
Spectrum of Imaging Patterns of Lung Cancer following Radiation Therapy

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Types of Radiotherapy
2.1. Conventional Radiotherapy
2.2. Three-Dimensional Conformal Radiotherapy
2.3. Intensity-Modulated Radiotherapy
2.4. Stereotactic Body Radiotherapy
2.5. Four-Dimensional Conformal Radiotherapy
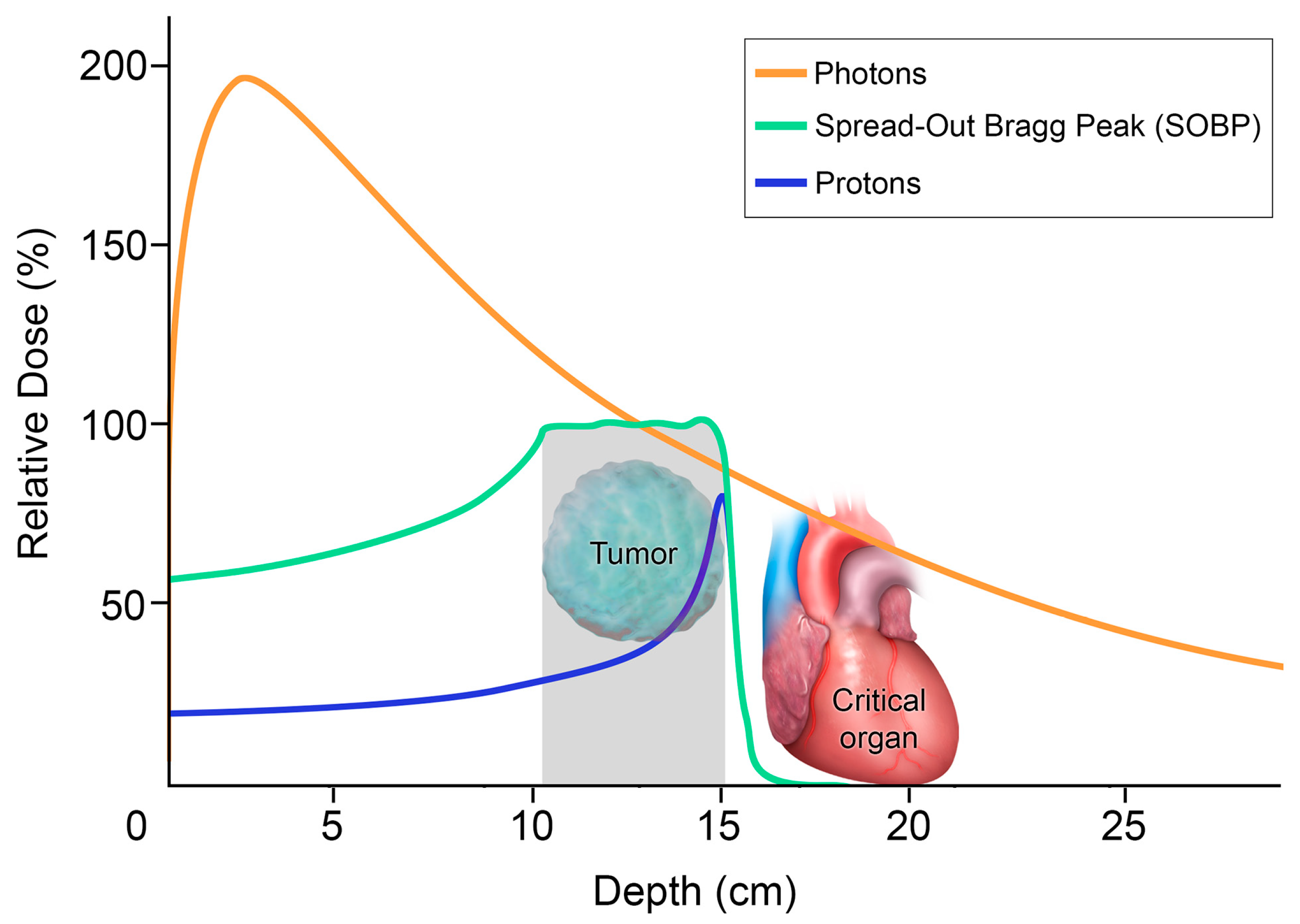
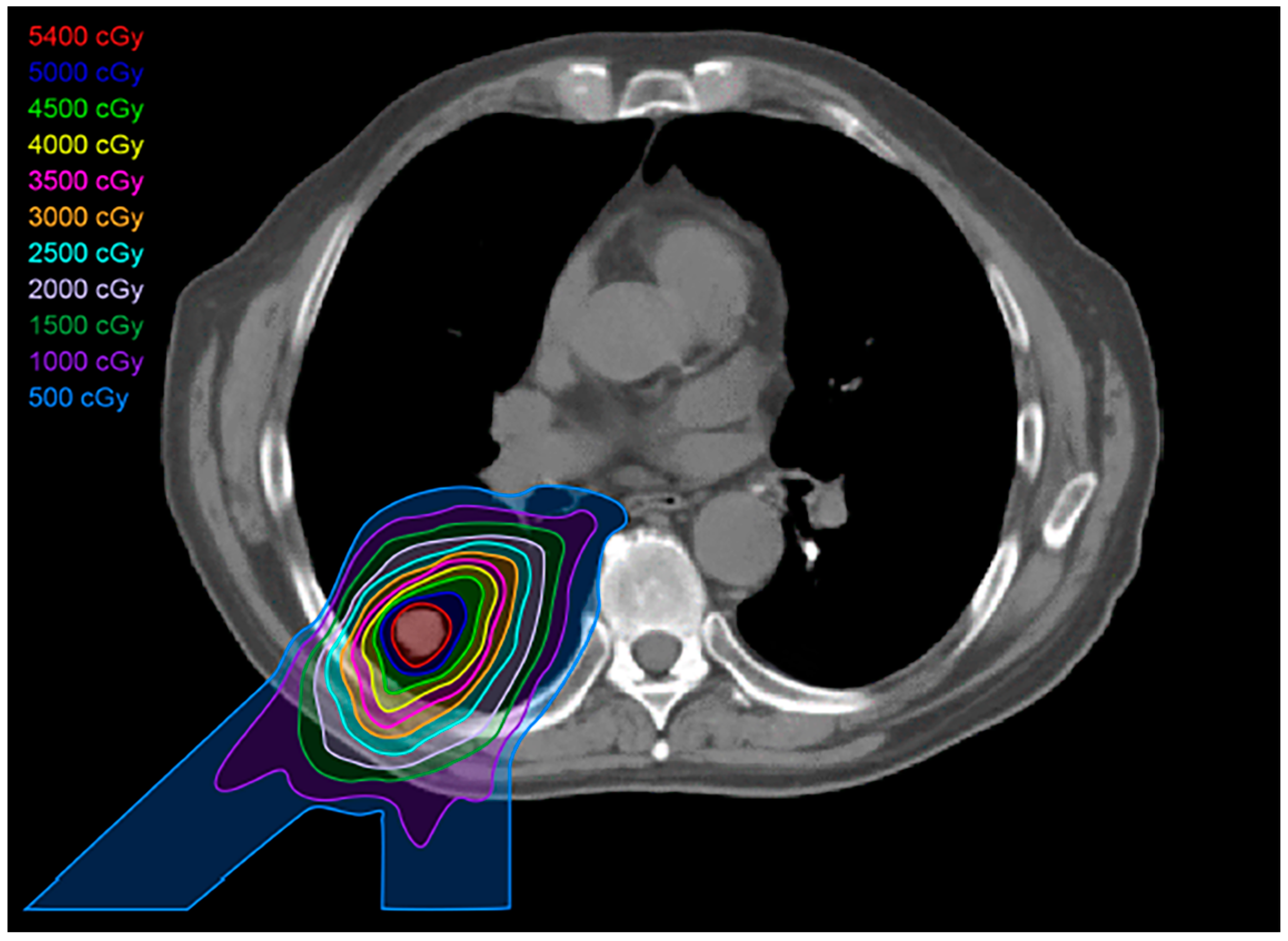
2.6. Proton Therapy
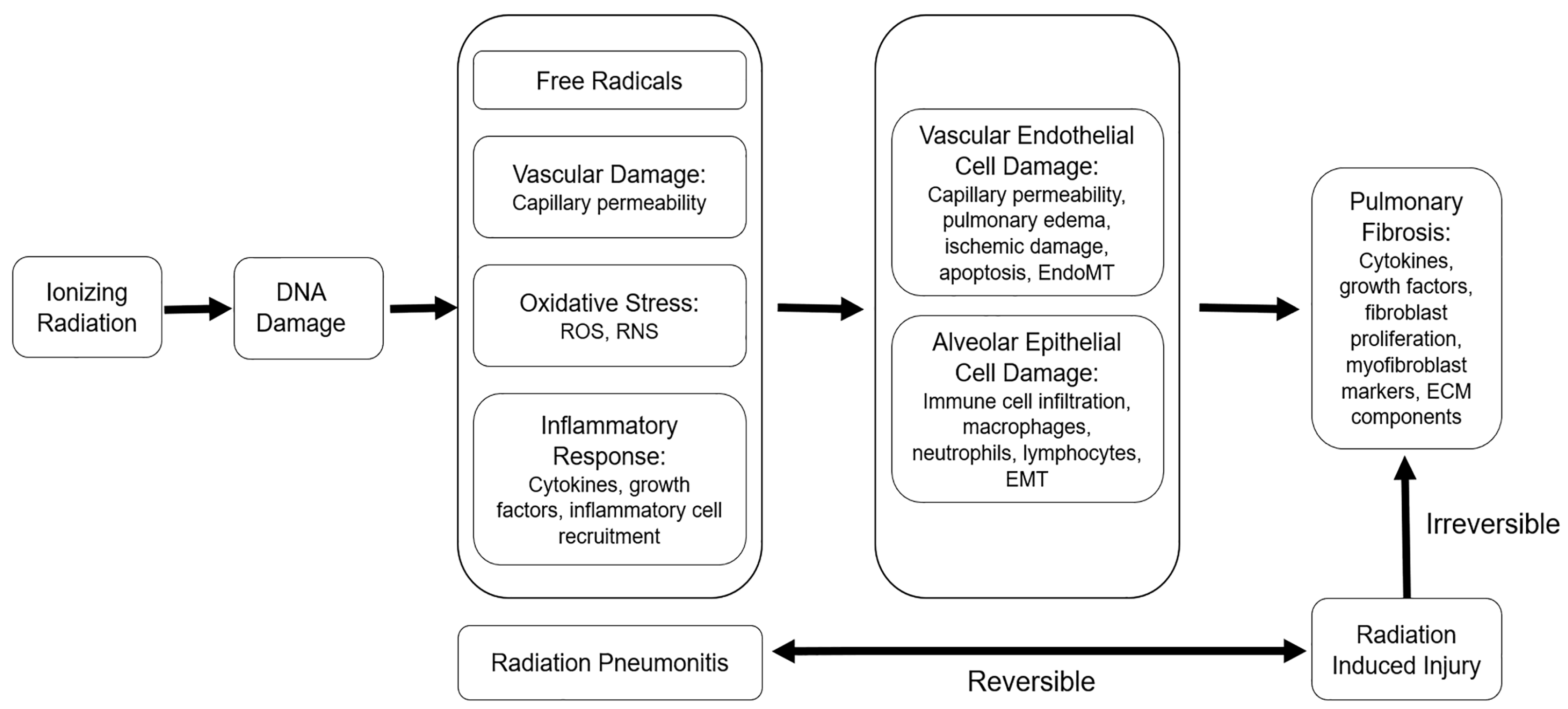
3. Post-Radiation Changes
4. Specific Imaging Patterns in RILI
4.1. Modified Conventional Pattern
4.2. Mass-like Pattern
4.3. Scar-like Pattern
4.4. Organizing Pneumonia
5. Imaging Modalities and Radiomics
5.1. Radiography
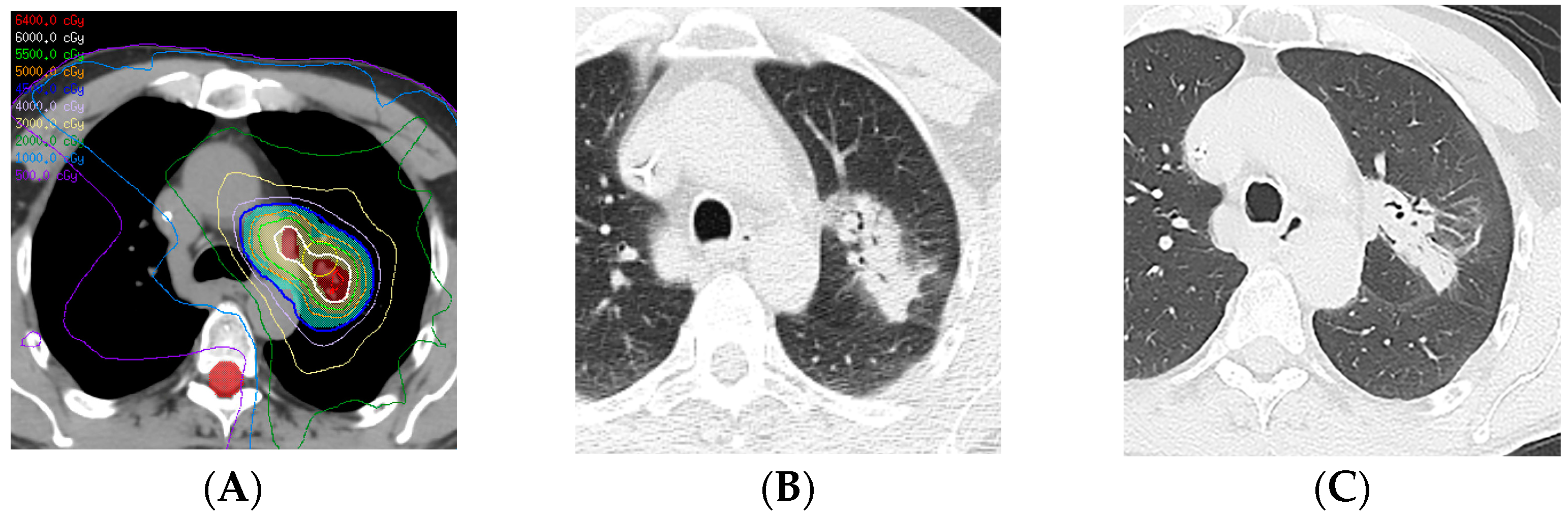
5.2. Computed Tomography
5.3. Positron Emission Tomography/Computed Tomography
5.4. Magnetic Resonance Imaging
5.5. Radiomics
6. Clinical Applications and Differential Diagnoses
6.1. Distinguishing Infection from the Acute Exudative Phase of RILI
6.2. Distinguishing Tumor Recurrence from the Chronic Mass-like Pattern of RILI
7. Complications of Lung Radiotherapy
7.1. In Situ Pulmonary Artery Thrombosis
7.2. Radiation Recall Pneumonitis
8. Follow-Up Recommendations
9. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hanania, A.N.; Mainwaring, W.; Ghebre, Y.T.; Hanania, N.A.; Ludwig, M. Radiation-Induced Lung Injury: Assessment and Management. Chest 2019, 156, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Sihoe, A.D.L. Video-assisted thoracoscopic surgery as the gold standard for lung cancer surgery. Respirology 2020, 25 (Suppl. 2), 49–60. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Chen, F.; Liu, R.; Fu, D.; Wang, Y.; Zhang, B.; Ren, D.; Ren, F.; Song, Z.; Chen, J.; et al. Outcomes of lobectomy on pulmonary function for early stage non-small cell lung cancer (NSCLC) patients with chronic obstructive pulmonary disease (COPD). Thorac. Cancer 2020, 11, 1784–1789. [Google Scholar] [CrossRef] [PubMed]
