
Comparison of Outcomes after Arthroscopic Rotator Cuff Repair between Elderly and Younger Patient Groups: A Systematic Review and Meta-Analysis of Comparative Studies

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment
2.4. Data Extraction
2.5. Data Analysis
3. Results
3.1. Included Studies
3.2. Study Characteristics
3.3. Details of Surgery
3.4. Study Quality
3.5. Primary Outcome
3.5.1. Pain Reduction
3.5.2. Function Improvement One Year after Surgery
- Patients ≥ 70 years of age versus patients < 70 years of age.
- Patients ≥ 65 years of age versus patients < 65 years of age.
3.6. Secondary Outcomes
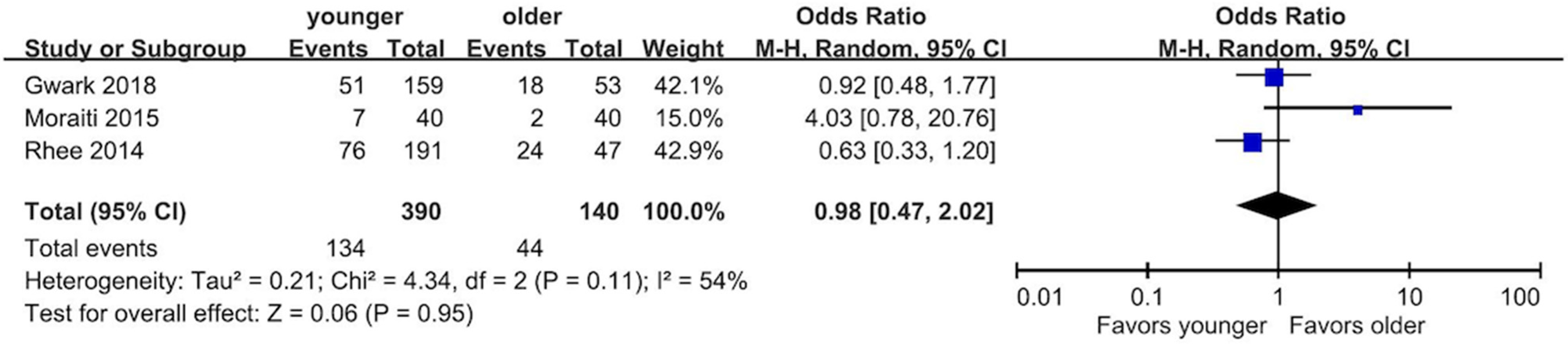
3.6.1. Re-Tear Rate
- Patients ≥ 70 years old versus patients < 70 years old.
- Patients ≥ 65 years old versus patients < 65 years old.
3.6.2. Abduction Muscle Power
- Patients ≥ 70 years old versus patients < 70 years old.
- Patients ≥ 65 years old versus patients < 65 years old.
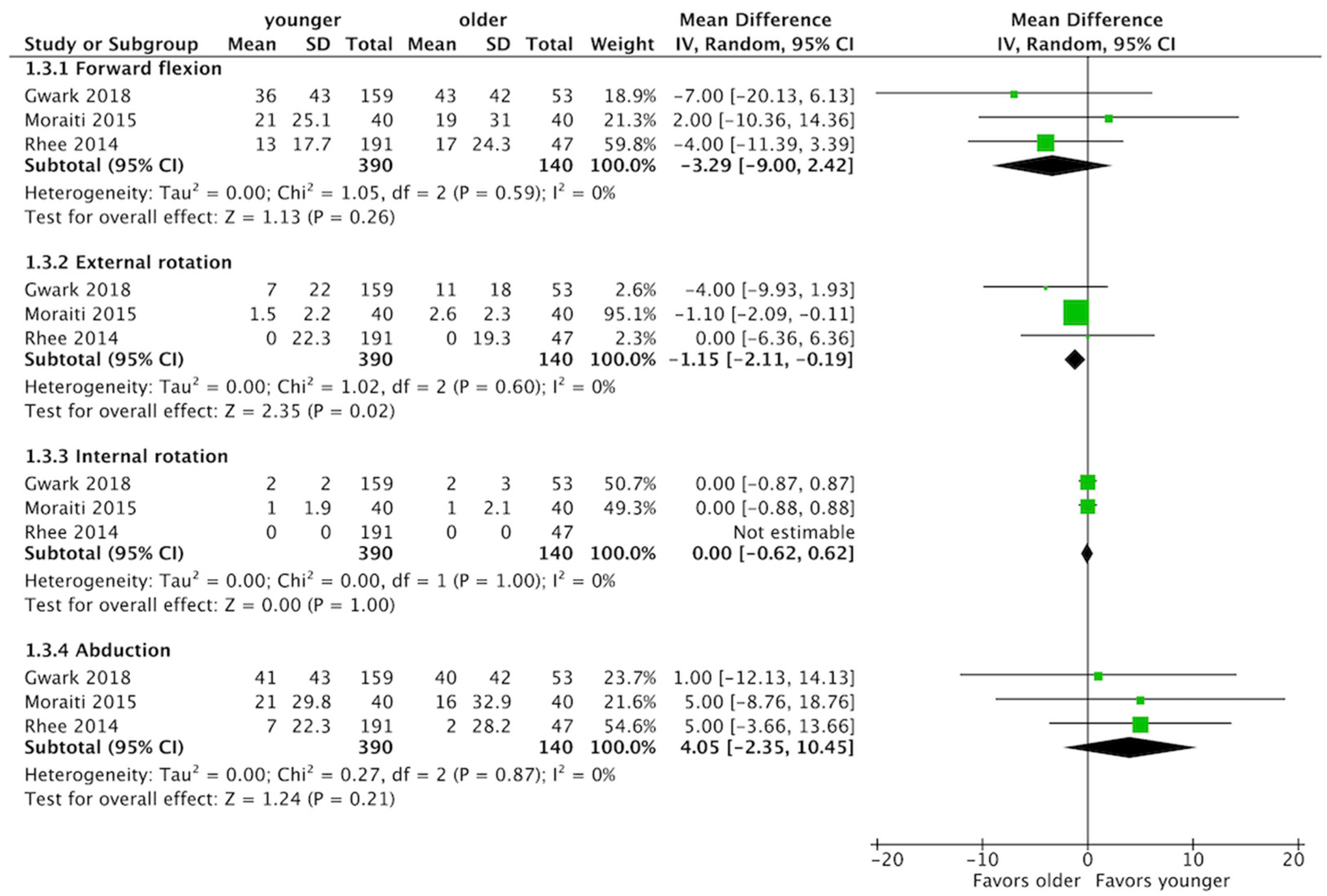
3.6.3. Shoulder Range of Motion Improvement
- Patients ≥ 70 years old versus patients < 70 years old.
- Patients ≥ 65 years old versus patients < 65 years old.
3.6.4. Quality of Life
3.6.5. Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sambandam, S.N.; Khanna, V.; Gul, A.; Mounasamy, V. Rotator cuff tears: An evidence based approach. World J. Orthop. 2015, 6, 902–918. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.R.; Cha, P.S.; Devana, S.K.; Ishmael, C.; Di Pauli von Treuheim, T.; D’Oro, A.; Wang, J.C.; McAllister, D.R.; Petrigliano, F.A. Evaluation of the Trends, Concomitant Procedures, and Complications With Open and Arthroscopic Rotator Cuff Repairs in the Medicare Population. Orthop. J. Sports Med. 2017, 5, 2325967117731310. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.; Cooper, C.; Campbell, M.K.; Rees, J.; Moser, J.; Beard, D.J.; Fitzpatrick, R.; Gray, A.; Dawson, J.; Murphy, J.; et al. Effectiveness of open and arthroscopic rotator cuff repair (UKUFF): A randomised controlled trial. Bone Jt. J. 2017, 99, 107–115. [Google Scholar] [CrossRef]
- Chung, S.W.; Oh, J.H.; Gong, H.S.; Kim, J.Y.; Kim, S.H. Factors affecting rotator cuff healing after arthroscopic repair: Osteoporosis as one of the independent risk factors. Am. J. Sports Med. 2011, 39, 2099–2107. [Google Scholar] [CrossRef] [PubMed]
- Maher, A.; Leigh, W.; Young, S.; Caughey, W.; Hoffman, T.; Brick, M.; Caughey, M. Do Age, Demographics, and Tear Characteristics Affect Outcomes After Rotator Cuff Repair? Results of Over 2000 Rotator Cuff Repairs at 5-Year Follow-up. Orthop. J. Sports Med. 2022, 10, 23259671221119222. [Google Scholar] [CrossRef] [PubMed]
