
Deep Learning-Based Classification and Feature Extraction for Predicting Pathogenesis of Foot Ulcers in Patients with Diabetes


Abstract
1. Introduction
2. Related Works
3. Proposed Work
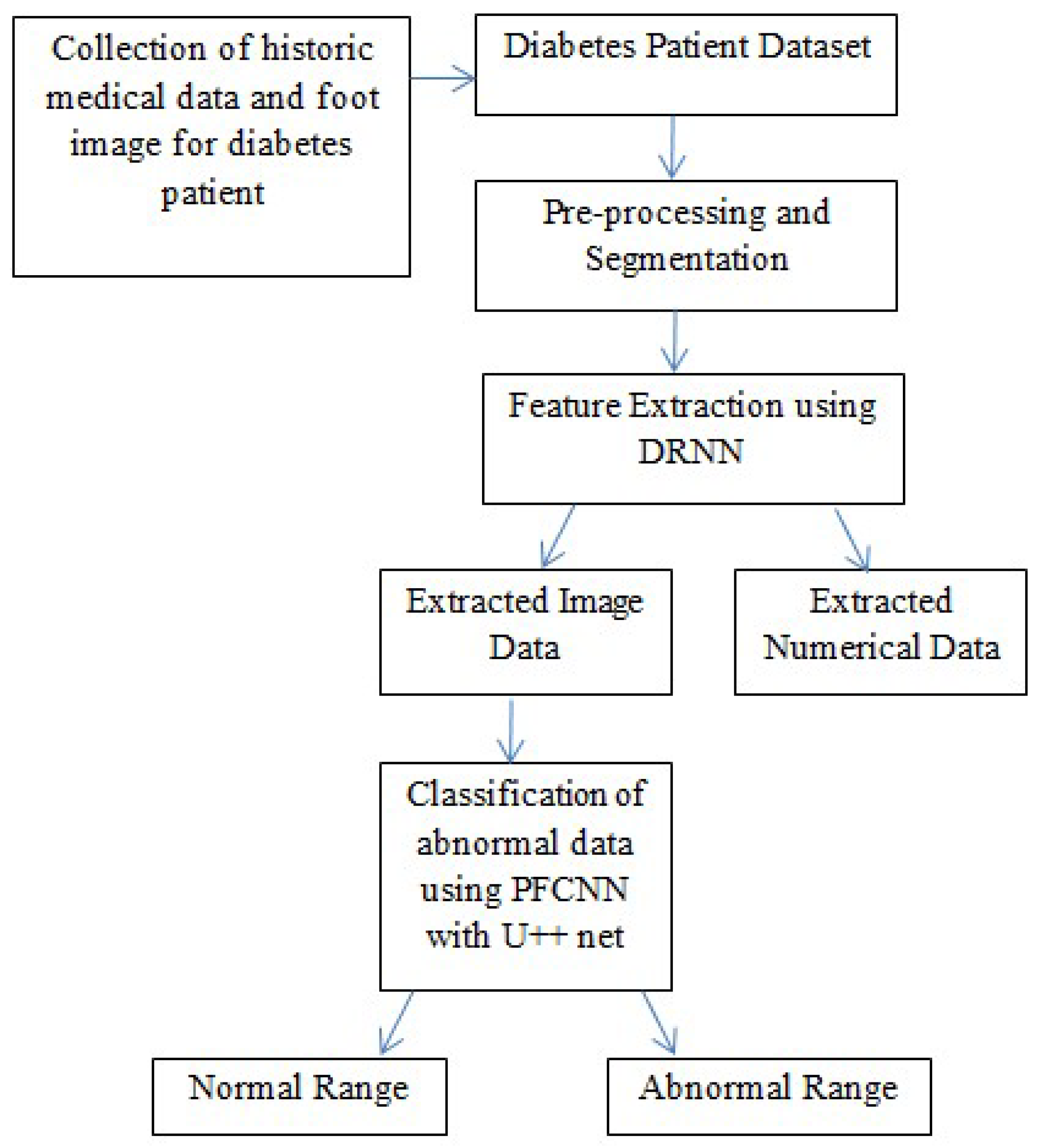
3.1. Architectural Framework
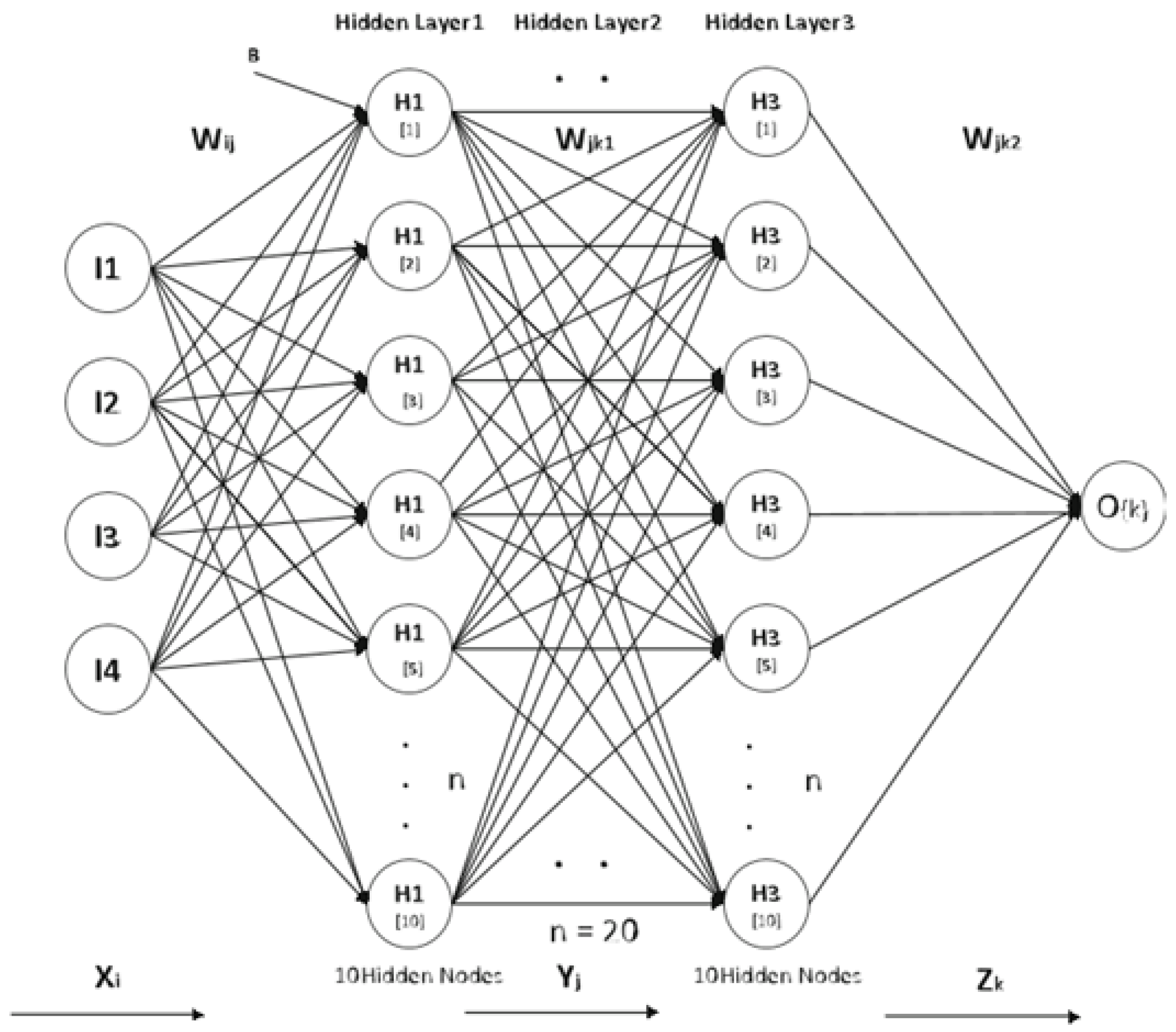
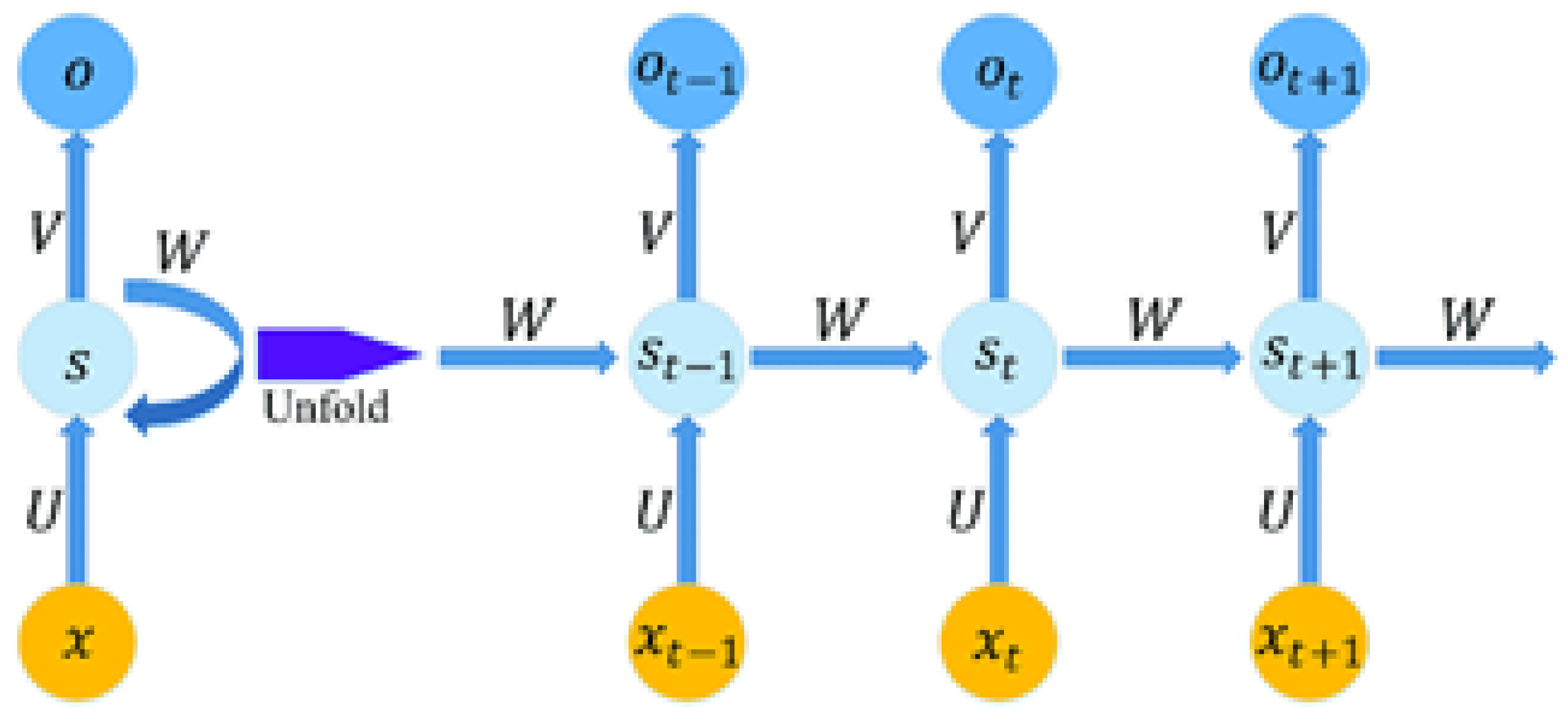
3.2. Feature Extraction Using Deep Recurrent Neural Network (DRNN)
3.3. Inference of CONV Layer in Forward Propagation
3.4. Training the CONV Layer in Backward Propagation
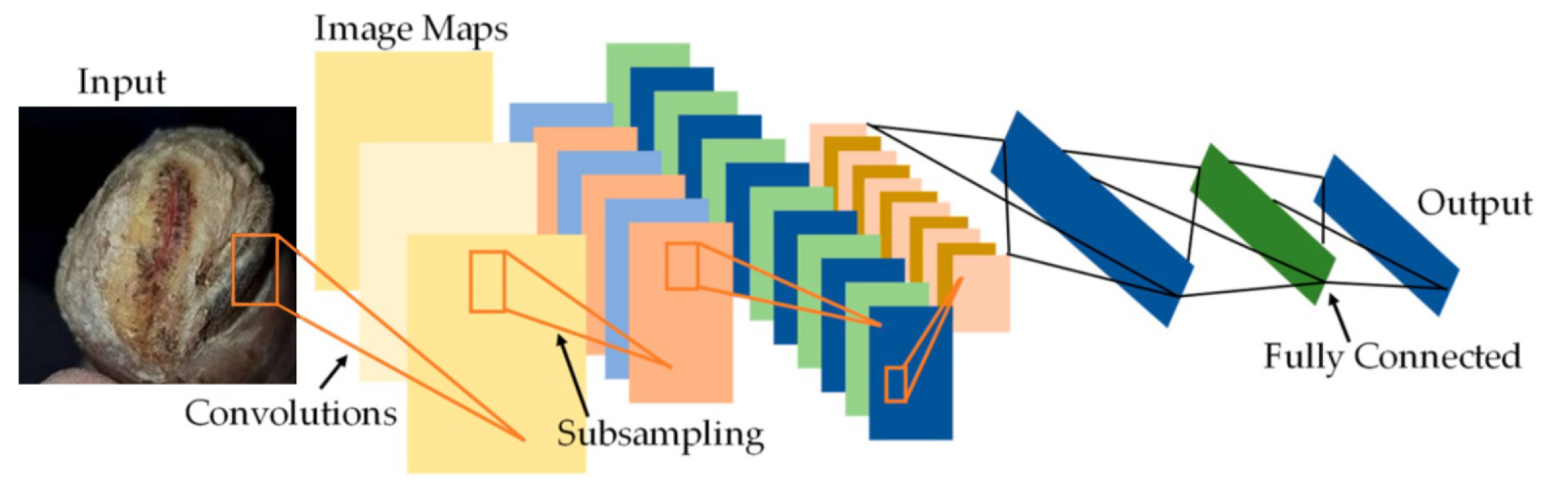
3.5. Pre-Trained Fast Convolution Neural Network (PFCNN) for Classification
4. Training
5. Performance Analysis
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fraiwan, L.; AlKhodari, M.; Ninan, J.; Mustafa, B.; Saleh, A.; Ghazal, M. Diabetic foot ulcer mobile detection system using smart phone thermal camera: A feasibility study. Biomed. Eng. Online 2017, 16, 117. [Google Scholar] [CrossRef] [PubMed]
- Thotad, P.N.; Bharamagoudar, G.R.; Anami, B.S. Diabetic foot ulcer detection using deep learning approaches. Sens. Int. 2023, 4, 100210. [Google Scholar] [CrossRef]
- Ahsan, M.; Naz, S.; Ahmad, R.; Ehsan, H.; Sikandar, A. A deep learning approach for diabetic foot ulcer classification and recognition. Information 2023, 14, 36. [Google Scholar] [CrossRef]
- Purnima, S.; Angelin, P.S.; Priyanka, R.; Subasri, G.; Venkatesh, R. Automated Detection of Diabetic Foot Using Thermal Images by Neural Network Classifiers. Int. J. Emerg. Trends Sci. Technol. 2017, 4, 6. [Google Scholar] [CrossRef]
