
Evaluation of a Point-of-Need Molecular Diagnostic Tool Coupled with Rapid DNA Extraction Methods for Visceral Leishmaniasis

 , ,
, ,  , , , , ,
, , , , , 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sites and Populations
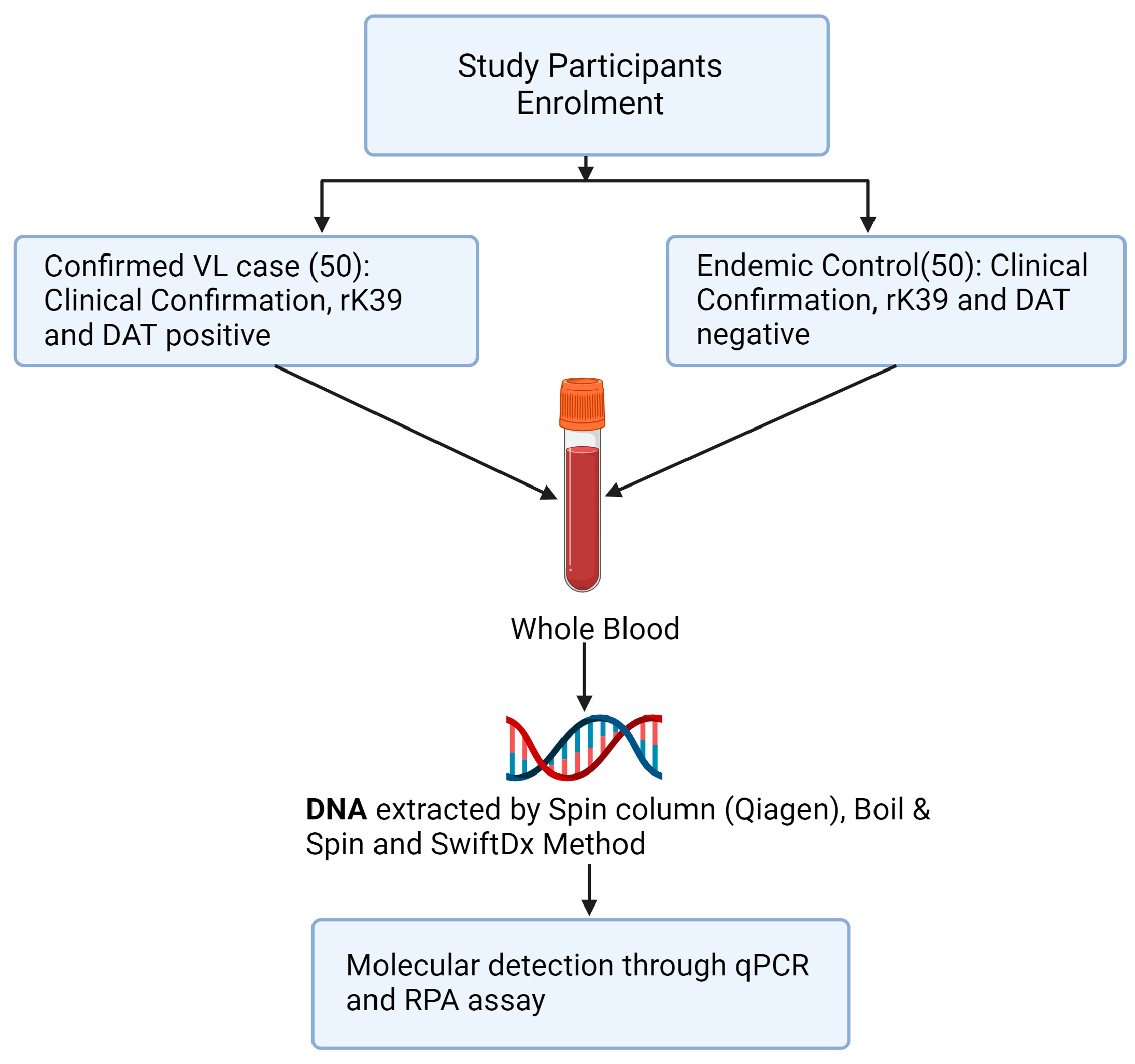
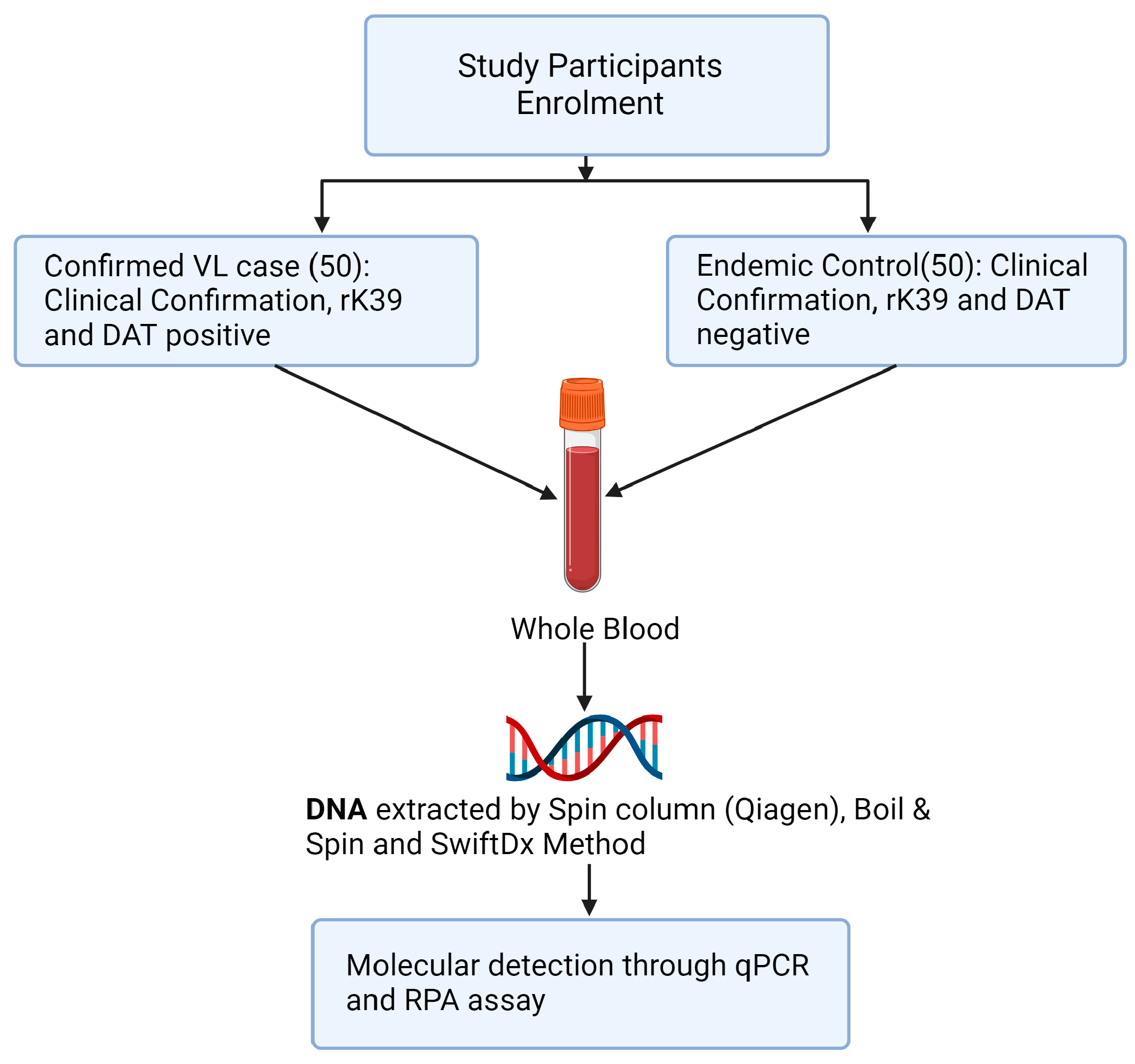
2.2. Study Design
2.3. Sample Collection and Storage
2.4. DNA Extraction from Clinical Specimens following Three DNA Extraction Methods
2.4.1. Qiagen DNA Extraction Method
2.4.2. SwiftDx DNA Extraction Method
2.4.3. Boil and Spin DNA Extraction Method
2.5. DNA Purity and Concentration
2.6. Molecular Detection of Leishmania Donovani DNA
2.6.1. Recombinase Polymerase Amplification (RPA) Assay
2.6.2. Real-Time PCR (qPCR)
2.7. Statistical Analysis
3. Results
3.1. Descriptive Characteristics of Study Participants
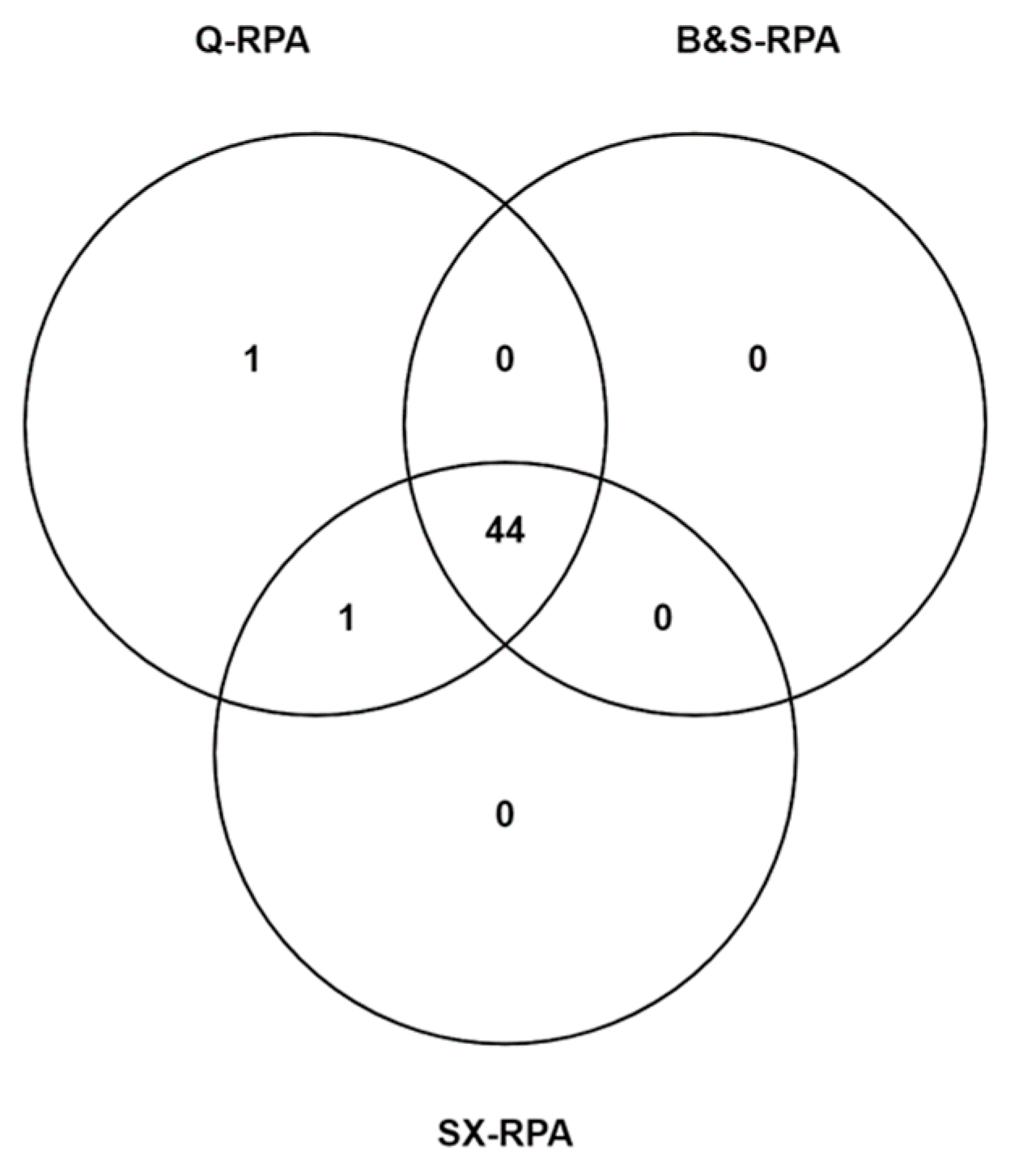
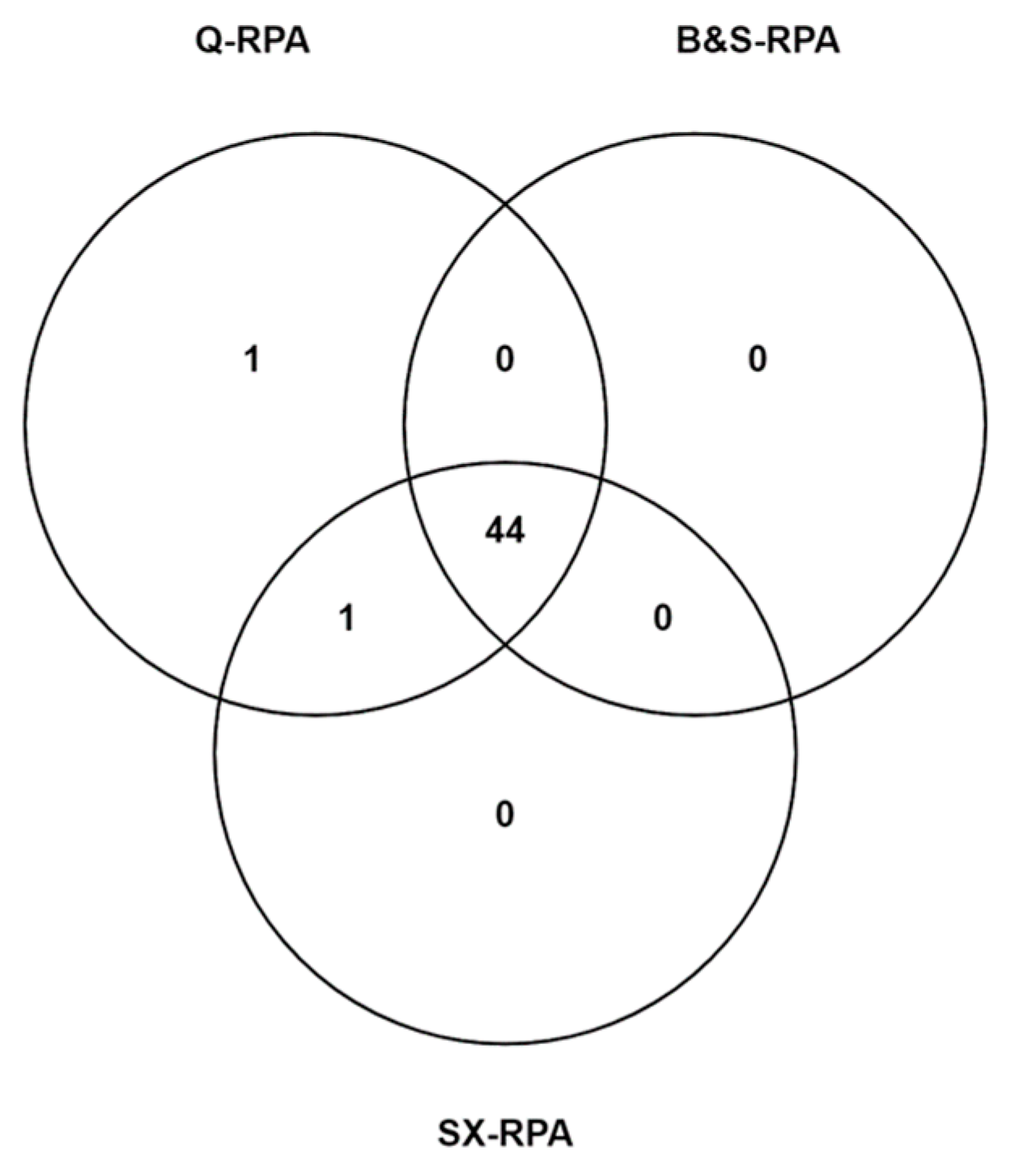
3.2. Diagnostic Performance of Molecular Assays with Different Extraction Methods
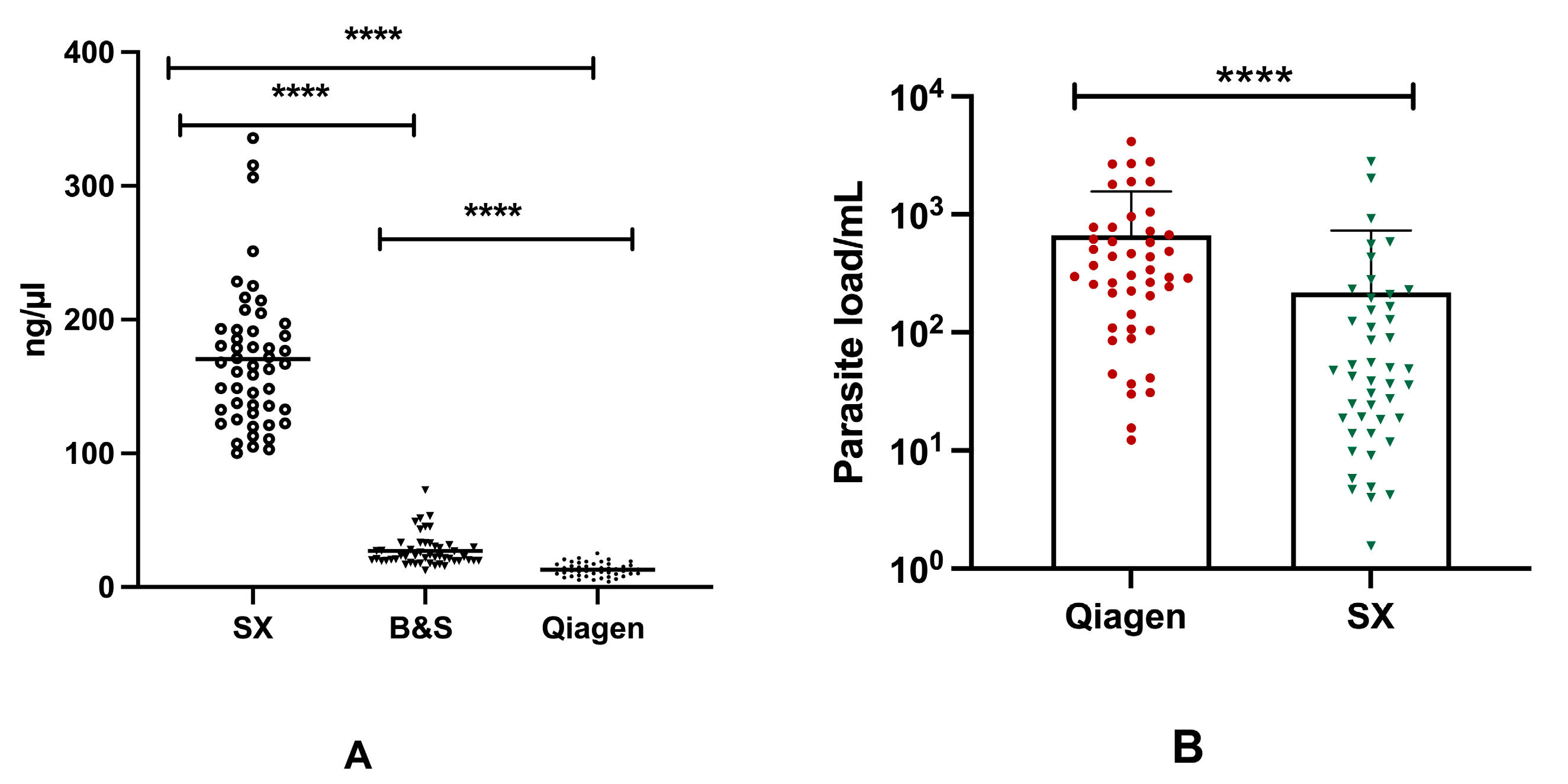
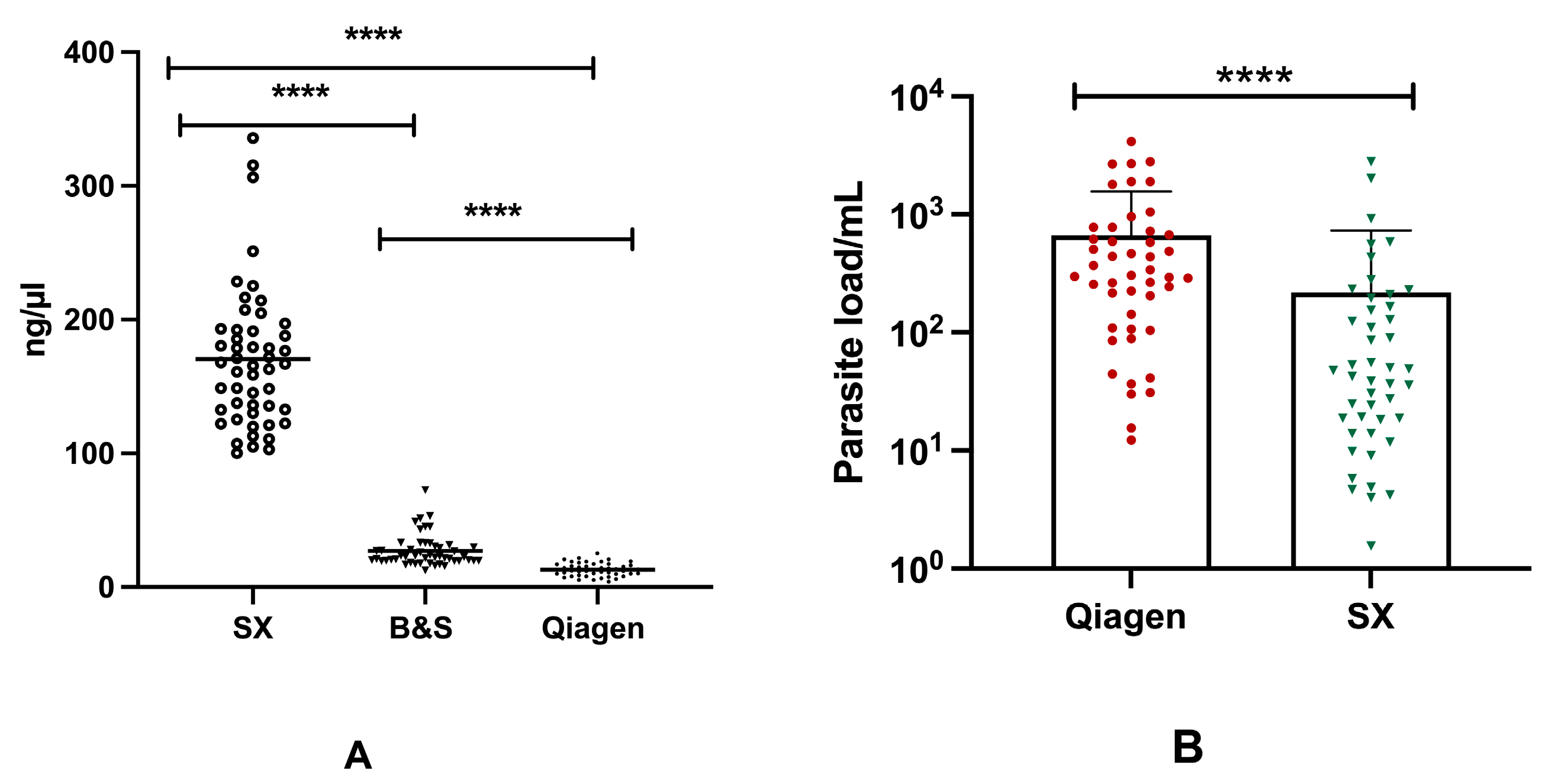
3.3. Effect of DNA Yields on Enumeration of Parasitemia through Molecular Methods
3.4. Comparative Analysis of Different DNA Extraction Methods
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chappuis, F.; Sundar, S.; Hailu, A.; Ghalib, H.; Rijal, S.; Peeling, R.W.; Boelaert, M. Visceral leishmaniasis: What are the needs for diagnosis, treatment and control? Nat. Rev. Microbiol. 2007, 5, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Wamai, R.G.; Kahn, J.; McGloin, J.; Ziaggi, G. Visceral leishmaniasis: A global overview. J. Glob. Health Sci. 2020, 2, e3. [Google Scholar] [CrossRef]
- Bi, K.; Chen, Y.; Zhao, S.; Kuang, Y.; Wu, C.-H.J. Current Visceral Leishmaniasis Research: A Research Review to Inspire Future Study. BioMed Res. Int. 2018, 2018, 9872095. [Google Scholar] [CrossRef]
