
Three-Dimensional Heads-Up vs. Standard Operating Microscope for Cataract Surgery: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Methods
2.3. Study Selection
2.4. Data Collection
2.5. Risk of Bias Assessment
2.6. Assessment of Quality of Evidence
2.7. Data Synthesis and Analysis
3. Results
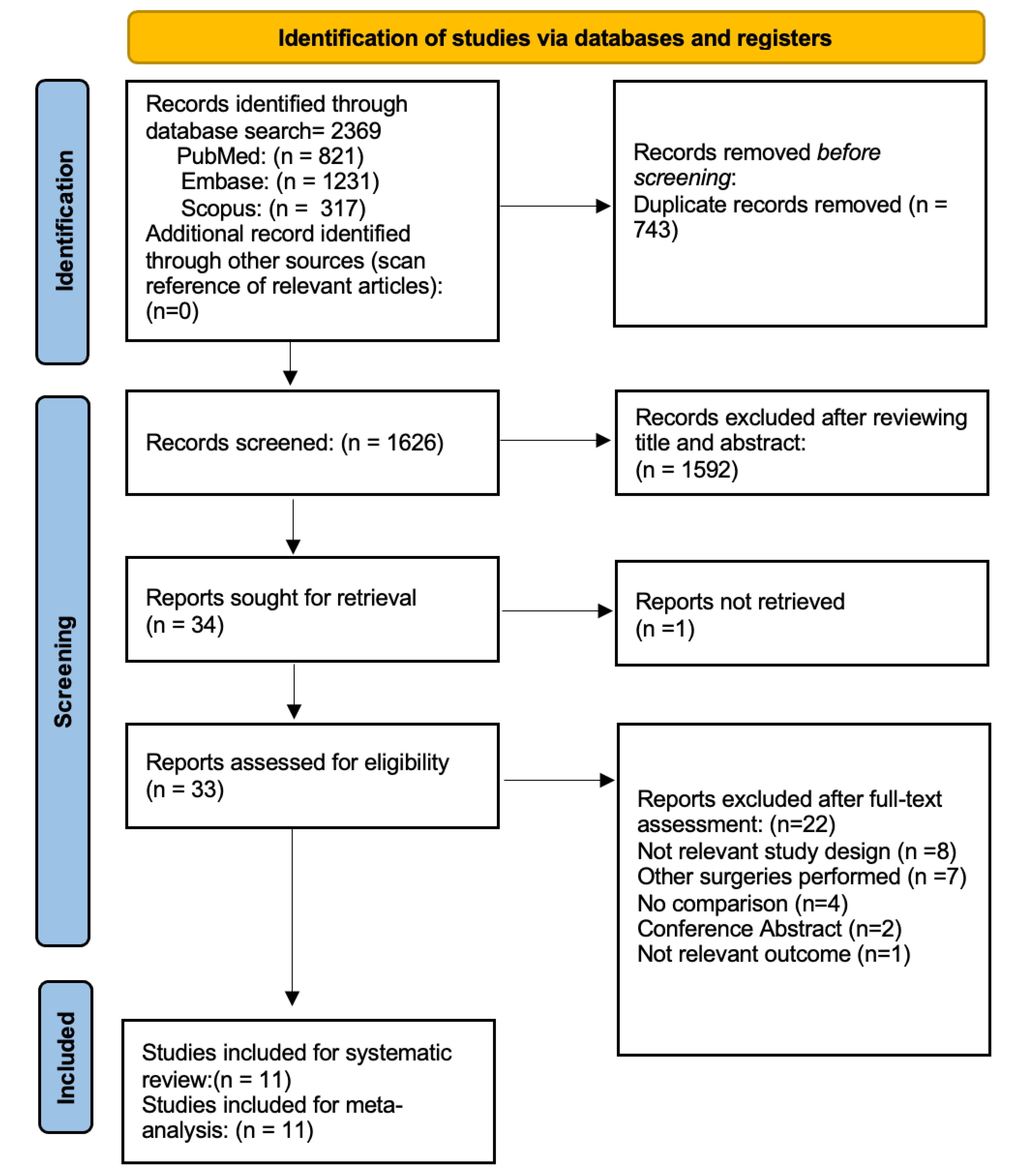
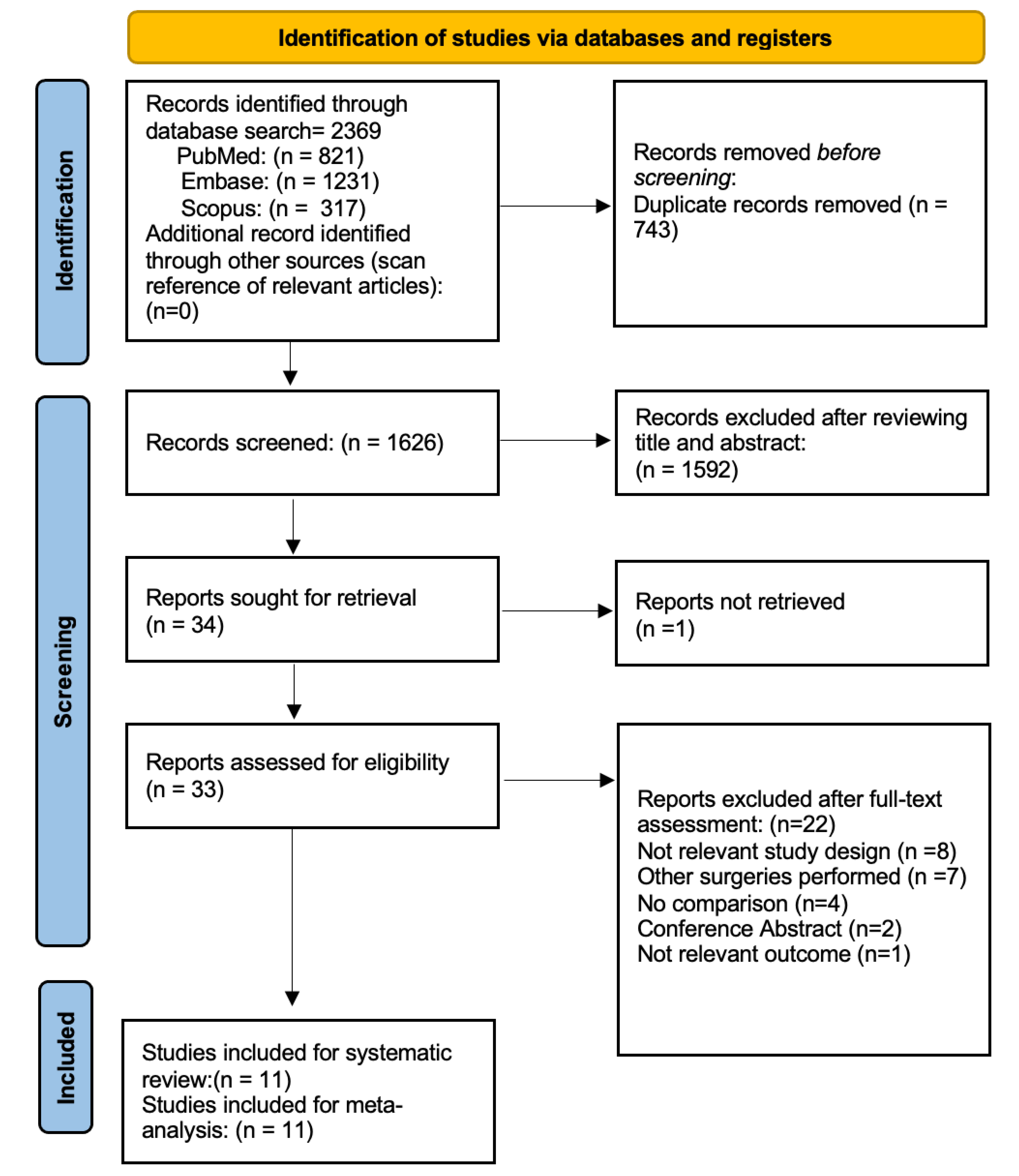
3.1. Study Selection
3.2. Study Characteristics
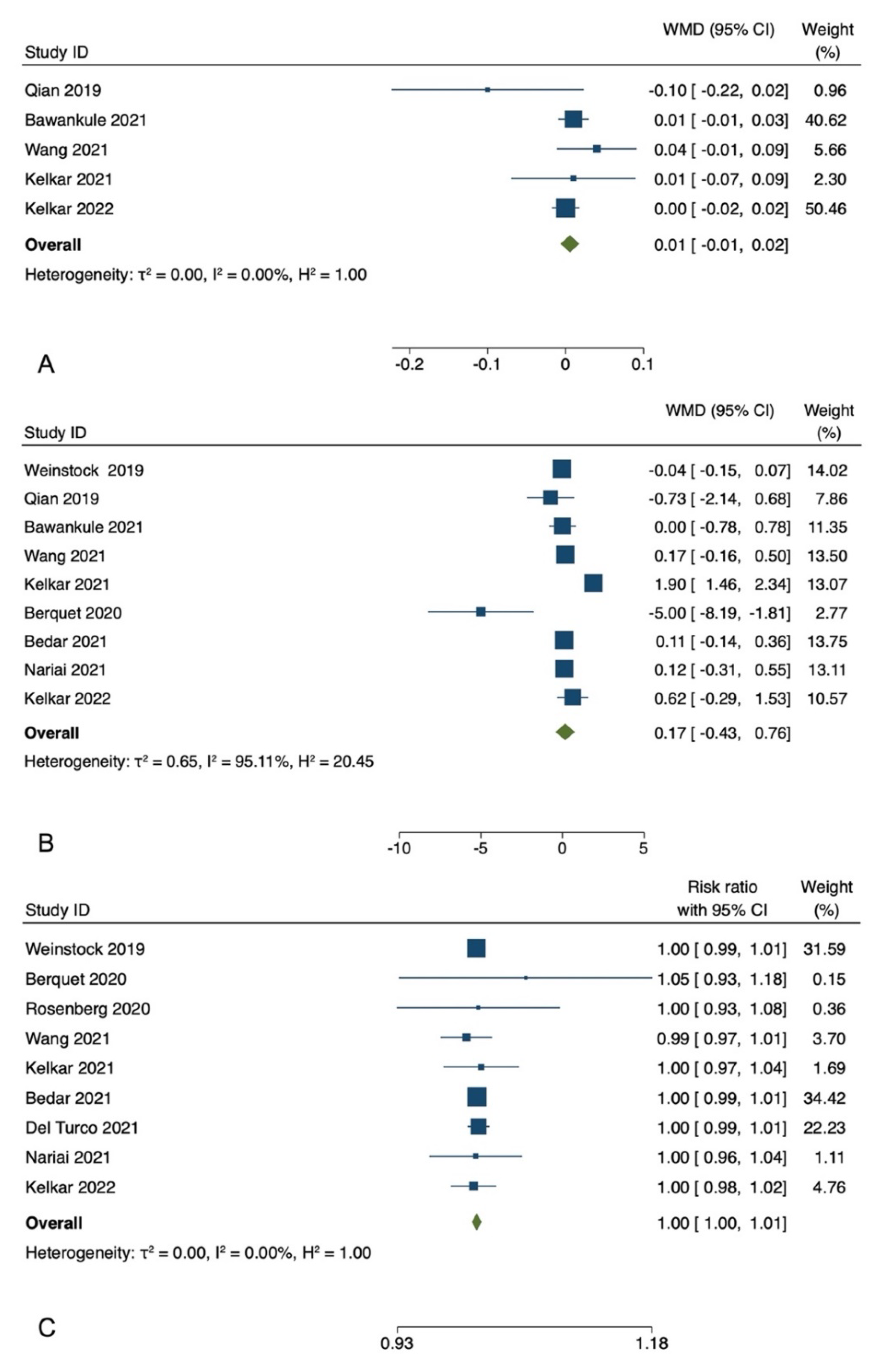
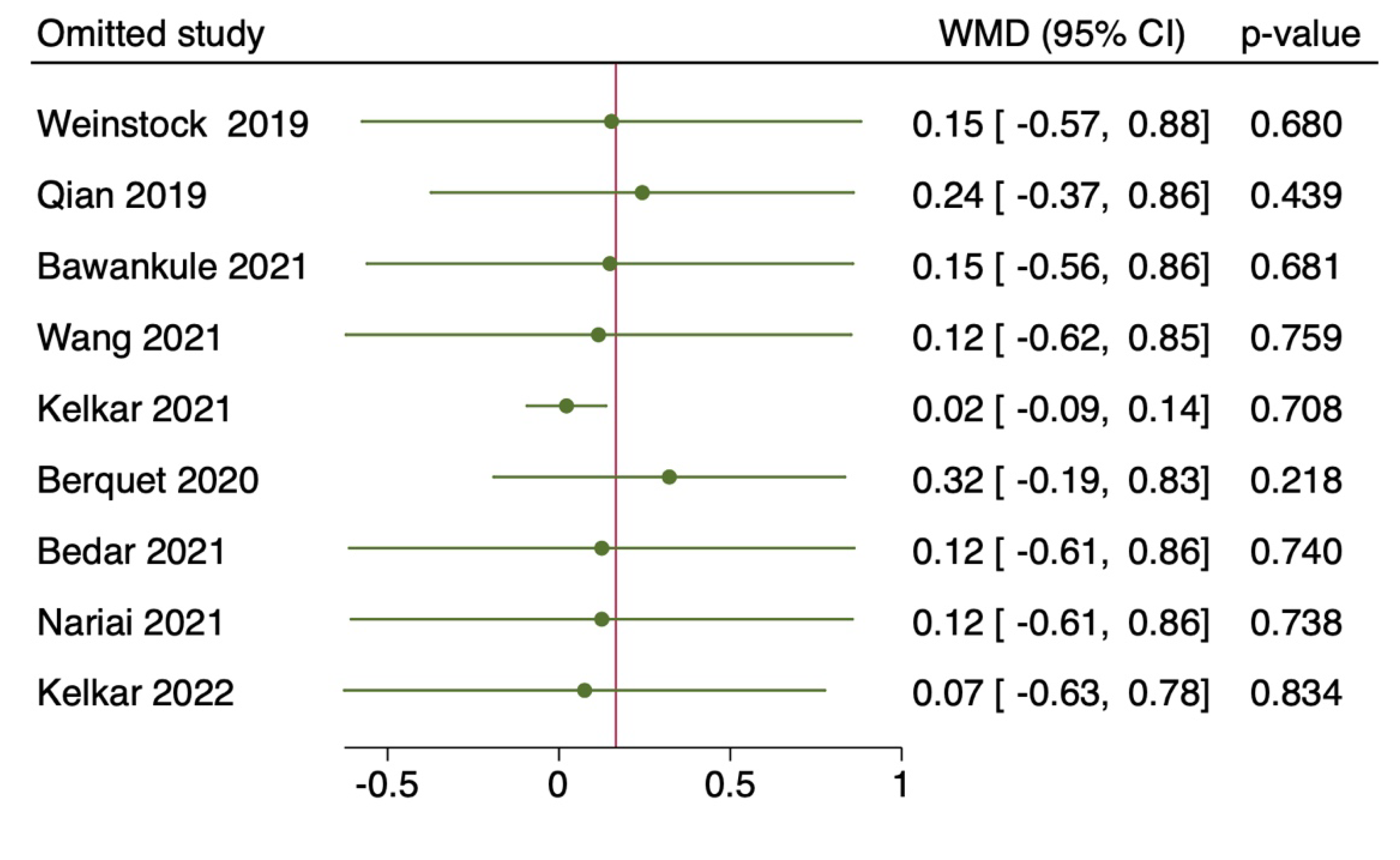
3.3. Postoperative Best-Corrected Visual Acuity
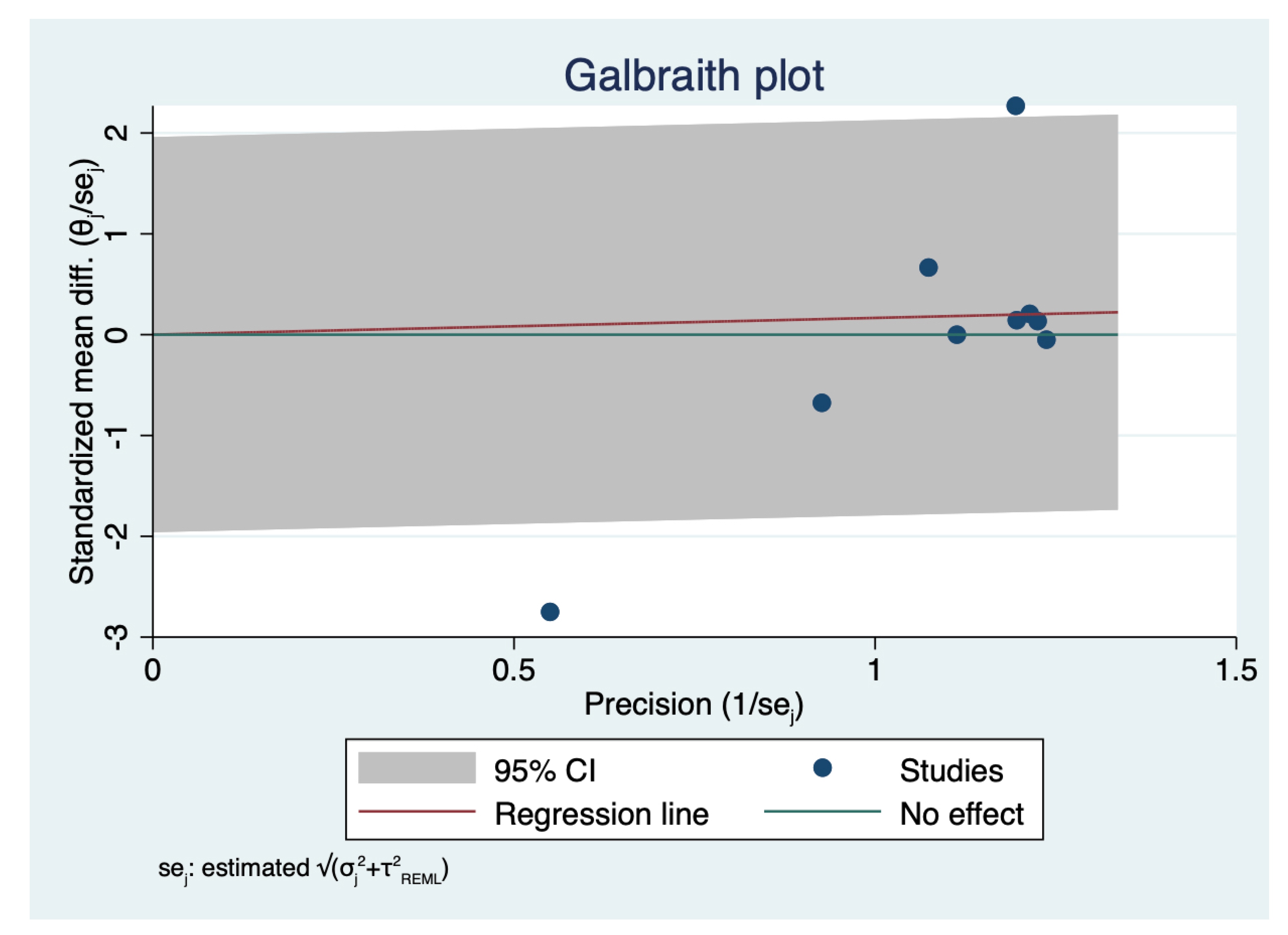
3.4. Duration of Surgical Time
3.5. Incidence Rate of Intraoperative Complications
3.6. Risk of Bias and GRADE Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moura-Coelho, N.; Henriques, J.; Nascimento, J.; Dutra-Medeiros, M. Three-Dimensional Display Systems in Ophthalmic Surgery—A Review. Eur. Ophthalmic Rev. 2019, 13, 31. [Google Scholar] [CrossRef]
- Savastano, A.; Ripa, M.; Savastano, M.C.; de Vico, U.; Caporossi, T.; Kilian, R.; Rizzo, S. Comparison of Novel Digital Microscope Using Integrated Intraoperative OCT with Ngenuity 3D Visualization System in Phacoemulsification. Can. J. Ophthalmol. 2021; Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wu, D.; Ren, X.; Li, X. Clinical Experience of Using the NGENUITY Three-Dimensional Surgery System in Ophthalmic Surgical Procedures. Acta Ophthalmol. 