- Xu, Y.; Han, K.; Zhou, Y.; Wu, J.; Xie, X.; Xiang, W. Classification of diabetic foot ulcers using class knowledge banks. Front. Bioeng. Biotechnol. 2021, 9, 811028. [Google Scholar] [CrossRef] [PubMed]
- Haque, F.; Reaz, M.B.I.; Chowdhury, M.E.H.; Ezeddin, M.; Kiranyaz, S.; Alhatou, M.; Ali, S.H.M.; Bakar, A.A.A.; Srivastava, G. Machine learning-based diabetic neuropathy and previous foot ulceration patients detection using electromyography and ground reaction forces during gait. Sensors 2022, 22, 3507. [Google Scholar] [CrossRef]
- Aiello, E.M.; Toffanin, C.; Messori, M.; Cobelli, C.; Magni, L. Postprandial glucose regulation via KNN meal classification in type 1 diabetes. IEEE Control Syst. Lett. 2018, 3, 230–235. [Google Scholar] [CrossRef]
- Raza, A.; Ayub, H.; Khan, J.A.; Ahmad, I.; Salama, A.S.; Daradkeh, Y.I.; Javeed, D.; Ur Rehman, A.; Hamam, H. A hybrid deep learning-based approach for brain tumor classification. Electronics 2022, 11, 1146. [Google Scholar] [CrossRef]
- Carracedo, J.; Alique, M.; Ramírez-Carracedo, R.; Bodega, G.; Ramírez, R. Endothelial extracellular vesicles produced by senescent cells: Pathophysiological role in the cardiovascular disease associated with all types of diabetes mellitus. Curr. Vasc. Pharmacol. 2019, 17, 447–454. [Google Scholar] [CrossRef]
- Sadiq, M.T.; Yu, X.; Yuan, Z.; Zeming, F.; Rehman, A.U.; Ullah, I.; Li, G.; Xiao, G. Motor imagery EEG signals decoding by multivariate empirical wavelet transform-based framework for robust brain–computer interfaces. IEEE Access 2019, 7, 171431–171451. [Google Scholar] [CrossRef]