- Selvapandiyan, A.; Croft, S.L.; Rijal, S.; Nakhasi, H.L.; Ganguly, N.K. Innovations for the elimination and control of visceral leishmaniasis. PLoS Neglected Trop. Dis. 2019, 13, e0007616. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.A.; Ducker, C.; Argaw, D.; King, J.D.; Solomon, A.W.; Biamonte, M.A.; Coler, R.N.; Cruz, I.; Lejon, V.; Levecke, B.; et al. Diagnostics and the neglected tropical diseases roadmap: Setting the agenda for 2030. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, E.E.; Alves, F.; Rijal, S.; Arana, B.; Alvar, J. Post-kala-azar dermal leishmaniasis in the Indian subcontinent: A threat to the South-East Asia Region Kala-azar Elimination Programme. PLoS Neglected Trop. Dis. 2017, 11, e0005877. [Google Scholar] [CrossRef]
- Sundar, S.R.M. Laboratory diagnosis of visceral leishmaniasis. Clin. Diagn. Lab. Immunol. 2002, 9, 951–958. [Google Scholar] [CrossRef]
- Thakur, S.; Joshi, J.; Kaur, S. Leishmaniasis diagnosis: An update on the use of parasitological, immunological and molecular methods. J. Parasit. Dis. 2020, 44, 253–272. [Google Scholar] [CrossRef]
- Reimão, J.Q.; Coser, E.M.; Lee, M.R.; Coelho, A.C. Laboratory Diagnosis of Cutaneous and Visceral Leishmaniasis: Current and Future Methods. Microorganisms 2020, 8, 1632. [Google Scholar] [CrossRef]
- Cota, G.F.; de Sousa, M.R.; Demarqui, F.N.; Rabello, A. The Diagnostic Accuracy of Serologic and Molecular Methods for Detecting Visceral Leishmaniasis in HIV Infected Patients: Meta-Analysis. PLoS Neglected Trop. Dis. 2012, 6, e1665. [Google Scholar] [CrossRef]
- Srividya, G.; Kulshrestha, A.; Singh, R.; Salotra, P. Diagnosis of visceral leishmaniasis: Developments over the last decade. Parasitol. Res. 2012, 110, 1065–1078. [Google Scholar] [CrossRef]
- Ejazi, S.A.; Bhattacharya, P.; Bakhteyar MA, K.; Mumtaz, A.A.; Pandey, K.; Das VN, R.; Ali, N. Noninvasive Diagnosis of Visceral Leishmaniasis: Development and Evaluation of Two Urine-Based Immunoassays for Detection of Leishmania donovani Infection in India. PLoS Negl. Trop. Dis. 2016, 10, e0005035. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, E.; Moreno, J. Editorial: Biomarkers in Leishmaniasis. Front. Cell. Infect. Microbiol. 