
Analysis of Positive Results of 18F-FDG PET/CT Imaging after Hematopoietic Stem Cell Transplantation in Lymphoma



Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. 18F-FDG-PET/CT Imaging
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Autologous SCTs
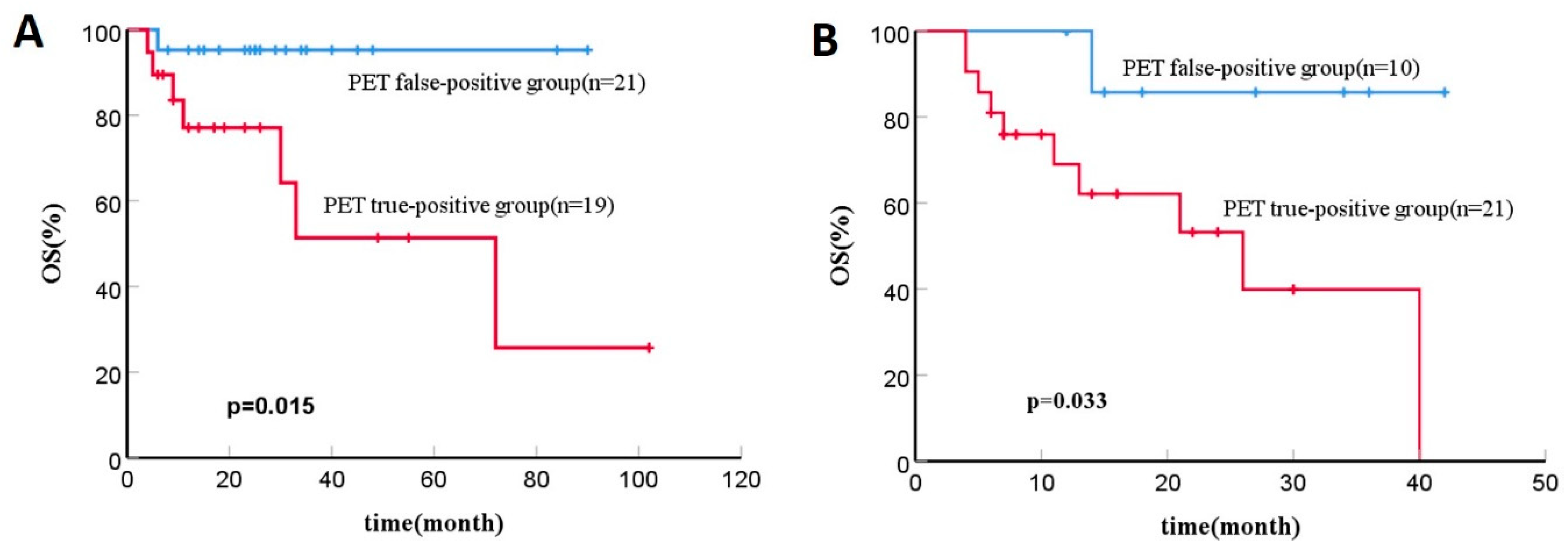
3.2.1. 18F-FDG PET-CT Results and Outcomes
3.2.2. Analysis of Positive Results of Post-SCT 18F-FDG PET/CT
3.3. Allogeneic SCTs
3.3.1. 18F-FDG PET-CT Results and Outcomes
3.3.2. Analysis of Positive Results of Post-SCT 18F-FDG PET/CT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Armitage, J.O.; Gascoyne, R.D.; Lunning, M.A.; Cavalli, F. Non-Hodgkin lymphoma. Lancet 2017, 390, 298–310. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Ambinder, R.F. Hodgkin lymphoma: A review and update on recent progress. CA Cancer J. Clin. 2018, 68, 116–132. [Google Scholar] [CrossRef] [PubMed]
- Mehta-Shah, N.; Teja, S.; Tao, Y.; Cashen, A.F.; Beaven, A.; Alpdogan, O.; Porcu, P.; Wiggin, M.; Song, K.W.; Alzahrani, M.; et al. Successful Treatment of Mature T-Cell Lymphoma with Allogeneic Stem Cell Transplantation: The Largest Multicenter Retrospective Analysis. Blood 2017, 130, 35–36. [Google Scholar] [CrossRef]
- Mamez, A.C.; Dupont, A.; Blaise, D.; Chevallier, P.; Forcade, E.; Ceballos, P.; Mohty, M.; Suarez, F.; Beguin, Y.; Peffault De Latour, R.; et al. Allogeneic stem cell transplantation for peripheral T cell lymphomas: A retrospective study in 285 patients from the Société Francophone de Greffe de Moelle et de Thérapie Cellulaire (SFGM-TC). J. Hematol. Oncol. 2020, 13, 56. [Google Scholar] [CrossRef]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A.; Alliance, Australasian Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group; European Mantle Cell Lymphoma Consortium; et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Dai, N.; Zhou, Y.; Deng, S.; Sang, S.; Wu, Y. Prognostic Value of 2-Deoxy-2-[18F]fluoro-D-glucose Positron Emission Tomography/Computed Tomography after Autologous Hematopoietic Stem Cell Transplantation in Lymphoma Using Deauville Scores. Contrast Media Mol. Imaging 2021, 2021, 5510825. [Google Scholar] [CrossRef]
- Dai, N.; Liu, H.; Deng, S.; Sang, S.; Wu, Y. Post-transplantation Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography in Patients with Lymphoblastic Lymphoma is an Independent Prognostic Factor with an Impact on Progression-Free Survival but not Overall Survival. Technol. Cancer Res. Treat. 2021, 20, 15330338211056478. [Google Scholar] [CrossRef]
- West, J.D.; Kim, M.E.; Lapalma, D.M.; Vergara-Lluri, M.; Conti, P.; Chambers, T.N.; Swanson, M.S. 18F-FDG-PET/CT Specificity for the Detection of Lymphoma Recurrence in the Tonsils. OTO Open 2021, 5, 2473974X211059081. [Google Scholar] [CrossRef]
