
User Perceptions of Visual Blood: An International Mixed Methods Study on Novel Blood Gas Analysis Visualization

 , , , , , , , , ,
, , , , , , , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Approval and Consent
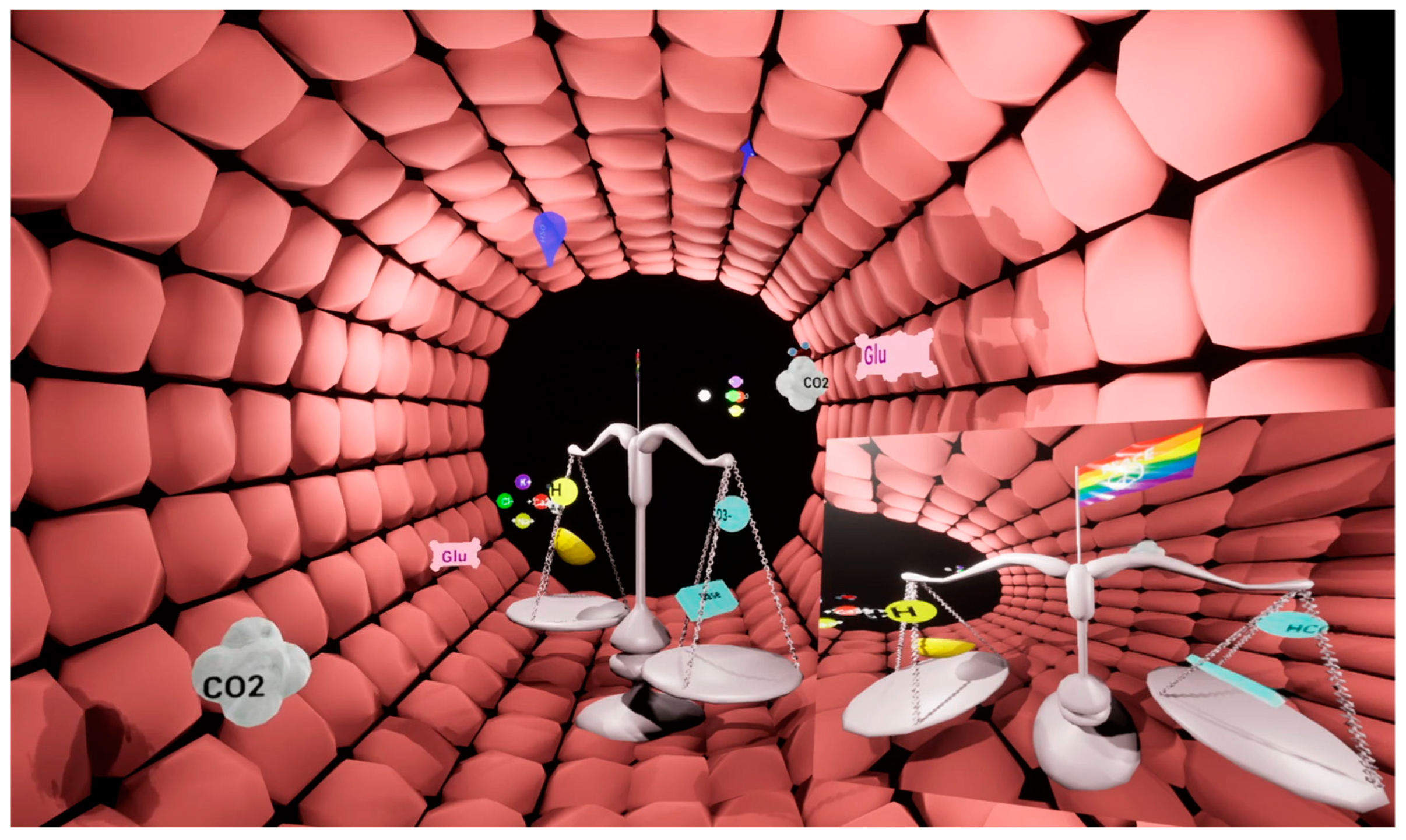
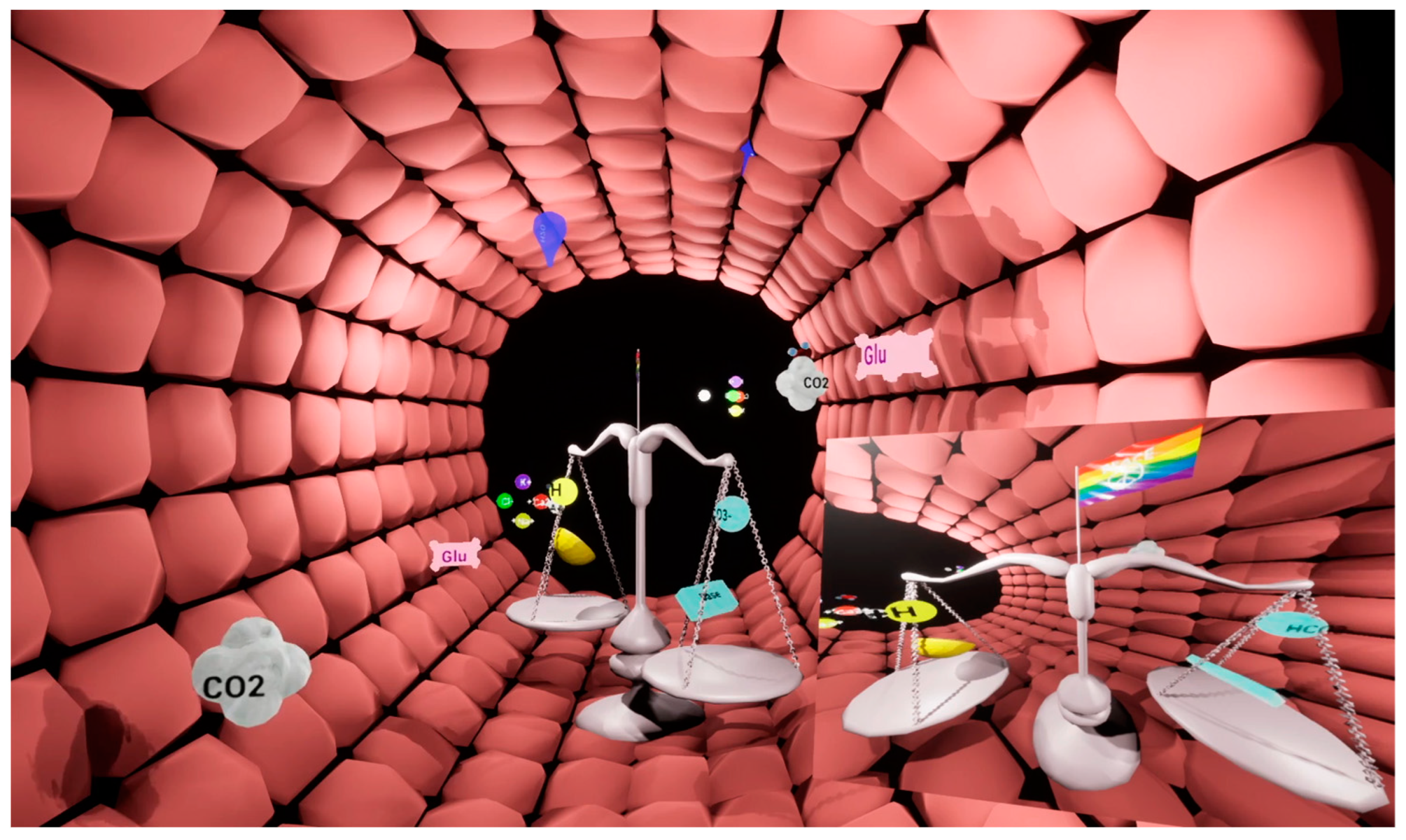
2.2. Visual Blood
2.3. Previous Visual Blood Simulation Studies
2.4. Study Design
2.4.1. Qualitative Part: Participant Interviews
2.4.2. Quantitative Part: Online Survey
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
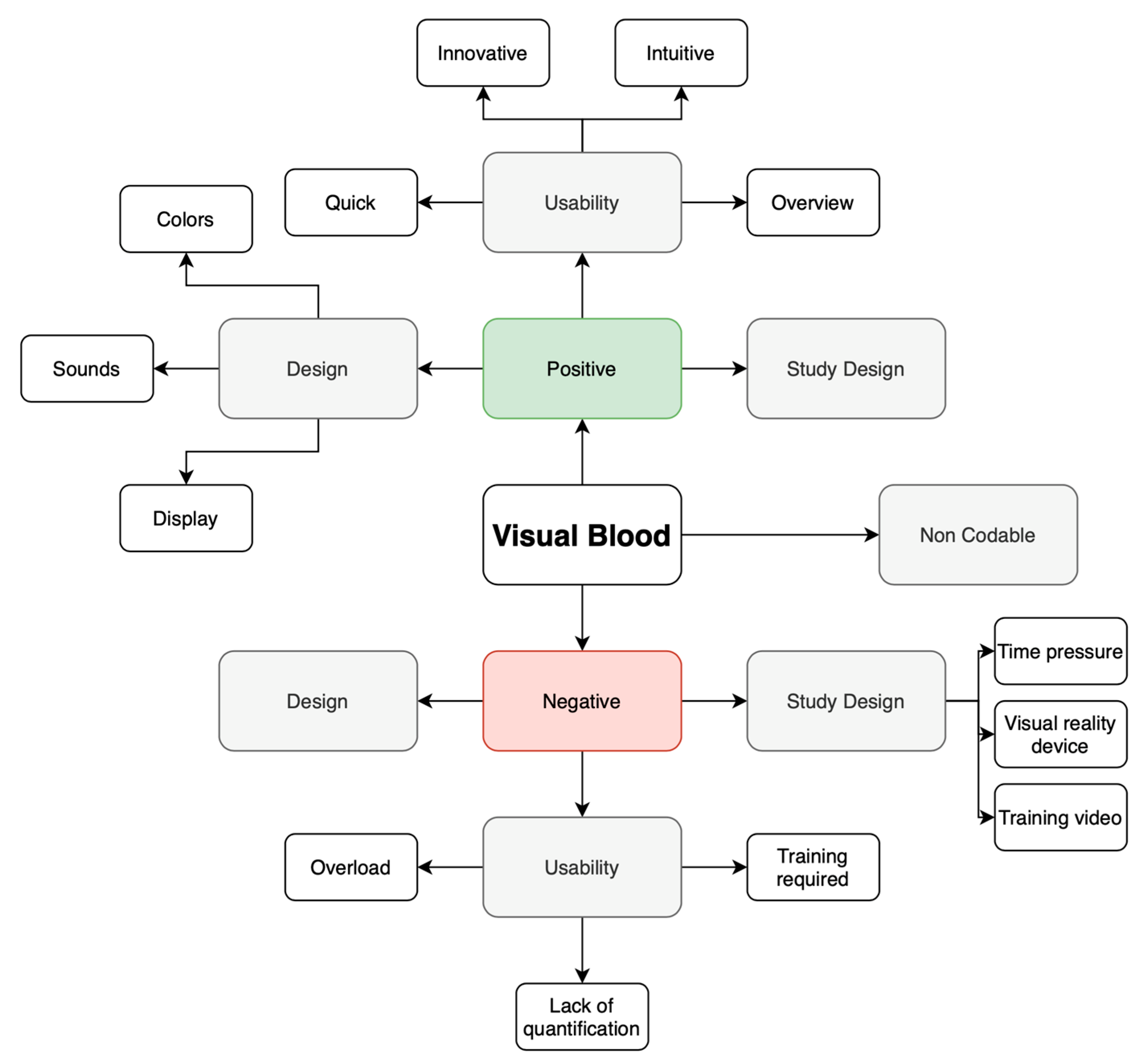
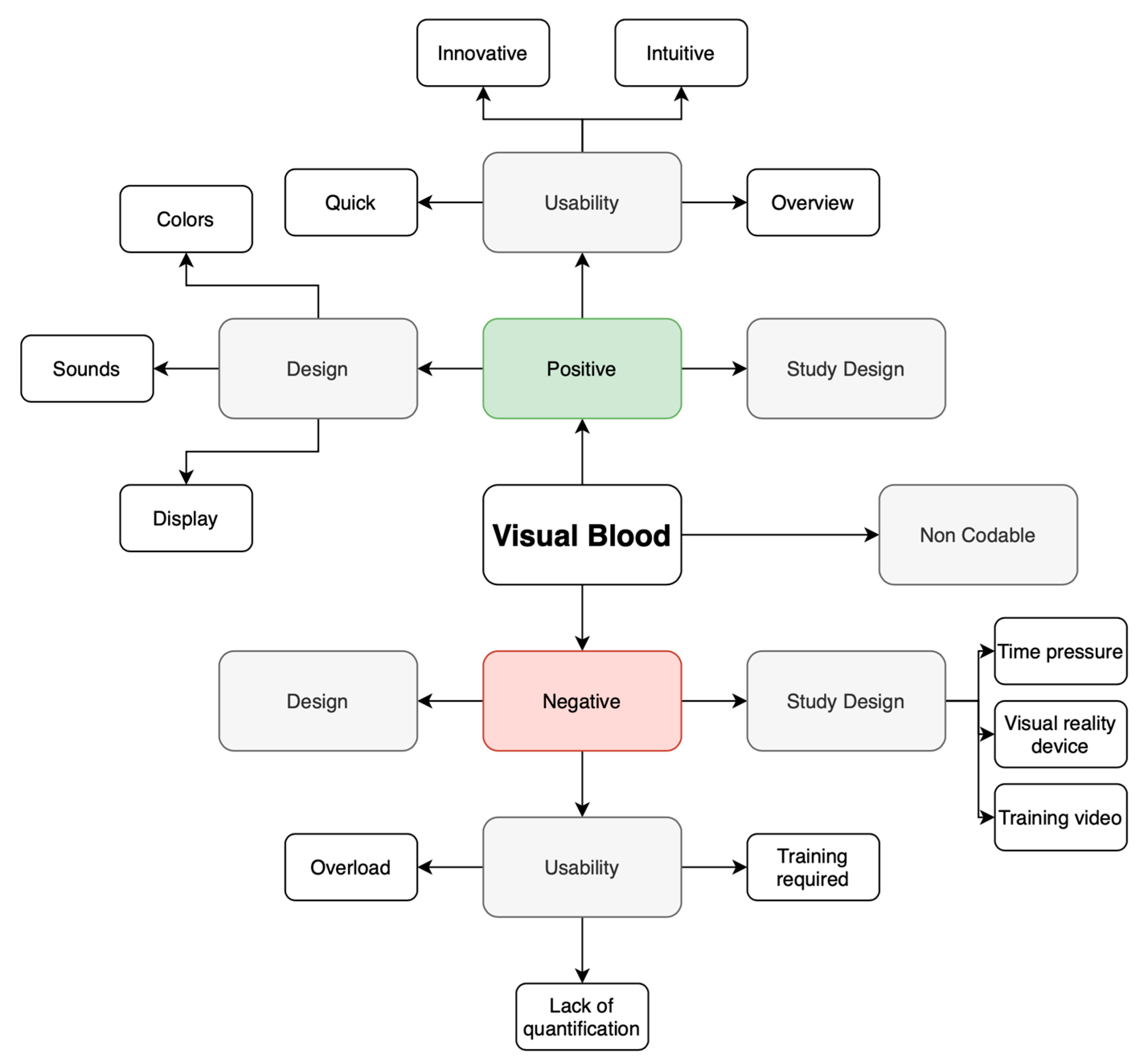
3.2. Qualitative Analysis
3.2.1. User Perceptions Following Virtual Reality Simulations
3.2.2. User Perceptions Following Simulations (No Virtual Reality Headset)
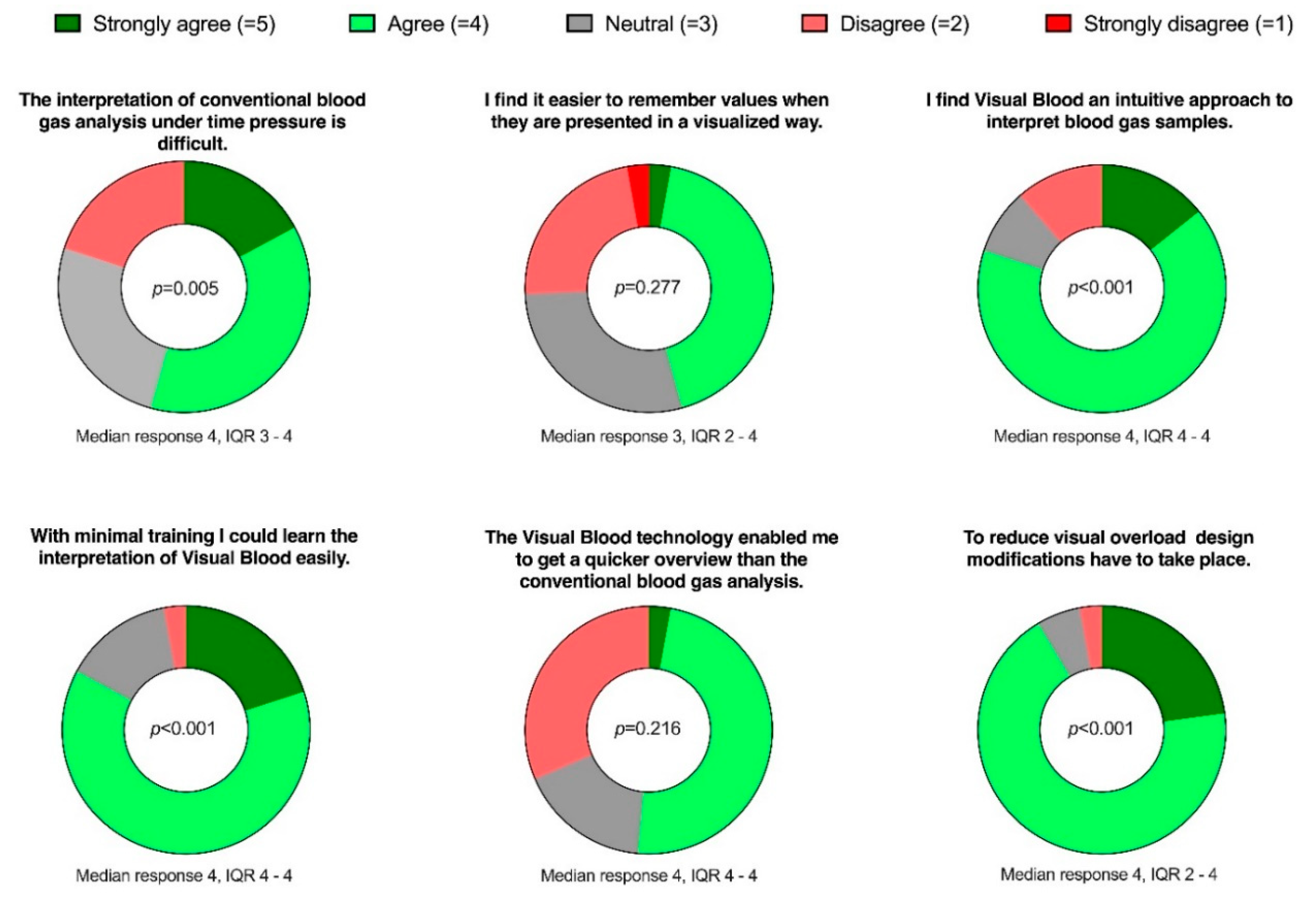
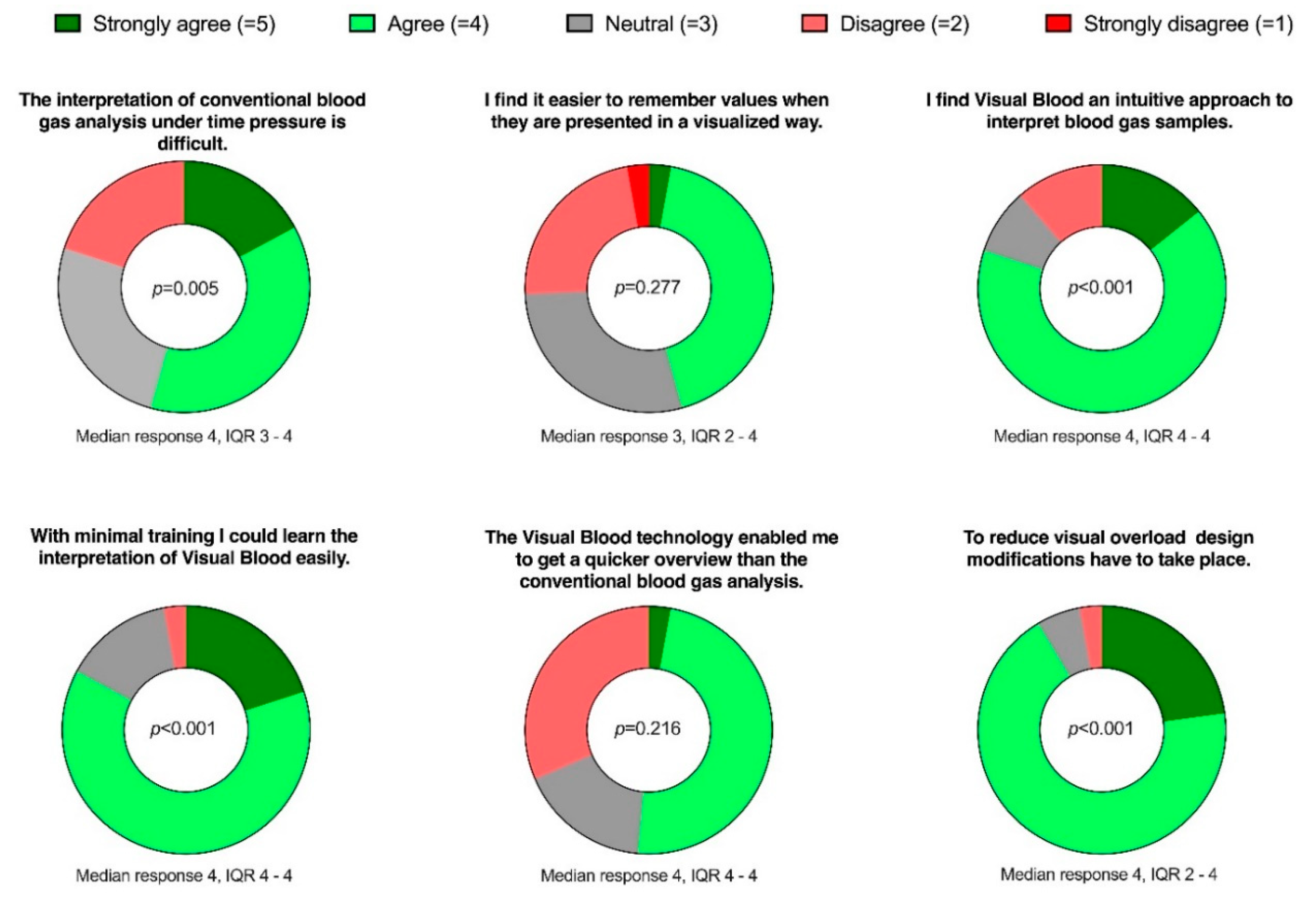
3.3. Online Survey (Quantitative Part)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Plsek, P.E.; Greenhalgh, T. Complexity science: The challenge of complexity in health care. BMJ 2001, 323, 625–628. [Google Scholar] [CrossRef]
- Olshansky, S.J. From Lifespan to Healthspan. JAMA 2018, 320, 1323–1324. [Google Scholar] [CrossRef]
