
A Brain Morphometry Study with Across-Site Harmonization Using a ComBat-Generalized Additive Model in Children and Adolescents

 ,
,  , , , ,
, , , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and MRI Acquisition
2.2. Structural MRI Processing
2.3. ComBat-GAM Harmonization and Attempting the Trained ComBat-GAM Model
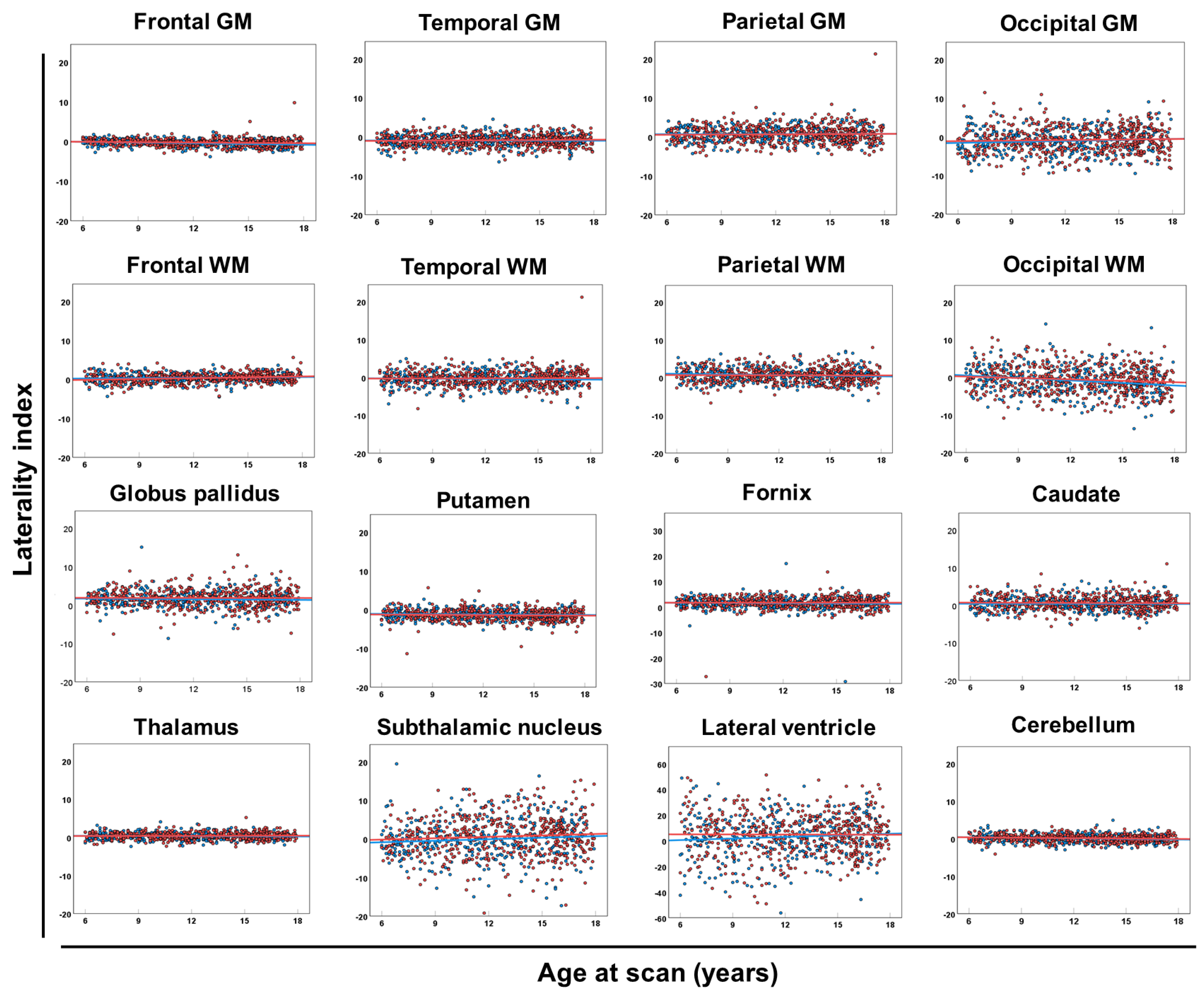
2.4. Laterality Index
2.5. Statistical Analyses
3. Results
3.1. Participants’ Background
3.2. Global and Regional Brain Volumes and Lateralities
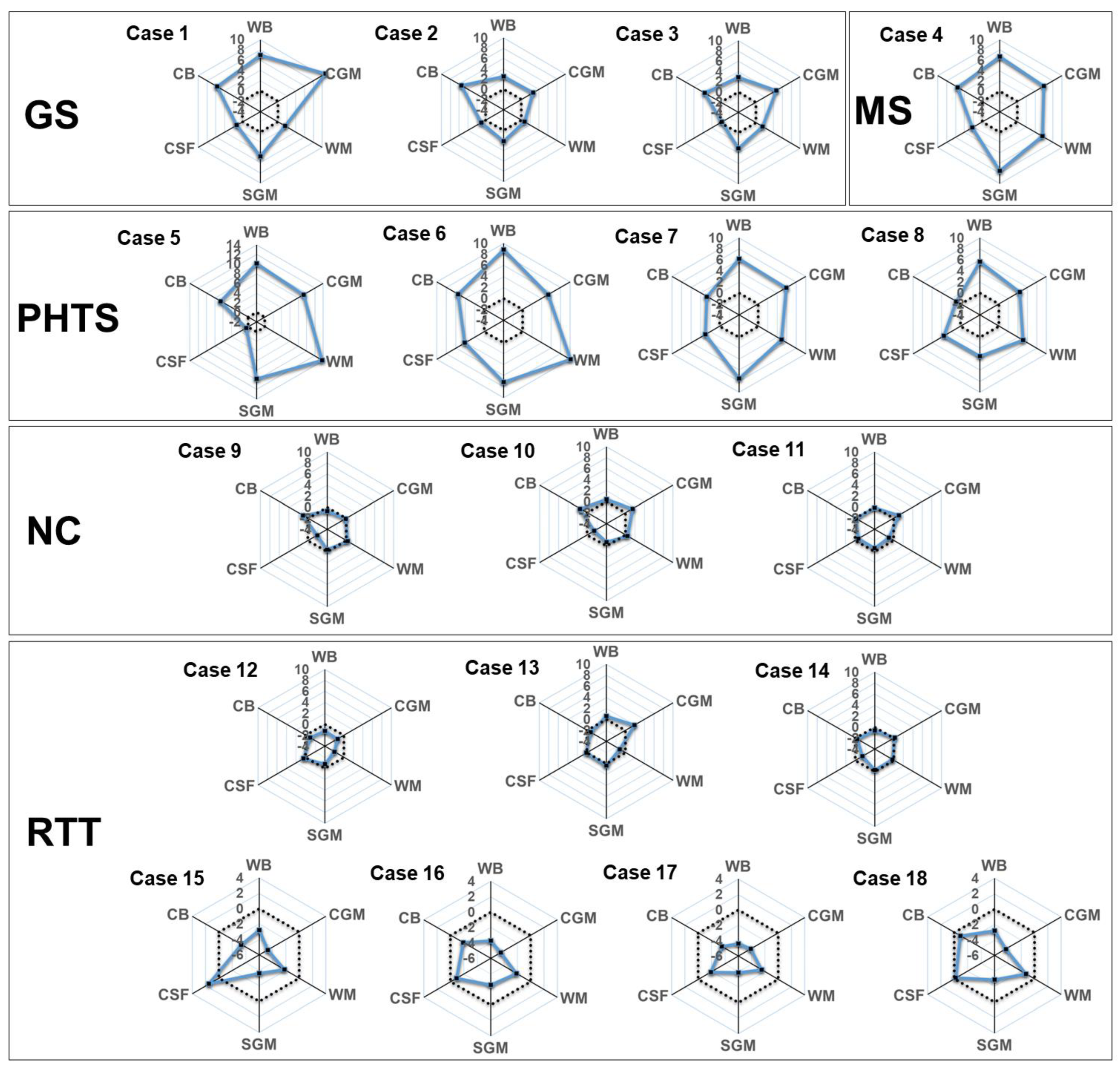
3.3. Applying the Trained ComBat-GAM Model to Additional Cases
4. Discussion
Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Qiu, A.; Zhang, H.; Kennedy, B.K.; Lee, A. Spatio-temporal correlates of gene expression and cortical morphology across lifespan and aging. Neuroimage 2021, 224, 117426. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.J.; Kawasawa, Y.I.; Cheng, F.; Zhu, Y.; Xu, X.; Li, M.; Sousa, A.M.; Pletikos, M.; Meyer, K.A.; Sedmak, G.; et al. Spatio-temporal transcriptome of the human brain. Nature 2011, 478, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wang, M.; Mi, D.; Lu, T.; Wang, B.; Dong, H.; Zhong, S.; Chen, Y.; Sun, L.; Zhou, X.; et al. Mouse and human share conserved transcriptional programs for interneuron development. Science 2021, 374, eabj6641. [Google Scholar] [CrossRef] [PubMed]
- Ball, G.; Seidlitz, J.; O’Muircheartaigh, J.; Dimitrova, R.; Fenchel, D.; Makropoulos, A.; Christiaens, D.; Schuh, A.; Passerat-Palmbach, J.; Hutter, J.; et al. Cortical morphology at birth reflects spatiotemporal patterns of gene expression in the fetal human brain. PLoS Biol. 2020, 18, e3000976. [Google Scholar] [CrossRef] [PubMed]
- Frangou, S.; Chitins, X.; Williams, S.C. Mapping IQ and gray matter density in healthy young people. Neuroimage 2004, 23, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Narr, K.L.; Woods, R.P.; Thompson, P.M.; Szeszko, P.; Robinson, D.; Dimtcheva, T.; Gurbani, M.; Toga, A.W.; Bilder, R.M. Relationships between IQ and regional cortical gray matter thickness in healthy adults. Cereb. Cortex 2007, 17, 2163–2171. [Google Scholar] [CrossRef]
- Levman, J.; Takahashi, E. Multivariate analyses applied to fetal, neonatal and pediatric MRI of neurodevelopmental disorders. Neuroimage Clin. 2015, 9, 532–544. [Google Scholar] [CrossRef]
- Arbabshirani, M.R.; Plis, S.; Sui, J.; Calhoun, V.D. Single subject prediction of brain disorders in neuroimaging: Promises and pitfalls. Neuroimage 2017, 145 Pt B, 137–165. [Google Scholar] [CrossRef]
- Levman, J.; MacDonald, P.; Lim, A.R.; Forgeron, C.; Takahashi, E. A pediatric structural MRI analysis of healthy brain development from newborns to young adults. Hum. Brain Mapp. 2017, 38, 5931–5942. [Google Scholar] [CrossRef]
- Courchesne, E.; Chisum, H.J.; Townsend, J.; Cowles, A.; Covington, J.; Egaas, B.; Harwood, M.; Hinds, S.; Press, G.A. Normal brain development and aging: Quantitative analysis at in vivo MR imaging in healthy volunteers. Radiology 2000, 216, 672–682. [Google Scholar] [CrossRef]
