
Identifying Effective Biomarkers for Accurate Pancreatic Cancer Prognosis Using Statistical Machine Learning


Abstract
:1. Introduction
- (1)
- Several clinical and biochemical biomarkers for 30 PC patients belonging to three groups of POCs are reported.
- (2)
- Various statistical and exploratory data analysis techniques are applied to examine and identify the most effective panel of biomarkers for the prediction of POCs among resected PDAC patients.
- (3)
- Statistical ML models are developed and a comparative performance analysis is performed to demonstrate the combined predictive power of the panel of significant biomarkers through an improved PC prognosis accuracy.
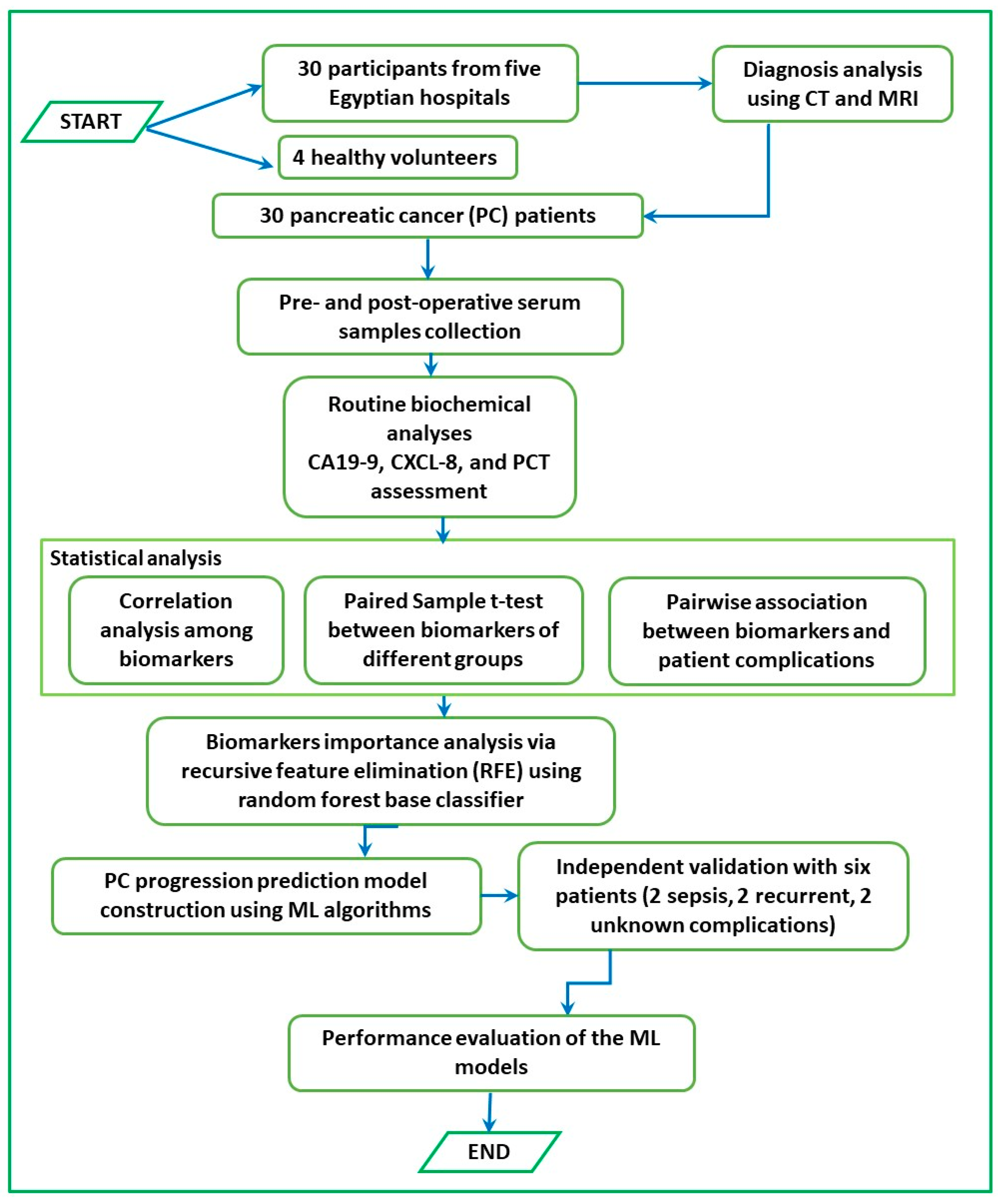
2. Materials and Methods
2.1. Patient Grouping
2.2. Serum Samples
2.3. Biochemical Assays
2.4. Total Leukocyte Count (TLC) Determination
2.5. Quantitative Determination of Serum Immunoglobulins
2.6. Determination of Serum Procalcitonin (PCT)
2.7. Analysis of Serum Tumor Markers
2.7.1. Carbohydrate Antigen 19-9 (CA 19-9)
2.7.2. CXCL-8/IL-8
2.8. Statistical Analysis
2.8.1. Paired Sample t-Test
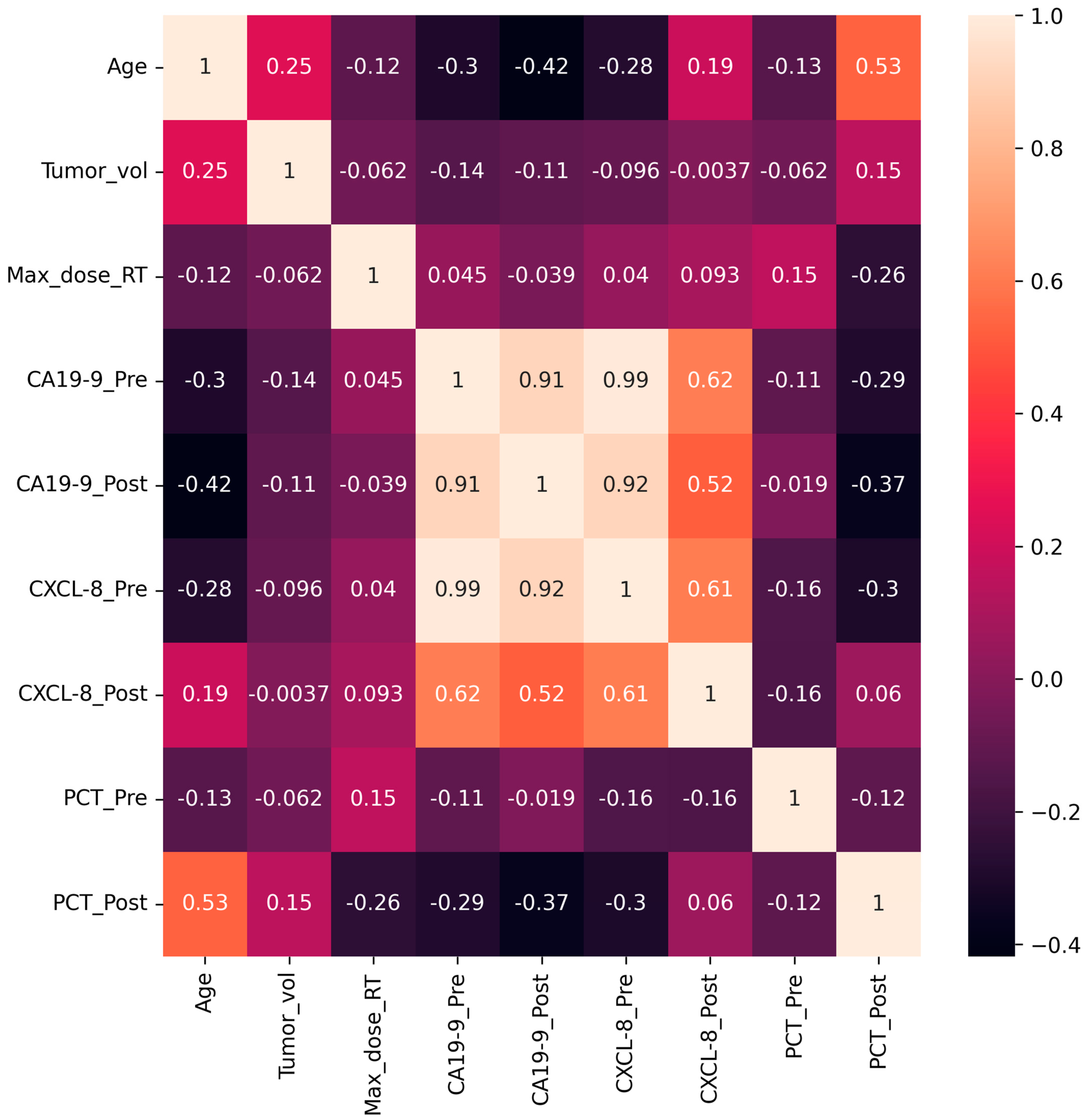
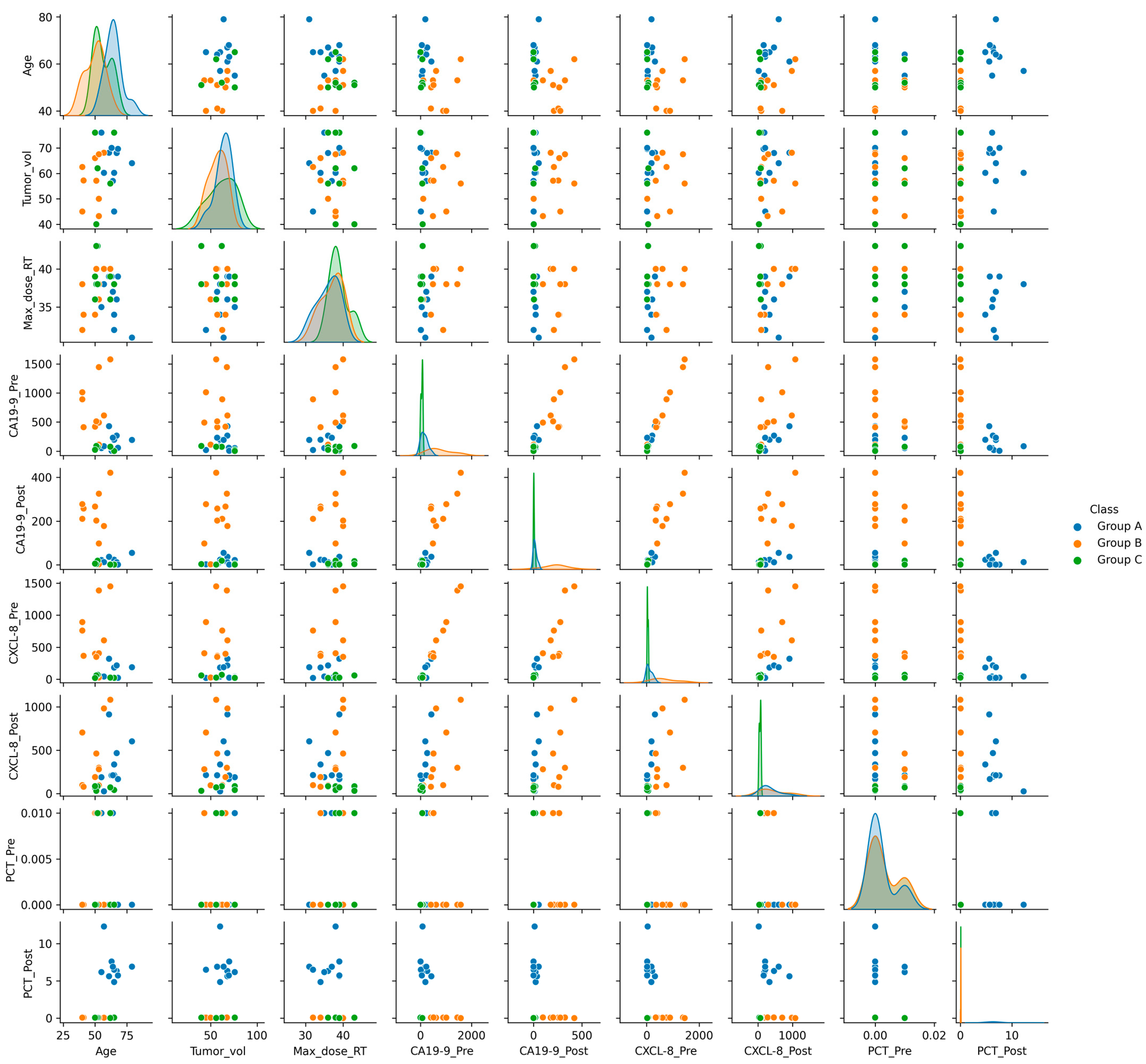
2.8.2. Correlation Analysis
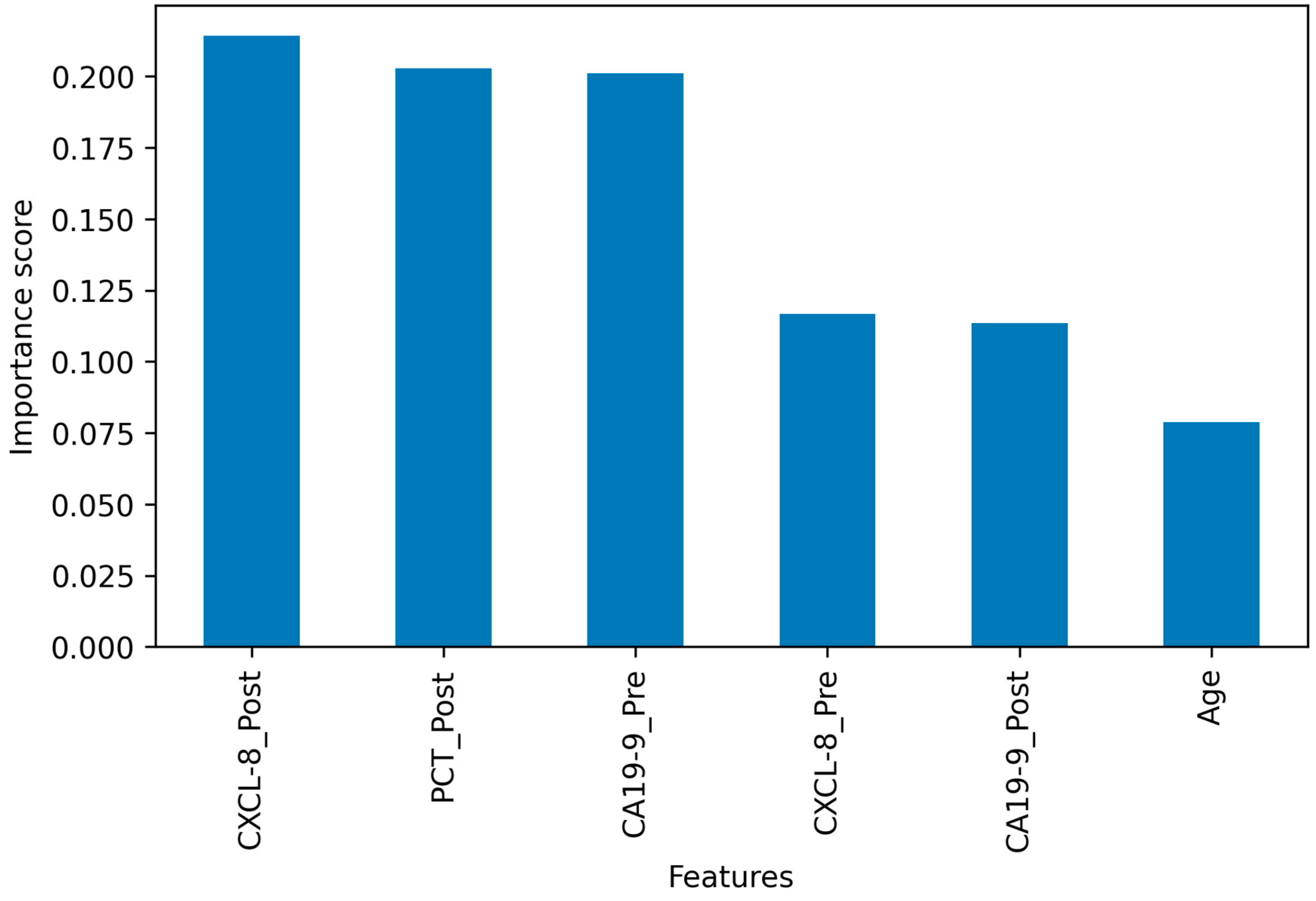
2.8.3. Biomarker Importance Analysis
2.8.4. Statistical ML Modeling
3. Results
3.1. Patient Characteristics and Radiotherapy
3.2. Findings of Biochemical Assays
3.2.1. Biochemical and Serological Parameters
3.2.2. Estimation of Total Leukocyte Count (TLC), Levels of IgG and IgA, and Procalcitonin (PCT)
3.3. Analysis of Serum Tumor Markers
3.3.1. Carbohydrate Antigen 19-9 (CA 19-9)
3.3.2. CXCL-8/IL-8
3.4. Statistical Analysis and Modeling
3.4.1. Paired Sample t-Test of Significant Biomarkers
3.4.2. Correlations between Biomarkers and Patients’ Postoperative Complications
3.4.3. Identification of Important Biomarkers
3.4.4. Statistical Learning for PC Complication Prognosis
4. Discussion
5. Limitations and Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Gao, H.L.; Wang, W.Q.; Yu, X.J.; Liu, L. Molecular drivers and cells of origin in pancreatic ductal adenocarcinoma and pancreatic neuroendocrine carcinoma. Exp. Hematol. Oncol. 2020, 9, 28. [Google Scholar] [CrossRef]
- Freedman, L.S.; Edwards, B.K.; Ries, L.A.G.; Young, J.L. (Eds.) Cancer Incidence in Four Member Countries (Cyprus, Egypt, Israel, and Jordan) of the Middle East Cancer Consortium (MECC) Compared with US SEER; National Cancer Institute: Bethesda, MD, USA, 2006. [Google Scholar]
- Baum, C.; Soliman, A.S.; Brown, H.E.; Seifeldin, I.A.; Ramadan, M.; Lott, B.; Nguyen, A.; El-Ghawalby, A.; Hablas, A. Regional Variation of Pancreatic Cancer Incidence in the Nile Delta Region of Egypt over a Twelve-Year Period. J. Cancer Epidemiol. 2020, 2020, 6031708. [Google Scholar] [CrossRef]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Maisonneuve, P. Epidemiology and burden of pancreatic cancer. Presse Med. 2019, 48 Pt 2, e113–e123. [Google Scholar] [CrossRef]
- Yang, H.; Li, W.; Ren, L.; Yang, Y.; Zhang, Y.; Ge, B.; Li, S.; Zheng, X.; Liu, J.; Zhang, S.; et al. Progress on diagnostic and prognostic markers of pancreatic cancer. Oncol. Res. 2023, 31, 83–99. [Google Scholar] [CrossRef]
- Winter, J.M.; Yeo, C.J.; Brody, J.R. Diagnostic, prognostic, and predictive biomarkers in pancreatic cancer. J. Surg. Oncol. 2013, 107, 15–22. [Google Scholar] [CrossRef]
- Xiang, J.F.; Wang, W.Q.; Liu, L.; Xu, H.X.; Wu, C.T.; Yang, J.X.; Qi, Z.H.; Wang, Y.Q.; Xu, J.; Liu, C.; et al. Mutant p53 determines pancreatic cancer poor prognosis to pancreatectomy through upregulation of cavin-1 in patients with preoperative serum CA19-9 ≥ 1000 U/mL. Sci. Rep. 2016, 6, 19222. [Google Scholar] [CrossRef]
- Tomishima, K.; Ishii, S.; Fujisawa, T.; Ikemura, M.; Ota, H.; Kabemura, D.; Ushio, M.; Fukuma, T.; Takahashi, S.; Yamagata, W.; et al. Duration of Reduced CA19-9 Levels Is a Better Prognostic Factor Than Its Rate of Reduction for Unresectable Locally Advanced Pancreatic Cancer. Cancers 2021, 13, 4224. [Google Scholar] [CrossRef]
- Ye, C.; Sadula, A.; Ren, S.; Guo, X.; Yuan, M.; Yuan, C.; Xiu, D. The prognostic value of CA19-9 response after neoadjuvant therapy in patients with pancreatic cancer: A systematic review and pooled analysis. Cancer Chemother. Pharmacol. 2020, 86, 731–740. [Google Scholar] [CrossRef]
- Kim, Y.J.; Koh, H.K.; Chie, E.K.; Oh, D.Y.; Bang, Y.J.; Nam, E.M.; Kim, K. Change in carbohydrate antigen 19-9 level as a prognostic marker of overall survival in locally advanced pancreatic cancer treated with concurrent chemoradiotherapy. Int. J. Clin. Oncol. 2017, 22, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Azizian, A.; Ruhlmann, F.; Krause, T.; Bernhardt, M.; Jo, P.; Konig, A.; Kleiss, M.; Leha, A.; Ghadimi, M.; Gaedcke, J. CA19-9 for detecting recurrence of pancreatic cancer. Sci. Rep. 2020, 10, 1332. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.M.; Wang, H.; Li, R.; Pan, G. Prognostic Role of Carbohydrate Antigen 19 to 9 in Predicting Survival of Patients With Pancreatic Cancer: A Meta-Analysis. Technol. Cancer Res. Treat. 2021, 20, 15330338211043030. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.Y.; Huang, S.P.; Chiu, H.M.; Lee, Y.C.; Chen, M.F.; Lin, J.T. Low efficacy of serum levels of CA 19-9 in prediction of malignant diseases in asymptomatic population in Taiwan. Hepatogastroenterology 2006, 53, 1–4. [Google Scholar]
- Kim, J.E.; Lee, K.T.; Lee, J.K.; Paik, S.W.; Rhee, J.C.; Choi, K.W. Clinical usefulness of carbohydrate antigen 19-9 as a screening test for pancreatic cancer in an asymptomatic population. J. Gastroenterol. Hepatol. 2004, 19, 182–186. [Google Scholar] [CrossRef]
- Bunger, S.; Laubert, T.; Roblick, U.J.; Habermann, J.K. Serum biomarkers for improved diagnostic of pancreatic cancer: A current overview. J. Cancer Res. Clin. Oncol. 2011, 137, 375–389. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yang, J.; Li, H.; Wu, Y.; Zhang, H.; Chen, W. Tumor markers CA19-9, CA242 and CEA in the diagnosis of pancreatic cancer: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 11683–11691. [Google Scholar]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef]
- Stone, M.L.; Beatty, G.L. Cellular determinants and therapeutic implications of inflammation in pancreatic cancer. Pharmacol. Ther. 2019, 201, 202–213. [Google Scholar] [CrossRef]
- Whittle, M.C.; Hingorani, S.R. Fibroblasts in Pancreatic Ductal Adenocarcinoma: Biological Mechanisms and Therapeutic Targets. Gastroenterology 2019, 156, 2085–2096. [Google Scholar] [CrossRef]