- Global Burden of Disease Study Collaboration. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Lee, T.H. Lost in Thought—The Limits of the Human Mind and the Future of Medicine. N. Engl. J. Med. 2017, 377, 1209–1211. [Google Scholar] [CrossRef]
- Makary, M.A.; Daniel, M. Medical error-the third leading cause of death in the US. BMJ 2016, 353, i2139. [Google Scholar] [CrossRef]
- Pickering, B.W.; Herasevich, V.; Ahmed, A.; Gajic, O. Novel Representation of Clinical Information in the ICU: Developing User Interfaces which Reduce Information Overload. Appl. Clin. Inform. 2010, 1, 116–131. [Google Scholar]
- Singh, H.; Spitzmueller, C.; Petersen, N.J.; Sawhney, M.K.; Sittig, D.F. Information overload and missed test results in electronic health record-based settings. JAMA Intern. Med. 2013, 173, 702–704. [Google Scholar] [CrossRef]
- Bracco, D.; Favre, J.B.; Bissonnette, B.; Wasserfallen, J.B.; Revelly, J.P.; Ravussin, P.; Chioléro, R. Human errors in a multidisciplinary intensive care unit: A 1-year prospective study. Intensive Care Med. 2001, 27, 137–145. [Google Scholar] [CrossRef]
- Severinghaus, J.W. The invention and development of blood gas analysis apparatus. Anesthesiology 2002, 97, 253–256. [Google Scholar] [CrossRef]
- Gattinoni, L.; Pesenti, A.; Matthay, M. Understanding blood gas analysis. Intensive Care Med. 2018, 44, 91–93. [Google Scholar] [CrossRef]