- Cronin, C.G.; Swords, R.; Truong, M.T.; Viswanathan, C.; Rohren, E.; Giles, F.J.; O’Dwyer, M.; Bruzzi, J.F. Clinical utility of PET/CT in lymphoma. AJR Am. J. Roentgenol. 2010, 194, W91–W103. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.A.; Kwee, T.C. Proportion of false-positive lesions at interim and end-of-treatment FDG-PET in lymphoma as determined by histology: Systematic review and meta-analysis. Eur. J. Radiol. 2016, 85, 1963–1970. [Google Scholar] [CrossRef] [PubMed]
- Oriuchi, N.; Sugawara, S.; Shiga, T. Positron Emission Tomography for Response Evaluation in Microenvironment-Targeted Anti-Cancer Therapy. Biomedicines 2020, 8, 371. [Google Scholar] [CrossRef] [PubMed]
- Maffione, A.M.; Rampin, L.; Rossella, P.; Pecori, S.; Colletti, P.M.; Rubello, D. False-Positive 18F-FDG PET/CT Due to Filgrastim That Induced Extramedullary Liver Hematopoiesis in a Burkitt Lymphoma. Clin. Nucl. Med. 2018, 43, e130–e131. [Google Scholar] [CrossRef] [PubMed]
- Spaepen, K.; Stroobants, S.; Dupont, P.; Bormans, G.; Balzarini, J.; Verhoef, G.; Mortelmans, L.; Vandenberghe, P.; Wolf-Peeters, C.D. [(18)F]FDG PET monitoring of tumour response to chemotherapy: Does [(18)F]FDG uptake correlate with the viable tumour cell fraction? Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 682–688. [Google Scholar] [CrossRef]
- Naumann, R.; Vaic, A.; Beuthien-Baumann, B.; Bredow, J.; Kropp, J.; Kittner, T.; Franke, W.G.; Ehninger, G. Prognostic value of positron emission tomography in the evaluation of post-treatment residual mass in patients with Hodgkin’s disease and non-Hodgkin’s lymphoma. Br. J. Haematol. 2001, 115, 793–800. [Google Scholar] [CrossRef]
- Weihrauch, M.R.; Re, D.; Scheidhauer, K.; Ansén, S.; Dietlein, M.; Bischoff, S.; Bohlen, H.; Wolf, J.; Schicha, H.; Diehl, V.; et al. Thoracic positron emission tomography using 18F-fluorodeoxyglucose for the evaluation of residual mediastinal Hodgkin disease. Blood 2001, 98, 2930–2934. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Lilienstein, J.; Gönen, M.; Maragulia, J.; Moskowitz, C.H.; Zelenetz, A.D. False-Positive [18F]fluorodeoxyglucose-avid lymph nodes on positron emission tomography-computed tomography after allogeneic but not autologous stem-cell transplantation in patients with lymphoma. J. Clin. Oncol. 2014, 32, 51–56. [Google Scholar] [CrossRef]
- Palmer, J.; Goggins, T.; Broadwater, G.; Chao, N.; Horwitz, M.; Beaven, A.; Sullivan, K.; Coleman, R.E.; Rizzieri, D. Early post transplant (F-18) 2-fluoro-2-deoxyglucose positron emission tomography does not predict outcome for patients undergoing auto-SCT in non-Hodgkin and Hodgkin lymphoma. Bone Marrow Transplant. 2011, 46, 847–851. [Google Scholar] [CrossRef]
- Wang, C.; Li, P.; Wu, S.; Lu, J.; Liu, Q.; Luo, H.; Song, S. The role of fluorine-18 fluorodeoxyglucose PET in prognosis evaluation for stem cell transplantation of lymphoma: A systematic review and meta-analysis. Nucl. Med. Commun. 2016, 37, 338–347. [Google Scholar] [CrossRef]
