diagnostics13030427