- General Medical Council. Practical Skills and Procedures; General Medical Council: London, UK, 2019. [Google Scholar]
- Austin, K.; Jones, P. Accuracy of interpretation of arterial blood gases by emergency medicine doctors. Emerg. Med. Australas. 2010, 22, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Powles, A.C.P.; Morse, J.L.C.; Pugsley, S.O.; Campbell, E.J.M. Interpretation of blood gas analysis by physicians in a community teaching hospital. Br. J. Dis. Chest 1979, 73, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.C.; Borbolla, D.; Waller, R.G.; Del Fiol, G.; Reese, T.; Nesbitt, P.; Segall, N. Critical care information display approaches and design frameworks: A systematic review and meta-analysis. J. Biomed. Inform. X 2019, 100, 100041. [Google Scholar] [CrossRef]
- Drews, F.A. Patient Monitors in Critical Care: Lessons for Improvement. In Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 3: Performance and Tools); Henriksen, K., Battles, J.B., Keyes, M.A., Grady, M.L., Eds.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Waller, R.G.; Wright, M.C.; Segall, N.; Nesbitt, P.; Reese, T.; Borbolla, D.; Del Fiol, G. Novel displays of patient information in critical care settings: A systematic review. J. Am. Med. Inform. Assoc. 2019, 26, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Drews, F.A.; Westenskow, D.R. The right picture is worth a thousand numbers: Data displays in anesthesia. Hum. Factors 2006, 48, 59–71. [Google Scholar] [CrossRef]
- Ensor, T.M.; Bancroft, T.D.; Hockley, W.E. Listening to the Picture-Superiority Effect Evidence for the Conceptual-Distinctiveness Account of Picture Superiority in Recognition. Exp. Psychol. 2019, 66, 134–153. [Google Scholar] [CrossRef]
- Drews, F.A.; Agutter, J.; Syroid, N.D.; Albert, R.W.; Westenskow, D.R.; Strayer, D.L. Evaluating a Graphical Cardiovascular Display for Anesthesia. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2016, 45, 1303–1307. [Google Scholar] [CrossRef]
- Wachter, S.B.; Johnson, K.; Albert, R.; Syroid, N.; Drews, F.; Westenskow, D. The evaluation of a pulmonary display to detect adverse respiratory events using high resolution human simulator. J. Am. Med. Inform. Assoc. 2006, 13, 635–642. [Google Scholar] [CrossRef]
- Philips. Patient Monitoring: Visual Patient Avatar. 2023. Available online: https://www.philips.co.uk/healthcare/technology/visual-patient-avatar (accessed on 12 June 2023).
