1. Introduction
Different imaging techniques, such as magnetic resonance imaging (MRI) [
1,
2] and computerized tomography scanning (CTS) [
3], are used to measure different parameters to assess musculoskeletal structures.
Being more expensive, these methods are considered unsuitable for managing some pathological conditions and not practical for large-scale studies. Nowadays, musculoskeletal ultrasound (US) imaging, being a readily accessible, cost-effective, and reliable imaging method, has increased its field of action in rehabilitation medicine [
4]. Playing an important role as pain generators in numerous musculoskeletal injuries, the thickness of various anatomical structures such as tendons, ligaments, and muscles are measured and monitored [
5,
6,
7,
8]. Moreover, knowing the size and thickness of these structures is important for specialists managing patients with different musculoskeletal injuries [
7,
8,
9,
10,
11,
12].
The reliability of US imaging for measuring these structures has also been assessed in various other studies [
7,
8,
9,
10,
13]. While there have been numerous investigations on the different musculoskeletal structures, fascial layers have not been studied in the upper limb except in two studies about the thickness of deep and superficial fascia in the arm and forearm [
14,
15]. The thickness of tendons, ligaments, and muscles has been reported, but the complex system of the fascia that covers the muscles and organizes the subcutaneous tissue has not been assessed.
We know from histological studies [
16] that the fasciae of the upper limb are composed of superficial fascia inside the subcutaneous tissue and deep fascia that envelop the muscles, as in other topographical regions [
14,
15,
17]. Numerous studies have reported the crucial role of deep fascia thickness knowledge in the management of regional anesthesiology for fascia plane, inter-fascial, and nerve blocks, reducing the risk of nerve damage [
14,
18]. Other studies have confirmed the importance of deep fascia thickness in the acute compartment syndrome in the upper limb [
14,
19]. Moreover, many studies in recent years have highlighted in plastic and reconstructive surgery how knowing the exact thickness of a patient’s superficial fascia and predicting the seal of it will reduce damage while making a flap [
14,
15,
20].
Some studies investigating the value of the US assessment of fasciae in other areas have demonstrated the efficacious evaluation of deep fascia thickness [
17,
21] and measurements of the thickness of superficial fascia and of subcutaneous tissue at a lower cost than other non-invasive methods [