2019, 9, 388. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Sivakumar, R. Recent advances in the diagnosis of leishmaniasis. J. Postgrad. Med. 2003, 49, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Salotra, P.; Singh, R. Challenges in the diagnosis of post kala-azar dermal leishmaniasis. Indian J. Med. Res. 2006, 123, 295–310. [Google Scholar]
- Mondal, D.; Ghosh, P.; Khan, A.A.; Hossain, F.; Böhlken-Fascher, S.; Matlashewski, G.; Kroeger, A.; Olliaro, P.; El Wahed, A.A. Mobile suitcase laboratory for rapid detection of Leishmania donovani using recombinase polymerase amplification assay. Parasites Vectors 2016, 9, 281. [Google Scholar] [CrossRef]
- Adams, E.R.; Versteeg, I.; Leeflang, M.M.G. Systematic Review into Diagnostics for Post-Kala-Azar Dermal Leishmaniasis (PKDL). J. Trop. Med. 2013, 2013, 150746. [Google Scholar] [CrossRef]
- Ghosh, P.; Sharma, A.; Bhattarai, N.R.; Abhishek, K.; Nisansala, T.; Kumar, A.; Abd El Wahed, A. A multi-country, single-blinded, phase 2 study to evaluate a point-of-need system for rapid detection of leishmaniasis and its implementation in endemic settings. Microorganisms 2021, 9, 588. [Google Scholar] [CrossRef]
- Batalini, L.; Castro, S.; Souto, C.; Neitzke-Abreu, H.; Lima-Junior, M. Evaluation of DNA Extraction Methods for Detection of Leishmania by Polymerase Chain Reaction. Am. J. Mol. Biol. 2020, 10, 265–272. [Google Scholar] [CrossRef]
- Paul, R.; Ostermann, E.; Wei, Q. Advances in point-of-care nucleic acid extraction technologies for rapid diagnosis of human and plant diseases. Biosens. Bioelectron. 2020, 169, 112592. [Google Scholar] [CrossRef]
- Gunaratna, G.; Manamperi, A.; Böhlken-Fascher, S.; Wickremasinge, R.; Gunawardena, K.; Yapa, B.; Pathirana, N.; Pathirana, H.; de Silva, N.; Sooriyaarachchi, M.; et al. Evaluation of rapid extraction and isothermal amplification techniques for the detection of Leishmania donovani DNA from skin lesions of suspected cases at the point of need in Sri Lanka. Parasites Vectors 2018, 11, 665. [Google Scholar] [CrossRef]