- Matsuzawa, J.; Matsui, M.; Konishi, T.; Noguchi, K.; Gur, R.C.; Bilker, W.; Miyawaki, T. Age-related volumetric changes of brain gray and white matter in healthy infants and children. Cereb. Cortex 2011, 11, 335–342. [Google Scholar] [CrossRef]
- Gogtay, N.; Giedd, J.N.; Lusk, L.; Hayashi, K.M.; Greenstein, D.; Vaituzis, A.C.; Nugent, T.F.; Herman, D.H., 3rd; Clasen, L.S.; Toga, A.W.; et al. Dynamic mapping of human cortical development during childhood through early adulthood. Proc. Natl. Acad. Sci. USA 2004, 101, 8174–8179. [Google Scholar] [CrossRef] [PubMed]
- Reiss, A.L.; Abrams, M.T.; Singer, H.S.; Ross, J.L.; Denckla, M.B. Brain development, gender and IQ in children. A volumetric imaging study. Brain 1996, 119 Pt 5, 1763–1774. [Google Scholar] [CrossRef]
- Bethlehem, R.A.I.; Seidlitz, J.; White, S.R.; Vogel, J.W.; Anderson, K.M.; Adamson, C.; Adler, S.; Alexopoulos, G.S.; Anagnostou, E.; Areces-Gonzalez, A.; et al. Brain charts for the human lifespan. Nature 2022, 604, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Koshiyama, D.; Fukunaga, M.; Okada, N.; Morita, K.; Nemoto, K.; Usui, K.; Yamamori, H.; Yasuda, Y.; Fujimoto, M.; Kudo, N.; et al. White matter microstructural alterations across four major psychiatric disorders: Mega-analysis study in 2937 individuals. Mol. Psychiatry 2020, 25, 883–895. [Google Scholar] [CrossRef]
- Nemoto, K.; Shimokawa, T.; Fukunaga, M.; Yamashita, F.; Tamura, M.; Yamamori, H.; Yasuda, Y.; Azechi, H.; Kudo, N.; Watanabe, Y.; et al. Differentiation of schizophrenia using structural MRI with consideration of scanner differences: A real-world multisite study. Psychiatry Clin. Neurosci. 2020, 74, 56–63. [Google Scholar] [CrossRef]
- Nazarova, A.; Schmidt, M.; Cookey, J.; Uher, R. Neural markers of familial risk for depression—A systematic review. Dev. Cogn. Neurosci. 2022, 58, 101161. [Google Scholar] [CrossRef] [PubMed]
- Shiohama, T.; Ortug, A.; Warren, J.L.A.; Valli, B.; Levman, J.; Faja, S.K.; Tsujimura, K.; Maunakea, A.K.; Takahashi, E. Small nucleus accumbens and large cerebral ventricles in infants and toddlers prior to receiving diagnoses of autism spectrum disorder. Cereb. Cortex 2022, 32, 1200–1211. [Google Scholar] [CrossRef]
- Hoogman, M.; van Rooij, D.; Klein, M.; Boedhoe, P.; Ilioska, I.; Li, T.; Patel, Y.; Postema, M.C.; Zhang-James, Y.; Anagnostou, E.; et al. Consortium neuroscience of attention deficit/hyperactivity disorder and autism spectrum disorder: The ENIGMA adventure. Hum. Brain Mapp. 2022, 43, 37–55. [Google Scholar] [CrossRef] [PubMed]
- Levman, J.; Forgeron, C.; Shiohama, T.; MacDonald, P.; Stewart, N.; Lim, A.; Berrigan, L.; Takahashi, E. Cortical thickness abnormalities in attention deficit hyperactivity disorder revealed by structural magnetic resonance imaging: Newborns to young adults. Int. J. Dev. Neurosci. 2022, 82, 584–595. [Google Scholar] [CrossRef]