- Robinson, P.M.; Wilson, J.; Dalal, S.; Parker, R.A.; Norburn, P.; Roy, B.R. Rotator cuff repair in patients over 70 years of age: Early outcomes and risk factors associated with re-tear. Bone Jt. J. 2013, 95, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Nolte, P.-C.; Seiter, M.; Elrick, B.P.; Millett, P.J. Rotator cuff tears in elderly patients: Is repair worthwhile? Ann. Jt. 2021, 6, 20. [Google Scholar] [CrossRef]
- Ainsworth, R.; Lewis, J.S. Exercise therapy for the conservative management of full thickness tears of the rotator cuff: A systematic review. Br. J. Sports Med. 2007, 41, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Lambers Heerspink, F.O.; van Raay, J.J.; Koorevaar, R.C.; van Eerden, P.J.; Westerbeek, R.E.; van ’t Riet, E.; van den Akker-Scheek, I.; Diercks, R.L. Comparing surgical repair with conservative treatment for degenerative rotator cuff tears: A randomized controlled trial. J. Shoulder Elb. Surg. 2015, 24, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Kukkonen, J.; Joukainen, A.; Lehtinen, J.; Mattila, K.T.; Tuominen, E.K.J.; Kauko, T.; Aärimaa, V. Treatment of non-traumatic rotator cuff tears: A randomised controlled trial with one-year clinical results. Bone Jt. J. 2014, 96, 75–81. [Google Scholar] [CrossRef]
- Geary, M.B.; Elfar, J.C. Rotator Cuff Tears in the Elderly Patients. Geriatr. Orthop. Surg. Rehabil. 2015, 6, 220–224. [Google Scholar] [CrossRef]
- Drake, G.N.; O’Connor, D.P.; Edwards, T.B. Indications for reverse total shoulder arthroplasty in rotator cuff disease. Clin. Orthop. Relat. Res. 2010, 468, 1526–1533. [Google Scholar] [CrossRef] [PubMed]
- Labriola, J.E.; Edwards, T.B. Reverse Total Shoulder Arthroplasty in the Senior Athlete. Oper. Tech. Sports Med. 2008, 16, 43–49. [Google Scholar] [CrossRef]
- Kennedy, J.; Klifto, C.S.; Ledbetter, L.; Bullock, G.S. Reverse total shoulder arthroplasty clinical and patient-reported outcomes and complications stratified by preoperative diagnosis: A systematic review. J. Shoulder Elb. Surg. 2021, 30, 929–941. [Google Scholar] [CrossRef]
- Dornan, G.J.; Katthagen, J.C.; Tahal, D.S.; Petri, M.; Greenspoon, J.A.; Denard, P.J.; Burkhart, S.S.; Millett, P.J. Cost-Effectiveness of Arthroscopic Rotator Cuff Repair Versus Reverse Total Shoulder Arthroplasty for the Treatment of Massive Rotator Cuff Tears in Patients With Pseudoparalysis and Nonarthritic Shoulders. Arthroscopy 2017, 33, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Walch, G.; Bacle, G.; Lädermann, A.; Nové-Josserand, L.; Smithers, C.J. Do the indications, results, and complications of reverse shoulder arthroplasty change with surgeon’s experience? J. Shoulder Elb. Surg. 2012, 21, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, B.M.; Chalmers, P.N.; Gupta, A.K.; Romeo, A.A.; Nicholson, G.P. Complication rates comparing primary with revision reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2014, 23, 1647–1654. [Google Scholar] [CrossRef]