- Chowdhury, R.; Ghosh, P.; Khan, M.; Ashfaq, A.; Hossain, F.; Faisal, K.; Nath, R.; Baker, J.; El Wahed, A.A.; Maruf, S.; et al. Evaluation of rapid extraction methods coupled with a recombinase polymerase amplification assay for point-of-need diagnosis of post-kala-azar dermal leishmaniasis. Trop. Med. Infect. Dis. 2020, 5, 95. [Google Scholar] [CrossRef]
- Hopkins, H.; González, I.J.; Polley, S.D.; Angutoko, P.; Ategeka, J.; Asiimwe, C.; Bell, D. Highly Sensitive Detection of Malaria Parasitemia in a Malaria-Endemic Setting: Performance of a New Loop-Mediated Isothermal Ampli fi cation Kit in a Remote Clinic in Uganda. J. Infect. Dis. 2013, 208, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, M.; Ali, S.S.; Boshara, S.A.; Albertini, A.; Monnerat, S.; Bessell, P.; Mori, Y.; Kubota, Y.; Ndung’u, J.M.; Cruz, I. Sensitive and less invasive confirmatory diagnosis of visceral leishmaniasis in Sudan using loop-mediated isothermal amplification (LAMP). PLoS Negl. Trop. Dis. 2018, 12, e0006264. [Google Scholar] [CrossRef] [PubMed]
- Hossain, F.; Picado, A.; Owen, S.I.; Ghosh, P.; Chowdhury, R.; Maruf, S.; Khan, M.A.A.; Rashid, M.U.; Nath, R.; Baker, J.; et al. Evaluation of Loopamp Leishmania Detection Kit and Leishmania Antigen ELISA for Post-Elimination Detection and Management of Visceral Leishmaniasis in Bangladesh. Front. Cell Infect. Microbiol. 2021, 11, 670759. [Google Scholar] [CrossRef]
- Li, J.; Macdonald, J.; von Stetten, F. Review: A comprehensive summary of a decade development of the recombinase polymerase amplification. Analyst 2019, 144, 31–67. [Google Scholar] [CrossRef] [PubMed]
- Lobato, I.M.; O’Sullivan, C.K. Recombinase polymerase amplification: Basics, applications and recent advances. TrAC Trends Anal. Chem. 2018, 98, 19–35. [Google Scholar] [CrossRef]
- Malecela, M.N.; Ducker, C. A road map for neglected tropical diseases 2021–2030. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 121–123. [Google Scholar] [CrossRef]