2021, 99, e101–e108. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, R.J.; Diakonis, V.F.; Schwartz, A.J.; Weinstock, A.J. Heads-up Cataract Surgery: Complication Rates, Surgical Duration, and Comparison with Traditional Microscopes. J. Refract. Surg. 2019, 35, 318–322. [Google Scholar] [CrossRef]
- Wang, K.; Song, F.; Zhang, L.; Xu, J.; Zhong, Y.; Lu, B.; Yao, K. Three-Dimensional Heads-up Cataract Surgery Using Femtosecond Laser: Efficiency, Efficacy, Safety, and Medical Education-A Randomized Clinical Trial. Transl. Vis. Sci. Technol. 2021, 10, 4. [Google Scholar] [CrossRef]
- Rosenberg, E.D.; Nuzbrokh, Y.; Sippel, K.C. Efficacy of 3D Digital Visualization in Minimizing Coaxial Illumination and Phototoxic Potential in Cataract Surgery: Pilot Study. J. Cataract Refract. Surg. 2021, 47, 291–296. [Google Scholar] [CrossRef]
- Qian, Z.; Wang, H.; Fan, H.; Lin, D.; Li, W. Three-Dimensional Digital Visualization of Phacoemulsification and Intraocular Lens Implantation. Indian J. Ophthalmol. 2019, 67, 341–343. [Google Scholar] [CrossRef]
- Nariai, Y.; Horiguchi, M.; Mizuguchi, T.; Sakurai, R.; Tanikawa, A. Comparison of Microscopic Illumination between a Three-Dimensional Heads-up System and Eyepiece in Cataract Surgery. Eur. J. Ophthalmol. 2021, 31, 1817–1821. [Google Scholar] [CrossRef]