- Shiohama, T.; Levman, J.; Baumer, N.; Takahashi, E. Structural magnetic resonance imaging-based brain morphology study in infants and toddlers with Down syndrome: The Effect of Comorbidities. Pediatr. Neurol. 2019, 100, 67–73. [Google Scholar] [CrossRef]
- McCann, B.; Levman, J.; Baumer, N.; Lam, M.Y.; Shiohama, T.; Cogger, L.; MacDonald, A.; Ijner, P.; Takahashi, E. Structural magnetic resonance imaging demonstrates volumetric brain abnormalities in Down syndrome: Newborns to young adults. Neuroimage Clin. 2021, 32, 102815. [Google Scholar] [CrossRef] [PubMed]
- Shiohama, T.; Levman, J.; Takahashi, E. Surface- and voxel-based brain morphologic study in Rett and Rett-like syndrome with MECP2 mutation. Int. J. Dev. Neurosci. 2019, 73, 83–88. [Google Scholar] [CrossRef]
- Takeguchi, R.; Kuroda, M.; Tanaka, R.; Suzuki, N.; Akaba, Y.; Tsujimura, K.; Itoh, M.; Takahashi, S. Structural and functional changes in the brains of patients with Rett syndrome: A multimodal MRI study. J. Neurol. Sci. 2022, 441, 120381. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Li, Q.B.; Yuan, Z.H.; Jiang, X.F.; Zhang, G.Q.; Cheng, N.; Dang, N. Multimodal neuroimaging in Rett syndrome with MECP2 mutation. Front. Neurol. 2022, 13, 838206. [Google Scholar] [CrossRef] [PubMed]
- Focke, N.K.; Helms, G.; Kaspar, S.; Diederich, C.; Tóth, V.; Dechent, P.; Mohr, A.; Paulus, W. Multi-site voxel-based morphometry--not quite there yet. Neuroimage 2011, 56, 1164–1170. [Google Scholar] [CrossRef]
- Iscan, Z.; Jin, T.B.; Kendrick, A.; Szeglin, B.; Lu, H.; Trivedi, M.; Fava, M.; McGrath, P.J.; Weissman, M.; Kurian, B.T.; et al. Test-retest reliability of freesurfer measurements within and between sites: Effects of visual approval process. Hum. Brain Mapp. 2015, 36, 3472–3485. [Google Scholar] [CrossRef] [PubMed]
- Vogelbacher, C.; Möbius, T.W.D.; Sommer, J.; Schuster, V.; Dannlowski, U.; Kircher, T.; Dempfle, A.; Jansen, A.; Bopp, M.H.A. The Marburg-Münster Affective Disorders Cohort Study (MACS): A quality assurance protocol for MR neuroimaging data. Neuroimage 2018, 172, 450–460. [Google Scholar] [CrossRef]
- Fortin, J.P.; Cullen, N.; Sheline, Y.I.; Taylor, W.D.; Aselcioglu, I.; Cook, P.A.; Adams, P.; Cooper, C.; Fava, M.; McGrath, P.J.; et al. Harmonization of cortical thickness measurements across scanners and sites. Neuroimage 2018, 167, 104–120. [Google Scholar] [CrossRef]
- Pomponio, R.; Erus, G.; Habes, M.; Doshi, J.; Srinivasan, D.; Mamourian, E.; Bashyam, V.; Nasrallah, I.M.; Satterthwaite, T.D.; Fan, Y.; et al. Harmonization of large MRI datasets for the analysis of brain imaging patterns throughout the lifespan. Neuroimage 2020, 208, 116450. [Google Scholar] [CrossRef]
- Sun, D.; Rakesh, G.; Haswell, C.C.; Logue, M.; Baird, C.L.; O’Leary, E.N.; Cotton, A.S.; Xie, H.; Tamburrino, M.; Chen, T.; et al. A comparison of methods to harmonize cortical thickness measurements across scanners and sites. Neuroimage 2022, 261, 119509. [Google Scholar] [CrossRef]