- Wall, B.; Nové-Josserand, L.; O’Connor, D.P.; Edwards, T.B.; Walch, G. Reverse total shoulder arthroplasty: A review of results according to etiology. J. Bone Jt. Surg. 2007, 89, 1476–1485. [Google Scholar] [CrossRef]
- Sheean, A.J.; Hartzler, R.U.; Denard, P.J.; Lädermann, A.; Sanders, T.G.; Zlatkin, M.B.; Burkhart, S.S. Preoperative Radiographic Risk Factors for Incomplete Arthroscopic Supraspinatus Tendon Repair in Massive Rotator Cuff Tears. Arthroscopy 2018, 34, 1121–1127. [Google Scholar] [CrossRef]
- Moraiti, C.; Valle, P.; Maqdes, A.; Boughebri, O.; Dib, C.; Giakas, G.; Kany, J.; Elkholti, K.; Garret, J.; Katz, D.; et al. Comparison of functional gains after arthroscopic rotator cuff repair in patients over 70 years of age versus patients under 50 years of age: A prospective multicenter study. Arthroscopy 2015, 31, 184–190. [Google Scholar] [CrossRef]
- Brewer, B.J. Aging of the rotator cuff. Am. J. Sports Med. 1979, 7, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Diebold, G.; Lam, P.; Walton, J.; Murrell, G.A.C. Relationship Between Age and Rotator Cuff Retear: A Study of 1,600 Consecutive Rotator Cuff Repairs. J. Bone Jt. Surg. 2017, 99, 1198–1205. [Google Scholar] [CrossRef]
- Bhatia, S.; Greenspoon, J.A.; Horan, M.P.; Warth, R.J.; Millett, P.J. Two-Year Outcomes After Arthroscopic Rotator Cuff Repair in Recreational Athletes Older Than 70 Years. Am. J. Sports Med. 2015, 43, 1737–1742. [Google Scholar] [CrossRef]
- Worland, R.L.; Arredondo, J.; Angles, F.; Lopez-Jimenez, F. Repair of massive rotator cuff tears in patients older than 70 years. J. Shoulder Elb. Surg. 1999, 8, 26–30. [Google Scholar] [CrossRef]
- Denard, P.J.; Lädermann, A.; Brady, P.C.; Narbona, P.; Adams, C.R.; Arrigoni, P.; Huberty, D.; Zlatkin, M.B.; Sanders, T.G.; Burkhart, S.S. Pseudoparalysis From a Massive Rotator Cuff Tear Is Reliably Reversed With an Arthroscopic Rotator Cuff Repair in Patients Without Preoperative Glenohumeral Arthritis. Am. J. Sports Med. 2015, 43, 2373–2378. [Google Scholar] [CrossRef] [PubMed]
- Charousset, C.; Bellaïche, L.; Kalra, K.; Petrover, D. Arthroscopic repair of full-thickness rotator cuff tears: Is there tendon healing in patients aged 65 years or older? Arthroscopy 2010, 26, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Verma, N.N.; Bhatia, S.; Baker, C.L., 3rd; Cole, B.J.; Boniquit, N.; Nicholson, G.P.; Romeo, A.A. Outcomes of arthroscopic rotator cuff repair in patients aged 70 years or older. Arthroscopy 2010, 26, 1273–1280. [Google Scholar] [CrossRef]
- Fossati, C.; Stoppani, C.; Menon, A.; Pierannunzii, L.; Compagnoni, R.; Randelli, P.S. Arthroscopic rotator cuff repair in patients over 70 years of age: A systematic review. J. Orthop. Traumatol. 2021, 22, 3. [Google Scholar] [CrossRef]