- Kelkar, J.A.; Kelkar, A.S.; Bolisetty, M. Initial Experience with Three-Dimensional Heads-up Display System for Cataract Surgery—A Comparative Study. Indian J. Ophthalmol. 2021, 69, 2304–2309. [Google Scholar] [CrossRef]
- del Turco, C.; D’Amico Ricci, G.; Dal Vecchio, M.; Bogetto, C.; Panico, E.; Giobbio, D.C.; Romano, M.R.; Panico, C.; la Spina, C. Heads-up 3D Eye Surgery: Safety Outcomes and Technological Review after 2 Years of Day-to-Day Use. Eur. J. Ophthalmol. 2022, 32, 1129–1135. [Google Scholar] [CrossRef]
- Berquet, F.; Henry, A.; Barbe, C.; Cheny, T.; Afriat, M.; Benyelles, A.K.; Bartolomeu, D.; Arndt, C. Comparing Heads-Up versus Binocular Microscope Visualization Systems in Anterior and Posterior Segment Surgeries: A Retrospective Study. Int. J. Ophthalmol. 2020, 243, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Bedar, M.S.; Kellner, U. Digital 3D “Heads-up” Cataract Surgery: Safety Profile and Comparison with the Conventional Microscope System. Klin. Mon. Fur Augenheilkd. 2022, 239, 991–995. [Google Scholar] [CrossRef]
- Bawankule, P.; Narnaware, S.; Chakraborty, M.; Raje, D.; Phusate, R.; Gupta, R.; Rewatkar, K.; Chivane, A.; Sontakke, S. Digitally Assisted Three-Dimensional Surgery—Beyond Vitreous. Indian J. Ophthalmol. 2021, 69, 1793–1800. [Google Scholar] [CrossRef]