- Li, X.; Morgan, P.S.; Ashburner, J.; Smith, J.; Rorden, C. The first step for neuroimaging data analysis: DICOM to NIfTI conversion. J. Neurosci. Methods 2016, 264, 47–56. [Google Scholar] [CrossRef]
- Zijdenbos, A.P.; Forghani, R.; Evans, A.C. Automatic “pipeline” analysis of 3-D MRI data for clinical trials: Application to multiple sclerosis. IEEE Trans. Med. Imaging 2002, 21, 1280–1291. [Google Scholar] [CrossRef] [PubMed]
- Sherif, T.; Rioux, P.; Rousseau, M.E.; Kassis, N.; Beck, N.; Adalat, R.; Das, S.; Glatard, T.; Evans, A.C. CBRAIN: A web-based, distributed computing platform for collaborative neuroimaging research. Front. Neuroinform. 2014, 8, 54. [Google Scholar] [CrossRef] [PubMed]
- Sled, J.G.; Zijdenbos, A.P.; Evans, A.C. A nonparametric method for automatic correction of intensity nonuniformity in MRI data. IEEE Trans. Med. Imaging 1998, 17, 87–97. [Google Scholar] [CrossRef]
- Fonov, V.S.; Evans, A.C.; McKinstry, R.C.; Almli, C.R.; Collins, D.L.L. Unbiased non-linear average age-appropriate brain templates from birth to adulthood. Neuroimage 2009, 47, S102. Available online: http://www.sciencedirect.com/science/article/pii/S1053811909708845 (accessed on 1 January 2023). [CrossRef]
- Smith, S.M. Fast robust automated brain extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Tohka, J.; Zijdenbos, A.; Evans, A. Fast and robust parameter estimation for statistical partial volume models in brain MRI. Neuroimage 2004, 23, 84–97. [Google Scholar] [CrossRef]
- Collins, D.L.; Zijdenbos, A.P.; Baaré, W.F.C.; Evans, A.C. ANIMAL + INSECT: Improved Cortical Structure Segmentation. In Information Processing in Medical Imaging. Lecture Notes in Computer Science; Kuba, A., Šáamal, M., Todd-Pokropek, A., Eds.; Springer: Heidelberg/Berlin, Germany, 1999; pp. 210–223. [Google Scholar]
- Springer, J.A.; Binder, J.R.; Hammeke, T.A.; Swanson, S.J.; Frost, J.A.; Bellgowan, P.S.; Brewer, C.C.; Perry, H.M.; Morris, G.L.; Mueller, W.M. Language dominance in neurologically normal and epilepsy subjects: A functional MRI study. Brain 1999, 122 Pt 11, 2033–2046. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8, 118–127. [Google Scholar] [CrossRef]
- Fennema-Notestine, C.; Gamst, A.C.; Quinn, B.T.; Pacheco, J.; Jernigan, T.L.; Thal, L.; Buckner, R.; Killiany, R.; Blacker, D.; Dale, A.M.; et al. Feasibility of multi-site clinical structural neuroimaging studies of aging using legacy data. Neuroinformatics 2007, 5, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Liu, J.; Calhoun, V.D.; Arias-Vasquez, A.; Zwiers, M.P.; Gupta, C.N.; Franke, B.; Turner, J.A. Exploration of scanning effects in multi-site structural MRI studies. J. Neurosci. Methods 2014, 230, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Venkatraman, V.K.; Gonzalez, C.E.; Landman, B.; Goh, J.; Reiter, D.A.; An, Y.; Resnick, S.M. Region