- Altintas, B.; Anderson, N.L.; Pitta, R.; Buckley, P.S.; Bhatia, S.; Provencher, M.T.; Millett, P.J. Repair of Rotator Cuff Tears in the Elderly: Does It Make Sense? A Systematic Review. Am. J. Sports Med. 2020, 48, 744–753. [Google Scholar] [CrossRef]
- Gwark, J.-Y.; Sung, C.-M.; Na, J.-B.; Park, H.B. Outcomes of Arthroscopic Rotator Cuff Repair in Patients Who Are 70 Years of Age or Older Versus Under 70 Years of Age: A Sex- and Tear Size-Matched Case-Control Study. Arthroscopy 2018, 34, 2045–2053. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Wells, G.; Shea, B.; O’connell, D.; Peterson, J.; Welch; Losos, M.; Tugwell, P.; Ga, S.W.; Zello, G.A.; Petersen, J. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 January 2023).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.A.; Searle, H.K.C.; MacDonald, D.; McBirnie, J. Cost-effectiveness and satisfaction following arthroscopic rotator cuff repair: Does age matter? Bone Jt. J. 2019, 101, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Osti, L.; Papalia, R.; Del Buono, A.; Denaro, V.; Maffulli, N. Comparison of arthroscopic rotator cuff repair in healthy patients over and under 65 years of age. Knee Surg. Sport. Traumatol. Arthrosc. 2010, 18, 1700–1706. [Google Scholar] [CrossRef] [PubMed]
- Rhee, Y.G.; Cho, N.S.; Yoo, J.H. Clinical outcome and repair integrity after rotator cuff repair in patients older than 70 years versus patients younger than 70 years. Arthroscopy 2014, 30, 546–554. [Google Scholar] [CrossRef]
- DeOrio, J.; Cofield, R.H. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J. Bone Jt. Surg. 1984, 66, 563–567. [Google Scholar] [CrossRef]
- Goutallier, D.; Postel, J.M.; Bernageau, J.; Lavau, L.; Voisin, M.C. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Witney-Lagen, C.; Mazis, G.; Bruguera, J.; Atoun, E.; Sforza, G.; Levy, O. Do elderly patients gain as much benefit from arthroscopic rotator cuff repair as their younger peers? J. Shoulder Elb. Surg. 2019, 28, 1056–1065. [Google Scholar] [CrossRef]
- Kukkonen, J.; Kauko, T.; Vahlberg, T.; Joukainen, A.; Aärimaa, V. Investigating minimal clinically important difference for Constant score in patients undergoing rotator cuff surgery. J. Shoulder Elb. Surg. 2013, 22, 1650–1655. [Google Scholar] [CrossRef]
- Hsu, J.E.; Horneff, J.G.; Gee, A.O. Immobilization After Rotator Cuff Repair: What Evidence Do We Have Now? Orthop. Clin. N. Am. 2016, 47, 169–177. [Google Scholar] [CrossRef]
- Keener, J.D.; Galatz, L.M.; Stobbs-Cucchi, G.; Patton, R.; Yamaguchi, K. Rehabilitation following arthroscopic rotator cuff repair: A prospective randomized trial of immobilization compared with early motion. J. Bone Jt. Surg. 2014, 96, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.H.; Lim, T.K.; Shon, M.S.; Park, Y.E.; Lee, S.W.; Yoo, J.C. Effect of immobilization without passive exercise after rotator cuff repair: Randomized clinical trial comparing four and eight weeks of immobilization. J. Bone Jt. Surg. 2014, 96, e44. [Google Scholar] [CrossRef] [PubMed]