- Kelkar, A.; Kelkar, J.; Chougule, Y.; Bolisetty, M.; Singhvi, P. Cognitive Workload, Complications and Visual Outcomes of Phacoemulsification Cataract Surgery: Three-Dimensional versus Conventional Microscope. Eur. J. Ophthalmol. 2022, 32, 2935–2941. [Google Scholar] [CrossRef]
- Agranat, J.S.; Douglas, V.P.; Douglas, K.A.A.; Miller, J.B. A Guarded Light Pipe for Direct Visualization during Primary Scleral Buckling on the Ngenuity Platform. Int. J. Retin. Vitr. 2020, 6, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.R.; Cennamo, G.; Comune, C.; Cennamo, M.; Ferrara, M.; Rombetto, L.; Cennamo, G. Evaluation of 3D Heads-up Vitrectomy: Outcomes of Psychometric Skills Testing and Surgeon Satisfaction. Eye 2018, 32, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Cleo, G.; Scott, A.M.; Islam, F.; Julien, B.; Beller, E. Usability and Acceptability of Four Systematic Review Automation Software Packages: A Mixed Method Design. Syst. Rev. 2019, 8, 1–5. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological Index for Non-Randomized Studies (Minors): Development and Validation of a New Instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Lo, C.K.L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing Reviewers’ to Authors’ Assessments. BMC Med. Res. Methodol. 