- Ahmad, I.; Ullah, I.; Khan, W.U.; Ur Rehman, A.; Adrees, M.S.; Saleem, M.Q.; Cheikhrouhou, O.; Hamam, H.; Shafiq, M. Efficient algorithms for E-healthcare to solve multiobject fuse detection problem. J. Healthc. Eng. 2021, 2021, 9500304. [Google Scholar] [CrossRef]
- Naqvi, R.A.; Arsalan, M.; Rehman, A.; Rehman, A.U.; Loh, W.K.; Paul, A. Deep learning-based drivers emotion classification system in time series data for remote applications. Remote Sens. 2020, 12, 587. [Google Scholar] [CrossRef]
- Sparapani, R.; Dabbouseh, N.M.; Gutterman, D.; Zhang, J.; Chen, H.; Bluemke, D.A.; Joao, A.C.L.; Gregory, L.B.; Soliman, E.Z. Detection of Left Ventricular Hypertrophy Using Bayesian Additive Regression Trees: The MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Heart Assoc. 2019, 8, e009959. [Google Scholar] [CrossRef] [PubMed]
- Sadiq, M.T.; Yu, X.; Yuan, Z.; Fan, Z.; Rehman, A.U.; Li, G.; Xiao, G. Motor imagery EEG signals classification based on mode amplitude and frequency components using empirical wavelet transform. IEEE Access 2019, 7, 127678–127692. [Google Scholar] [CrossRef]
- Jaiswal, V.; Negi, A.; Pal, T. A review on current advances in machine learning based diabetes prediction. Prim. Care Diabetes 2021, 15, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Muthuraja, M.; Shanthi, N. A Survey on Classification of Diabetic Foot Ulcer Using Machine Learning Algorithms. Ann. Rom. Soc. Cell Biol. 2021, 25, 1881–1894. [Google Scholar]