- Velasco, R.M.; Garcia, A.G.; Sanchez, P.J.; Sellart, I.M.; Sanchez-Arevalo Lobo, V.J. Tumour microenvironment and heterotypic interactions in pancreatic cancer. J. Physiol. Biochem. 2023, 79, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Stopa, K.B.; Kusiak, A.A.; Szopa, M.D.; Ferdek, P.E.; Jakubowska, M.A. Pancreatic Cancer and Its Microenvironment-Recent Advances and Current Controversies. Int. J. Mol. Sci. 2020, 21, 3218. [Google Scholar] [CrossRef] [PubMed]
- Yako, Y.Y.; Kruger, D.; Smith, M.; Brand, M. Cytokines as Biomarkers of Pancreatic Ductal Adenocarcinoma: A Systematic Review. PLoS ONE 2016, 11, e0154016. [Google Scholar] [CrossRef]
- Dima, S.O.; Tanase, C.; Albulescu, R.; Herlea, V.; Chivu-Economescu, M.; Purnichescu-Purtan, R.; Dumitrascu, T.; Duda, D.G.; Popescu, I. An exploratory study of inflammatory cytokines as prognostic biomarkers in patients with ductal pancreatic adenocarcinoma. Pancreas 2012, 41, 1001–1007. [Google Scholar] [CrossRef]
- Feng, L.; Qi, Q.; Wang, P.; Chen, H.; Chen, Z.; Meng, Z.; Liu, L. Serum levels of IL-6, IL-8, and IL-10 are indicators of prognosis in pancreatic cancer. J. Int. Med. Res. 2018, 46, 5228–5236. [Google Scholar] [CrossRef] [PubMed]
- van Duijneveldt, G.; Griffin, M.D.W.; Putoczki, T.L. Emerging roles for the IL-6 family of cytokines in pancreatic cancer. Clin. Sci. 2020, 134, 2091–2115. [Google Scholar] [CrossRef]
- Litman-Zawadzka, A.; Lukaszewicz-Zajac, M.; Gryko, M.; Kulczynska-Przybik, A.; Mroczko, B. Serum chemokine CXCL8 as a better biomarker for diagnosis and prediction of pancreatic cancer than its specific receptor CXCR2, C-reactive protein, and classic tumor markers CA 19-9 and CEA. Pol. Arch. Intern. Med. 2018, 128, 524–531. [Google Scholar]
- Yang, C.; Bork, U.; Scholch, S.; Kulu, Y.; Kaderali, L.; Bolstorff, U.L.; Kahlert, C.; Weitz, J.; Rahbari, N.N.; Reissfelder, C. Postoperative course and prognostic value of circulating angiogenic cytokines after pancreatic cancer resection. Oncotarget 2017, 8, 72315–72323. [Google Scholar] [CrossRef]
- Lewis, H.L.; Chakedis, J.M.; Talbert, E.; Haverick, E.; Rajasekera, P.; Hart, P.; Bloomston, M.; Dillhoff, M.; Pawlik, T.M.; Guttridge, D.; et al. Perioperative cytokine levels portend early death after pancreatectomy for ductal adenocarcinoma. J. Surg. Oncol. 2018, 117, 1260–1266. [Google Scholar] [CrossRef]
- Jing, Y.; Wang, F.; Zhang, K.; Chen, Z. Comprehensive analysis of prognostic value and immune infiltration of CXC chemokines in pancreatic cancer. BMC Med. Genom. 2022, 15, 96. [Google Scholar] [CrossRef]
- Yin, Z.; Chen, S. Therapeutic Targets and Prognostic Biomarkers Among CXC Chemokines in Pancreatic Ductal Adenocarcinoma Microenvironment. Pancreas 2022, 51, 1235–1247. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Jarczak, D.; Kluge, S.; Nierhaus, A. Sepsis-Pathophysiology and Therapeutic Concepts. Front. Med. 2021, 8, 628302. [Google Scholar] [CrossRef] [PubMed]
- Mirijello, A.; Tosoni, A.; on Behalf of The Internal Medicine Sepsis Study Group. New Strategies for Treatment of Sepsis. Medicina 2020, 56, 527. [Google Scholar] [CrossRef] [PubMed]
- Teggert, A.; Datta, H.; Ali, Z. Biomarkers for Point-of-Care Diagnosis of Sepsis. Micromachines 2020, 11, 286. [Google Scholar] [CrossRef] [PubMed]
- Agnello, L.; Ciaccio, M. Biomarkers of Sepsis. Diagnostics 2023, 13, 435. [Google Scholar] [CrossRef] [PubMed]
- Arina, P.; Singer, M. Pathophysiology of sepsis. Curr. Opin. Anaesthesiol. 2021, 34, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Cai, S.; Su, J. The Pathogenesis of Sepsis and Potential Therapeutic Targets. Int. J. Mol. Sci. 2019, 20, 5376. [Google Scholar] [CrossRef]
- Dolin, H.H.; Papadimos, T.J.; Chen, X.; Pan, Z.K. Characterization of Pathogenic Sepsis Etiologies and Patient Profiles: A Novel Approach to Triage and Treatment. Microbiol. Insights 2019, 12, 1178636118825081. [Google Scholar] [CrossRef]
- Gudiol, C.; Albasanz-Puig, A.; Cuervo, G.; Carratala, J. Understanding and Managing Sepsis in Patients With Cancer in the Era of Antimicrobial Resistance. Front. Med. 2021, 8, 636547. [Google Scholar] [CrossRef]
- Danai, P.A.; Moss, M.; Mannino, D.M.; Martin, G.S. The epidemiology of sepsis in patients with malignancy. Chest 2006, 129, 1432–1440. [Google Scholar] [CrossRef]
- Meyer, N.; Harhay, M.O.; Small, D.S.; Prescott, H.C.; Bowles, K.H.; Gaieski, D.F.; Mikkelsen, M.E. Temporal Trends in Incidence, Sepsis-Related Mortality, and Hospital-Based Acute Care After Sepsis. Crit. Care Med. 2018, 46, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Mestanza, C.; Andaluz-Ojeda, D.; Gomez-Lopez, J.R.; Bermejo-Martin, J.F. Clinical factors influencing mortality risk in hospital-acquired sepsis. J. Hosp. Infect. 2018, 98, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Namendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.N.; Vincent, J.L.; et al. Sepsis in Intensive Care Unit Patients: Worldwide Data From the Intensive Care over Nations Audit. Open Forum Infect. Dis. 2018, 5, ofy313. [Google Scholar] [CrossRef]
- Riedel, S.; Carroll, K.C. Blood cultures: Key elements for best practices and future directions. J. Infect. Chemother. 2010, 16, 301–316. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Carlet, J.M.; Bion, J.; Parker, M.M.; Jaeschke, R.; Reinhart, K.; Angus, D.C.; Brun-Buisson, C.; Beale, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 2008, 34, 17–60. [Google Scholar] [CrossRef]
- Garcia, R.A.; Spitzer, E.D.; Beaudry, J.; Beck, C.; Diblasi, R.; Gilleeny-Blabac, M.; Haugaard, C.; Heuschneider, S.; Kranz, B.P.; McLean, K.; et al. Multidisciplinary team review of best practices for collection and handling of blood cultures to determine effective interventions for increasing the yield of true-positive bacteremias, reducing contamination, and eliminating false-positive central line-associated bloodstream infections. Am. J. Infect. Control 2015, 43, 1222–1237. [Google Scholar]
- Gunsolus, I.L.; Sweeney, T.E.; Liesenfeld, O.; Ledeboer, N.A. Diagnosing and Managing Sepsis by Probing the Host Response to Infection: Advances, Opportunities, and Challenges. J. Clin. Microbiol. 2019, 57, e00425-19. [Google Scholar] [CrossRef] [PubMed]
- Leong, K.; Gaglani, B.; Khanna, A.K.; McCurdy, M.T. Novel Diagnostics and Therapeutics in Sepsis. Biomedicines 2021, 9, 311. [Google Scholar] [CrossRef]
- Watkins, R.R.; Bonomo, R.A.; Rello, J. Managing sepsis in the era of precision medicine: Challenges and opportunities. Expert Rev. Anti Infect. Ther. 2022, 20, 871–880. [Google Scholar] [CrossRef]
- Eubank, T.A.; Long, S.W.; Perez, K.K. Role of Rapid Diagnostics in Diagnosis and Management of Patients With Sepsis. J. Infect. Dis. 2020, 222 (Suppl. S2), S103–S109. [Google Scholar] [CrossRef]