- Arroyo-Hernandez, M.; Maldonado, F.; Lozano-Ruiz, F.; Munoz-Montano, W.; Nunez-Baez, M.; Arrieta, O. Radiation-induced lung injury: Current evidence. BMC Pulm. Med. 2021, 21, 9. [Google Scholar] [CrossRef]
- Li, Q.; Liu, Y.; Su, B.; Zhao, H.; Lin, Q.; Zhu, Y.; Zhang, L.; Weng, D.; Gong, X.; Sun, X.; et al. The CT appearance pattern of radiation-induced lung injury and tumor recurrence after stereotactic body radiation therapy in early stage non-small cell lung cancer. Transl. Lung Cancer Res. 2020, 9, 713–721. [Google Scholar] [CrossRef]
- Casal-Mouriño, A.; Ruano-Ravina, A.; Lorenzo-González, M.; Rodríguez-Martínez, Á.; Giraldo-Osorio, A.; Varela-Lema, L.; Pereiro-Brea, T.; Barros-Dios, J.M.; Valdés-Cuadrado, L.; Pérez-Ríos, M. Epidemiology of stage III lung cancer: Frequency, diagnostic characteristics, and survival. Transl. Lung Cancer Res. 2021, 10, 506–518. [Google Scholar] [CrossRef]
- Benveniste, M.F.; Gomez, D.; Carter, B.W.; Betancourt Cuellar, S.L.; Shroff, G.S.; Benveniste, A.P.A.; Odisio, E.G.; Marom, E.M. Recognizing Radiation Therapy–related Complications in the Chest. RadioGraphics 2019, 39, 344–366. [Google Scholar] [CrossRef]
- Huang, K.; Palma, D.A. Follow-Up of Patients after Stereotactic Radiation for Lung Cancer: A Primer for the Nonradiation Oncologist. J. Thorac. Oncol. 2015, 10, 412–419. [Google Scholar] [CrossRef]
- Brown, S.; Banfill, K.; Aznar, M.C.; Whitehurst, P.; Faivre Finn, C. The evolving role of radiotherapy in non-small cell lung cancer. Br. J. Radiol. 2019, 92, 20190524. [Google Scholar] [CrossRef] [PubMed]
- Ghaye, B.; Wanet, M.; El Hajjam, M. Imaging after radiation therapy of thoracic tumors. Diagn. Interv. Imaging 2016, 97, 1037–1052. [Google Scholar] [CrossRef] [PubMed]
- Benveniste, M.F.; Gomez, D.; Viswanathan, C.; Shroff, G.S.; Betancourt Cuellar, S.L.; Carter, B.W.; Marom, E.M. Lung Cancer. J. Thorac. Imaging 2017, 32, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Guillemin, F.; Berger, L.; Lapeyre, M.; Belliere-Calandry, A. [Dosimetric and toxicity comparison of IMRT and 3D-CRT of non-small cell lung cancer]. Cancer Radiother. 2021, 25, 747–754. [Google Scholar] [CrossRef]