- Louizi, C.; Khan, A.A.; Faisal, K.; Chowdhury, R.; Ghosh, P.; Hossain, F.; Nisansala, T.; Ranasinghe, S.; Moreno, J.; Alvar, J.; et al. Assessment of pan-Leishmania detection by recombinase polymerase amplification assay. Diagn. Microbiol. Infect. Dis. 2023, 105, 115862. [Google Scholar] [CrossRef]
- Mesquita, S.G.; Lugli, E.B.; Matera, G.; Fonseca, C.T.; Caldeira, R.L.; Webster, B. Development of real-time and lateral flow recombinase polymerase amplification assays for rapid detection of Schistosoma mansoni. Front. Microbiol. 2022, 13, 1043596. [Google Scholar] [CrossRef]
- Lalremruata, A.; Nguyen, T.T.; McCall, M.B.B.; Mombo-Ngoma, G.; Agnandji, S.T.; Adegnika, A.A.; Lell, B.; Ramharter, M.; Hoffman, S.L.; Kremsner, P.G.; et al. Recombinase Polymerase Amplification and Lateral Flow Assay for Ultrasensitive Detection of Low-Density Plasmodium falciparum Infection from Controlled Human Malaria Infection Studies and Naturally Acquired Infections. J. Clin. Microbiol. 2020, 58, 10–128. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Yu, L.; Liu, C.; Ye, S.; Chen, W.; Li, D.; Huang, W. One-tube SARS-CoV-2 detection platform based on RT-RPA and CRISPR/Cas12a. J. Transl. Med. 2021, 19, 74. [Google Scholar] [CrossRef] [PubMed]
- Xiong, E.; Jiang, L.; Tian, T.; Hu, M.; Yue, H.; Huang, M.; Lin, W.; Jiang, Y.; Zhu, D.; Zhou, X. Simultaneous Dual-Gene Diagnosis of SARS-CoV-2 Based on CRISPR/Cas9-Mediated Lateral Flow Assay. Angew. Chem. Int. Ed. 2021, 60, 5307–5315. [Google Scholar] [CrossRef]
- Power, M.; Fell, G.; Wright, M. Principles for high-quality, high-value testing. Evid. Base. Med. 2013, 18, 5–10. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Case (n = 50) | Control (n = 50) |
|---|---|---|
| Male, n/N (%) | 28/50 (56.0%) | 29/50 (58.0%) |
| Age in years, mean ± SD | 31.50 ± 14.99 | 27.64 ± 14.21 |
| Past history of VL, n (%) | 15/50 (30.0%) | 0 (0%) |
| Fever more than two weeks, n (%) | 50/50 (100.0%) | 0 (0%) |