- Broyles, M.R. Impact of Procalcitonin-Guided Antibiotic Management on Antibiotic Exposure and Outcomes: Real-world Evidence. Open Forum Infect. Dis. 2017, 4, ofx213. [Google Scholar] [CrossRef]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: A patient level meta-analysis. Lancet Infect. Dis. 2018, 18, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Fioretto, J.R.; Martin, J.G.; Kurokawa, C.S.; Carpi, M.F.; Bonatto, R.C.; de Moraes, M.A.; Ricchetti, S.M. Comparison between procalcitonin and C-reactive protein for early diagnosis of children with sepsis or septic shock. Inflamm. Res. 2010, 59, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Riedel, S.; Carroll, K.C. Laboratory detection of sepsis: Biomarkers and molecular approaches. Clin. Lab. Med. 2013, 33, 413–437. [Google Scholar] [CrossRef] [PubMed]
- Nargis, W.; Ibrahim, M.; Ahamed, B.U. Procalcitonin versus C-reactive protein: Usefulness as biomarker of sepsis in ICU patient. Int. J. Crit. Illn. Inj. Sci. 2014, 4, 195–199. [Google Scholar] [CrossRef]
- Liu, D.; Su, L.; Han, G.; Yan, P.; Xie, L. Prognostic Value of Procalcitonin in Adult Patients with Sepsis: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0129450. [Google Scholar] [CrossRef]
- Sager, R.; Wirz, Y.; Amin, D.; Amin, A.; Hausfater, P.; Huber, A.; Haubitz, S.; Kutz, A.; Mueller, B.; Schuetz, P. Are admission procalcitonin levels universal mortality predictors across different medical emergency patient populations? Results from the multi-national, prospective, observational TRIAGE study. Clin. Chem. Lab. Med. 2017, 55, 1873–1880. [Google Scholar] [CrossRef]
- Memar, M.Y.; Baghi, H.B. Presepsin: A promising biomarker for the detection of bacterial infections. Biomed. Pharmacother. 2019, 111, 649–656. [Google Scholar] [CrossRef]
- Bauer, P.R.; Kashyap, R.; League, S.C.; Park, J.G.; Block, D.R.; Baumann, N.A.; Algeciras-Schimnich, A.; Jenkins, S.M.; Smith, C.Y.; Gajic, O.; et al. Diagnostic accuracy and clinical relevance of an inflammatory biomarker panel for sepsis in adult critically ill patients. Diagn. Microbiol. Infect. Dis. 2016, 84, 175–180. [Google Scholar] [CrossRef]
- Jedynak, M.; Siemiatkowski, A.; Milewski, R.; Mroczko, B.; Szmitkowski, M. Diagnostic effectiveness of soluble triggering receptor expressed on myeloid cells-1 in sepsis, severe sepsis and septic shock. Arch. Med. Sci. 2019, 15, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Xiong, H.; Yan, P.; Shuai, T.; Liu, J.; Zhu, L.; Lu, J.; Yang, K.; Liu, J. The Diagnostic and Prognostic Value of suPAR in Patients with Sepsis: A Systematic Review and Meta-Analysis. Shock 2020, 53, 416–425. [Google Scholar] [CrossRef]
- Taneja, R.; Batra, P. Biomarkers as point of care tests (POCT) in neonatal sepsis: A state of science review. J. Neonatal Perinat. Med. 2021, 14, 331–338. [Google Scholar] [CrossRef]
- Zhang, Y.; Khalid, S.; Jiang, L. Diagnostic and predictive performance of biomarkers in patients with sepsis in an intensive care unit. J. Int. Med. Res. 2019, 47, 44–58. [Google Scholar] [CrossRef] [PubMed]
- Gaur, K.; Jagtap, M.M. Role of Artificial Intelligence and Machine Learning in Prediction, Diagnosis, and Prognosis of Cancer. Cureus 2022, 14, e31008. [Google Scholar] [CrossRef]
- Alpaydin, E. Introduction to Machine Learning, 4th ed.; MIT Press: Cambridge, MA, USA; London, UK, 2020. [Google Scholar]
- Ahmad, M.; Khan, Z.; Rahman, Z.U.; Khattak, S.I.; Khan, Z.U. Can innovation shocks determine CO2 emissions (CO2e) in the OECD economies? A new perspective. Econ. Innov. New Technol. 2021, 30, 89–109. [Google Scholar] [CrossRef]
- Dlamini, Z.; Francies, F.Z.; Hull, R.; Marima, R. Artificial intelligence (AI) and big data in cancer and precision oncology. Comput. Struct. Biotechnol. J. 2020, 18, 2300–2311. [Google Scholar] [CrossRef]
- Yu, C.; Helwig, E.J. The role of AI technology in prediction, diagnosis and treatment of colorectal cancer. Artif. Intell. Rev. 2022, 55, 323–343. [Google Scholar] [CrossRef]
- Majumder, A.; Sen, D. Artificial intelligence in cancer diagnostics and therapy: Current perspectives. Indian J. Cancer 2021, 58, 481–492. [Google Scholar]
- Wang, L.; Song, Y.; Wang, H.; Zhang, X.; Wang, M.; He, J.; Li, S.; Zhang, L.; Li, K.; Cao, L. Advances of Artificial Intelligence in Anti-Cancer Drug Design: A Review of the Past Decade. Pharmaceuticals 2023, 16, 253. [Google Scholar] [CrossRef]
- Zhang, H.; Ji, J.; Liu, Z.; Lu, H.; Qian, C.; Wei, C.; Chen, S.; Lu, W.; Wang, C.; Xu, H.; et al. Artificial intelligence for the diagnosis of clinically significant prostate cancer based on multimodal data: A multicenter study. BMC Med. 2023, 21, 270. [Google Scholar] [CrossRef] [PubMed]
- Lehman, C.D.; Mercaldo, S.; Lamb, L.R.; King, T.A.; Ellisen, L.W.; Specht, M.; Tamimi, R.M. Deep Learning vs Traditional Breast Cancer Risk Models to Support Risk-Based Mammography Screening. J. Natl. Cancer Inst. 2022, 114, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Buk Cardoso, L.; Cunha Parro, V.; Verzinhasse Peres, S.; Curado, M.P.; Fernandes, G.A.; Wunsch Filho, V.; Natasha Toporcov, T. Machine learning for predicting survival of colorectal cancer patients. Sci. Rep. 2023, 13, 8874. [Google Scholar] [CrossRef]
- Doan, L.M.T.; Angione, C.; Occhipinti, A. Machine Learning Methods for Survival Analysis with Clinical and Transcriptomics Data of Breast Cancer. Methods Mol. Biol. 2023, 2553, 325–393. [Google Scholar]
- Bao, L.; Wang, Y.T.; Zhuang, J.L.; Liu, A.J.; Dong, Y.J.; Chu, B.; Chen, X.H.; Lu, M.Q.; Shi, L.; Gao, S.; et al. Machine Learning-Based Overall Survival Prediction of Elderly Patients With Multiple Myeloma From Multicentre Real-Life Data. Front. Oncol. 2022, 12, 922039. [Google Scholar] [CrossRef]
- Zhu, F.; Zhong, R.; Li, F.; Li, C.; Din, N.; Sweidan, H.; Potluri, L.B.; Xiong, S.; Li, J.; Cheng, B.; et al. Development and validation of a deep transfer learning-based multivariable survival model to predict overall survival in lung cancer. Transl. Lung Cancer Res. 2023, 12, 471–482. [Google Scholar] [CrossRef]
- Zhang, B.; Shi, H.; Wang, H. Machine Learning and AI in Cancer Prognosis, Prediction, and Treatment Selection: A Critical Approach. J. Multidiscip. Healthc. 2023, 16, 1779–1791. [Google Scholar] [CrossRef]
- Zeng, J.; Li, K.; Cao, F.; Zheng, Y. Development and validation of survival prediction model for gastric adenocarcinoma patients using deep learning: A SEER-based study. Front. Oncol. 2023, 13, 1131859. [Google Scholar] [CrossRef]
- Ma, H.; Liu, Z.X.; Zhang, J.J.; Wu, F.T.; Xu, C.F.; Shen, Z.; Yu, C.H.; Li, Y.M. Construction of a convolutional neural network classifier developed by computed tomography images for pancreatic cancer diagnosis. World J. Gastroenterol. 2020, 26, 5156–5168. [Google Scholar] [CrossRef]