- Huang, K.; Dahele, M.; Senan, S.; Guckenberger, M.; Rodrigues, G.B.; Ward, A.; Boldt, R.G.; Palma, D.A. Radiographic changes after lung stereotactic ablative radiotherapy (SABR)—Can we distinguish recurrence from fibrosis? A systematic review of the literature. Radiother. Oncol. 2012, 102, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.J.; Mayoral, M.; Larici, A.R.; Ginsberg, M.S.; Cicchetti, G.; Fintelmann, F.J.; Marom, E.M.; Truong, M.T.; Gill, R.R. Imaging Follow-Up of Nonsurgical Therapies for Lung Cancer: AJR Expert Panel Narrative Review. Am. J. Roentgenol. 2023, 221, 409–424. [Google Scholar] [CrossRef]
- Thompson, M.; Rosenzweig, K.E. The evolving toxicity profile of SBRT for lung cancer. Transl. Lung Cancer Res. 2019, 8, 48–57. [Google Scholar] [CrossRef]
- Baumann, K.S.; Flatten, V.; Weber, U.; Lautenschlager, S.; Eberle, F.; Zink, K.; Engenhart-Cabillic, R. Effects of the Bragg peak degradation due to lung tissue in proton therapy of lung cancer patients. Radiat. Oncol. 2019, 14, 183. [Google Scholar] [CrossRef]
- Brooks, E.D.; Ning, M.S.; Verma, V.; Zhu, X.R.; Chang, J.Y. Proton therapy for non-small cell lung cancer: The road ahead. Transl. Lung Cancer Res. 2019, 8 (Suppl. 2), S202–S212. [Google Scholar] [CrossRef]
- Giuranno, L.; Ient, J.; De Ruysscher, D.; Vooijs, M.A. Radiation-Induced Lung Injury (RILI). Front. Oncol. 2019, 9, 877. [Google Scholar] [CrossRef]
- Konkol, M.; Sniatala, P.; Milecki, P. Radiation-induced lung injury—What do we know in the era of modern radiotherapy? Rep. Pr. Oncol. Radiother. 2022, 27, 552–565. [Google Scholar] [CrossRef] [PubMed]
- Rahi, M.S.; Parekh, J.; Pednekar, P.; Parmar, G.; Abraham, S.; Nasir, S.; Subramaniyam, R.; Jeyashanmugaraja, G.P.; Gunasekaran, K. Radiation-Induced Lung Injury-Current Perspectives and Management. Clin. Pr. 2021, 11, 410–429. [Google Scholar] [CrossRef] [PubMed]