2014, 14, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE Guidelines: 3. Rating the Quality of Evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Rani, D.; Kumar, A.; Chandra, P.; Chawla, R.; Hasan, N.; Agarwal, D.; Prasad, R. Heads-up 3D Viewing System in Rhegmatogenous Retinal Detachment with Proliferative Vitreoretinopathy—A Prospective Randomized Trial. Indian J. Ophthalmol. 2021, 69, 320. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, C.; Paulo, E.B. Heads-Up Surgery for Vitreoretinal Procedures. Retina 2016, 36, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Hasan, N.; Kakkar, P.; Mutha, V.; Karthikeya, R.; Sundar, D.; Ravani, R. Comparison of Clinical Outcomes between “Heads-up” 3D Viewing System and Conventional Microscope in Macular Hole Surgeries: A Pilot Study. Indian J. Ophthalmol. 2018, 66, 1816–1819. [Google Scholar] [CrossRef]
- Coppola, M.; la Spina, C.; Rabiolo, A.; Querques, G.; Bandello, F. Heads-up 3D Vision System for Retinal Detachment Surgery. Int. J. Retin. Vitr. 2017, 3, 1–3. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, L.; Wei, Y.; Fang, D.; Fan, S.; Zhang, S. The Preliminary Experiences with Three-Dimensional Heads-Up Display Viewing System for Vitreoretinal Surgery under Various Status. Curr. Eye Res. 2019, 44, 102–109. [Google Scholar] [CrossRef]