- Viriyasaranon, T.; Chun, J.W.; Koh, Y.H.; Cho, J.H.; Jung, M.K.; Kim, S.H.; Kim, H.J.; Lee, W.J.; Choi, J.H.; Woo, S.M. Annotation-Efficient Deep Learning Model for Pancreatic Cancer Diagnosis and Classification Using CT Images: A Retrospective Diagnostic Study. Cancers 2023, 15, 3392. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.; Gu, J.; Xu, D.; Song, L.; Zhao, Q.; Cheng, F.; Yuan, Z.; Tian, S.; Yang, X.; Tian, J.; et al. Deep learning radiomics based on contrast-enhanced ultrasound images for assisted diagnosis of pancreatic ductal adenocarcinoma and chronic pancreatitis. BMC Med. 2022, 20, 74. [Google Scholar] [CrossRef] [PubMed]
- Kriegsmann, M.; Kriegsmann, K.; Steinbuss, G.; Zgorzelski, C.; Kraft, A.; Gaida, M.M. Deep Learning in Pancreatic Tissue: Identification of Anatomical Structures, Pancreatic Intraepithelial Neoplasia, and Ductal Adenocarcinoma. Int. J. Mol. Sci. 2021, 22, 5385. [Google Scholar] [CrossRef] [PubMed]
- Niazi, M.K.K.; Tavolara, T.E.; Arole, V.; Hartman, D.J.; Pantanowitz, L.; Gurcan, M.N. Identifying tumor in pancreatic neuroendocrine neoplasms from Ki67 images using transfer learning. PLoS ONE 2018, 13, e0195621. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Tsuneki, M.; Fukushima, N.; Koga, Y.; Higashi, M.; Notohara, K.; Aishima, S.; Ohike, N.; Tajiri, T.; Yamaguchi, H.; et al. A deep learning model to detect pancreatic ductal adenocarcinoma on endoscopic ultrasound-guided fine-needle biopsy. Sci. Rep. 2021, 11, 8454. [Google Scholar] [CrossRef]
- Yang, Z.; LaRiviere, M.J.; Ko, J.; Till, J.E.; Christensen, T.; Yee, S.S.; Black, T.A.; Tien, K.; Lin, A.; Shen, H.; et al. A Multianalyte Panel Consisting of Extracellular Vesicle miRNAs and mRNAs, cfDNA, and CA19-9 Shows Utility for Diagnosis and Staging of Pancreatic Ductal Adenocarcinoma. Clin. Cancer Res. 2020, 26, 3248–3258. [Google Scholar] [CrossRef]
- Mori, Y.; Yokota, H.; Hoshino, I.; Iwatate, Y.; Wakamatsu, K.; Uno, T.; Suyari, H. Deep learning-based gene selection in comprehensive gene analysis in pancreatic cancer. Sci. Rep. 2021, 11, 16521. [Google Scholar] [CrossRef]
- Huang, J.; Zhou, Y.; Zhang, H.; Wu, Y. A neural network model to screen feature genes for pancreatic cancer. BMC Bioinform. 2023, 24, 193. [Google Scholar] [CrossRef]
- Hossen, B.; Islam, A.; Reza, S.; Kibria, K.; Horaira, A.; Tuly, K.F.; Faruqe, M.O.; Kabir, F.; Mollah, N.H. Robust identification of common genomic biomarkers from multiple gene expression profiles for the prognosis, diagnosis, and therapies of pancreatic cancer. Comput. Biol. Med. 2023, 152, 106411. [Google Scholar] [CrossRef]
- Iwatate, Y.; Yokota, H.; Hoshino, I.; Ishige, F.; Kuwayama, N.; Itami, M.; Mori, Y.; Chiba, S.; Arimitsu, H.; Yanagibashi, H.; et al. Machine learning with imaging features to predict the expression of ITGAV, which is a poor prognostic factor derived from transcriptome analysis in pancreatic cancer. Int. J. Oncol. 2022, 60, 1–13. [Google Scholar] [CrossRef]
- Kernbach, J.M.; Staartjes, V.E. Predicted Prognosis of Pancreatic Cancer Patients by Machine Learning-Letter. Clin. Cancer Res. 2020, 26, 3891. [Google Scholar] [CrossRef] [PubMed]
- Bakasa, W.; Viriri, S. Pancreatic Cancer Survival Prediction: A Survey of the State-of-the-Art. Comput. Math. Methods Med. 2021, 2021, 1188414. [Google Scholar] [CrossRef] [PubMed]
- Keyl, J.; Kasper, S.; Wiesweg, M.; Gotze, J.; Schonrock, M.; Sinn, M.; Berger, A.; Nasca, E.; Kostbade, K.; Schumacher, B.; et al. Multimodal survival prediction in advanced pancreatic cancer using machine learning. ESMO Open 2022, 7, 100555. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Jang, J.Y.; Yu, Y.D.; Heo, J.S.; Han, H.S.; Yoon, Y.S.; Kang, C.M.; Hwang, H.K.; Kang, S. Usefulness of artificial intelligence for predicting recurrence following surgery for pancreatic cancer: Retrospective cohort study. Int. J. Surg. 2021, 93, 106050. [Google Scholar] [CrossRef]
- Huang, L.; Yuan, X.; Zhao, L.; Han, Q.; Yan, H.; Yuan, J.; Guan, S.; Xu, X.; Dai, G.; Wang, J.; et al. Gene signature developed for predicting early relapse and survival in early-stage pancreatic cancer. BJS Open 2023, 7, zrad031. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Yang, M.; Ji, L.; Fan, H. A multi-omics machine learning framework in predicting the recurrence and metastasis of patients with pancreatic adenocarcinoma. Front. Microbiol. 2022, 13, 1032623. [Google Scholar] [CrossRef]
- An, C.; Li, D.; Li, S.; Li, W.; Tong, T.; Liu, L.; Jiang, D.; Jiang, L.; Ruan, G.; Hai, N.; et al. Deep learning radiomics of dual-energy computed tomography for predicting lymph node metastases of pancreatic ductal adenocarcinoma. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1187–1199. [Google Scholar] [CrossRef] [PubMed]
- Zambirinis, C.P.; Midya, A.; Chakraborty, J.; Chou, J.F.; Zheng, J.; McIntyre, C.A.; Koszalka, M.A.; Wang, T.; Do, R.K.; Balachandran, V.P.; et al. Recurrence After Resection of Pancreatic Cancer: Can Radiomics Predict Patients at Greatest Risk of Liver Metastasis? Ann. Surg. Oncol. 2022, 29, 4962–4974. [Google Scholar] [CrossRef] [PubMed]
- Gregucci, F.; Fiorentino, A.; Mazzola, R.; Ricchetti, F.; Bonaparte, I.; Surgo, A.; Figlia, V.; Carbonara, R.; Caliandro, M.; Ciliberti, M.P.; et al. Radiomic analysis to predict local response in locally advanced pancreatic cancer treated with stereotactic body radiation therapy. Radiol. Med. 2022, 127, 100–107. [Google Scholar] [CrossRef]
- Shao, Y.; Dang, Y.; Cheng, Y.; Gui, Y.; Chen, X.; Chen, T.; Zeng, Y.; Tan, L.; Zhang, J.; Xiao, M.; et al. Predicting the Efficacy of Neoadjuvant Chemotherapy for Pancreatic Cancer Using Deep Learning of Contrast-Enhanced Ultrasound Videos. Diagnostics 2023, 13, 2183. [Google Scholar] [CrossRef]
- Simpson, G.; Jin, W.; Spieler, B.; Portelance, L.; Mellon, E.; Kwon, D.; Ford, J.C.; Dogan, N. Predictive Value of Delta-Radiomics Texture Features in 0.35 Tesla Magnetic Resonance Setup Images Acquired During Stereotactic Ablative Radiotherapy of Pancreatic Cancer. Front. Oncol. 2022, 12, 807725. [Google Scholar] [CrossRef] [PubMed]
- Kaissis, G.; Ziegelmayer, S.; Lohofer, F.; Steiger, K.; Algul, H.; Muckenhuber, A.; Yen, H.Y.; Rummeny, E.; Friess, H.; Schmid, R.; et al. A machine learning algorithm predicts molecular subtypes in pancreatic ductal adenocarcinoma with differential response to gemcitabine-based versus FOLFIRINOX chemotherapy. PLoS ONE 2019, 14, e0218642. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, G.; Scoppettuolo, M.N.; Cammarota, A.L.; Rosati, A.; Palmieri, F. A genetic programming-based approach for classifying pancreatic adenocarcinoma: The SICED experience. Soft Comput. 2022, 26, 10063–10074. [Google Scholar] [CrossRef]