| Splenomegaly, n (%) | 50/50 (100.0%) | 0 (0%) |
| Hepatomegaly, n (%) | 14 (28.0%) | 0 (0%) |
| Pancytopenia, n (%) | 28 (56.0%) | 0 (0%) |
| rk39 RDT positive, n (%) | 50/50 (100.0%) | 0 (0%) |
| DAT positive, n (%) | 50/50 (100.0%) | 0 (0%) |
| DNA Extraction Methods | Mean OD 260/280 Ratio ± SD [95% CI] N = 50 | Mean DNA Conc. (ng/µL) ± SD [95% CI] N = 50 | Sensitivity of qPCR [95% CI] (n/N) N = 50 | Sensitivity of RPA [95% CI] (n/N) N = 50 | Specificity of qPCR and RPA [95% CI] (n/N) N = 50 |
|---|---|---|---|---|---|
| Qiagen | 1.82 ± 0.22 [1.76–1.88] | 13.10 ± 4.72 [11.75–14.45] | 94.00% [83.45–98.75%] (47/50) | 92.00% [80.77–97.78%] (46/50) | 100.00% [92.89–100.00%] (0/50) |
| SwiftDx (SX) | 0.59 ± 0.11 [0.57–0.63] | 170.4 ± 52.69 [155.4–185.4] | 92.00% [80.77–97.78%] (46/50) | 90.00% [78.19–96.67%] (45/50) | |
| Boil and Spin (BS) | 2.02 ± 0.49 [1.88–2.22] | 26.91 ± 11.69 [23.58–30.23] | 88.00% [75.69–95.47%] (44/50) |
| Assays | Kappa (k) | Agreement | McNemar (p-Value) |
|---|---|---|---|
| Q-qPCR vs. SX-qPCR | 0.980 | Excellent | 0.50 |
| Q-qPCR vs. Q-RPA | 0.980 | Excellent | 1.00 |
| Q-qPCR vs. BS-RPA | 0.940 | Excellent | 0.25 |
| Q-qPCR vs. SX-RPA | 0.960 | Excellent | 0.50 |
| SX-qPCR vs. Q-RPA | 0.960 | Excellent | 1.00 |
| SX-qPCR vs. BS-RPA | 0.919 | Excellent | 1.00 |
| SX-qPCR vs. SX-RPA | 0.940 | Excellent | 1.000 |
| Q-RPA vs. BS-RPA | 0.960 | Excellent | 0.500 |
| Q-RPA vs. SX-RPA | 0.980 | Excellent | 1.000 |
| SX-RPA vs. BS-RPA | 0.980 | Excellent | 1.000 |
| References | Country | Study Population | Reference Test | Clinical Specimen Tested | DNA Isolation Assay | Molecular Technique | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|---|
| Mondal et al. (2016) [16] | Bangladesh | 23 VL, 20 PKDL cases, and 5 Asymptomatic | qPCR | Buffy Coat, Skin Biopsy | Qiagen DNeasy Blood and tissue kit, SwiftDx (SX) | RPA | 100% | 100% |
| Gunaratna et al. (2018) [21] | Sri Lanka | 150 suspected CL cases | Microscopy, Conventional PCR | Direct Skin Punch Biopsy | SwiftDx (SX) | RPA | 65.5% | 100% |