- Strange, C.D.; Shroff, G.S.; Truong, M.T.; Nguyen, Q.N.; Vlahos, I.; Erasmus, J.J. Imaging of the post-radiation chest in lung cancer. Clin. Radiol. 2022, 77, 19–30. [Google Scholar] [CrossRef]
- Brada, M.; Forbes, H.; Ashley, S.; Fenwick, J. Improving Outcomes in NSCLC: Optimum Dose Fractionation in Radical Radiotherapy Matters. J. Thorac. Oncol. 2022, 17, 532–543. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, P.; Zhang-Velten, E.; Court, L.; Westover, K.; Yan, Y.; Lin, M.-H.; Xiong, Z.; Patel, M.; Rivera, D.; Chang, J.; et al. Accelerated Hypofractionated Image-Guided vs Conventional Radiotherapy for Patients With Stage II/III Non-Small Cell Lung Cancer and Poor Performance Status: A Randomized Clinical Trial. JAMA Oncol. 2021, 7, 1497–1505. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhou, J.; Verma, V.; Liu, X.; Wu, M.; Yu, J.; Chen, D. Crossed Pathways for Radiation-Induced and Immunotherapy-Related Lung Injury. Front. Immunol. 2021, 12, 774807. [Google Scholar] [CrossRef]
- Benveniste, M.F.K.; Welsh, J.; Godoy, M.C.B.; Betancourt, S.L.; Mawlawi, O.R.; Munden, R.F. New era of radiotherapy: An update in radiation-induced lung disease. Clin. Radiol. 2013, 68, e275–e290. [Google Scholar] [CrossRef]
- Chassagnon, G.; Martini, K.; Giraud, P.; Revel, M.P. Radiological assessment after stereotactic body radiation of lung tumours. Cancer Radiother. 2020, 24, 379–387. [Google Scholar] [CrossRef]
- Al-Umairi, R.; Tarique, U.; Moineddin, R.; Jimenez-Juan, L.; Kha, L.C.; Cheung, P.; Oikonomou, A. CT patterns and serial CT Changes in lung Cancer patients post stereotactic body radiotherapy (SBRT). Cancer Imaging 2022, 22, 51. [Google Scholar] [CrossRef]
- Febbo, J.A.; Gaddikeri, R.S.; Shah, P.N. Stereotactic Body Radiation Therapy for Early-Stage Non–Small Cell Lung Cancer: A Primer for Radiologists. RadioGraphics 2018, 38, 1312–1336. [Google Scholar] [CrossRef]