- Chen, X.; Lin, X.; Shen, Q.; Qian, X. Combined Spiral Transformation and Model-Driven Multi-Modal Deep Learning Scheme for Automatic Prediction of TP53 Mutation in Pancreatic Cancer. IEEE Trans. Med. Imaging 2021, 40, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Xing, F.; Xie, Y.; Yang, L. An Automatic Learning-Based Framework for Robust Nucleus Segmentation. IEEE Trans. Med. Imaging 2016, 35, 550–566. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, T.; Kouzahkanan, Z.M.; Radmard, A.R.; Kafieh, R.; Salehnia, A.; Davarpanah, A.H.; Arabalibeik, H.; Ahmadian, A. Segmentation of pancreatic ductal adenocarcinoma (PDAC) and surrounding vessels in CT images using deep convolutional neural networks and texture descriptors. Sci. Rep. 2022, 12, 3092. [Google Scholar] [CrossRef]
- Zhao, W.; Shen, L.; Han, B.; Yang, Y.; Cheng, K.; Toesca, D.A.S.; Koong, A.C.; Chang, D.T.; Xing, L. Markerless Pancreatic Tumor Target Localization Enabled By Deep Learning. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 432–439. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhu, S.; Yuan, Z.; Li, Q.; Ding, R.; Bao, X.; Zhen, T.; Fu, Z.; Fu, H.; Xing, K.; et al. Risk factors and socio-economic burden in pancreatic ductal adenocarcinoma operation: A machine learning based analysis. BMC Cancer 2020, 20, 1161. [Google Scholar] [CrossRef]
- Neeman, U.; Lahat, G.; Goykhman, Y.; Geva, R.; Peles-Avraham, S.; Nachmany, I.; Nakache, R.; Klausner, J.M.; Lubezky, N. Prognostic significance of pancreatic fistula and postoperative complications after pancreaticoduodenectomy in patients with pancreatic ductal adenocarcinoma. Surgeon 2020, 18, 24–30. [Google Scholar] [CrossRef]
- Coppola, A.; Farolfi, T.; La Vaccara, V.; Iannone, I.; Giovinazzo, F.; Panettieri, E.; Tarallo, M.; Cammarata, R.; Coppola, R.; Caputo, D. Neoadjuvant Treatments for Pancreatic Ductal Adenocarcinoma: Where We Are and Where We Are Going. J. Clin. Med. 2023, 12, 3677. [Google Scholar] [CrossRef]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Coles, E.H. Veterinary Clinical Pathology, 4th ed.; W.B. Saunders Company: Philadelphia, PA, USA, 1986. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn Res. 2011, 12, 2825–2830. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference, and Prediction, 2nd ed.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Martin-Perez, E.; Dominguez-Munoz, J.E.; Botella-Romero, F.; Cerezo, L.; Matute Teresa, F.; Serrano, T.; Vera, R. Multidisciplinary consensus statement on the clinical management of patients with pancreatic cancer. Clin. Transl. Oncol. 2020, 22, 1963–1975. [Google Scholar] [CrossRef]
- Varadhachary, G.R.; Tamm, E.P.; Abbruzzese, J.L.; Xiong, H.Q.; Crane, C.H.; Wang, H.; Lee, J.E.; Pisters, P.W.; Evans, D.B.; Wolff, R.A. Borderline resectable pancreatic cancer: Definitions, management, and role of preoperative therapy. Ann. Surg. Oncol. 2006, 13, 1035–1046. [Google Scholar] [CrossRef]
- Giuliano, K.; Ejaz, A.; He, J. Technical aspects of pancreaticoduodenectomy and their outcomes. Chin. Clin. Oncol. 2017, 6, 64. [Google Scholar] [CrossRef]
- Schorn, S.; Demir, I.E.; Vogel, T.; Schirren, R.; Reim, D.; Wilhelm, D.; Friess, H.; Ceyhan, G.O. Mortality and postoperative complications after different types of surgical reconstruction following pancreaticoduodenectomy-a systematic review with meta-analysis. Langenbecks Arch. Surg. 2019, 404, 141–157. [Google Scholar] [CrossRef]
- Cardini, B.; Primavesi, F.; Maglione, M.; Oberschmied, J.; Guschlbauer, L.; Gasteiger, S.; Kuscher, S.; Resch, T.; Oberhuber, R.; Margreiter, C.; et al. Outcomes following pancreatic resections—Results and challenges of an Austrian university hospital compared to nationwide data and international centres. Eur. Surg. 2019, 51, 81–89. [Google Scholar] [CrossRef]
- Sharon, C.E.; Thaler, A.S.; Straker, R.J., 3rd; Kelz, R.R.; Raper, S.E.; Vollmer, C.M.; DeMatteo, R.P.; Miura, J.T.; Karakousis, G.C. Fourteen years of pancreatic surgery for malignancy among ACS-NSQIP centers: Trends in major morbidity and mortality. Surgery 2022, 172, 708–714. [Google Scholar] [CrossRef]
- Chincarini, M.; Zamboni, G.A.; Pozzi Mucelli, R. Major pancreatic resections: Normal postoperative findings and complications. Insights Imaging 2018, 9, 173–187. [Google Scholar] [CrossRef]
- Watanabe, Y.; Nishihara, K.; Matsumoto, S.; Okayama, T.; Abe, Y.; Nakano, T. Effect of postoperative major complications on prognosis after pancreatectomy for pancreatic cancer: A retrospective review. Surg. Today 2017, 47, 555–567. [Google Scholar] [CrossRef]
- Henry, A.C.; van Dongen, J.C.; van Goor, I.; Smits, F.J.; Nagelhout, A.; Besselink, M.G.; Busch, O.R.; Bonsing, B.A.; Bosscha, K.; van Dam, R.M.; et al. Impact of complications after resection of pancreatic cancer on disease recurrence and survival, and mediation effect of adjuvant chemotherapy: Nationwide, observational cohort study. BJS Open 2023, 7, zrac174. [Google Scholar] [CrossRef]
- Smits, F.J.; van Santvoort, H.C.; Besselink, M.G.; Batenburg, M.C.T.; Slooff, R.A.E.; Boerma, D.; Busch, O.R.; Coene, P.; van Dam, R.M.; van Dijk, D.P.J.; et al. Management of Severe Pancreatic Fistula After Pancreatoduodenectomy. JAMA Surg. 2017, 152, 540–548. [Google Scholar] [CrossRef]
- Penumadu, P.; Barreto, S.G.; Goel, M.; Shrikhande, S.V. Pancreatoduodenectomy-preventing complications. Indian J. Surg. Oncol. 2015, 6, 6–15. [Google Scholar] [CrossRef]
- Okano, K.; Hirao, T.; Unno, M.; Fujii, T.; Yoshitomi, H.; Suzuki, S.; Satoi, S.; Takahashi, S.; Kainuma, O.; Suzuki, Y. Postoperative infectious complications after pancreatic resection. Br. J. Surg. 2015, 102, 1551–1560. [Google Scholar] [CrossRef]
- Kent, T.S.; Sachs, T.E.; Callery, M.P.; Vollmer, C.M., Jr. The burden of infection for elective pancreatic resections. Surgery 2013, 153, 86–94. [Google Scholar] [CrossRef]
- Kimura, W.; Miyata, H.; Gotoh, M.; Hirai, I.; Kenjo, A.; Kitagawa, Y.; Shimada, M.; Baba, H.; Tomita, N.; Nakagoe, T.; et al. A pancreaticoduodenectomy risk model derived from 8575 cases from a national single-race population (Japanese) using a web-based data entry system: The 30-day and in-hospital mortality rates for pancreaticoduodenectomy. Ann. Surg. 2014, 259, 773–780. [Google Scholar] [CrossRef]
- Fried, E.; Weissman, C.; Sprung, C. Postoperative sepsis. Curr. Opin. Crit. Care 2011, 17, 396–401. [Google Scholar] [CrossRef]
- Finks, J.F.; Osborne, N.H.; Birkmeyer, J.D. Trends in hospital volume and operative mortality for high-risk surgery. N. Engl. J. Med. 2011, 364, 2128–2137. [Google Scholar] [CrossRef]
- Anderson, R.N.; Smith, B.L. Deaths: Leading causes for 2002. Natl. Vital Stat. Rep. 2005, 53, 1–89. [Google Scholar]
- Vogel, T.R.; Dombrovskiy, V.Y.; Lowry, S.F.; Bouza, C.; López-Cuadrado, T.; Amate-Blanco, J.M.; Ramanathan, R.; Leavell, P.; Mays, C.; Duane, T.M.; et al. Trends in postoperative sepsis: Are we improving outcomes? Surg. Infect. 2009, 10, 71–78. [Google Scholar] [CrossRef]
- Elias, A.C.; Matsuo, T.; Grion, C.M.; Cardoso, L.T.; Verri, P.H. Incidence and risk factors for sepsis in surgical patients: A cohort study. J. Crit. Care 2012, 27, 159–166. [Google Scholar] [CrossRef]