- Cruz-Vega, I.; Gutiérrez-Rodríguez, A.K.; Sánchez-Pérez, H.J.; García-Rodríguez, M.L. Deep learning classification for diabetic foot thermograms. Sensors 2020, 20, 1762. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, P.L.; Rodríguez, R.; Montalvo, N. Automatic Segmentation of Diabetic foot ulcer from Mask Region-Based Convolutional Neural Networks. J. Biomed. Res. Clin. Investig. 2020, 1, 1006. [Google Scholar]
- Maheswari, D.; Kayalvizhi, M. A Hybrid Deep Learning Algorithms for Diabetes Mellitus Prediction Using Thermal Foot Images. Eur. J. Mol. Clin. Med. 2021, 7, 5176–5183. [Google Scholar]
- Islam, M.M.; Ferdousi, R.; Rahman, S.; Bushra, H.Y. Likelihood prediction of diabetes at early stage using data mining techniques. In Computer Vision and Machine Intelligence in Medical Image Analysis; Springer: Berlin/Heidelberg, Germany, 2020; pp. 113–125. [Google Scholar]
- Chaki, J.; Ganesh, S.T.; Cidham, S.K.; Theertan, S.A. Machine learning and artificial intelligence based Diabetes Mellitus detection and self-management: A systematic review. J. King Saud-Univ.-Comput. Inf. Sci. 2020, 34, 3204–3225. [Google Scholar] [CrossRef]
- Abaker, A.A.; Saeed, F.A. A Comparative Analysis of Machine Learning Algorithms to Build a Predictive Model for Detecting Diabetes Complications. Informatica 2021, 45, 1–10. [Google Scholar] [CrossRef]
- Ramsingh, J.; Bhuvaneswari, V. An efficient Map Reduce-Based Hybrid NBC-TFIDF algorithm to mine the public sentiment on diabetes mellitus—A big data approach. J. King Saud-Univ.-Comput. Inf. Sci. 2018, 33, 1018–1029. [Google Scholar] [CrossRef]