22,
23]. Furthermore, although US imaging appears to be the best type of imaging for studying and assessing fasciae, standard reference values and their appearance on scans have not been entirely clarified. To date, some studies have examined different types of fasciae by US imaging, reporting reliable results in US fasciae thickness assessments [
17,
21,
22,
23]. Pirri et al. [
23] demonstrated that expertise in US imaging and expertise in identifying anatomical landmarks from a fascial point of view are fundamental for reliable results, pointing out possible sources of error that lie in measurements or interpretation errors linked to the US technique, including difficulty in identifying anatomical landmarks during the US exam [
23]. In addition, a known obstacle in ultrasound imaging is obtaining exact US images. Nevertheless, despite rigorous efforts and extensive previous training, there may be measurement inaccuracies by distortions that could influence the measurements, as demonstrated for other anatomical structures [
24]. Furthermore, the experience level of the raters, especially in these types of assessments, must be considered a possible cause of error in the evaluation of fasciae thickness [
23]. Finally, in CT and MRI, the measurements are based on an identical data set, whereas in US imaging, the measurements of the different raters are based on different images that they acquire themselves. However, only a few studies have focused on inter-rater reliability [
23,
25] between raters with different levels of experience in fascial anatomy.
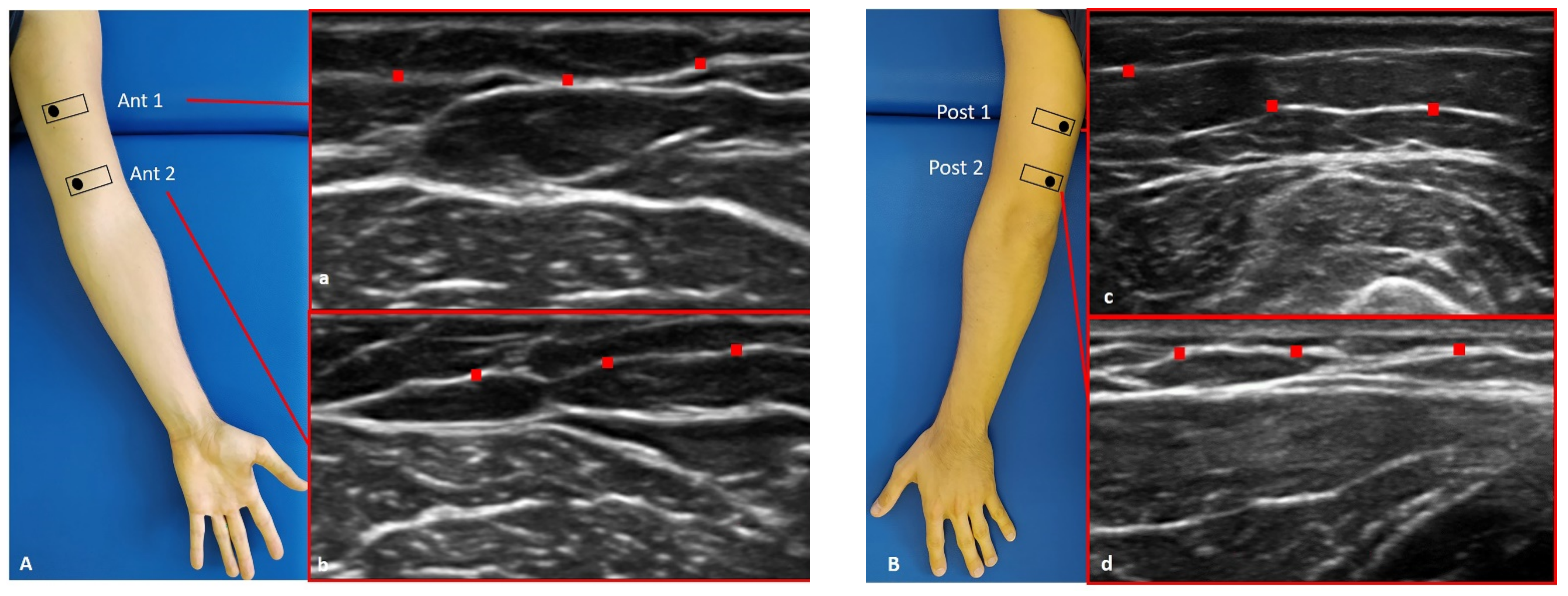
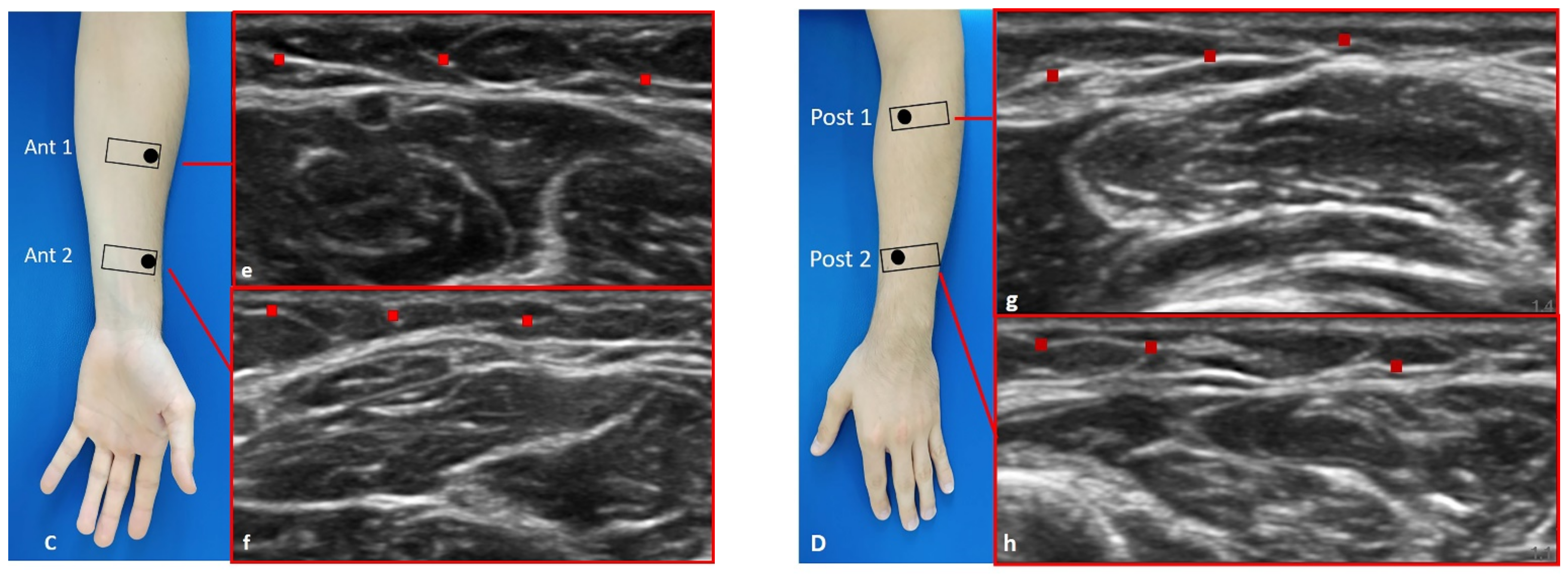
The current study sets out to assess the inter-reliability of US thickness measurements of superficial and deep fasciae in the upper limb of healthy volunteers between raters with different levels of experience in the sono-anatomy of fasciae (an expert and a novice), performing the evaluations at different times on the same US images taken by the expert rater to eliminate error in the acquisition of the images.
4. Discussion
To our current knowledge, this study may be stated as the first study detailing the intra- and inter-reliability of US measurements of fascial thickness in the arm and forearm. The primary aim of this study is to assess the inter-reliability of US measurements of superficial and deep fascia thicknesses in the arm and forearm. Two raters with different backgrounds and levels of expertise assessed the US images and measured the US superficial and deep fascia thicknesses of the arms and forearms of 30 healthy volunteers.