- Mokart, D.; Leone, M.; Sannini, A.; Brun, J.P.; Tison, A.; Delpero, J.R.; Houvenaeghel, G.; Blache, J.L.; Martin, C. Predictive perioperative factors for developing severe sepsis after major surgery. Br. J. Anaesth. 2005, 95, 776–781. [Google Scholar] [CrossRef]
- Sammon, J.D.; Klett, D.E.; Sood, A.; Olugbade, K., Jr.; Schmid, M.; Kim, S.P.; Menon, M.; Trinh, Q.D. Sepsis after major cancer surgery. J. Surg. Res. 2015, 193, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Greenblatt, D.Y.; Kelly, K.J.; Rajamanickam, V.; Wan, Y.; Hanson, T.; Rettammel, R.; Winslow, E.R.; Cho, C.S.; Weber, S.M. Preoperative factors predict perioperative morbidity and mortality after pancreaticoduodenectomy. Ann. Surg. Oncol. 2011, 18, 2126–2135. [Google Scholar] [CrossRef] [PubMed]
- Mokart, D.; Giaoui, E.; Barbier, L.; Lambert, J.; Sannini, A.; Chow-Chine, L.; Brun, J.P.; Faucher, M.; Guiramand, J.; Ewald, J.; et al. Postoperative sepsis in cancer patients undergoing major elective digestive surgery is associated with increased long-term mortality. J. Crit. Care 2016, 31, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Claxton, A.J.; Thompson-Leduc, P.; Kirson, N.Y.; Rice, B.; Hey, J.; Iankova, I.; Krause, A.; Schonfeld, S.A.; DeBrase, C.R.; Bozzette, S.; et al. Efficacy and safety of procalcitonin guidance in patients with suspected or confirmed sepsis: A systematic review and meta-analysis: Author correction. Crit. Care Med. 2018, 46, 1560. [Google Scholar] [CrossRef]
- Giannakopoulos, K.; Hoffmann, U.; Ansari, U.; Bertsch, T.; Borggrefe, M.; Akin, I.; Behnes, M. The Use of Biomarkers in Sepsis: A Systematic Review. Curr. Pharm. Biotechnol. 2017, 18, 499–507. [Google Scholar] [CrossRef]
- Kondo, Y.; Umemura, Y.; Hayashida, K.; Hara, Y.; Aihara, M.; Yamakawa, K. Diagnostic value of procalcitonin and presepsin for sepsis in critically ill adult patients: A systematic review and meta-analysis. J. Intensive Care 2019, 7, 22. [Google Scholar] [CrossRef]
- Lee, S.; Song, J.; Park, D.W.; Seok, H.; Ahn, S.; Kim, J.; Park, J.; Cho, H.J.; Moon, S. Diagnostic and prognostic value of presepsin and procalcitonin in non-infectious organ failure, sepsis, and septic shock: A prospective observational study according to the Sepsis-3 definitions. BMC Infect. Dis. 2022, 22, 8. [Google Scholar] [CrossRef]
- Kim, H.; Hur, M.; Moon, H.W.; Yun, Y.M.; Di Somma, S.; Network, G. Multi-marker approach using procalcitonin, presepsin, galectin-3, and soluble suppression of tumorigenicity 2 for the prediction of mortality in sepsis. Ann. Intensive Care 2017, 7, 27. [Google Scholar] [CrossRef]
- Kim, H.; Kang, K.N.; Shin, Y.S.; Byun, Y.; Han, Y.; Kwon, W.; Kim, C.W.; Jang, J.Y. Biomarker Panel for the Diagnosis of Pancreatic Ductal Adenocarcinoma. Cancers 2020, 12, 1443. [Google Scholar] [CrossRef]
- Song, J.; Sokoll, L.J.; Chan, D.W.; Zhang, Z. Validation of Serum Biomarkers That Complement CA19-9 in Detecting Early Pancreatic Cancer Using Electrochemiluminescent-Based Multiplex Immunoassays. Biomedicines 2021, 9, 1897. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Yoon, W.; Lee, A.; Han, Y.; Byun, Y.; Kang, J.S.; Kim, H.; Kwon, W.; Suh, Y.A.; Choi, Y.; et al. Multi-biomarker panel prediction model for diagnosis of pancreatic cancer. J. Hepato-Biliary-Pancreat. Sci. 2023, 30, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Komorowski, M.; Green, A.; Tatham, K.C.; Seymour, C.; Antcliffe, D. Sepsis biomarkers and diagnostic tools with a focus on machine learning. EBioMedicine 2022, 86, 104394. [Google Scholar] [CrossRef]
- Deng, H.F.; Sun, M.W.; Wang, Y.; Zeng, J.; Yuan, T.; Li, T.; Li, D.H.; Chen, W.; Zhou, P.; Wang, Q.; et al. Evaluating machine learning models for sepsis prediction: A systematic review of methodologies. iScience 2022, 25, 103651. [Google Scholar] [CrossRef]
- Alanazi, A.; Aldakhil, L.; Aldhoayan, M.; Aldosari, B. Machine Learning for Early Prediction of Sepsis in Intensive Care Unit (ICU) Patients. Medicina 2023, 59, 1276. [Google Scholar] [CrossRef]
- Ocampo-Quintero, N.; Vidal-Cortes, P.; Del Rio Carbajo, L.; Fdez-Riverola, F.; Reboiro-Jato, M.; Glez-Pena, D. Enhancing sepsis management through machine learning techniques: A review. Med. Intensiv. 2022, 46, 140–156. [Google Scholar] [CrossRef] [PubMed]
- Sardesai, A.U.; Tanak, A.S.; Krishnan, S.; Striegel, D.A.; Schully, K.L.; Clark, D.V.; Muthukumar, S.; Prasad, S. An approach to rapidly assess sepsis through multi-biomarker host response using machine learning algorithm. Sci. Rep. 2021, 11, 16905. [Google Scholar] [CrossRef] [PubMed]
- Taneja, I.; Reddy, B.; Damhorst, G.; Dave Zhao, S.; Hassan, U.; Price, Z.; Jensen, T.; Ghonge, T.; Patel, M.; Wachspress, S.; et al. Combining Biomarkers with EMR Data to Identify Patients in Different Phases of Sepsis. Sci. Rep. 2017, 7, 10800. [Google Scholar] [CrossRef] [PubMed]
- Mao, Q.; Jay, M.; Hoffman, J.L.; Calvert, J.; Barton, C.; Shimabukuro, D.; Shieh, L.; Chettipally, U.; Fletcher, G.; Kerem, Y.; et al. Multicentre validation of a sepsis prediction algorithm using only vital sign data in the emergency department, general ward and ICU. BMJ Open 2018, 8, e017833. [Google Scholar] [CrossRef]
- Fleuren, L.M.; Klausch, T.L.T.; Zwager, C.L.; Schoonmade, L.J.; Guo, T.; Roggeveen, L.F.; Swart, E.L.; Girbes, A.R.J.; Thoral, P.; Ercole, A.; et al. Machine learning for the prediction of sepsis: A systematic review and meta-analysis of diagnostic test accuracy. Intensive Care Med. 2020, 46, 383–400. [Google Scholar] [CrossRef] [PubMed]
- Shashikumar, S.P.; Wardi, G.; Malhotra, A.; Nemati, S. Artificial intelligence sepsis prediction algorithm learns to say “I don’t know”. NPJ Digit. Med. 2021, 4, 134. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.; Henry, K.E.; Sridharan, A.; Soleimani, H.; Zhan, A.; Rawat, N.; Johnson, L.; Hager, D.N.; Cosgrove, S.E.; Markowski, A.; et al. Prospective, multi-site study of patient outcomes after implementation of the TREWS machine learning-based early warning system for sepsis. Nat. Med. 2022, 28, 1455–1460. [Google Scholar] [CrossRef]
- Ren, Y.; Loftus, T.J.; Datta, S.; Ruppert, M.M.; Guan, Z.; Miao, S.; Shickel, B.; Feng, Z.; Giordano, C.; Upchurch, G.R., Jr.; et al. Performance of a Machine Learning Algorithm Using Electronic Health Record Data to Predict Postoperative Complications and Report on a Mobile Platform. JAMA Netw. Open 2022, 5, e2211973. [Google Scholar] [CrossRef] [PubMed]
- Thottakkara, P.; Ozrazgat-Baslanti, T.; Hupf, B.B.; Rashidi, P.; Pardalos, P.; Momcilovic, P.; Bihorac, A. Application of Machine Learning Techniques to High-Dimensional Clinical Data to Forecast Postoperative Complications. PLoS ONE 2016, 11, e0155705. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Afzal, N.; Sohn, S.; Habermann, E.B.; Naessens, J.M.; Larson, D.W.; Liu, H. Postoperative bleeding risk prediction for patients undergoing colorectal surgery. Surgery 2018, 164, 1209–1216. [Google Scholar] [CrossRef]
