
Usefulness of Contrast-Enhanced Endoscopic Ultrasound (CH-EUS) to Guide the Treatment Choice in Superficial Rectal Lesions: A Case Series

 , ,
, ,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients’ Selection
- -
- Paris and Laterally Spreading Tumor (LST) classification corresponding to 0-Is, 0-IIa, 0-IIb or mixed lesions (0-IIc + IIa or 0-IIa + IIc); LST nongranular (LST-NG or pseudodepressed, IIc); or LST granular nodular mixed type.
- -
- The concomitant presence of a demarcated focal area depressed or with an irregular surface pattern or bulky component corresponding to JNET 2B/3 (Figure 1).
2.2. Contrast-Enhanced Endoscopic Ultrasound Technique
- -
- Standard EUS for the definition of the degree of parietal infiltration without contrast agent and the search for pathological lymph nodes providing staging.
- -
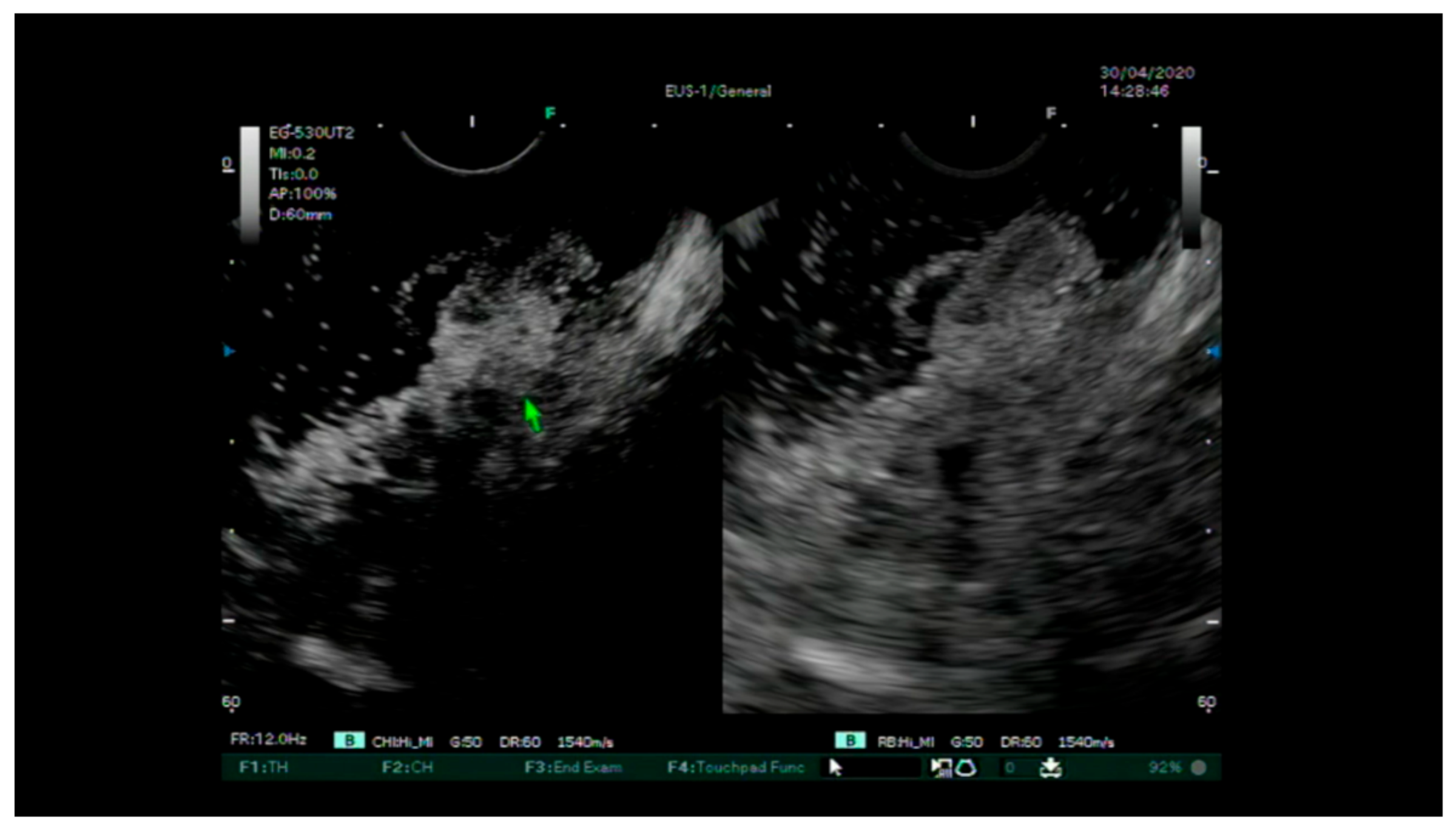
- The injection of the intravenous contrast agent (Sonovue ©) and the assessment of the entirety of the various layers of the rectum wall arterial and portal venous phases (Figure 2 and Figure 3). Finally, a uT and N stage was assigned for each lesion. After the removal of the lesions via an endoscopic or surgical procedure, complete pathological staging (pTNM) was performed, including the degree of differentiation, lymphatic invasion, vascular invasion and tumor budding according to the WHO classification [27].