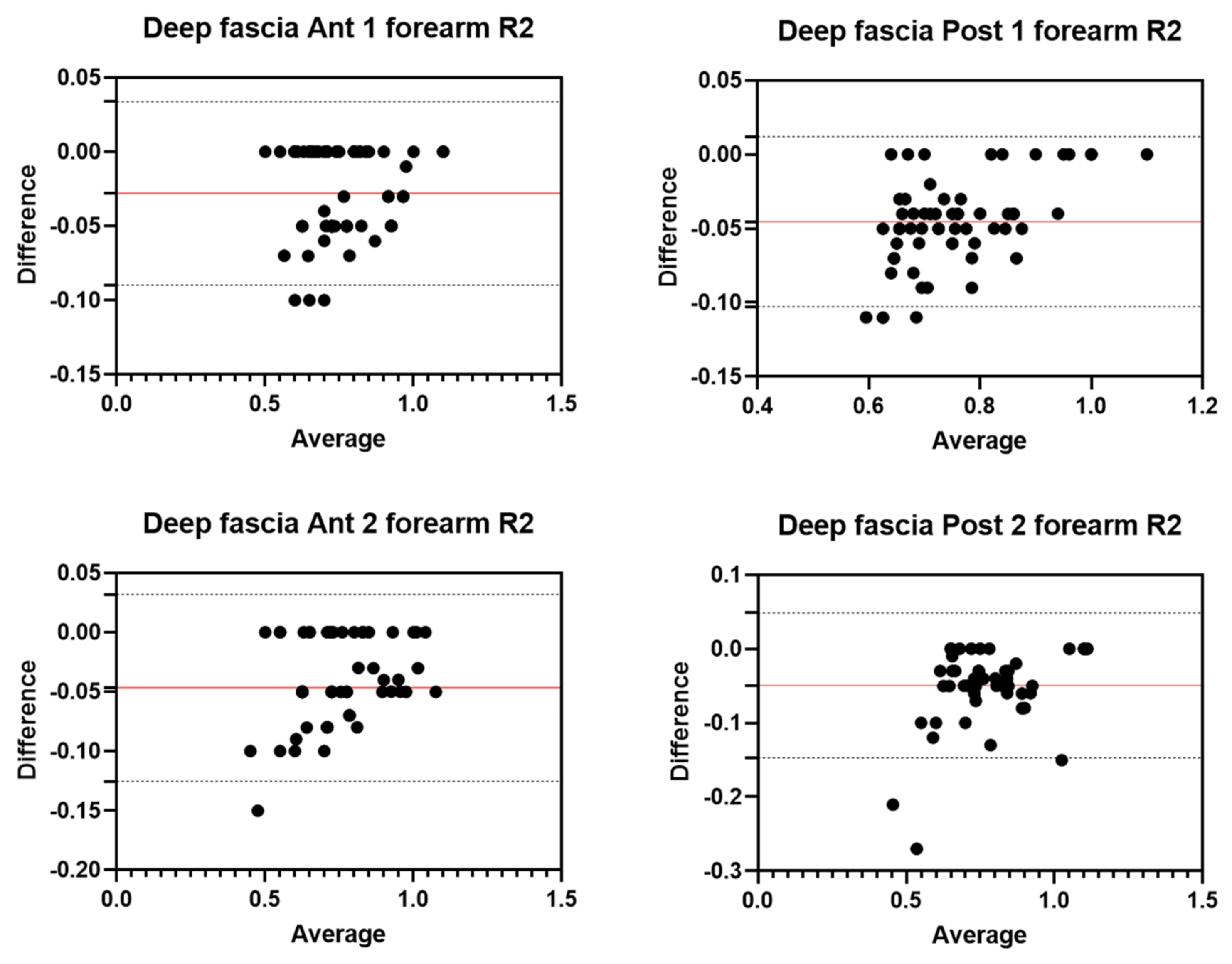
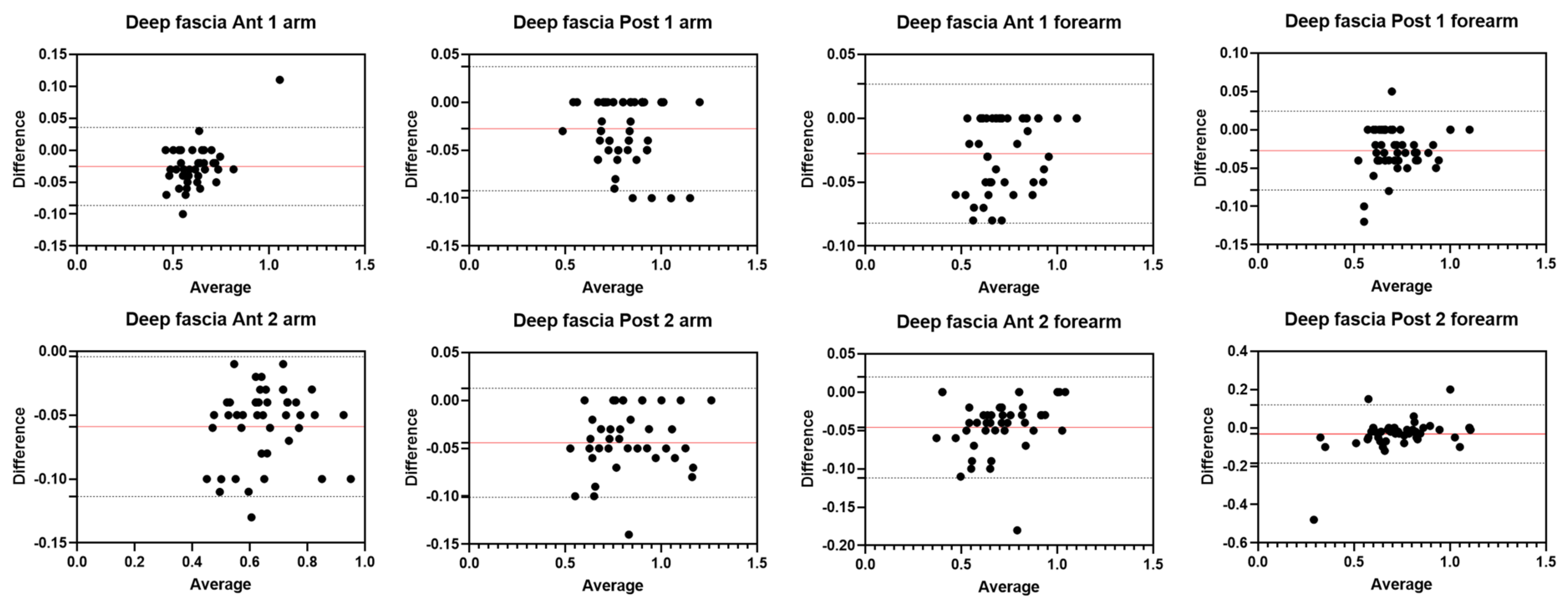
An analysis of our results about the reliability of deep fascia measurements showed excellent inter-rater reliability and intra-rater reliability at different regions/levels. For the anterior region of the arm (Ant 1: ICC2,2 = 0.95; 95% CI = 0.81–0.98; Ant 2: ICC2,2 = 0.92; 95% CI = 0.78–0.98) and for the posterior region of the arm (Post 1: ICC2,2 = 0.97; 95% CI = 