- Tscholl, D.W.; Rössler, J.; Said, S.; Kaserer, A.; Spahn, D.R.; Nöthiger, C.B. Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research. Sensors 2020, 20, 2112. [Google Scholar] [CrossRef]
- Gasciauskaite, G.; Lunkiewicz, J.; Roche, T.R.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Human-centered visualization technologies for patient monitoring are the future: A narrative review. Crit. Care 2023, 27, 254. [Google Scholar] [CrossRef]
- Schweiger, G.; Malorgio, A.; Henckert, D.; Braun, J.; Meybohm, P.; Hottenrott, S.; Froehlich, C.; Zacharowski, K.; Raimann, F.J.; Piekarski, F.; et al. Visual Blood, a 3D Animated Computer Model to Optimize the Interpretation of Blood Gas Analysis. Bioengineering 2023, 10, 293. [Google Scholar] [CrossRef] [PubMed]
- Bergauer, L.; Akbas, S.; Braun, J.; Ganter, M.T.; Meybohm, P.; Hottenrott, S.; Zacharowski, K.; Raimann, F.J.; Rivas, E.; López-Baamonde, M.; et al. Visual Blood, Visualisation of Blood Gas Analysis in Virtual Reality, Leads to More Correct Diagnoses: A Computer-Based, Multicentre, Simulation Study. Bioengineering 2023, 10, 340. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Endsley, M.R. Designing for Situation Awareness: An Approach to User-Centered Design, 2nd ed.; CRC Press Inc.: Boca Raton, FL, USA, 2011. [Google Scholar]