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zauber, A.G.; Winawer, S.J.; O’Brien, M.J.; Lansdorp-Vogelaar, I.; van Ballegooijen, M.; Hankey, B.F.; Shi, W.; Bond, J.H.; Schapiro, M.; Panish, J.F.; et al. Colonoscopic Polypectomy and Long-Term Prevention of Colorectal-Cancer Deaths. N. Engl. J. Med. 2012, 366, 687–696. [Google Scholar] [CrossRef]
- ASGE Standards of Practice Committee; Fisher, D.A.; Shergill, A.K.; Early, D.S.; Acosta, R.D.; Chandrasekhara, V.; Chathadi, K.V.; Decker, G.A.; Evans, J.A.; Fanelli, R.D.; et al. Role of endoscopy in the staging and management of colorectal cancer. Gastrointest. Endosc. 2013, 78, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Fujishiro, M.; Yahagi, N.; Nakamura, M.; Kakushima, N.; Kodashima, S.; Ono, S.; Kobayashi, K.; Hashimoto, T.; Yamamichi, N.; Tateishi, A.; et al. Endoscopic Submucosal Dissection for Rectal Epithelial Neoplasia. Endoscopy 2006, 38, 493–497. [Google Scholar] [CrossRef]
- Probst, A.; Ebigbo, A.; Märkl, B.; Schaller, T.; Anthuber, M.; Fleischmann, C.; Messmann, H. Endoscopic submucosal dissection for early rectal neoplasia: Experience from a European center. Endoscopy 2016, 49, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Oka, S.; Kaneko, I.; Hirata, M.; Mouri, R.; Kanao, H.; Yoshida, S.; Chayama, K. Endoscopic submucosal dissection for colorectal neoplasia: Possibility of standardization. Gastrointest. Endosc. 2007, 66, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Hashiguchi, Y.; Muro, K.; Saito, Y.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hasegawa, K.; Hotta, K.; Ishida, H.; Ishiguro, M.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2019, 25, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Ferlitsch, M.; Moss, A.; Hassan, C.; Bhandari, P.; Dumonceau, J.-M.; Paspatis, G.; Jover, R.; Langner, C.; Bronzwaer, M.; Nalankilli, K.; et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017, 49, 270–297. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Dinis-Ribeiro, M.; Ponchon, T.; Repici, A.; Vieth, M.; De Ceglie, A.; Amato, A.; Berr, F.; Bhandari, P.; Bialek, A.; et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015, 47, 829–854. [Google Scholar] [CrossRef]
- Rutter, D. British Society of Gastroenterology/Association of Coloproctologists of Great Britain and Ireland guidelines for the management of large non-pedunculated colorectal polyps. Gut 2015, 64, 1847–1873. [Google Scholar] [CrossRef]
- Bourke, M.J. Colorectal endoscopic submucosal dissection: When and by whom? Endoscopy 2014, 46, 677–679. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Libânio, D.; Bastiaansen, B.A.J.; Bhandari, P.; Bisschops, R.; Bourke, M.J.; Esposito, G.; Lemmers, A.; Maselli, R.; Messmann, H.; et al. Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2022. Endoscopy 2022, 54, 591–622. [Google Scholar] [CrossRef] [PubMed]
- Kudo, S.; Rubino, C.A.; Teixeira, C.R.; Kashida, H.; Kogure, E. Pit Pattern in Colorectal Neoplasia: Endoscopic Magnifying View. Endoscopy 2001, 33, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Kouyama, Y.; Kudo, S.-E.; Miyachi, H.; Ichimasa, K.; Hisayuki, T.; Oikawa, H.; Matsudaira, S.; Kimura, Y.J.; Misawa, M.; Mori, Y.; et al. Practical problems of measuring depth of submucosal invasion in T1 colorectal carcinomas. Int. J. Color. Dis. 2015, 31, 137–146. [Google Scholar] [CrossRef]