- Houck, D.A.; Kraeutler, M.J.; Schuette, H.B.; McCarty, E.C.; Bravman, J.T. Early Versus Delayed Motion After Rotator Cuff Repair: A Systematic Review of Overlapping Meta-analyses. Am. J. Sports Med. 2017, 45, 2911–2915. [Google Scholar] [CrossRef] [PubMed]
- Severud, E.L.; Ruotolo, C.; Abbott, D.D.; Nottage, W.M. All-arthroscopic versus mini-open rotator cuff repair: A long-term retrospective outcome comparison. Arthroscopy 2003, 19, 234–238. [Google Scholar] [CrossRef]
- Bayle, X.; Pham, T.T.; Faruch, M.; Gobet, A.; Mansat, P.; Bonnevialle, N. No difference in outcome for open versus arthroscopic rotator cuff repair: A prospective comparative trial. Arch. Orthop. Trauma Surg. 2017, 137, 1707–1712. [Google Scholar] [CrossRef]
- Nazari, G.; MacDermid, J.C.; Bryant, D.; Dewan, N.; Athwal, G.S. Effects of arthroscopic vs. mini-open rotator cuff repair on function, pain & range of motion. A systematic review and meta-analysis. PLoS ONE 2019, 14, e0222953. [Google Scholar] [CrossRef]
- Xu, C.; Zhao, J.; Li, D. Meta-analysis comparing single-row and double-row repair techniques in the arthroscopic treatment of rotator cuff tears. J. Shoulder Elb. Surg. 2014, 23, 182–188. [Google Scholar] [CrossRef]
- Sobhy, M.H.; Khater, A.H.; Hassan, M.R.; El Shazly, O. Do functional outcomes and cuff integrity correlate after single-versus double-row rotator cuff repair? A systematic review and meta-analysis study. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 593–605. [Google Scholar] [CrossRef]
- Hein, J.; Reilly, J.M.; Chae, J.; Maerz, T.; Anderson, K. Retear Rates After Arthroscopic Single-Row, Double-Row, and Suture Bridge Rotator Cuff Repair at a Minimum of 1 Year of Imaging Follow-up: A Systematic Review. Arthroscopy 2015, 31, 2274–2281. [Google Scholar] [CrossRef]
- Plachel, F.; Siegert, P.; Rüttershoff, K.; Thiele, K.; Akgün, D.; Moroder, P.; Scheibel, M.; Gerhardt, C. Long-term Results of Arthroscopic Rotator Cuff Repair: A Follow-up Study Comparing Single-Row Versus Double-Row Fixation Techniques. Am. J. Sport. Med. 2020, 48, 1568–1574. [Google Scholar] [CrossRef]
- Ying, Z.-M.; Lin, T.; Yan, S.-G. Arthroscopic single-row versus double-row technique for repairing rotator cuff tears: A systematic review and meta-analysis. Orthop. Surg. 2014, 6, 300–312. [Google Scholar] [CrossRef] [PubMed]
- van Deurzen, D.F.P.; Auw Yang, K.G.; Onstenk, R.; Raven, E.E.J.; van den Borne, M.P.J.; Hoelen, M.A.; Wessel, R.N.; Willigenburg, N.W.; Klaassen, A.D.; van den Bekerom, M.P.J.; et al. Long Head of Biceps Tenotomy Is Not Inferior to Suprapectoral Tenodesis in Arthroscopic Repair of Nontraumatic Rotator Cuff Tears: A Multicenter, Non-inferiority, Randomized, Controlled Clinical Trial. Arthroscopy 2021, 37, 1767–1776.e1. [Google Scholar] [CrossRef] [PubMed]