- Cheson, B.D.; Horning, S.J.; Coiffier, B.; Shipp, M.A.; Fisher, R.I.; Connors, J.M.; Lister, T.A.; Vose, J.; Grillo-López, A.; Hagenbeek, A.; et al. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J. Clin. Oncol. 1999, 17, 1244. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, R.T.; Advani, R.H.; Ai, W.Z.; Ambinder, R.F.; Armand, P.; Bello, C.M.; Benitez, C.M.; Chen, W.; Dabaja, B.; Daly, M.E.; et al. NCCN Guidelines® Insights: Hodgkin Lymphoma, Version 2. J. Natl. Compr. Cancer Netw. 2022, 20, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Zelenetz, A.D.; Gordon, L.I.; Chang, J.E.; Christian, B.; Abramson, J.S.; Advani, R.H.; Bartlett, N.L.; Budde, L.E.; Caimi, P.F.; De Vos, S.; et al. NCCN Guidelines® Insights: B-Cell Lymphomas, Version 5. J. Natl. Compr. Cancer Netw. 2021, 19, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, S.M.; Ansell, S.; Ai, W.Z.; Barnes, J.; Barta, S.K.; Brammer, J.; Clemens, M.W.; Dogan, A.; Foss, F.; Ghione, P.; et al. T-Cell Lymphomas, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 285–308. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of imaging in the staging and response assessment of lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef]
- Barrington, S.F.; Trotman, J. The role of PET in the first-line treatment of the most common subtypes of non-Hodgkin lymphoma. Lancet Haematol. 2021, 8, e80–e93. [Google Scholar] [CrossRef]
- Trotman, J.; Barrington, S.F. The role of PET in first-line treatment of Hodgkin lymphoma. Lancet Haematol. 2021, 8, e67–e79. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mir, F.; El-Galaly, T.C.; Knapp, A.; Nielsen, T.G.; Sahin, D.; Wenger, M.; Kostakoglu, L.; Trotman, J.; Meignan, M. Follicular Lymphoma Treated with First-Line Immunochemotherapy: A Review of PET/CT in Patients Who Did Not Achieve a Complete Metabolic Response in the GALLIUM Study. J. Nucl. Med. 2022, 63, 1149–1154. [Google Scholar] [CrossRef]
- Qiao, W.; Zhao, J.; Xing, Y.; Wang, C.; Wang, T. Predictive value of [¹⁸F]fluoro-2-deoxy-D-glucose positron emission tomography for clinical outcome in patients with relapsed/refractory diffuse large B-cell lymphoma prior to and after autologous stem cell transplant. Leuk. Lymphoma 2014, 55, 276–282. [Google Scholar] [CrossRef]
- Sohn, B.S.; Yoon, D.H.; Kim, K.P.; Kim, S.; Lee, K.M.; Park, J.S.; Lee, D.H.; Ryu, J.S.; Huh, J.; Hong, I.K.; et al. The role of ¹⁸F-fluorodeoxyglucose positron emission tomography at response assessment after autologous stem cell transplantation in T-cell non-Hodgkin’s lymphoma patients. Ann. Hematol. 2013, 92, 1369–1377. [Google Scholar] [CrossRef]
- Lavi, N.; Shapira, G.; Zilberlicht, A.; Benyamini, N.; Farbstein, D.; Dann, E.J.; Bar-Shalom, R.; Avivi, I. Integration of CT-Based Measurements into Surveillance PET/CT in Patients with Diffuse Large B Cell Lymphoma. Isr. Med. Assoc. J. 2016, 18, 411–417. [Google Scholar] [PubMed]