- Palácios, R.M.; de Carvalho, A.C.M.; Maia, M.; Caiado, R.R.; Camilo, D.A.G.; Farah, M.E. An Experimental and Clinical Study on the Initial Experiences of Brazilian Vitreoretinal Surgeons with Heads-up Surgery. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 473–483. [Google Scholar] [CrossRef]
- Rizzo, S.; Abbruzzese, G.; Savastano, A.; Caporossi, T.; Barca, F. 3D Surgical viewing system in ophthalmology: Perceptions of the Surgical Team. Retina 2018, 38, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Mendez, B.M.; Chiodo, M.V.; Vandevender, D.; Patel, P.A. Heads-up 3D Microscopy: An Ergonomic and Educational Approach to Microsurgery. Plast. Reconstr. Surg. Glob. Open 2016, 4, e717. [Google Scholar] [CrossRef] [PubMed]
- De, J.; Barbosa, P.; Ribeiro, J.C.; Machado, A.J. Heads-up Surgery with Three-Dimensional Display Devices for Cataract Surgeries Cirurgia Heads-up Com Sistemas de Visualização Tridimensional Para Cirurgias Oftálmicas de Catarata. Arq. Bras. Oftalmol. 2021, 84, 193–197. [Google Scholar] [CrossRef]
- Ohno, H. Utility Of Three-Dimensional Heads-Up Surgery In Cataract And Minimally Invasive Glaucoma Surgeries. Clin. Ophthalmol. 2019, 13, 2071–2073. [Google Scholar] [CrossRef] [PubMed]
- Hamasaki, I.; Shibata, K.; Shimizu, T.; Kono, R.; Morizane, Y.; Shiraga, F. Lights-out Surgery for Strabismus Using a Heads-Up 3D Vision System. Acta Med. Okayama 2019, 73, 229–233. [Google Scholar] [CrossRef]