- Ando, S.M.; Fonseca, E.; Frassei, J.D.S.; de Farias, L.P.G.; Neves, Y.C.S.; Chate, R.C.; Sawamura, M.V.Y. The role of the radiologist in the assessment of thoracic changes after radiotherapy. Radiol. Bras. 2021, 54, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Fanetti, G.; Bazzani, F.; Ferrari, A.; Alterio, D.; Donghi, S.M.; Pounou Kamga, F.A.; Orecchia, R.; Jereczek-Fossa, B.A. Bronchiolitis obliterans organizing pneumonia after stereotactic ablative radiation therapy for lung cancer: A case report. Cancer Radiother. 2018, 22, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Libshitz, H.I.; Southard, M.E. Complications of radiation therapy: The thorax. Semin. Roentgenol. 1974, 9, 41–49. [Google Scholar] [CrossRef]
- DeLappe, E.; Dunphy, M. 18F-2-Deoxy-d-Glucose Positron Emission Tomography-Computed Tomography in Lung Cancer. Semin. Roentgenol. 2011, 46, 208–223. [Google Scholar] [CrossRef] [PubMed]
- Fonti, R.; Conson, M.; Del Vecchio, S. PET/CT in radiation oncology. Semin. Oncol. 2019, 46, 202–209. [Google Scholar] [CrossRef]
- Geets, X.; Sterpin, E.; Wanet, M.; Di Perri, D.; Lee, J. Metabolic imaging in non-small cell lung cancer radiotherapy. Cancer/RadiothÉRapie 2014, 18, 402–405. [Google Scholar] [CrossRef]
- Dreyfuss, A.D.; Jahangiri, P.; Simone, C.B., 2nd; Alavi, A. Evolving Role of Novel Quantitative PET Techniques to Detect Radiation-Induced Complications. PET Clin. 2020, 15, 89–100. [Google Scholar] [CrossRef]
- Sim, A.J.; Kaza, E.; Singer, L.; Rosenberg, S.A. A review of the role of MRI in diagnosis and treatment of early stage lung cancer. Clin. Transl. Radiat. Oncol. 2020, 24, 16–22. [Google Scholar] [CrossRef]
- Omidi, A.; Weiss, E.; Trankle, C.R.; Rosu-Bubulac, M.; Wilson, J.S. Quantitative assessment of radiotherapy-induced myocardial damage using MRI: A systematic review. Cardiooncology 2023, 9, 24. [Google Scholar] [CrossRef]