- Endoh, H.; Yamamoto, R.; Ichikawa, A.; Shiozawa, S.; Nishizawa, N.; Satoh, Y.; Oriuchi, N. Clinicopathologic Significance of False-Positive Lymph Node Status on FDG-PET in Lung Cancer. Clin. Lung Cancer 2021, 22, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Meignan, M.; Itti, E.; Gallamini, A.; Younes, A. FDG PET/CT imaging as a biomarker in lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Younes, A.; Hilden, P.; Coiffier, B.; Hagenbeek, A.; Salles, G.; Wilson, W.; Seymour, J.F.; Kelly, K.; Gribben, J.; Pfreunschuh, M.; et al. International Working Group consensus response evaluation criteria in lymphoma (RECIL 2017). Ann. Oncol. 2017, 28, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D. PET/CT in Lymphoma: Current Overview and Future Directions. Semin. Nucl. Med. 2018, 48, 76–81. [Google Scholar] [CrossRef]
- Luminari, S.; Galimberti, S.; Versari, A.; Biasoli, I.; Anastasia, A.; Rusconi, C.; Ferrari, A.; Petrini, M.; Manni, M.; Federico, M. Positron emission tomography response and minimal residual disease impact on progression-free survival in patients with follicular lymphoma. A subset analysis from the FOLL05 trial of the Fondazione Italiana Linfomi. Haematologica 2016, 101, e66–e68. [Google Scholar] [CrossRef]
- Hayden, A.R.; Tonseth, P.; Lee, D.G.; Villa, D.; Gerrie, A.S.; Scott, D.W.; Freeman, C.L.; Slack, G.W.; Farinha, P.; Skinnider, B.; et al. Outcome of primary mediastinal large B-cell lymphoma using R-CHOP: Impact of a PET-adapted approach. Blood 2020, 136, 2803–2811. [Google Scholar] [CrossRef]
- Isik, E.G.; Kuyumcu, S.; Kebudi, R.; Sanli, Y.; Karakas, Z.; Cakir, F.B.; Unal, S.N. Prediction of outcome in pediatric Hodgkin lymphoma based on interpretation of 18FDG-PET/CT according to ΔSUVmax, Deauville 5-point scale and IHP criteria. Ann. Nucl. Med. 2017, 31, 660–668. [Google Scholar] [CrossRef]
- Yuan, L.; Kreissl, M.C.; Su, L.; Wu, Z.; Hacker, M.; Liu, J.; Zhang, X.; Bo, Y.; Zhang, H.; Li, X.; et al. Prognostic analysis of interim 18F-FDG PET/CT in patients with diffuse large B cell lymphoma after one cycle versus two cycles of chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 478–488. [Google Scholar] [CrossRef]
- Kim, J.; Song, Y.S.; Lee, J.S.; Lee, W.W.; Kim, S.E. Risk stratification of diffuse large B-cell lymphoma with interim PET-CT based on different cutoff Deauville scores. Leuk. Lymphoma 2018, 59, 340–347. [Google Scholar] [CrossRef]
- Xie, W.; Liu, M.K.; Jiang, X.F.; Gao, X.D.; Li, B.; Wang, L.; Zhao, W.L. Improved prediction of chemoresistance in patients with diffuse large B-cell lymphoma through a new interim positron emission tomography-computed tomography evaluation model. Acta Oncol. 2021, 60, 735–743. [Google Scholar] [CrossRef]
- Rekowski, J.; Hüttmann, A.; Schmitz, C.; Müller, S.P.; Kurch, L.; Kotzerke, J.; Franzius, C.; Weckesser, M.; Bengel, F.M.; Freesmeyer, M.; et al. Interim PET Evaluation in Diffuse Large B-Cell Lymphoma Using Published Recommendations: Comparison of the Deauville 5-Point Scale and the ΔSUVmax Method. J. Nucl. Med. 2021, 62, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Nachmias, B.; Godefroy, J.; Rozenbach, E.; Ganzel, C.; Bar-Shalom, R.; Goldschmidt, N.; Vainstein, V. Posttreatment FDG-Avid Splenic Lesions in DLBCL and HD: Clinical and Radiographic Characteristics for Risk Assessment. Clin. Nucl. Med. 2020, 45, 542–544. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Krishnaraju, V.; Mittal, B.; Bhattacharya, A.; Singh, H.; Prakash, G. Role of Fluorodeoxyglucose Positron emission tomography/computed tomography and PET/CT guided directed core needle biopsy during the different management stages of lymphoma. J. Nucl. Med. 2022, 63 (Suppl. S2), 3130. [Google Scholar]