- Galvis, V.; Berrospi, R.D.; Arias, J.D.; Tello, A.; Bernal, J.C. Heads up Descemet Membrane Endothelial Keratoplasty Performed Using a 3D Visualization System. J. Surg. Case Rep. 2017, 2017, rjx231. [Google Scholar] [CrossRef]
- Reddy, S.; Mallikarjun, K.; Mohamed, A.; Mruthyunjaya, P.; Dave, V.P.; Pappuru, R.R.; Chhablani, J.; Narayanan, R. Comparing Clinical Outcomes of Macular Hole Surgeries Performed by Trainee Surgeons Using a 3D Heads-up Display Viewing System versus a Standard Operating Microscope. Int. Ophthalmol. 2021, 41, 2649–2655. [Google Scholar] [CrossRef]
- Gupta, Y.; Tandon, R. Optimization of Surgeon Ergonomics with Three-Dimensional Heads-up Display for Ophthalmic Surgeries. Indian J. Ophthalmol. 2022, 70, 847–850. [Google Scholar] [CrossRef]
- Kaur, M.; Titiyal, J.S. Three-Dimensional Heads up Display in Anterior Segment Surgeries- Expanding Frontiers in the COVID-19 Era. Indian J. Ophthalmol. 2020, 68, 2338–2340. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Study Design | 3D HUVS Used | SOM Used | Number of Cataract Surgeries (n.) | Surgical Duration: (min.) | Intraoperative Complications:(n.) | Postoperative BCVA (LogMar) | Mean Light Exposure Time (min.)/Ocular Surface Illuminance (lux) | Other Parameters Evaluated |
|---|---|---|---|---|---|---|---|---|---|---|