- Natarajan, S.; Jain, A.; Krishnan, R.; Rogye, A.; Sivaprasad, S. Diagnostic accuracy of community-based diabetic retinopathy screening with an offline artificial intelligence system on a smartphone. JAMA Ophthalmol. 2019, 137, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Younus, M.; Munna, M.T.A.; Alam, M.M.; Allayear, S.M.; Ara, S.J.F. Prediction model for prevalence of type-2 diabetes mellitus complications using machine learning approach. In Data Management and Analysis; Springer: Berlin/Heidelberg, Germany, 2020; pp. 103–116. [Google Scholar]
- Mainenti, G.; Campanile, L.; Marulli, F.; Ricciardi, C.; Valente, A.S. Machine Learning Approaches for Diabetes Classification: Perspectives to Artificial Intelligence Methods Updating. In Proceedings of the 5th International Conference on Internet of Things, Big Data and Security (IoTBDS 2020), Prague, Czech Republic, 7–9 May 2020. [Google Scholar]
- Mwawado, R.H. Development of a Fast and Accurate Method for the Segmentation of Diabetic Foot Ulcer Images. Ph.D. Thesis, NM-AIST, Arusha, Tanzania, 2020. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer | Params | Activation | Output |
|---|---|---|---|
| Input | |||
| Conv 1 | ReLu | ||
| Max Pool | , stride | ||
| Conv 2 | ReLu | ||
| Max Pool | , stride | ||
| Dense | 256 | ||
| Dense | 2 |
| S.NO | Input Image | Pre-Processing | Segmentation | Classified Output |
|---|---|---|---|---|
| Abnormal Ulcer |  |  |  |  |
 |  |  |  | |
 |  |  |  | |
 |  |  |  | |
| Normal (Healthy skin) |  |  |  |  |
 |  |  |  | |