- Zhao, Z.; Zhou, Y.; Wang, J.; Zhang, T.; Li, J.; Zhang, B.; Li, Q.; Deng, S. The value of 18F-FDG PET/CT in the prediction of clinical outcomes of patients with acute leukemia treated with allogeneic hematopoietic stem cell transplantation. Oncol. Lett. 2020, 20, 175. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Autologous SCT | Allogeneic SCT |
|---|---|---|
| No. of patients | 101 | 84 |
| No. of post-transplantation PET/CT scans | 105 | 130 |
| Sex | ||
| Male | 65/101 | 53/84 |
| Female | 36/101 | 31/84 |
| Age | 37 (12–73) | 28 (8–58) |
| Histology | ||
| HL | 16/101 | 2/84 |
| B-NHL | 48/101 | 20/84 |
| T-NHL | 37/101 | 62/84 |
| Median follow-up, month (range) | 24 (4–120) | 16 (4–99) |
| Number of previous treatments | ||
| 1 | 50/101 | 33/84 |
| >1 | 51/101 | 51/84 |
| Status at SCT | ||
| CR + PR | 87/101 | 66/84 |
| SD + PD | 14/101 | 18/84 |
| PET results | ||
| Negative (DS < 4) | 65/105 | 99/130 |
| Positive (DS = 4 or 5) | 40/105 | 31/130 |
| Integrated CT results | ||
| Negative | 76/105 | 100/130 |
| Positive | 29/105 | 30/130 |
| lymphoma involvement | 19/105 | 21/130 |
| Variable | Autologous SCT | Allogeneic SCT | Autologous and Allogeneic SCT | ||||||
|---|---|---|---|---|---|---|---|---|---|
| False-Positive | True-Positive | p Value | False-Positive | True-Positive | p Value | False-Positive | True-Positive | p Value | |
| No. of positive post-transplantation PET/CT scans | 21 | 19 | 10 | 21 | 31 | 40 | |||
| Sex | |||||||||
| Male | 12 | 13 | 0.527 | 5 | 13 | 0.701 | 17 | 26 | 0.465 |
| Female | 9 | 6 | 5 | 8 | 14 | 14 | |||
| Age | 31 (13–66) | 37 (18–59) | 0.506 | 44 (8–46) | 29 (13–58) | 0.102 | 37 (8–66) | 34 (13–59) | 0.431 |
| Histology | |||||||||
| HL | 5 | 3 | 0.546 | 0 | 1 | 0.615 | 5 | 4 | 0.226 |
| B-NHL | 9 | 6 | 4 | 5 | 13 | 11 | |||
| T-NHL | 7 | 10 | 6 | 15 | 13 | 25 | |||
| Number of previous treatments | |||||||||
| 1 | 9 | 6 | 0.527 | 5 | 3 | 0.074 | 14 | 9 | 0.072 |
| >1 | 12 | 13 | 5 | 18 | 17 | 31 | |||
| Status at SCT | |||||||||
| CR + PR | 19 | 16 | 0.654 | 10 | 15 | 0.141 | 29 | 31 | 0.098 |
| SD + PD | 2 | 3 | 0 | 6 | 2 | 9 | |||
| Conditioning regimen (auto-SCT) | |||||||||
| BEAM | 14 | 14 | 0.886 | - | - | - | - | - | - |
| BuCy | 4 | 2 | - | - | |||||
| others | 3 | 3 | - | - | - | - | |||
| Conditioning regimen (allo-SCT) | |||||||||
| BuCy | - | - | - | 6 | 11 | 1.000 | - | - | - |
| TBI containing treatment | - | - | 4 | 10 | - | - | |||
| Donor type | |||||||||
| HLA identical sibling | - | - | - | 1 | 6 | 0.193 | - | - | - |
| HLA haploidentical sibling | - | - | - | 8 | 9 | - | - | ||