- Zeng, S.; Li, L.; Hu, Y.; Luo, L.; Fang, Y. Machine learning approaches for the prediction of postoperative complication risk in liver resection patients. BMC Med. Inform. Decis. Mak. 2021, 21, 371. [Google Scholar] [CrossRef]
- van Roessel, S.; Strijker, M.; Steyerberg, E.W.; Groen, J.V.; Mieog, J.S.; Groot, V.P.; He, J.; De Pastena, M.; Marchegiani, G.; Bassi, C.; et al. International validation and update of the Amsterdam model for prediction of survival after pancreatoduodenectomy for pancreatic cancer. Eur. J. Surg. Oncol. 2020, 46, 796–803. [Google Scholar] [CrossRef]
- Latenstein, A.E.J.; van Roessel, S.; van der Geest, L.G.M.; Bonsing, B.A.; Dejong, C.H.C.; Groot Koerkamp, B.; de Hingh, I.; Homs, M.Y.V.; Klaase, J.M.; Lemmens, V.; et al. Conditional Survival After Resection for Pancreatic Cancer: A Population-Based Study and Prediction Model. Ann. Surg. Oncol. 2020, 27, 2516–2524. [Google Scholar] [CrossRef]
- Merath, K.; Hyer, J.M.; Mehta, R.; Farooq, A.; Bagante, F.; Sahara, K.; Tsilimigras, D.I.; Beal, E.; Paredes, A.Z.; Wu, L.; et al. Use of Machine Learning for Prediction of Patient Risk of Postoperative Complications After Liver, Pancreatic, and Colorectal Surgery. J. Gastrointest. Surg. 2020, 24, 1843–1851. [Google Scholar] [CrossRef]
- Cos, H.; Li, D.; Williams, G.; Chininis, J.; Dai, R.; Zhang, J.; Srivastava, R.; Raper, L.; Sanford, D.; Hawkins, W.; et al. Predicting Outcomes in Patients Undergoing Pancreatectomy Using Wearable Technology and Machine Learning: Prospective Cohort Study. J. Med. Internet Res. 2021, 23, e23595. [Google Scholar] [CrossRef] [PubMed]
- van Roessel, S.; Mackay, T.M.; van Dieren, S.; van der Schelling, G.P.; Nieuwenhuijs, V.B.; Bosscha, K.; van der Harst, E.; van Dam, R.M.; Liem, M.S.L.; Festen, S.; et al. Textbook Outcome: Nationwide Analysis of a Novel Quality Measure in Pancreatic Surgery. Ann. Surg. 2020, 271, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, T.; Uesaka, K.; Kanemoto, H.; Mizuno, T.; Sasaki, K.; Furukawa, H.; Matsunaga, K.; Maeda, A. Serum CA19-9 is a significant predictor among preoperative parameters for early recurrence after resection of pancreatic adenocarcinoma. J. Gastrointest. Surg. 2012, 16, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Shimoda, M.; Shimazaki, J.; Maruyama, T.; Oshiro, Y.; Nishida, K.; Sahara, Y.; Nagakawa, Y.; Tsuchida, A. Predictive Early Recurrence Factors of Preoperative Clinicophysiological Findings in Pancreatic Cancer. Eur. Surg. Res. 2018, 59, 329–338. [Google Scholar] [CrossRef]
- Yoon, S.J.; Park, B.; Kwon, J.; Lim, C.S.; Shin, Y.C.; Jung, W.; Shin, S.H.; Heo, J.S.; Han, I.W. Development of Nomograms for Predicting Prognosis of Pancreatic Cancer after Pancreatectomy: A Multicenter Study. Biomedicines 2022, 10, 1341. [Google Scholar] [CrossRef]
- Ono, S.; Adachi, T.; Ohtsuka, T.; Kimura, R.; Nishihara, K.; Watanabe, Y.; Nagano, H.; Tokumitsu, Y.; Nanashima, A.; Imamura, N.; et al. Predictive factors for early recurrence after pancreaticoduodenectomy in patients with resectable pancreatic head cancer: A multicenter retrospective study. Surgery 2022, 172, 1782–1790. [Google Scholar] [CrossRef]
- Groot, V.P.; Gemenetzis, G.; Blair, A.B.; Rivero-Soto, R.J.; Yu, J.; Javed, A.A.; Burkhart, R.A.; Rinkes, I.; Molenaar, I.Q.; Cameron, J.L.; et al. Defining and Predicting Early Recurrence in 957 Patients With Resected Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2019, 269, 1154–1162. [Google Scholar] [CrossRef]
- He, M.; Chen, X.; Wels, M.; Lades, F.; Li, Y.; Liu, Z.; Jin, Z.; Xue, H. Computed Tomography-based Radiomics Evaluation of Postoperative Local Recurrence of Pancreatic Ductal Adenocarcinoma. Acad. Radiol. 2023, 30, 680–688. [Google Scholar] [CrossRef]
- Li, X.; Wan, Y.; Lou, J.; Xu, L.; Shi, A.; Yang, L.; Fan, Y.; Yang, J.; Huang, J.; Wu, Y.; et al. Preoperative recurrence prediction in pancreatic ductal adenocarcinoma after radical resection using radiomics of diagnostic computed tomography. EClinicalMedicine 2022, 43, 101215. [Google Scholar] [CrossRef]
- Sturm, N.; Ettrich, T.J.; Perkhofer, L. The Impact of Biomarkers in Pancreatic Ductal Adenocarcinoma on Diagnosis, Surveillance and Therapy. Cancers 2022, 14, 217. [Google Scholar] [CrossRef]
- Al Abbas, A.I.; Zenati, M.; Reiser, C.J.; Hamad, A.; Jung, J.P.; Zureikat, A.H.; Zeh, H.J., 3rd; Hogg, M.E. Serum CA19-9 Response to Neoadjuvant Therapy Predicts Tumor Size Reduction and Survival in Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2020, 27, 2007–2014. [Google Scholar] [CrossRef]
- Li, J.; Li, Z.; Kan, H.; Sun, Z.; Xing, J.; Cheng, Y.; Bai, C. CA19-9 elevation as an indication to start salvage treatment in surveillance after pancreatic cancer resection. Pancreatol. 2019, 19, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Rieser, C.J.; Zenati, M.; Hamad, A.; Al Abbas, A.I.; Bahary, N.; Zureikat, A.H.; Zeh, H.J., 3rd; Hogg, M.E. CA19-9 on Postoperative Surveillance in Pancreatic Ductal Adenocarcinoma: Predicting Recurrence and Changing Prognosis over Time. Ann. Surg. Oncol. 2018, 25, 3483–3491. [Google Scholar] [CrossRef]
- Vasavada, B.; Patel, H. Postoperative serum procalcitonin versus C-reactive protein as a marker of postoperative infectious complications in pancreatic surgery: A meta-analysis. ANZ J. Surg. 2021, 91, E260–E270. [Google Scholar] [CrossRef] [PubMed]
- Iida, H.; Maehira, H.; Mori, H.; Tani, M. Serum procalcitonin as a predictor of infectious complications after pancreaticoduodenectomy: Review of the literature and our experience. Surg. Today 2020, 50, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Hata, T.; Mizuma, M.; Motoi, F.; Hayashi, H.; Ishida, M.; Ohtsuka, H.; Nakagawa, K.; Morikawa, T.; Kamei, T.; Unno, M. Serum procalcitonin as an early diagnostic marker of severe postoperative complications after elective pancreaticoduodenectomy. J. Hepato-Biliary-Pancreat. Sci. 2020, 27, 767–775. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Gender | Age (Year) | Tumor Volume (cc) | Maximum Dose of RT (Dmax, Gy) | Cause of Death or Complications in ICU |
|---|---|---|---|---|---|
| Group A | |||||
| 1 | F | 65 | 60.2 | 34.0 | Septic shock |
| 2 | F | 61 | 68.1 | 39.0 | Sepsis |
| 3 | F | 67 | 68.0 | 36.0 | Sepsis and septic shock |
| 4 | F | 55 | 76.0 | 35.0 | Sepsis with renal and liver impairment |
| 5 | M | 79 | 64.0 | 31.0 | Septic shock |
| 6 | M | 65 | 45.0 | 32.0 | Sepsis |
| 7 | F | 68 | 69.6 | 39.0 | Sepsis and septic shock |
| 8 | M | 63 | 70.0 | 39.0 | Sepsis |
| 9 | F | 64 | 57.0 | 37.0 | Septic shock |
| 10 | M | 57 | 60.2 | 38.0 | Sepsis * |
| Group B | |||||
| 1 | F | 50 | 66.0 | 34.0 | Recurrence |