| Skin Punch Biopsy-ATL | Qiagen DNeasy Blood and tissue kit | Conventional PCR | 92.4% | |||||
| Skin Punch Biopsy-RNAlater | 63.4% | |||||||
| Mukhtar et al. (2018) [24] | Sudan | 198 VL suspected cases | Microscopy of lymph node aspirates | Whole Blood | QIAamp mini kit (QIAGEN) | LAMP | 100% | 99.01% |
| Buffy Coat | 97.62% | |||||||
| Whole Blood | Boil and Spin (BS) | 97.62% | ||||||
| Buffy Coat | 95.24% | |||||||
| L. S. Batalini et al. (2020) [19] | Brazil | 30 Volunteers with negative serology for Leishmaniasis | Serology | Peripheral Blood | 20% sodium dodecyl sulfate (SDS), Guanidine isothiocyanate-phenol-chloroform (GTPC), and Commercial kit (GE Healthcare GenomicPrep Blood DNA Isolation KitTM) | Conventional PCR | 100% | 100% |
| Chowdhury R et al. (2020) [22] | Bangladesh | 30 PKDL cases and 30 endemic controls | Clinical evaluation and rK39 rapid diagnostic | Skin punch biopsy | Spin-column-based method (Qiagen) | qPCR | 86.67% | 100% |
| Spin-column-based method (Qiagen) | RPA | 93.33% | ||||||
| Boil and Spin (BS) | 76.67% | |||||||
| SwiftDx (SX) | 63.33% | |||||||
| Hossain et al. (2021) [25] | Bangladesh | 80 cases and 80 controls | Clinical evaluation and Rk39 rapid diagnostic test | Whole blood | QIAamp mini kit (Qiagen) | qPCR | 72.5% | 100% |
| Boil and Spin (BS) | - | |||||||
| QIAamp mini kit (Qiagen) | LAMP | 85% | 100% | |||||
| Boil and Spin (BS) | 96.2% | |||||||
| Present Study | Bangladesh | 50 cases and 50 controls | Clinical evaluation, rK39 rapid diagnostic test and DAT | Whole blood | Spin-column method (Qiagen) | qPCR | 94% | 100% |
| SwiftDx (SX) | 92% | |||||||
| Spin-column method (Qiagen) | RPA | 92% | ||||||
| SwiftDx (SX) | 90% | |||||||
| Boil and Spin (BS) | 88% |
| Aspect | Qiagen | Boil and Spin | SwiftDx |
|---|---|---|---|
| Principle | Silica membrane-based spin column | Boiling and centrifugation | Magnetic-bead-based extraction |