- Santyr, G.; Fox, M.; Thind, K.; Hegarty, E.; Ouriadov, A.; Jensen, M.; Scholl, T.J.; Van Dyk, J.; Wong, E. Anatomical, functional and metabolic imaging of radiation-induced lung injury using hyperpolarized MRI. NMR Biomed. 2014, 27, 1515–1524. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging-"how-to" guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Desideri, I.; Loi, M.; Francolini, G.; Becherini, C.; Livi, L.; Bonomo, P. Application of Radiomics for the Prediction of Radiation-Induced Toxicity in the IMRT Era: Current State-of-the-Art. Front. Oncol. 2020, 10, 1708. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, N.; Chang, C.F.; Lee, C. Special Considerations for Tree-in-Bud Nodules. Ann. Am. Thorac. Soc. 2019, 16, 636–638. [Google Scholar] [CrossRef] [PubMed]
- Gafoor, K.; Patel, S.; Girvin, F.; Gupta, N.; Naidich, D.; Machnicki, S.; Brown, K.K.; Mehta, A.; Husta, B.; Ryu, J.H.; et al. Cavitary Lung Diseases: A Clinical-Radiologic Algorithmic Approach. Chest 2018, 153, 1443–1465. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Nishino, M.; Jagannathan, J.P.; Ramaiya, N.H.; Van den Abbeele, A.D. Revised RECIST Guideline Version 1.1: What Oncologists Want to Know and What Radiologists Need to Know. Am. J. Roentgenol. 2010, 195, 281–289. [Google Scholar] [CrossRef]
- Nakamura, N.; Hojo, H.; Inoue, K.; Hotta, K.; Zenda, S.; Baba, H.; Onozawa, M.; Motegi, A.; Nakamura, M.; Kibe, Y.; et al. Late radiological changes after passive scattering proton beam therapy for Stage I lung cancer. J. Radiat. Res. 2018, 59, 456–461. [Google Scholar] [CrossRef]
- Yang, Y.; Li, G.; Li, S.; Wang, Y.; Zhao, Y.; Dong, B.; Wang, J.; Zhu, R.; Chen, M. CT Appearance Pattern After Stereotactic Body Radiation Therapy Predicts Outcomes in Early-Stage Non-Small-Cell Lung Cancer. Front. Oncol. 2021, 11, 746785. [Google Scholar] [CrossRef]
- Kato, S.; Nambu, A.; Onishi, H.; Saito, A.; Kuriyama, K.; Komiyama, T.; Marino, K.; Araki, T. Computed tomography appearances of local recurrence after stereotactic body radiation therapy for stage I non-small-cell lung carcinoma. Jpn. J. Radiol. 2010, 28, 259–265. [Google Scholar] [CrossRef]