of interest correction factors improve reliability of diffusion imaging measures within and across scanners and field strengths. Neuroimage 2015, 119, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Radua, J.; Vieta, E.; Shinohara, R.; Kochunov, P.; Quidé, Y.; Green, M.J.; Weickert, C.S.; Weickert, T.; Bruggemann, J.; Kircher, T.; et al. Increased power by harmonizing structural MRI site differences with the ComBat batch adjustment method in ENIGMA. Neuroimage 2020, 218, 116956. [Google Scholar] [CrossRef]
- Gilmore, J.H.; Knickmeyer, R.C.; Gao, W. Imaging structural and functional brain development in early childhood. Nature reviews. Neuroscience 2018, 19, 123–137. [Google Scholar] [CrossRef]
- Goldenberg, G. Apraxia in left-handers. Brain 2013, 136 Pt 8, 2592–2601. [Google Scholar] [CrossRef]
- Kong, X.Z.; Mathias, S.R.; Guadalupe, T.; ENIGMA Laterality Working Group; Glahn, D.C.; Franke, B.; Crivello, F.; Tzourio-Mazoyer, N.; Fisher, S.E.; Thompson, P.M.; et al. Mapping cortical brain asymmetry in 17,141 healthy individuals worldwide via the ENIGMA Consortium. Proc. Natl. Acad. Sci. USA 2018, 115, E5154–E5163. [Google Scholar] [CrossRef]
- Guadalupe, T.; Mathias, S.R.; vanErp, T.G.M.; Whelan, C.D.; Zwiers, M.P.; Abe, Y.; Abramovic, L.; Agartz, I.; Andreassen, O.A.; Arias-Vásquez, A.; et al. Human subcortical brain asymmetries in 15,847 people worldwide reveal effects of age and sex. Brain Imaging Behav. 2017, 11, 1497–1514. [Google Scholar] [CrossRef]
- Shiohama, T.; McDavid, J.; Levman, J.; Takahashi, E. Quantitative brain morphological analysis in CHARGE syndrome. Neuroimage Clin. 2019, 23, 101866. [Google Scholar] [CrossRef]
- Conway, R.L.; Pressman, B.D.; Dobyns, W.B.; Danielpour, M.; Lee, J.; Sanchez-Lara, P.A.; Butler, M.G.; Zackai, E.; Campbell, L.; Saitta, S.C.; et al. Neuroimaging findings in macrocephaly-capillary malformation: A longitudinal study of 17 patients. Am. J. Med. Genet. A 2007, 143A, 2981–3008. [Google Scholar] [CrossRef]
- Cabrera, M.T.; Winn, B.J.; Porco, T.; Strominger, Z.; Barkovich, A.J.; Hoyt, C.S.; Wakahiro, M.; Sherr, E.H. Laterality of brain and ocular lesions in Aicardi syndrome. Pediatr. Neurol. 2011, 45, 149–154. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Riikonen, R.; Salonen, I.; Partanen, K.; Verho, S. Brain perfusion SPECT and MRI in foetal alcohol syndrome. Dev. Med. Child Neurol. 1999, 41, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Kelley, T.M.; Hatfield, L.A.; Lin, D.D.; Comi, A.M. Quantitative analysis of cerebral cortical atrophy and correlation with clinical severity in unilateral Sturge-Weber syndrome. J. Child. Neurol. 2005, 20, 867–870. [Google Scholar] [CrossRef] [PubMed]
- Schaer, M.; Cuadra, M.B.; Schmansky, N.; Fischl, B.; Thiran, J.P.; Eliez, S. How to measure cortical folding from MR images: A step-by-step tutorial to compute local gyrification index. J. Vis. Exp. 2012, 59, e3417. [Google Scholar] [CrossRef]