| Unrelated | - | - | - | 1 | 6 | - | - | ||
| Timing of Post-SCT 18F-FDG PET-CT | |||||||||
| Within 3 months | 10 | 10 | 1.000 | 5 | 7 | 0.447 | - | - | - |
| Within 3–6 months (auto-SCT) | 11 | 9 | - | - | |||||
| Within 3–12 months (allo-SCT) | 5 | 14 | - | - | |||||
| Immunomodulatory or CAR-T therapy prior to post-SCT PET scan | |||||||||
| Yes | 0 | 1 | 0.475 | 0 | 3 | 0.533 | 0 | 4 | 0.126 |
| No | 21 | 18 | 10 | 18 | 31 | 36 | |||
| DS score | |||||||||
| DS = 4 | 16 | 9 | 0.102 | 9 | 10 | 0.046 * | 25 | 19 | 0.006 * |
| DS = 5 | 5 | 10 | 1 | 11 | 6 | 21 | |||
| Unifocal or multifocal | |||||||||
| Unifocal | 15 | 7 | 0.055 | 7 | 7 | 0.121 | 22 | 14 | 0.004 * |
| Multifocal | 6 | 12 | 3 | 14 | 9 | 26 | |||
| FDG-avid foci occurred in the sites of original disease | |||||||||
| Yes | 10 | 1 | 0.004 * | 5 | 2 | 0.022 * | 15 | 3 | 0.000 * |
| No | 11 | 18 | 5 | 19 | 16 | 37 | |||
| FDG-avid foci were in lymph nodes only | |||||||||
| Yes | 16 | 13 | 0.723 | 5 | 7 | 0.447 | 21 | 20 | 0.153 |
| No | 5 | 6 | 5 | 14 | 10 | 20 | |||
| Integrated CT results | |||||||||
| Negative | 18 | 1 | 0.000 * | 7 | 2 | 0.001 * | 25 | 3 | 0.000 * |
| Positive | 3 | 18 | 3 | 19 | 6 | 37 | |||
| Median follow-up, month (range) | 26 (6–90) | 17 (4–102) | 0.015 * | 12 (7–42) | 14 (4–40) | 0.033 * | 25(6–90) | 14 (4–102) | 0.000 * |
| Variable | Autologous SCT | Allogeneic SCT | Autologous and Allogeneic SCT | |||
|---|---|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Number of previous treatments | - | - | - | 0.626 | - | 0.106 |
| Unifocal or multifocal | - | 0.504 | - | - | - | 0.380 |
| FDG-avid foci occurred in the sites of original disease | - | 0.079 | 19.706 (1.347–288.297) | 0.029 * | 14.849 (2.324–95.469) | 0.004 * |
| DS score | - | - | - | 0.353 | - | 0.361 |
| Integrated CT results | 108.000 (10.243–1138.782) | 0.000 * | 38.741 (3.028–495.745) | 0.005 * | 151.307 (14.646–1563.120) | 0.000 * |
| Status at SCT | - | - | - | - | 54.583 (2.182–1365.641) | 0.015 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, N.; Cai, R.; Deng, S.; Sang, S. Analysis of Positive Results of 18F-FDG PET/CT Imaging after Hematopoietic Stem Cell Transplantation in Lymphoma. Diagnostics 2023, 13, 2027. https://doi.org/10.3390/diagnostics13122027
Dai N, Cai R, Deng S, Sang S. Analysis of Positive Results of 18F-FDG PET/CT Imaging after Hematopoietic Stem Cell Transplantation in Lymphoma. Diagnostics. 2023; 13(12):2027. https://doi.org/10.3390/diagnostics13122027
Chicago/Turabian StyleDai, Na, Rongcui Cai, Shengming Deng, and Shibiao Sang. 2023. "Analysis of Positive Results of 18F-FDG PET/CT Imaging after Hematopoietic Stem Cell Transplantation in Lymphoma" Diagnostics 13, no. 12: 2027. https://doi.org/10.3390/diagnostics13122027
APA StyleDai, N., Cai, R., Deng, S., & Sang, S. (2023). Analysis of Positive Results of 18F-FDG PET/CT Imaging after Hematopoietic Stem Cell Transplantation in Lymphoma. Diagnostics, 13(12), 2027. https://doi.org/10.3390/diagnostics13122027