- Larici, A.R.; del Ciello, A.; Maggi, F.; Santoro, S.I.; Meduri, B.; Valentini, V.; Giordano, A.; Bonomo, L. Lung Abnormalities at Multimodality Imaging after Radiation Therapy for Non–Small Cell Lung Cancer. RadioGraphics 2011, 31, 771–789. [Google Scholar] [CrossRef]
- Cao, Y.; Geng, C.; Li, Y.; Zhang, Y. In situ Pulmonary Artery Thrombosis: A Previously Overlooked Disease. Front. Pharmacol. 2021, 12, 671589. [Google Scholar] [CrossRef] [PubMed]
- Porembskaya, O.; Zinserling, V.; Tomson, V.; Toropova, Y.; Starikova, E.A.; Maslei, V.V.; Bulavinova, N.I.; Kirik, O.V.; Syrtsova, M.A.; Laberko, L.; et al. Neutrophils Mediate Pulmonary Artery Thrombosis In Situ. Int. J. Mol. Sci. 2022, 23, 5829. [Google Scholar] [CrossRef] [PubMed]
- Baranga, L.; Khanuja, S.; Scott, J.A.; Provancha, I.; Gosselin, M.; Walsh, J.; Arancibia, R.; Bruno, M.A.; Waite, S. In Situ Pulmonary Arterial Thrombosis: Literature Review and Clinical Significance of a Distinct Entity. AJR Am. J. Roentgenol. 2023, 221, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, J.; Shroff, G.S.; Benveniste, M.F.; Marom, E.M.; Truong, M.T.; Wu, C.C. In Situ Pulmonary Artery Thrombosis: Unrecognized Complication of Radiation Therapy. AJR Am. J. Roentgenol. 2020, 215, 1329–1334. [Google Scholar] [CrossRef]
- Jan, P.R.; Chang, J.W.; Wu, C.E. Radiation Recall Pneumonitis: A Rare Syndrome That Should Be Recognized. Cancers 2022, 14, 4642. [Google Scholar] [CrossRef] [PubMed]
- McGovern, K.; Ghaly, M.; Esposito, M.; Barnaby, K.; Seetharamu, N. Radiation recall pneumonitis in the setting of immunotherapy and radiation: A focused review. Future Sci. OA 2019, 5, FSO378. [Google Scholar] [CrossRef] [PubMed]
- Teng, F.; Li, M.; Yu, J. Radiation recall pneumonitis induced by PD-1/PD-L1 blockades: Mechanisms and therapeutic implications. BMC Med. 2020, 18, 275. [Google Scholar] [CrossRef]