 |  |  |  | |
 |  |  |  |
| Author | Classification Technique | Feature Extraction Method | Accuracy |
|---|---|---|---|
| Xu Y et al. [5] | Class Knowledge Bank(CKB) | DNN-MLP | 79% |
| Haque et al. [6] | K-Means Clustering | Chi-square, mrmr, Relief Algorithm, FSCNCA | 96% |
| Ahsan et al. [3] | End to end CNN | DFUNet | 98.49% |
| Thotad et al. [2] | EfficientNet | DFUNet | 98.97% |
| Proposed work | Pre-trained Fast Convolution neural network (PFCNN) | Deep recurrent neural network (DRNN) | 99.32% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sathya Preiya, V.; Kumar, V.D.A. Deep Learning-Based Classification and Feature Extraction for Predicting Pathogenesis of Foot Ulcers in Patients with Diabetes. Diagnostics 2023, 13, 1983. https://doi.org/10.3390/diagnostics13121983
Sathya Preiya V, Kumar VDA. Deep Learning-Based Classification and Feature Extraction for Predicting Pathogenesis of Foot Ulcers in Patients with Diabetes. Diagnostics. 2023; 13(12):1983. https://doi.org/10.3390/diagnostics13121983
Chicago/Turabian StyleSathya Preiya, V., and V. D. Ambeth Kumar. 2023. "Deep Learning-Based Classification and Feature Extraction for Predicting Pathogenesis of Foot Ulcers in Patients with Diabetes" Diagnostics 13, no. 12: 1983. https://doi.org/10.3390/diagnostics13121983
APA StyleSathya Preiya, V., & Kumar, V. D. A. (2023). Deep Learning-Based Classification and Feature Extraction for Predicting Pathogenesis of Foot Ulcers in Patients with Diabetes. Diagnostics, 13(12), 1983. https://doi.org/10.3390/diagnostics13121983