| 2 | F | 40 | 62.5 | 32.0 | Recurrence |
| 3 | M | 57 | 68.1 | 40.0 | Recurrence |
| 4 | M | 53 | 67.5 | 38.0 | Recurrence |
| 5 | M | 53 | 43.2 | 38.0 | Recurrence |
| 6 | M | 41 | 57.2 | 34.0 | Recurrence |
| 7 | M | 40 | 45.0 | 38.0 | Recurrence |
| 8 | M | 53 | 50.0 | 36.0 | Recurrence |
| 9 | M | 51 | 57.1 | 40.0 | Recurrence |
| 10 | M | 62 | 56.0 | 40.0 | Recurrence |
| Group C | |||||
| 1 | F | 52 | 62.0 | 43.0 | Unknown |
| 2 | M | 51 | 40.0 | 38.0 | Unknown |
| 3 | F | 50 | 76.0 | 39.0 | Unknown |
| 4 | M | 65 | 76.0 | 38.0 | Unknown |
| 5 | M | 62 | 56.0 | 36.0 | Unknown |
| 6 | F | 52 | 62.0 | 38.0 | Unknown |
| 7 | F | 51 | 40.0 | 43.0 | Unknown |
| 8 | M | 50 | 76.0 | 36.0 | Unknown |
| 9 | M | 65 | 76.0 | 38.0 | Unknown |
| 10 | M | 62 | 56.0 | 39.0 | Unknown |
| Biochemical Test | Preoperative Findings | Postoperative Findings | Healthy Controls | ||
|---|---|---|---|---|---|
| Sepsis (Group A: 10) | Recurrence (Group B: 10) | Unknown Complications (Group C: 10) | |||
| TBIL (mg/dL) | 2.3 ± 0.5 ** | 0.87 ± 0.1 * | 0.84 ± 0.1 * | 0.86 ± 0.1 * | 0.72 ± 0.1 |
| DBIL (mg/dL) | 0.78 ± 0.08 ** | 0.16 ± 0.01 * | 0.15 ± 0.05 * | 0.16 ± 0.05 * | 0.13 ± 0.01 |
| ALT (U/L) | 106.0 ± 8.5 ** | 26.0 ± 1.2 * | 21.0 ± 0.9 * | 15.0 ± 0.9 * | 19.0 ± 1.0 |
| ALB (g/L) | 4.14 ± 0.3 ** | 3.5 ± 0.2 ** | 4.35 ± 0.3 * | 4.35 ± 0.3 * | 4.7 ± 0.5 |
| TLC (×103/mm3) | 5.99 ± 0.085 ns | 17.12 ± 0.15 ** | 4.2 ± 0.331 * | 4.0 ± 0.331 * | 5.8 ± 0.04 |
| IgG (g/L) | 8.01 ± 0.6 ns | 5.96 ± 0.44 ** | 8.76 ± 0.7 ns | 8.01 ± 0.7 ns | 8.57 ± 0.76 |
| IgA (×102 g/L) | 9.41 ± 0.8 ** | 7.8 ± 0.6 ** | 7.81 ± 0.7 ** | 7.71 ± 0.7 ** | 31.2 ± 2.5 |
| PCT (ng/mL) | 0.00 | 6.9 ± 0.8 ** | 0.072 ± 0.01 * | 0.070 ± 0.001 * | 0.01 |
| Patient No. | Preoperative CA19-9 (U/mL) | Postoperative CA19-9 (U/mL) | Preoperative CXCL-8 (pg/mL) | Postoperative CXCL-8 (pg/mL) |
|---|---|---|---|---|
| Group A | ||||
| 1 | 196.0 ± 29.0 ** | 23.5 ± 2.0 ** | 182.0 ± 13.0 ** | 336.0 ± 35.0 ** |
| 2 | 429.0 ± 39.0 ** | 37.0 ± 2.0 ** | 319.0 ± 40.0 ** | 912.0 ± 82.0 ** |
| 3 | 267.0 ± 18.0 ** | 12.0 ± 1.1 ** | 215.0 ±17.0 ** | 467.0 ± 48.0 ** |
| 4 | 53.0 ± 6.0 ** | 22.0 ± 1.0 ** | 42.1 ±37.0 ** | 189.0 ± 17.0 ** |
| 5 | 193.0 ± 17.0 ** | 55.0 ± 4.0 ** | 187.0 ± 15.0 ** | 602.0 ± 55.0 ** |
| 6 | 19.8 ± 1.8 ** | 2.5 ± 1.0 ** | 20.3 ± 1.0 ** | 214.0 ± 22.0 ** |
| 7 | 58.0 ± 5.0 ** | 1.2 ± 0.1 ** | 22.0 ± 1.0 ** | 168.0 ± 15.0 ** |
| 8 | 6.47 ± 0.3 ** | 1.3 ± 0.1 ** | 24.0 ± 1.0 ** | 210.0 ± 17.0 ** |
| 9 | 231.0 ± 15.0 ** | 1.2 ± 0.1 ** | 22.0 ± 1.0 ** | 211.5 ± 17.0 ** |
| 10 | 85.0 ± 8.0 ** | 12.7 ± 1.0 ** | 42.1 ± 6.0 ** | 26.5 ± 2.0 ** |
| Mean ± SD | 153.83 ± 13.9 ** | 24.3 ± 1.2 ** | 107.5 ± 11.0 ** | 333.6 ± 29.0 ** |
| Group B | ||||
| 1 | 421.0 ± 55.0 ** | 266.0 ± 18.0 ** | 396.0 ± 36.0 ** | 191.0 ± 18.0 ** |
| 2 | 891.0 ± 111.0 ** | 211.0 ± 15.0 ** | 759.0 ± 81.0 ** | 98.0 ± 6.0 ** |
| 3 | 613.0 ± 29.0 ** | 178.0 ± 16.0 ** | 606.0 ± 50.0 ** | 981.0 ± 96.0 ** |
| 4 | 1444.0 ± 112.0 * | 325.0 ± 26.0 ** | 1384.0 ± 112.0 ** | 298.0 ± 22.0 ** |
| 5 | 491.0 ± 40.0 ** | 98.0 ± 8.0 ** | 405.0 ± 36.0 ** | 281.0 ± 21.0 ** |
| 6 | 412.0 ± 36.0 ** | 257.0 ± 16.0 ** | 365.0 ± 11.0 ** | 79.0 ± 8.0 ** |
| 7 | 1012.0 ± 98.0 ** | 277.0 ± 17.0 ** | 891.0 ± 66.0 ** | 704.0 ± 60.0 ** |
| 8 | 112.0 ± 10.0 ** | 2.7 ± 0.1 ** | 26.3 ± 2.0 ** | 96.2 ± 6.0 ** |
| 9 | 512.0 ± 53.0 ** | 203.0 ± 19.0 ** | 349.0 ± 28.0 ** | 462.0 ± 12.0 ** |
| 10 | 1577.0 ± 150.0 * | 421.0 ± 36.0 ** | 1448.0 ± 132.0 * | 1081.0 ± 95.0 ** |
| Mean ± SD | 748.5 ± 59.4 ** | 233.7 ± 17.22 ** | 659.5 ± 55.4 ** | 427.1 ± 34.4 ** |
| Group C | ||||
| 1 | 80.0 ± 17.0 ** | 17.0 ± 1.5 ** | 65.0 ± 6.0 * | 85.0 ± 7.0 * |
| 2 | 84.0 ± 6.5 ** | 3.5 ± 0.5 ** | 56.0 ± 4.0 * | 32.5 ± 3.0 * |
| 3 | 23.6 ± 3.0 ** | 5.7 ± 0.2 ** | 31.0 ± 1.0 * | 66.0 ± 2.9 * |
| 4 | 3.34 ± 0.5 ** | 1.2 ± 0.6 ** | 25.3 ± 1.0 * | 35.8 ± 1.0 * |
| 5 | 65.7 ± 5.0 ** | 1.3 ± 0.1 ** | 29.0 ± 2.0 * | 78.0 ± 7.0 * |
| 6 | 75.0 ± 17.0 ** | 19.0 ± 1.5 ** | 69.0 ± 6.0 * | 85.0 ± 7.0 * |
| 7 | 89.0 ± 6.5 ** | 3.5 ± 0.5 ** | 59.0 ± 4.0 * | 32.5 ±3.0 * |
| 8 | 23.6 ± 3.0 ** | 5.7 ± 0.2 ** | 19.5 ± 1.0 * | 86.0 ± 2.9 * |
| 9 | 3.34 ± 0.5 ** | 1.2 ± 0.6 ** | 21.3 ± 1.0 * | 42.3 ± 1.0 * |
| 10 | 75.7 ± 5.0 ** | 1.3 ± 0.1 ** | 25.0 ± 2.0 * | 72.0 ± 7.0 * |
| Mean ± SD | 52.2 ± 5.9 ** | 5.39 ± 0.58 ** | 39.95 ± 2.8 * | 61.6 ± 4.18 * |
| Healthy controls | ||||
| 1 | 11.0 ± 1.0 | - | 23.0 ± 2.0 | - |
| 2 | 18.0 ± 1.0 | - | 21.8 ± 2.0 | - |
| 3 | 12.3 ± 1.0 | - | 22.0 ± 2.0 | - |
| 4 | 21.2 ± 1.2 | - | 21.5 ± 1.5 | - |
| Mean ± SD | 15.6 ± 2.0 | - | 22.07 ± 1.9 | - |
| Sample Parameters | t-Value | p-Value | Cohen-d | |
|---|---|---|---|---|
| CA19-9_post | G2 vs. G3 | 5.91106 | 0.00023 | 2.64 |
| G1 vs. G2 | −5.448325 | 0.00041 | 2.48 | |
| G1 vs. G3 | 1.686535 | 0.125969 | 0.804603 | |
| CXCL-8_post | G2 vs. G3 | 3.076225 | 0.01322 | 1.387486 |
| G1 vs. G2 | −0.564692 | 0.58608 | 0.291199 | |
| G1 vs. G3 | 3.236429 | 0.010217 | 1.470414 | |
| PCT_post | G2 vs. G3 | 0.631454 | 0.543447 | 0.059925 |
| G1 vs. G2 | 10.414405 | 0.00003 | 4.701717 | |
| G1 vs. G3 | 10.433683 | 0.000003 | 4.702802 | |
| Model | Accuracy | Precision | Recall | F-Score | AUC-ROC Score |
|---|---|---|---|---|---|
| GNB | 100 | 100 | 100 | 100 | 100 |
| MLR | 100 | 100 | 100 | 100 | 100 |
| RC | 100 | 100 | 100 | 100 | 100 |
| GPC | 100 | 100 | 100 | 100 | 100 |
| KNN | 100 | 100 | 100 | 100 | 100 |
| DT | 100 | 100 | 100 | 100 | 100 |
| Model | Accuracy | Precision | Recall | F-Score | AUC-ROC Score |
|---|---|---|---|---|---|
| GNB | 66.67 | 66.67 | 66.67 | 66.67 | 50 |
| MLR | 66.67 | 66.67 | 66.67 | 66.67 | 50 |
| RC | 66.67 | 66.67 | 66.67 | 66.67 | 50 |
| GPC | 83.33 | 83.33 | 83.33 | 83.33 | 75 |
| KNN | 83.33 | 83.33 | 83.33 | 83.33 | 75 |
| DT | 83.33 | 83.33 | 83.33 | 83.33 | 75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Khudir, R.; Hafsa, N.; Badr, B.E. Identifying Effective Biomarkers for Accurate Pancreatic Cancer Prognosis Using Statistical Machine Learning. Diagnostics 2023, 13, 3091. https://doi.org/10.3390/diagnostics13193091
Abu-Khudir R, Hafsa N, Badr BE. Identifying Effective Biomarkers for Accurate Pancreatic Cancer Prognosis Using Statistical Machine Learning. Diagnostics. 2023; 13(19):3091. https://doi.org/10.3390/diagnostics13193091
Chicago/Turabian StyleAbu-Khudir, Rasha, Noor Hafsa, and Badr E. Badr. 2023. "Identifying Effective Biomarkers for Accurate Pancreatic Cancer Prognosis Using Statistical Machine Learning" Diagnostics 13, no. 19: 3091. https://doi.org/10.3390/diagnostics13193091
APA StyleAbu-Khudir, R., Hafsa, N., & Badr, B. E. (2023). Identifying Effective Biomarkers for Accurate Pancreatic Cancer Prognosis Using Statistical Machine Learning. Diagnostics, 13(19), 3091. https://doi.org/10.3390/diagnostics13193091