- Pienaar, R.; Fischl, B.; Caviness, V.; Makris, N.; Grant, P.E. A methodology for analyzing curvature in the developing brain from preterm to adult. Int. J. Imaging Syst. Technol. 2008, 18, 42–68. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scan-Site | BCH | CHBC | CUH | NGO | TYMC |
|---|---|---|---|---|---|
| Subject | Neurotypical controls | Healthy volunteers | Neurotypical controls | Healthy volunteers | Neurotypical controls |
| Sex (n) | Male 274 Female 438 | Male 20 Female 16 | Male 14 Female 16 | Male 19 Female 15 | Male 12 Female 22 |
| Age at scan (mean (SD), years) | 12.4 (3.4) | 14.2 (2.1) | 10.8 (2.8) | 10.9 (2.9) | 12.0 (2.6) |
| Vender | Siemens Healthcare | GE Healthcare | GE Healthcare | Siemens Healthcare | Philips Healthcare |
| MRI scanner | Skyra 3.0T | Discovery MR750 3.0T | Signa 1.5T EX-HDX | Prisma fit 3.0T | Ingenia CX 3.0T |
| Sequence | 3D-T1-MPRAGE | 3D-IR-T1-SPGR | 3D-IR-T1-SPGR | 3D-T1-MPRAGE | 3D-IR-T1-TFE |
| Repetition time (ms) | 1130–2530 | 8.1 | 7–22 | 1570 | 8.8 |
| Echo time (ms) | 1.69–2.52 | 3.2 | 2–5 | 2.2 | 4.9 |
| Matrix | 192–256 × 192–256 | 256 × 256 | 256 × 256 | 256 × 256 | 288 × 288 |
| FOV | 192–220 | 256 | 256 | 256 | 240 |
| ANIMAL Label | Description | ANIMAL Label | Description |
|---|---|---|---|
| 2 | Rt Parietal GM | 53 | Rt Caudate |
| 3 | Lt Lateral ventricle | 57 | Lt Parietal WM |
| 4 | Rt Occipital GM | 59 | Rt Temporal WM |
| 6 | Lt Parietal GM | 67 | Lt Cerebellum |
| 8 | Lt Occipital GM | 73 | Lt Occipital WM |
| 9 | Rt Lateral ventricle | 76 | Rt Cerebellum |
| 11 | Rt Globus pallidus | 83 | Lt Temporal WM |
| 12 | Lt Globus pallidus | 102 | Lt Thalamus |
| 14 | Lt Putamen | 105 | Rt Parietal WM |
| 16 | Rt Putamen | 203 | Rt Thalamus |
| 17 | Rt Frontal WM | 210 | Lt Frontal GM |
| 20 | Brainstem | 211 | Rt Frontal GM |
| 23 | Rt Subthalamic nucleus | 218 | Lt Temporal GM |
| 29 | Lt Fornix | 219 | Rt Temporal GM |
| 30 | Lt Frontal WM | 232 | Third ventricle |
| 33 | Lt Subthalamic nucleus | 233 | Fourth ventricle |
| 39 | Lt Caudate | 254 | Rt Fornix |
| 45 | Rt Occipital WM | 255 | Extracerebral CSF |
| Global measurements | Children (ANIMAL label numbers) | ||
| Whole brain | 2, 3, 4, 6, 8, 9, 11, 12, 14, 16, 17, 20, 23, 29, 30, 33, 39, 45, 53, 57, 59, 67, 73, 76, 83, 102, 105, 203, 210, 211, 218, 219, 232, 233, 254, 255 | ||
| Cortical gray matter (CGM) | 2, 4, 6, 8, 210, 211, 218, 219 | ||
| White matter (WM) | 17, 30, 45, 57, 59, 73, 83, 105 | ||
| Subcortical gray matter and fornix (SGM) | 11, 12, 14, 16, 23, 29, 33, 39, 53, 102, 203, 254 | ||
| Extra-axial CSF (CSF) | 3, 9, 232, 233, 255 | ||
| Cerebellum and brainstem (CB) | 20, 67, 76 | ||
| 6 YO ≤ Age < 9 YO | ||||||||
|---|---|---|---|---|---|---|---|---|
| Male (n = 89) | Female (n = 86) | Total (n = 175) | ||||||
| Description | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | p-Value (Male vs. Female) | Absolute Cohen’s d (Male vs. Female) |