- Iwatate, M.; Sano, Y.; Tanaka, S.; Kudo, S.; Saito, S.; Matsuda, T.; Wada, Y.; Fujii, T.; Ikematsu, H.; Uraoka, T.; et al. Validation study for development of the Japan NBI Expert Team classification of colorectal lesions. Dig. Endosc. 2018, 30, 642–651. [Google Scholar] [CrossRef]
- Ma, M.X.; Tate, D.J.; Sidhu, M.; Zahid, S.; Bourke, M.J. Effect of pre-resection biopsy on detection of advanced dysplasia in large nonpedunculated colorectal polyps undergoing endoscopic mucosal resection. Endoscopy 2022, 55, 267–273. [Google Scholar] [CrossRef]
- Markarian, E.; Fung, B.M.; Girotra, M.; Tabibian, J.H. Large polyps: Pearls for the referring and receiving endoscopist. World J. Gastrointest. Endosc. 2021, 13, 638–648. [Google Scholar] [CrossRef]
- Beynon, J.; Foy, D.M.A.; Temple, L.N.; Channer, J.L.; Virjee, J.; Mortensen, N.J.M.C. The endosonic appearances of normal colon and rectum. Dis. Colon Rectum 1986, 29, 810–813. [Google Scholar] [CrossRef]
- Uberoi, A.S.; Bhutani, M.S. Has the role of EUS in rectal cancer staging changed in the last decade? Endosc. Ultrasound 2018, 7, 366–370. [Google Scholar]
- Marusch, F.; Koch, A.; Schmidt, U.; Zippel, R.; Kuhn, R.; Wolff, S.; Pross, M.; Wierth, A.; Gastinger, I.; Lippert, H. Routine Use of Transrectal Ultrasound in Rectal Carcinoma: Results of a Prospective Multicenter Study. Endoscopy 2002, 34, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Akasu, T.; Kondo, H.; Moriya, Y.; Sugihara, K.; Gotoda, T.; Fujita, S.; Muto, T.; Kakizoe, T. Endorectal ultrasonography and treatment of early stage rectal cancer. World J. Surg. 2000, 24, 1061–1068. [Google Scholar] [CrossRef]
- Puli, S.R.; Bechtold, M.L.; Reddy, J.B.K.; Choudhary, A.; Antillon, M.R.; Brugge, W.R. How Good is Endoscopic Ultrasound in Differentiating Various T Stages of Rectal Cancer? Meta-Analysis and Systematic Review. Ann. Surg. Oncol. 2008, 16, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Esparrach, G.; Ayuso-Colella, J.R.; Sendino, O.; Pagés, M.; Cuatrecasas, M.; Pellisé, M.; Maurel, J.; Ayuso-Colella, C.; González-Suárez, B.; Llach, J.; et al. EUS and magnetic resonance imaging in the staging of rectal cancer: A prospective and comparative study. Gastrointest. Endosc. 2011, 74, 347–354. [Google Scholar] [CrossRef]
- Hurlstone, D.P.; Hunter, M.D.; Sanders, D.S.; Thomson, M.; Cross, S.S. Olympus Lucera high-resolution vascular ectasia mapping in combination with the type V crypt pattern for the invasive depth estimation and nodal disease estimation in Paris type II colorectal cancers: A comparative prospective analysis to 20 MHz ultrasound. J. Clin. Gastroenterol. 2007, 41, 178–184. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Sahai, A.V.; D’Onofrio, M.; Will, U.; Arcidiacono, P.G.; Petrone, M.C.; Hocke, M.; Braden, B.; Burmester, E.; Möller, K.; et al. Differential diagnosis of small solid pancreatic lesions. Gastrointest. Endosc. 2016, 84, 933–940. [Google Scholar] [CrossRef]