- O’Connor, C.; Joffe, H. Intercoder Reliability in Qualitative Research: Debates and Practical Guidelines. Int. J. Qual. Methods 2020, 19, 1609406919899220. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Hussain, R.; Chessa, M.; Solari, F. Mitigating Cybersickness in Virtual Reality Systems through Foveated Depth-of-Field Blur. Sensors 2021, 21, 4006. [Google Scholar] [CrossRef]
- Bruno, R.R.; Bruining, N.; Jung, C.; VR-ICU Study group Kelm Malte Wolff Georg Wernly Bernhard. Virtual reality in intensive care. Intensive Care Med. 2022, 48, 1227–1229. [Google Scholar] [CrossRef]
- Atieno, O.P. An analysis of the strengths and limitation of qualitative and quantitative research paradigms. Probl. Educ. 21st Century 2009, 13, 13–38. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Participant Characteristics | Values |
|---|---|
| Simulations with visual reality device | |
| Study centers, n | 5 |
| Participants per study center, n | 10 |
| Female participants, n (%) | 31 (62%) |
| Age (years), median (*IQR) | 31 (28–41) |
| Senior physicians, n (%) | 22 (44%) |
| Resident physicians, n (%) | 28 (56%) |
| Total work experience (years), median (IQR) | 5 (2–10) |
| Blood gas analysis skills, self-rated, (0 = novice, 100 = expert), median (IQR) | 70.5 (60–83) |