0.87–0.99; Post 2: ICC2,2 = 0.93; 95% CI = 0.75–0.97), the inter-reliability was excellent and no significant differences were present between the measurements of the two raters (p > 0.05). Similar to the deep fascia of the arm, also for the forearm, the results showed excellent reliability between the two raters for both the anterior region (Ant 1: ICC2,2 = 0.98; 95% CI = 0.84–0.99; Ant 2: ICC2,2 = 0.97; 95% CI = 0.60–0.99) and the posterior region (Post 1: ICC2,2 = 0.97; 95% CI = 0.79–0.99; Post 2: ICC2,2 = 0.94; 95% CI = 0.90–0.97). No significant differences were present between the measurements of the two raters (p > 0.05).
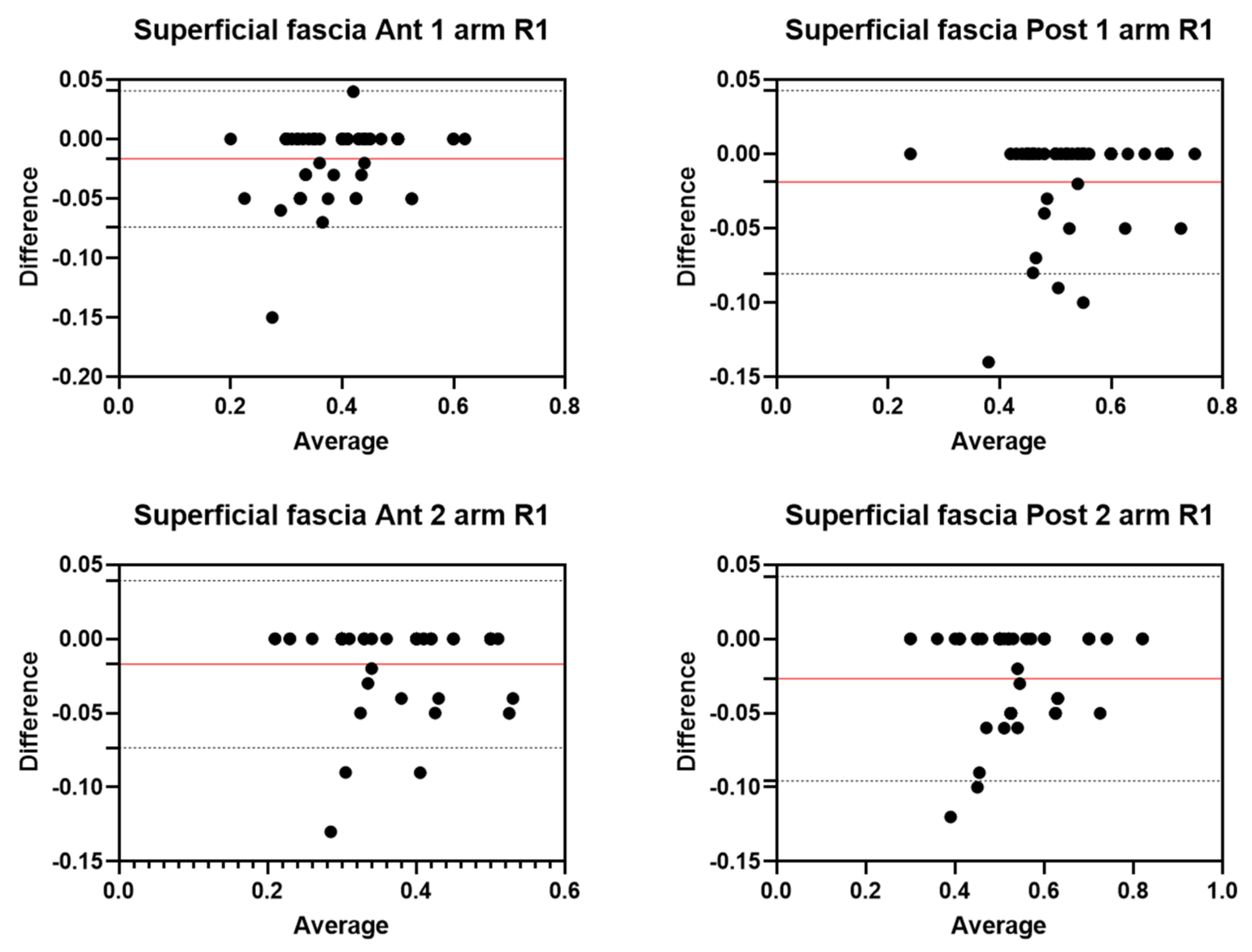
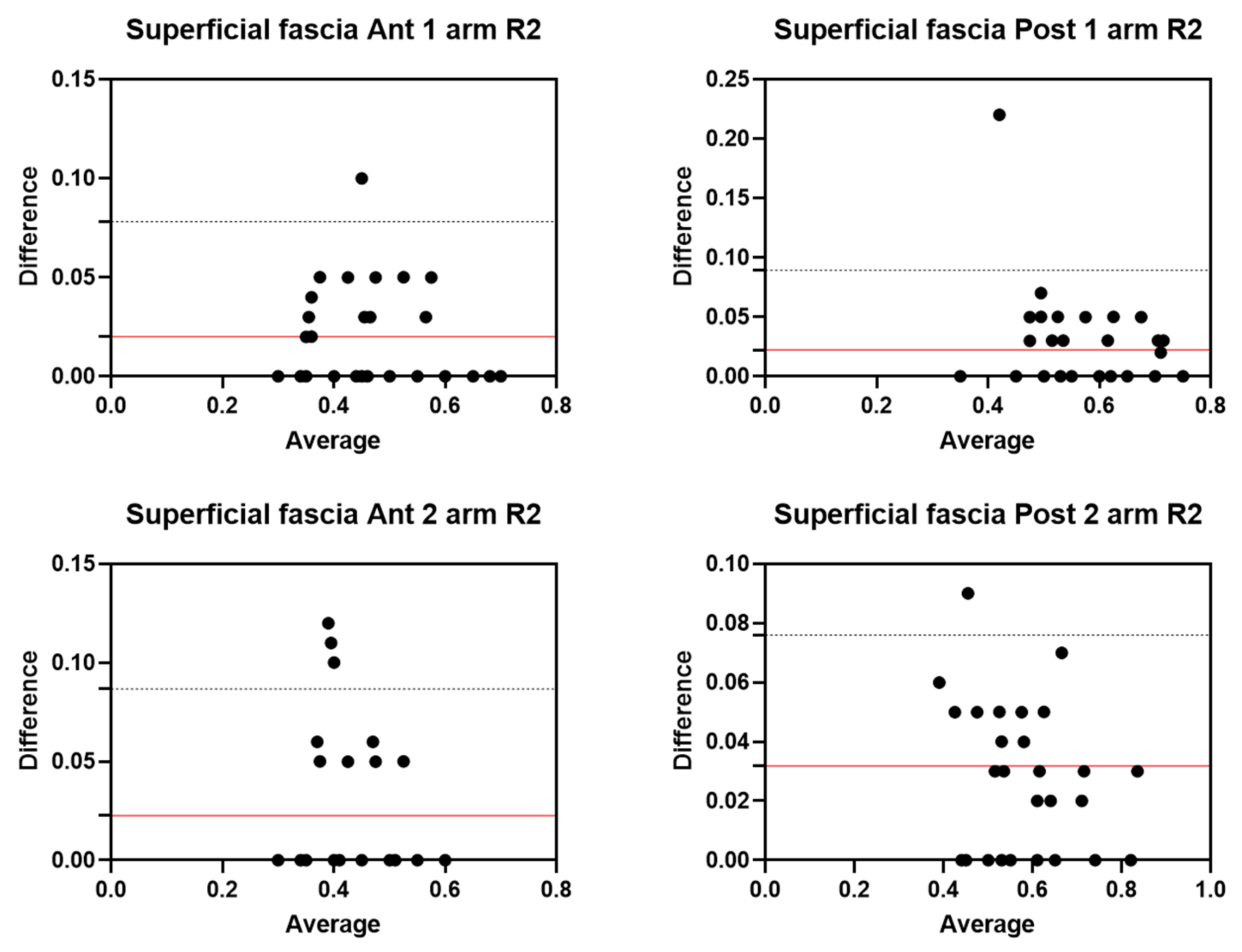
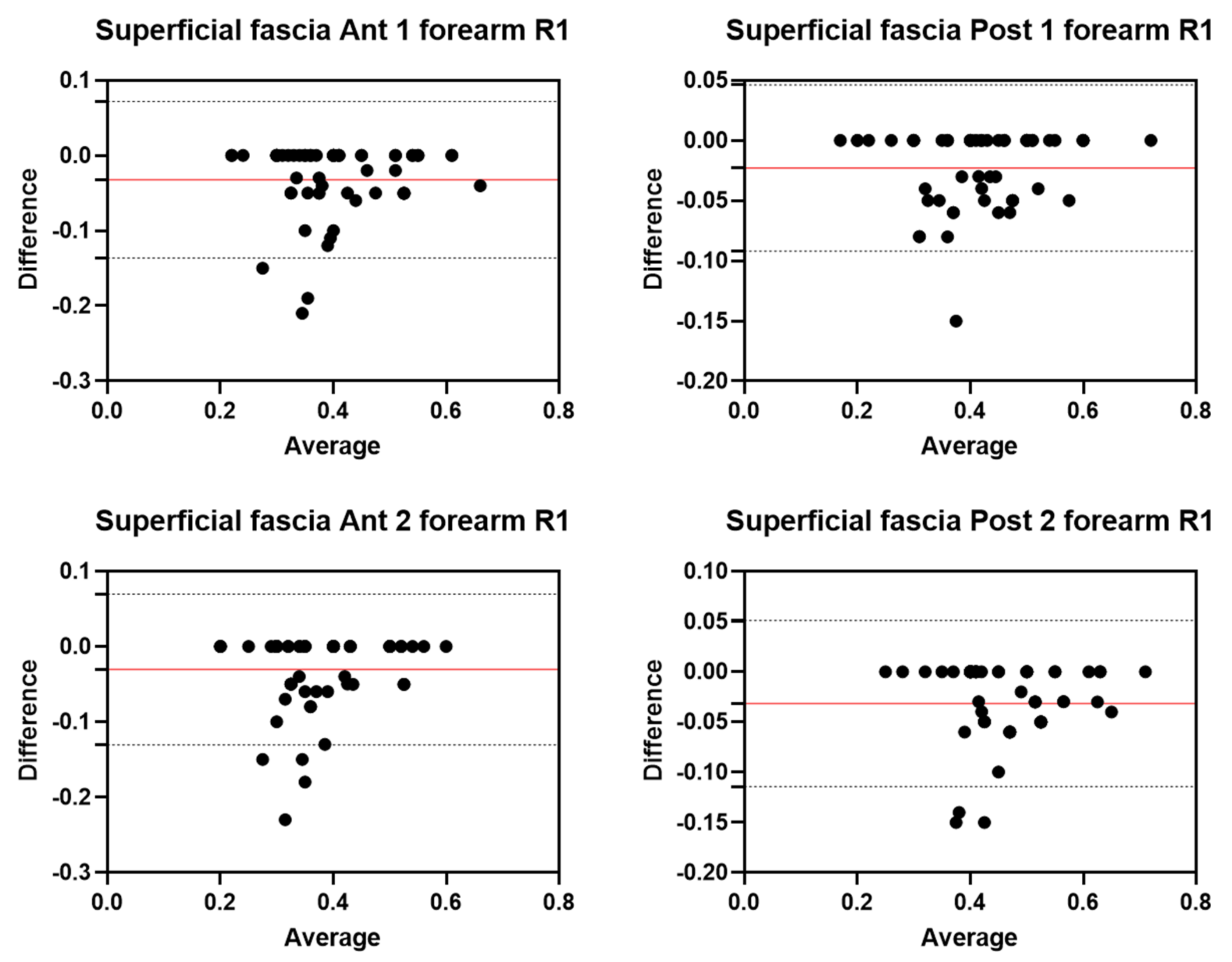
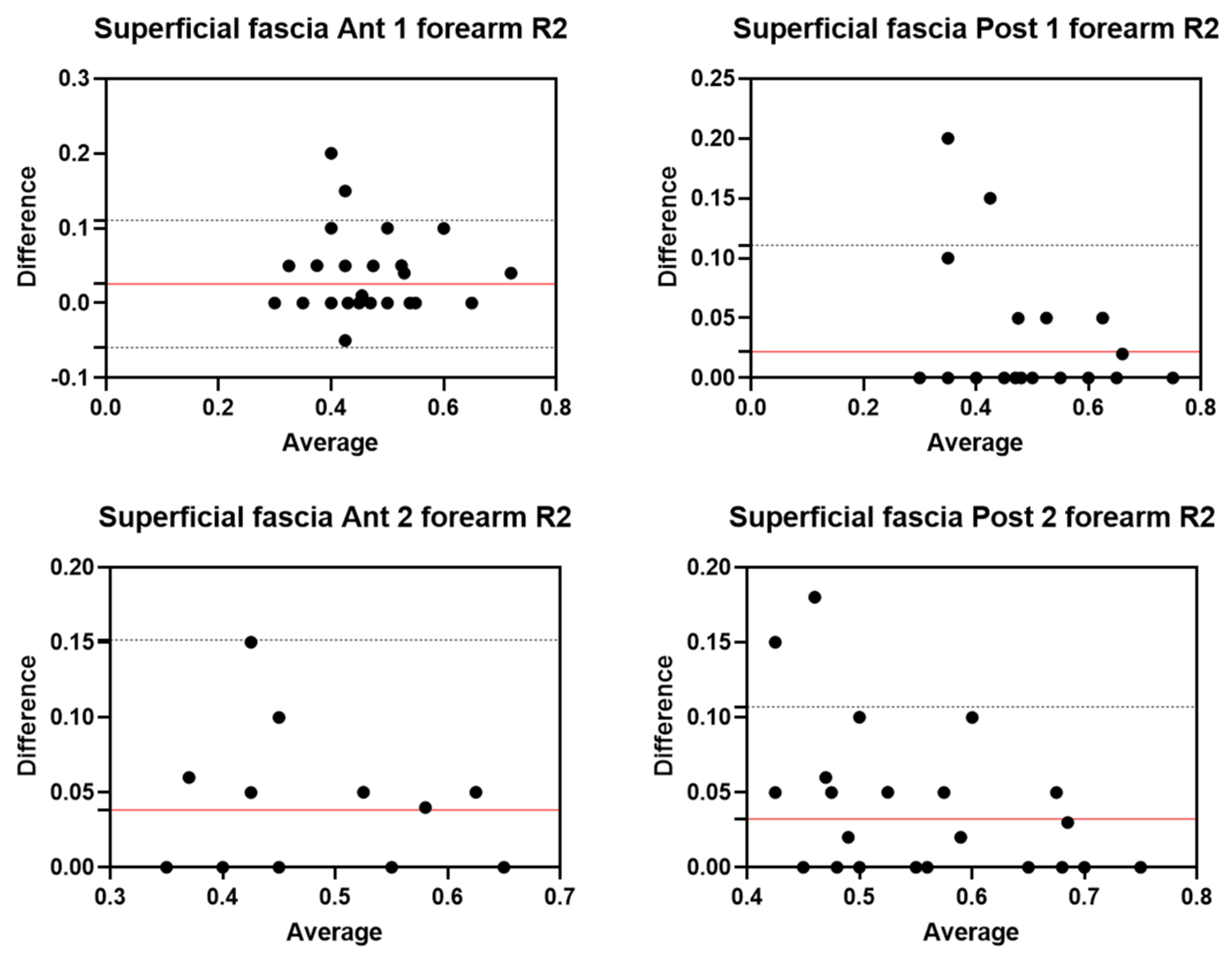
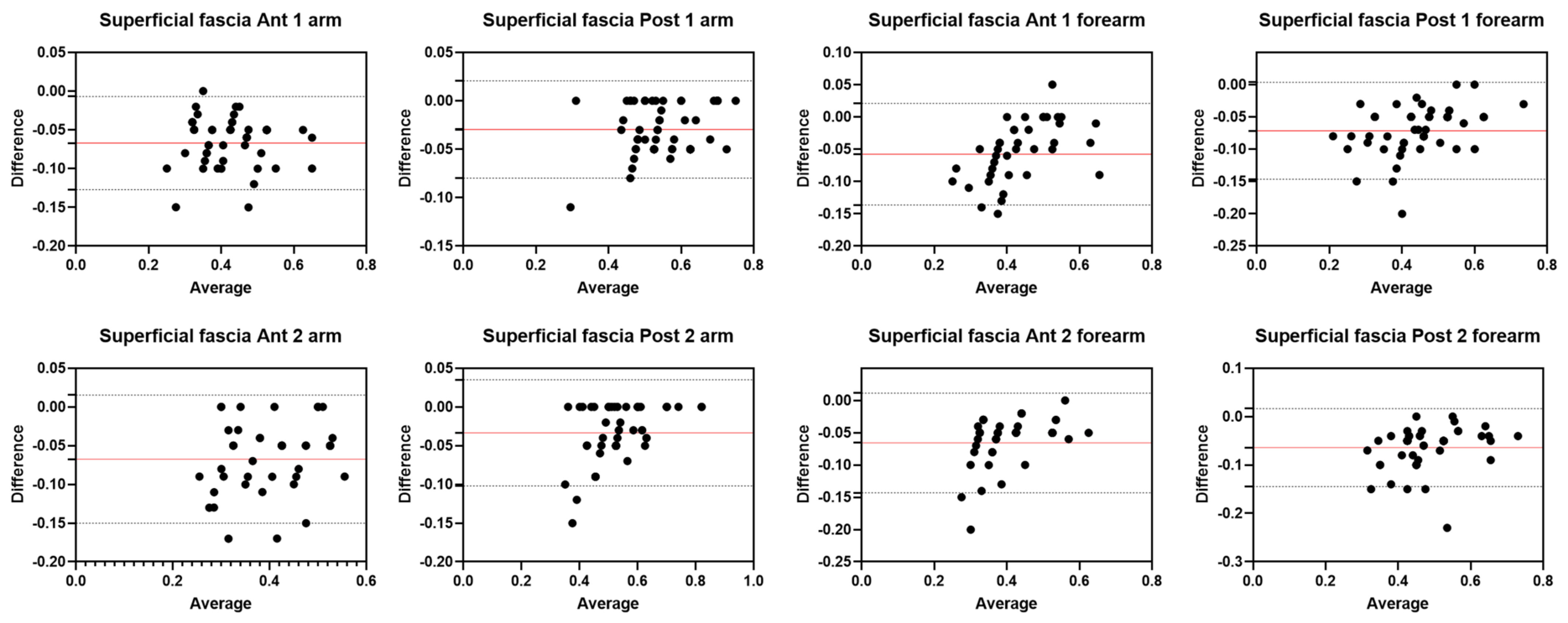
As to the superficial fascia, the inter-rater reliability showed good and excellent inter-rater reliability for all regions/levels for both the arm and forearm. For the posterior region of the arm (Post 1: ICC2,2 = 0.95; 95% CI = 0.70–0.98; Post 2: ICC2,2 = 0.94; 95% CI = 0.67–0.98), the inter-reliability was excellent, whereas for the anterior region of the arm (Ant 1: ICC2,2 = 0.85; 95% CI = 0.79–0.88; Ant 2: ICC2,2 = 0.78; 95% CI = 0.80–0.96), the inter-reliability was good. No significant differences were present between the measurements of the two raters (p > 0.05). Overall, for the forearm, the results showed good reliability between the two raters for both the anterior region (Ant 1: ICC2,2 = 0.86; 95% CI = 0.82–0.96; Ant 2: ICC2,2 = 0.83; 95% CI = 0.82–0.95) and the posterior region (Post 1: ICC2,2 = 0.86; 95% CI = 0.79–0.96; Post 2: ICC2,2 = 0.80; 95% CI = 0.80–0.95). No significant differences were present between the measurements of the two raters (p > 0.05).