- Woodmass, J.M.; Al Khatib, L.; McRae, S.; Lapner, P.; Mascarenhas, R.; Neogi, D.; MacDonald, P.B. Arthroscopic Rotator Cuff Repair with and without Acromioplasty in the Treatment of Full-Thickness Rotator Cuff Tears: Long-Term Outcomes of a Multicenter, Randomized Controlled Trial. J. Bone Jt. Surg. 2022, 104, 2101–2107. [Google Scholar] [CrossRef]
- Yoo, J.C.; Ahn, J.H.; Koh, K.H.; Lim, K.S. Rotator cuff integrity after arthroscopic repair for large tears with less-than-optimal footprint coverage. Arthroscopy 2009, 25, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.B.; Jeong, J.Y.; Kim, J.S.; Yoo, J.C. Evaluation of risk factors for irreparable rotator cuff tear in patients older than age 70 including evaluation of radiologic factors of the shoulder. J. Shoulder Elb. Surg. 2018, 27, 1932–1938. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year) | Country | Study Design, LOE | Inclusion/Exclusion Criteria | Sample Size (M/F) | Outcomes | NOS | Funding |
|---|---|---|---|---|---|---|---|
| Osti, 2010 [36] | Italy | Retrospective cohort, II | Inclusion: FTRCT with cuff repair surgery Exclusion: Advanced rotator cuff arthropathy (Hamada Grade 3–5), severe fatty infiltration (Goutallier stage 3 or 4), subscapularis tear, fracture, instability, previous surgery, etc. | Age > 65: 28 (19/9) Age < 65: 28 (19/9) | Function (UCLA score), shoulder ROM, QoL (SF-36) | 7 | NR |
| Rhee, 2014 [37] | Korea | Retrospective cohort, II | Inclusion: FTRCT with ARCR surgery Exclusion: AC joint OA requiring resection, advanced GH OA, biceps lesion, revision surgery | Age > 70: 47 (14/33) Age < 70: 191 (74/117) | Function (Constant score, UCLA score), re-tear rate, shoulder ROM, pain level (VAS), muscle strength | 7 | NR |
| Moraiti, 2015 [20] | France/ Greece | Prospective cohort, II | Inclusion: FTRCT with ARCR surgery Exclusion: Previous trauma or surgery, advanced GH joint OA | Age > 70: 41 Age < 70: 40 | Function (Constant score), re-tear rate, shoulder ROM | 7 | NR |
| Gwark, 2018 [30] | Korea | Retrospective case–control, III | Inclusion: FTRCT with ARCR surgery Exclusion: previous trauma history | Age > 70: 53 (19/34) Age < 70: 159 (57/102) | Function (Constant score), re-tear rate, shoulder ROM, pain level (VAS), muscle strength | 7 | NR |
| Nicolson, 2019 [35] | United Kingdom | Prospective case–control, III | Inclusion: FTRCT with ARCR surgery Exclusion: Previous Injury, revision surgery, partial tear, unable to complete repair | Age > 65: 28 (17/11) Age < 65: 56 (28/28) | Function (DASH score, OSS score), QoL (EQ-5D), re-tear rate | 7 | Yes |