| Video game playing, subjective frequency (0 = never, 100 = very often), median (IQR) | 6 (0–31) |
| Simulations without visual reality device | |
Study centers, n
| 3
|
| Female participants, n (%) | 42 (60%) |
| Age (years), median (IQR) | 30 (28–39) |
| Senior physicians, n (%) | 15 (21.4%) |
| Resident physicians, n (%) | 55 (78.6%) |
| Total work experience (years), median (IQR) | 6 (3–8) |
| Blood gas analysis skills, self-rated, (0 = novice, 100 = expert), median (IQR) | 29 (22–37) |
| Users’ Perceptions after the Computer-Based Simulations with Virtual Reality | Users’ Perceptions after the Computer-Based Simulations without Virtual Reality |
|---|---|
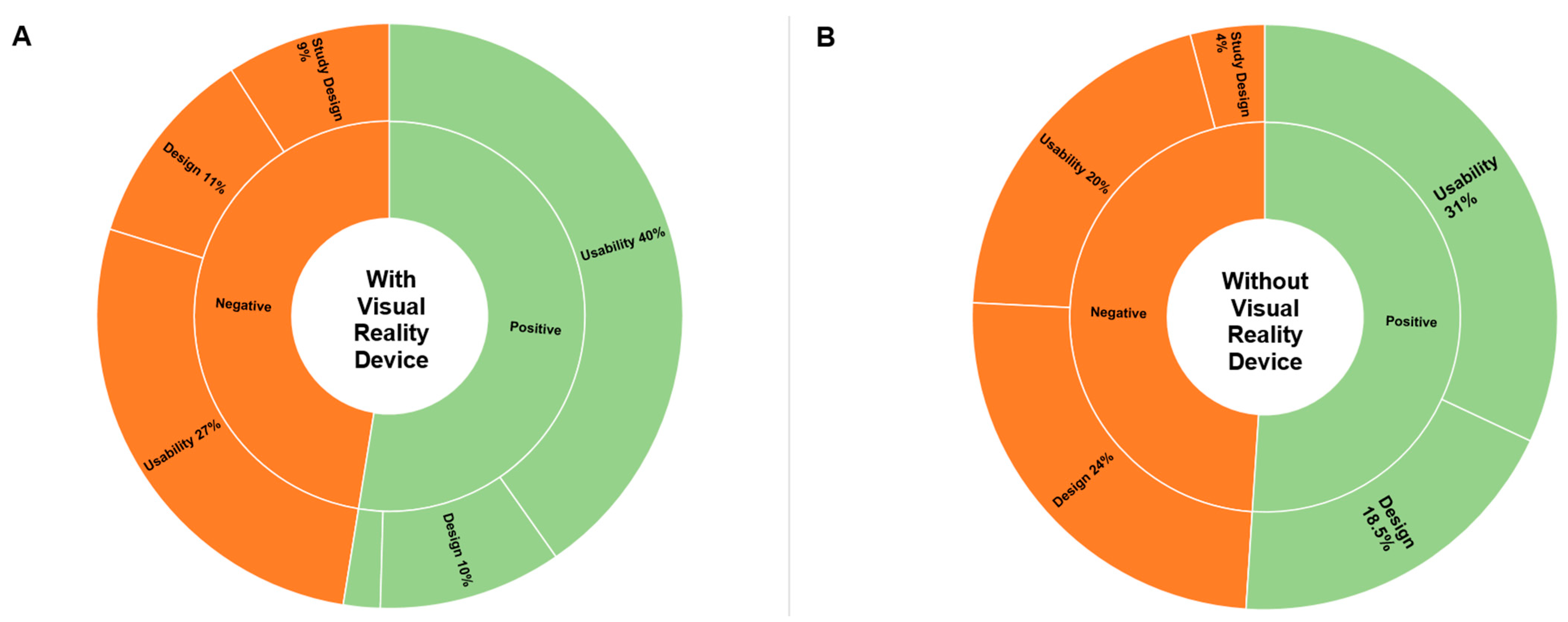
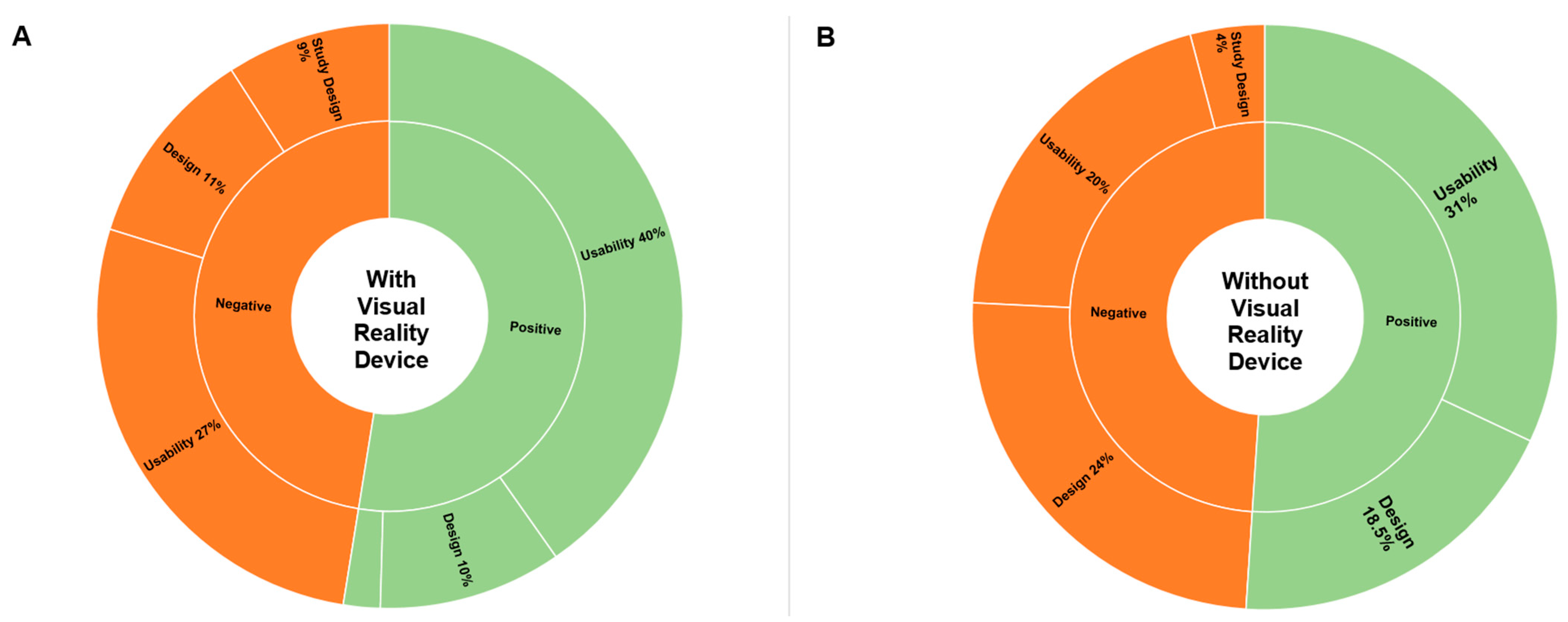
Positive (87/165, 53%)
| Positive (103/200, 52%)
|
Negative (78/165 47%)
| Negative (97/200 48.5%)
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasciauskaite, G.; Lunkiewicz, J.; Schweiger, G.; Budowski, A.D.; Henckert, D.; Roche, T.R.; Bergauer, L.; Meybohm, P.; Hottenrott, S.; Zacharowski, K.; et al. User Perceptions of Visual Blood: An International Mixed Methods Study on Novel Blood Gas Analysis Visualization. Diagnostics 2023, 13, 3103. https://doi.org/10.3390/diagnostics13193103