| Whole brain * | 1,819,754 | 142,320 | 1,682,695 | 143,133 | 1,752,399 | 158,031 | 1.8 × 10−9 | 0.96 |
| Cortical GM * | 801,934 | 63,252 | 745,662 | 71,998 | 774,280 | 73,155 | 1.5 × 10−7 | 0.83 |
| WM * | 436,705 | 52,331 | 390,500 | 42,780 | 413,998 | 53,063 | 1.4 × 10−9 | 0.97 |
| SGM * | 37,714 | 2708 | 35,171 | 2758 | 36,464 | 3008 | 5.2 × 10−9 | 0.93 |
| Extra-axial CSF | 363,811 | 62,982 | 347,218 | 62,073 | 355,657 | 62,910 | 0.081 | 0.27 |
| CB * | 179,590 | 14,080 | 164,145 | 13,832 | 172,000 | 15,928 | 9.0 × 10−12 | 1.11 |
| 9 YO ≤ Age < 12 YO | ||||||||
| Male (n = 85) | Female (n = 127) | Total (n = 212) | ||||||
| Description | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | p-value (male vs. female) | Absolute Cohen’s d (male vs. female) |
| Whole brain * | 1,870,988 | 133,244 | 1,729,428 | 140,313 | 1,786,186 | 153,820 | 4.0 × 10−12 | 1.03 |
| Cortical GM * | 787,813 | 63,495 | 733,343 | 70,839 | 755,183 | 72,922 | 2.2 × 10−8 | 0.8 |
| WM * | 473,186 | 44,321 | 424,176 | 47,318 | 443,826 | 51,949 | 8.5 × 10−13 | 1.06 |
| SGM * | 38,328 | 2530 | 36,241 | 3024 | 37,078 | 3010 | 1.6 × 10−7 | 0.74 |
| Extra-axial CSF | 388,022 | 73,526 | 365,506 | 69,591 | 374,534 | 71,878 | 0.027 | 0.32 |
| CB * | 183,639 | 13,842 | 170,163 | 14,034 | 175,566 | 15,418 | 7.9 × 10−11 | 0.97 |
| 12 YO ≤ Age < 15 YO | ||||||||
| Male (n = 93) | Female (n = 115) | Total (n = 208) | ||||||
| Description | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | p-value (male vs. female) | Absolute Cohen’s d (male vs. female) |
| Whole brain * | 1,921,579 | 164,698 | 1,768,993 | 116,849 | 1,837,216 | 159,244 | 3.4 × 10−12 | 1.09 |
| Cortical GM * | 767,612 | 76,019 | 681,028 | 61,996 | 719,741 | 80,915 | 8.6 × 10−16 | 1.26 |
| WM * | 493,138 | 60,699 | 443,730 | 43,184 | 465,821 | 57,192 | 5.3 × 10−10 | 0.95 |
| SGM * | 38,053 | 3318 | 36,274 | 2567 | 37,070 | 3051 | 3.6 × 10−5 | 0.61 |
| Extra-axial CSF | 435,120 | 78,133 | 435,147 | 66,097 | 435,135 | 71,548 | 0.998 | 3.8 × 10−4 |
| CB * | 187,656 | 14,739 | 172,814 | 12,441 | 179,450 | 15,379 | 7.1 × 10−13 | 1.01 |
| 15 YO ≤ Age < 18 YO | ||||||||
| Male (n = 72) | Female (n = 179) | Total (n = 251) | ||||||
| Description | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | Mean (mm3) | SD (mm3) | p-value (male vs. female) | Absolute Cohen’s d (male vs. female) |
| Whole brain * | 2,014,618 | 148,885 | 1,775,840 | 133,929 | 1,844,334 | 175,433 | 7.8 × 10−22 | 1.73 |
| Cortical GM * | 751,846 | 70,895 | 645,060 | 67,774 | 675,692 | 83,905 | 5.8 × 10−20 | 1.55 |
| WM * | 528,250 | 53,938 | 449,966 | 50,174 | 472,422 | 62,268 | 4.6 × 10−19 | 1.53 |
| SGM * | 39,862 | 3081 | 35,853 | 2632 | 37,003 | 3306 | 1.2 × 10−16 | 1.45 |
| Extra-axial CSF | 502,777 | 80,760 | 473,363 | 62,903 | 481,801 | 69,622 | 6.6 × 10−3 | 0.43 |
| CB * | 191,883 | 15,048 | 171,598 | 15,155 | 177,417 | 17,674 | 5.7 × 10−17 | 1.34 |