- Linda, A.; Trovo, M.; Bradley, J.D. Radiation injury of the lung after stereotactic body radiation therapy (SBRT) for lung cancer: A timeline and pattern of CT changes. Eur. J. Radiol. 2011, 79, 147–154. [Google Scholar] [CrossRef]
- Patz, E.F.; Lowe, V.J.; Hoffman, J.M.; Paine, S.S.; Harris, L.K.; Goodman, P.C. Persistent or recurrent bronchogenic carcinoma: Detection with PET and 2-[F-18]-2-deoxy-D-glucose. Radiology 1994, 191, 379–382. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Enlarging Opacity at the Primary Site |
|---|
| Sequential enlargement |
| Enlargement 12 months after RT completion |
| Bulging margins |
| Linear margin disappearance |
| Loss of air bronchogram |
| Craniocaudal growth of ≥5 mm and ≥20% |
| Risk Level | Number of High-Risk Features | Management |
|---|---|---|
| Low | 0 | CT every 3 to 6 months for 1 year, and every 6 to 12 months thereafter |
| Intermediate | 1–2 | CT at 3 months or FDG PET/CT |
| High | ≥3 | Biopsy or salvage therapy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strange, T.A.; Erasmus, L.T.; Ahuja, J.; Agrawal, R.; Shroff, G.S.; Truong, M.T.; Strange, C.D. Spectrum of Imaging Patterns of Lung Cancer following Radiation Therapy. Diagnostics 2023, 13, 3283. https://doi.org/10.3390/diagnostics13203283
Strange TA, Erasmus LT, Ahuja J, Agrawal R, Shroff GS, Truong MT, Strange CD. Spectrum of Imaging Patterns of Lung Cancer following Radiation Therapy. Diagnostics. 2023; 13(20):3283. https://doi.org/10.3390/diagnostics13203283
Chicago/Turabian StyleStrange, Taylor A., Lauren T. Erasmus, Jitesh Ahuja, Rishi Agrawal, Girish S. Shroff, Mylene T. Truong, and Chad D. Strange. 2023. "Spectrum of Imaging Patterns of Lung Cancer following Radiation Therapy" Diagnostics 13, no. 20: 3283. https://doi.org/10.3390/diagnostics13203283
APA StyleStrange, T. A., Erasmus, L. T., Ahuja, J., Agrawal, R., Shroff, G. S., Truong, M. T., & Strange, C. D. (2023). Spectrum of Imaging Patterns of Lung Cancer following Radiation Therapy. Diagnostics, 13(20), 3283. https://doi.org/10.3390/diagnostics13203283