Gasciauskaite G, Lunkiewicz J, Schweiger G, Budowski AD, Henckert D, Roche TR, Bergauer L, Meybohm P, Hottenrott S, Zacharowski K, et al. User Perceptions of Visual Blood: An International Mixed Methods Study on Novel Blood Gas Analysis Visualization. Diagnostics. 2023; 13(19):3103. https://doi.org/10.3390/diagnostics13193103
Chicago/Turabian StyleGasciauskaite, Greta, Justyna Lunkiewicz, Giovanna Schweiger, Alexandra D. Budowski, David Henckert, Tadzio R. Roche, Lisa Bergauer, Patrick Meybohm, Sebastian Hottenrott, Kai Zacharowski, and et al. 2023. "User Perceptions of Visual Blood: An International Mixed Methods Study on Novel Blood Gas Analysis Visualization" Diagnostics 13, no. 19: 3103. https://doi.org/10.3390/diagnostics13193103
APA StyleGasciauskaite, G., Lunkiewicz, J., Schweiger, G., Budowski, A. D., Henckert, D., Roche, T. R., Bergauer, L., Meybohm, P., Hottenrott, S., Zacharowski, K., Raimann, F. J., Rivas, E., López-Baamonde, M., Ganter, M. T., Schmidt, T., Nöthiger, C. B., Tscholl, D. W., & Akbas, S. (2023). User Perceptions of Visual Blood: An International Mixed Methods Study on Novel Blood Gas Analysis Visualization. Diagnostics, 13(19), 3103. https://doi.org/10.3390/diagnostics13193103