| Brain Volumetric Measurements | Male (n = 339) | Female (n = 507) | Total (n = 846) | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | p-Value (Male vs. Female) | Absolute Cohen’s d (Male vs. Female) | |
| Frontal GM | −0.45 | 0.91 | −0.30 | 0.98 | −0.36 | 0.96 | 0.024 | 0.16 |
| Temporal GM | −0.98 | 1.58 | −0.89 | 2.04 | −0.93 | 1.87 | 0.44 | 0.05 |
| Parietal GM | 0.72 | 1.91 | 0.66 | 2.29 | 0.69 | 2.15 | 0.67 | 0.03 |
| Occipital GM | −1.09 | 3.29 | −0.82 | 3.27 | −0.93 | 3.28 | 0.24 | 0.08 |
| Frontal WM | 0.40 | 1.20 | 0.37 | 1.16 | 0.38 | 1.18 | 0.74 | 0.02 |
| Temporal WM | −0.42 | 2.04 | −0.24 | 2.13 | −0.31 | 2.10 | 0.22 | 0.08 |
| Parietal WM | 0.69 | 2.07 | 0.62 | 1.92 | 0.65 | 1.98 | 0.66 | 0.03 |
| Occipital WM | −0.78 | 3.84 | −0.65 | 3.62 | −0.70 | 3.71 | 0.62 | 0.04 |
| Globus pallidus | 1.53 | 2.16 | 1.87 | 2.37 | 1.73 | 2.29 | 0.032 | 0.15 |
| Putamen | −1.25 | 1.28 | −1.43 | 1.49 | −1.36 | 1.41 | 0.051 | 0.13 |
| Fornix | 1.45 | 2.69 | 1.65 | 2.35 | 1.57 | 2.49 | 0.26 | 0.08 |
| Caudate | 0.37 | 1.92 | 0.59 | 1.87 | 0.50 | 1.89 | 0.091 | 0.12 |
| Thalamus | 0.28 | 0.96 | 0.36 | 0.91 | 0.33 | 0.93 | 0.24 | 0.08 |
| Subthalamic nucleus | −0.12 | 5.18 | 0.64 | 5.09 | 0.33 | 5.14 | 0.035 | 0.15 |
| Lateral ventricle | 2.86 | 16.94 | 4.83 | 16.07 | 4.04 | 16.44 | 0.092 | 0.12 |
| Cerebellum | 0.05 | 1.18 | 0.07 | 0.98 | 0.06 | 1.06 | 0.77 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiohama, T.; Maikusa, N.; Kawaguchi, M.; Natsume, J.; Hirano, Y.; Saito, K.; Takanashi, J.-i.; Levman, J.; Takahashi, E.; Matsumoto, K.; et al. A Brain Morphometry Study with Across-Site Harmonization Using a ComBat-Generalized Additive Model in Children and Adolescents. Diagnostics 2023, 13, 2774. https://doi.org/10.3390/diagnostics13172774
Shiohama T, Maikusa N, Kawaguchi M, Natsume J, Hirano Y, Saito K, Takanashi J-i, Levman J, Takahashi E, Matsumoto K, et al. A Brain Morphometry Study with Across-Site Harmonization Using a ComBat-Generalized Additive Model in Children and Adolescents. Diagnostics. 2023; 13(17):2774. https://doi.org/10.3390/diagnostics13172774
Chicago/Turabian StyleShiohama, Tadashi, Norihide Maikusa, Masahiro Kawaguchi, Jun Natsume, Yoshiyuki Hirano, Keito Saito, Jun-ichi Takanashi, Jacob Levman, Emi Takahashi, Koji Matsumoto, and et al. 2023. "A Brain Morphometry Study with Across-Site Harmonization Using a ComBat-Generalized Additive Model in Children and Adolescents" Diagnostics 13, no. 17: 2774. https://doi.org/10.3390/diagnostics13172774
APA StyleShiohama, T., Maikusa, N., Kawaguchi, M., Natsume, J., Hirano, Y., Saito, K., Takanashi, J.-i., Levman, J., Takahashi, E., Matsumoto, K., Yokota, H., Hattori, S., Tsujimura, K., Sawada, D., Uchida, T., Takatani, T., Fujii, K., Naganawa, S., Sato, N., & Hamada, H. (2023). A Brain Morphometry Study with Across-Site Harmonization Using a ComBat-Generalized Additive Model in Children and Adolescents. Diagnostics, 13(17), 2774. https://doi.org/10.3390/diagnostics13172774