| Study | Group | Tear size a (I/II/III or Small Medium/Large/Massive) | Fatty Infiltration b | Repair Method (SR/DR or TOE) |
|---|---|---|---|---|
| Osti, 2010 [36] | Age > 65 | 3/15/10 | SSP (18/10) c ISP (23/5) SSC (24/4) | All single row |
| Age < 65 | 5/16/7 | SSP (19/9) ISP (25/3) SSC (25/3) | ||
| Rhee, 2014 [37] | Age > 70 | 22/9/16 | NR | 27/15 |
| Age < 70 | 85/68/38 | 101/65 | ||
| Moraiti, 2015 [20] | Age > 70 | NR | SSP 1.9 ± 0.1 ISP 1.6 ± 0.2 SSC 1.6 ± 0.2 | 22/18 |
| Age < 70 | SSP 0.8 ± 0.1 ISP 1.0 ± 0.3 SSC 0.75 ± 0.3 | 15/25 | ||
| Gwark, 2018 [30] | Age > 70 | 22/15/16 | GFDI d 1.6 ± 0.3 ISP 2.2 ± 0.7 | 38/15 |
| Age < 70 | 66/45/48 | GFDI 1.7 ± 0.5 ISP 2.0 ± 0.8 | 118/41 | |
| Nicholson, 2019 [35] | Age > 65 | 9/19 large or massive | NR | All double row |
| Age < 65 | 23/33 large or massive |
| Outcomes | No. of Studies, n | Patients in Younger Group, n | Patients in Older Group, n | OR/MD (95% CI) | p | I2 |
|---|---|---|---|---|---|---|
| Pain level (VAS) improvement | 2 | 350 | 100 | −0.33 (−0.80, 0.15) | 0.18 | 0% |
| Constant score improvement | 3 | 390 | 140 | −0.30 (−2.84, 2.24) | 0.82 | 0% |
| Re-tear rate | 3 | 390 | 140 | 0.98 (0.47, 2.02) | 0.95 | 54% |
| Muscle power | 2 | 350 | 100 | 0.31 (−0.13, 0.75) | 0.17 | 0% |
| Joint ROM improvement | ||||||
| Forward flexion | 3 | 390 | 140 | −3.29 (−9.00, 2.42) | 0.26 | 0% |
| External rotation | 3 | 390 | 140 | −1.15 (−2.11, −0.19) | 0.02 | 0% |
| Abduction | 3 | 390 | 140 | 4.05 (−2.35, 10.45) | 0.21 | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, Y.-C.; Kuo, L.-T.; Hsu, W.-H.; Tsai, Y.-H.; Peng, K.-T. Comparison of Outcomes after Arthroscopic Rotator Cuff Repair between Elderly and Younger Patient Groups: A Systematic Review and Meta-Analysis of Comparative Studies. Diagnostics 2023, 13, 1770. https://doi.org/10.3390/diagnostics13101770
Hsieh Y-C, Kuo L-T, Hsu W-H, Tsai Y-H, Peng K-T. Comparison of Outcomes after Arthroscopic Rotator Cuff Repair between Elderly and Younger Patient Groups: A Systematic Review and Meta-Analysis of Comparative Studies. Diagnostics. 2023; 13(10):1770. https://doi.org/10.3390/diagnostics13101770
Chicago/Turabian StyleHsieh, Yu-Chieh, Liang-Tseng Kuo, Wei-Hsiu Hsu, Yao-Hung Tsai, and Kuo-Ti Peng. 2023. "Comparison of Outcomes after Arthroscopic Rotator Cuff Repair between Elderly and Younger Patient Groups: A Systematic Review and Meta-Analysis of Comparative Studies" Diagnostics 13, no. 10: 1770. https://doi.org/10.3390/diagnostics13101770
APA StyleHsieh, Y.-C., Kuo, L.-T., Hsu, W.-H., Tsai, Y.-H., & Peng, K.-T. (2023). Comparison of Outcomes after Arthroscopic Rotator Cuff Repair between Elderly and Younger Patient Groups: A Systematic Review and Meta-Analysis of Comparative Studies. Diagnostics, 13(10), 1770. https://doi.org/10.3390/diagnostics13101770