- Wang, Y.; Li, L.; Wang, Y.-X.J.; Cui, N.-Y.; Zou, S.-M.; Zhou, C.-W.; Jiang, Y.-X. Time-Intensity Curve Parameters in Rectal Cancer Measured Using Endorectal Ultrasonography with Sterile Coupling Gels Filling the Rectum: Correlations with Tumor Angiogenesis and Clinicopathological Features. BioMed Res. Int. 2014, 2014, 587806. [Google Scholar] [CrossRef]
- Dabizzi, E.; La Marca, M.; Carlini, E.; Landi, S.; Polifemo, A.; Ghersi, S.; Bassi, M.; Cennamo, V. OC.10.1 Reliability of linear eus in rectal cancer staging: A non-inferiority evaluation between gold standards. Dig. Liver Dis. 2021, 53, S131–S132. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; the WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Hsieh, M.-C.; Chen, C.-J.; Huang, W.-S. McKittrick–Wheelock Syndrome. Clin. Gastroenterol. Hepatol. 2016, 14, e41–e42. [Google Scholar] [CrossRef]
- Van Doorn, S.C.; Hazewinkel, Y.; East, J.E.; van Leerdam, M.E.; Rastogi, A.; Pellise, M.; Sanduleanu-Dascalescu, S.; Bastiaansen, B.A.J.; Fockens, P.; Dekker, E. Polyp Morphology: An Interobserver Evaluation for the Paris Classification Among International Experts. Am. J. Gastroenterol. 2015, 110, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Yamada, M.; Takamaru, H.; Sakamoto, T.; Matsuda, T.; Sekine, S.; Igarashi, Y.; Saito, Y. Diagnostic yield of the Japan NBI Expert Team (JNET) classification for endoscopic diagnosis of superficial colorectal neoplasms in a large-scale clinical practice database. United Eur. Gastroenterol. J. 2019, 7, 914–923. [Google Scholar] [CrossRef]
- Lu, M.; Yan, B.; Song, J.; Ping, W.; Yue, L.-X.; Song, B. Double-Contrast-Enhanced Sonography for Diagnosis of Rectal Lesions With Pathologic Correlation. J. Ultrasound Med. 2014, 33, 575–583. [Google Scholar] [CrossRef]
- Binda, C.; Coluccio, C.; Marocchi, G.; Sbrancia, M.; Fabbri, C. The Role of Contrast-Enhanced Harmonic Endoscopic Ultrasound in Interventional Endoscopic Ultrasound. Medicina 2021, 57, 1085. [Google Scholar] [CrossRef] [PubMed]
- Fusaroli, P.; Kypraios, D.; Mancino, M.G.; Spada, A.; Benini, M.C.; Bianchi, M.; Bocus, P.; De Angelis, C.; De Luca, L.; Fabbri, C.; et al. Interobserver agreement in contrast harmonic endoscopic ultrasound. J. Gastroenterol. Hepatol. 2012, 27, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Moons, L.M.G.; Bastiaansen, B.A.J.; Richir, M.C.; Hazen, W.L.; Tuynman, J.; Elias, S.G.; Schrauwen, R.W.M.; Vleggaar, F.P.; Dekker, E.; Bos, P.; et al. Endoscopic intermuscular dissection for deep submucosal invasive cancer in the rectum: A new endoscopic approach. Endoscopy 2022, 54, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, S.; Hompes, R.; Slater, A.; Lindsey, I.; Bach, S.; Mortensen, N.J.; Cunningham, C.; Association of Coloproctology of Great Britain and Ireland Transanal Endoscopic Microsurgery (TEM) Collaboration. A critical appraisal of endorectal ultrasound and transanal endoscopic microsurgery and decision-making in early rectal cancer. Color. Dis. 2011, 14, 821–826. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Sex | Age | Location 1 | Size, mm | Paris and/or LST Classification | JNET Classification | Biopsy | CH-EUS Stage | MRI Stage | Treatment | pTNM Stage |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 74 | Proximal | 30 | 0-Is | Type 3 in the central area | Tubular adenoma HGD | uT2N+ | T2/T3 | RAR | pT2N0G1LV0R0 |