Bland–Altman plots showed that the limits of agreement were quite narrow and the majority of measurements were contained within the 95% limits of agreement. To interpret these results, the normal distribution of the differences was verified by the Kolmogorov–Smirnov test, confirming the normality of the distribution. Bland–Altman analysis showed moderate and optimal agreement between the two raters in the assessment of deep and superficial fascia in the different regions/levels of the arm and forearm. The biases were low for both anterior and posterior regions/levels of deep fascia of the arm and forearm. As to the superficial fascia, the biases were low for both regions but slightly higher than those observed for the deep fascia of the arm. Moreover, overall, for the forearm, the biases were low for both regions but slightly higher than those observed for the deep fascia of the arm.
The regions/levels of the forearm and arm that have good reliability and moderate agreement are points in which the superficial fascia adheres more firmly to the deep fascia; therefore, thicker retinacula cutis can confuse the US images. Moreover, the results confirmed, as has been demonstrated by other studies, that in the evaluation of superficial fascia, the inter-reliability is not as excellent as for the deep fascia; however, it maintains good reliability. Furthermore, the Bland–Altman analysis showed that as most measurements fall below the zero line for superficial fascia, R2 consistently measured a higher thickness than R1, indicating that slight disagreement is more systematic than random, underlining how important continuous training is to acquire specific knowledge for the recognition of these anatomical structures. This aspect underlines that the measurement of the superficial fascia, in particular in the forearm, is more difficult as it is a smaller structure than the deep fascia [
30], although there are no significant differences between the measurements of the two raters.
These data confirm that US imaging is an excellent tool to evaluate the fasciae, both superficial and deep, and that excellent inter-rater reliability exists. The reliability found in this study is in line with the results of other reliability studies that have evaluated other areas, such as abdominal fasciae [
23] and lower limb fasciae [
17,
21].
In light of these results, the excellent and good inter-reliability values can be explained by a single rater taking the US images using the same protocol. The possible error by image acquisition was eliminated as a source of variation. US measurements were made on the recorded images by the two raters using the same protocol to assess US images and measure the thicknesses.
The choice to have the US images taken by R1 was made to avoid inter-rater differences that could be linked to the tilting of the transducer or the placement of pressure or the imperfect use of the protocol by R2 as the procedure takes experience and practice.
As reported by other studies, inter-rater reliability is defined as the degree of agreement among measurements by multiple examiners, and it is considered a key factor in research, guaranteeing that different researchers using the same procedure/protocol obtain the same results. In daily practice, in the clinical environment, inter-rater reliability enables physicians to diagnose and monitor a patient’s progress reliably over time [
31,
32].
Therefore, the first step in the training path of the novice R2 is to acquire the specific knowledge of recognizing the anatomical structures through the best ultrasound images; then, with time, experience, and, above all, the study of the various protocols [
14,
15,
17,
21,
23], he will arrive at the final step of taking the images and their analysis. The high variability of these structures imposes specific steps to acquiring the skills, from anatomy to sono-anatomy.
This is the first work, to our knowledge, to examine the intra- and inter-rater reliability in US measurements of superficial and deep fasciae thicknesses in the arm and forearm, as assessed by two raters with different knowledge and experience. The agreement between R1 and R2 suggests and supports that the initial training to increase fascial anatomical knowledge and translate it to sono-anatomy is essential for the good and excellent interpretation and analysis of US images. Moreover, it underlines that it is fundamental to take the images in an optimal manner, arriving at this step of training after having obtained optimal knowledge and experience in skeletal–muscle US imaging.
Limitations of the Study
This study was intentionally focused on a healthy cohort to demonstrate the importance of continuous training to acquire specific knowledge for the recognition of anatomical structures. Nevertheless, despite rigorous efforts (multiple controls of the measurement region/level by each rater) and previous training, the level of experience of the raters, especially in such examiner-dependent assessments as US imaging, must be considered. Finally, the small number of healthy volunteers and the importance of the qualitative aspects in the fascial assessment mean that it is not possible to statistically analyze the prevalence of US findings and to explain their possible causes, prognostic significance, and therapeutic implications.




 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}