| Volume of sample required | 200 μL whole blood | 60 μL whole blood | 500 μL whole blood |
| Workflow simplicity | Multiple steps | Fewer steps | Fewer steps |
| * Turnaround time | 50 min | 12 min | 15 min |
| * Hands-on time | 20 min | 4 min | 5 min |
| Downstream applications | Suitable for various applications | Limited applications | Suitable for various applications |
| ** Cost | Relatively high (USD 3.4) | Relatively low (USD 0.006) | Moderate (USD 1.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghosh, P.; Chowdhury, R.; Faisal, K.; Khan, M.A.A.; Hossain, F.; Rahat, M.A.; Chowdhury, M.A.A.; Mithila, N.T.; Kamal, M.; Maruf, S.; et al. Evaluation of a Point-of-Need Molecular Diagnostic Tool Coupled with Rapid DNA Extraction Methods for Visceral Leishmaniasis. Diagnostics 2023, 13, 3639. https://doi.org/10.3390/diagnostics13243639
Ghosh P, Chowdhury R, Faisal K, Khan MAA, Hossain F, Rahat MA, Chowdhury MAA, Mithila NT, Kamal M, Maruf S, et al. Evaluation of a Point-of-Need Molecular Diagnostic Tool Coupled with Rapid DNA Extraction Methods for Visceral Leishmaniasis. Diagnostics. 2023; 13(24):3639. https://doi.org/10.3390/diagnostics13243639
Chicago/Turabian StyleGhosh, Prakash, Rajashree Chowdhury, Khaledul Faisal, Md. Anik Ashfaq Khan, Faria Hossain, Md. Abu Rahat, Md. Arko Ayon Chowdhury, Nishad Tasnim Mithila, Mostafa Kamal, Shomik Maruf, and et al. 2023. "Evaluation of a Point-of-Need Molecular Diagnostic Tool Coupled with Rapid DNA Extraction Methods for Visceral Leishmaniasis" Diagnostics 13, no. 24: 3639. https://doi.org/10.3390/diagnostics13243639
APA StyleGhosh, P., Chowdhury, R., Faisal, K., Khan, M. A. A., Hossain, F., Rahat, M. A., Chowdhury, M. A. A., Mithila, N. T., Kamal, M., Maruf, S., Nath, R., Kobialka, R. M., Ceruti, A., Cameron, M., Duthie, M. S., Wahed, A. A. E., & Mondal, D. (2023). Evaluation of a Point-of-Need Molecular Diagnostic Tool Coupled with Rapid DNA Extraction Methods for Visceral Leishmaniasis. Diagnostics, 13(24), 3639. https://doi.org/10.3390/diagnostics13243639