| 2 | F * | 68 | Medium-distal | 180 | 0-IIa + Is/LST-G nodular mixed | 2b/focal 3 in dominant nodule | Tubular adenoma HGD | uT1aN0 | T1/T2 | ESD converted to RAR | pT2N1b |
| 3 | M | 79 | Medium-distal | 60 | 0-IIa + Is/LST-G nodular mixed | 2b/focal 3 | - | uT1N0 | - | Hybrid-ESD | pT1a G1 |
| 4 | M | 74 | Proximal | 20 | 0-Is | 2b/focal 3 | Adenoma HGD | uT2N0 | T2/T3 | RAR | pT2 N0 G2 LV0R0 |
| 5 | F | 70 | Distal | 30 | 0-Is + IIa/LST-G nodular mixed type | 2b/focal 3 in dominant nodule | Villous adenoma HGD | uT1N0 | - | ESD | Villous Adenoma HGD |
| 6 | M | 65 | Distal | 35 | 0-Is + IIa/LST-G nodular mixed type | 2b/focal 3 in dominant nodule | - | uTisN0 | - | ESD | TV Adenoma HGD |
| 7 | F | 65 | Medium-distal | 45 | 0-Is + IIa/LST-G nodular mixed type | 2b/focal 3 | - | uTis | - | Hybrid-ESD | TV Adenoma HGD |
| 8 | F | 72 | Distal | 35 | 0-Is + IIa/LST-G nodular mixed type | 2b/focal 3 | Previous piecemeal resection: TV adenoma HGD | uT1aN0 | - | ESD | TV Adenoma HGD |
| 9 | F | 68 | Medium-distal | 80 | 0-IIa + Is/LST-G nodular mixed type | 2b/focal 3 in 20 mm-dominant nodule | - | uTis | - | Hybrid-ESD | TV Adenoma HGD |
| 10 | M | 81 | Proximal | 35 | 0-Is | 2b/focal 3 | - | uTis | - | Hybrid-ESD | TV Adenoma HGD |
| 11 | F | 72 | Medium-distal | 30 | 0-IIa + IIc/LST-NG | 2b/focal 3 | Adenoma HGD and focal adenocarcinoma | uT1N0 | T2 | RAR + TME | pT1 N1b G2 LV0 R0 |
| 12 | F | 57 | Distal | 30 | 0-IIa + IIc/LST-NG | 2b/focal 3 | - | uT1N0 | - | ESD | pT1a G1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibiino, G.; Sbrancia, M.; Binda, C.; Coluccio, C.; Fabbri, S.; Giuffrida, P.; Gallo, G.; Saragoni, L.; Maselli, R.; Repici, A.; et al. Usefulness of Contrast-Enhanced Endoscopic Ultrasound (CH-EUS) to Guide the Treatment Choice in Superficial Rectal Lesions: A Case Series. Diagnostics 2023, 13, 2267. https://doi.org/10.3390/diagnostics13132267
Gibiino G, Sbrancia M, Binda C, Coluccio C, Fabbri S, Giuffrida P, Gallo G, Saragoni L, Maselli R, Repici A, et al. Usefulness of Contrast-Enhanced Endoscopic Ultrasound (CH-EUS) to Guide the Treatment Choice in Superficial Rectal Lesions: A Case Series. Diagnostics. 2023; 13(13):2267. https://doi.org/10.3390/diagnostics13132267
Chicago/Turabian StyleGibiino, Giulia, Monica Sbrancia, Cecilia Binda, Chiara Coluccio, Stefano Fabbri, Paolo Giuffrida, Graziana Gallo, Luca Saragoni, Roberta Maselli, Alessandro Repici, and et al. 2023. "Usefulness of Contrast-Enhanced Endoscopic Ultrasound (CH-EUS) to Guide the Treatment Choice in Superficial Rectal Lesions: A Case Series" Diagnostics 13, no. 13: 2267. https://doi.org/10.3390/diagnostics13132267
APA StyleGibiino, G., Sbrancia, M., Binda, C., Coluccio, C., Fabbri, S., Giuffrida, P., Gallo, G., Saragoni, L., Maselli, R., Repici, A., & Fabbri, C. (2023). Usefulness of Contrast-Enhanced Endoscopic Ultrasound (CH-EUS) to Guide the Treatment Choice in Superficial Rectal Lesions: A Case Series. Diagnostics, 13(13), 2267. https://doi.org/10.3390/diagnostics13132267