| Weinstock et al. | 2019 | RS | Ngenuity 3D visualization system | Not reported | Total: 2320 HUVS: 1673 SOM: 647 | HUVS: 6.48 ± 1.15 SOM: 6.52 ± 1.38 | Total: 17 HUVS: 12 SOM: 5 | Not reported | Not reported | None |
| Qian et al. | 2019 | RCT | Ngenuity 3D visualization system | OPMI LUMERA T surgical microscope | Total: 20 HUVS: 10 SOM: 10 | HUVS: 8.3 ± 1.73 SOM:9.03 ± 1.47 | Not reported | HUVS: 0.19 ± 0.2 SOM: 0.09 ± 0.14 | Not reported | Preoperative BCVA and Preoperative and Postoperative ECD |
| Berquet et al. | 2020 | RS | Ngenuity 3D visualization system | OPMI LUMERA 700 | Total: 73 HUVS: 25 SOM: 48 | HUVS: 16.44 ± 4.36 SOM: 21.44 ± 7.50 | Total: 5 HUVS: 1 SOM: 4 | Not reported | Not reported | Visual comfort; Operative Fluency; Backache; Headache |
| Rosenberg et al. | 2020 | RS | Ngenuity 3D visualization system | OPMI LUMERA 700 | Total: 51 HUVS: 27 SOM: 24 | Not reported | Total: 0 HUVS: 0 SOM: 0 | UDVA in lines of vision gained | HUVS: 23.8 ± 1.9 SOM: 25.8 ± 3.0 | None |
| Bawankule et al. | 2021 | RCT | Ngenuity 3D visualization system | Not reported | Total: 213 HUVS: 101 SOM: 112 | HUVS: 13.11 ± 3.7 (learning phase) 9.74 ± 2.79 (post-learning phase) SOM: 9.74 ± 2.97 | Not reported | HUVS: 0.02 ± 0.06 (learning Phase) 3D: 0.03 ± 0.07 (Post-learning Phase) SOM: 0.03 ± 0.07 | Not reported | Surgical outcomes surgeon’s perspective like time lag, illumination, learning curve, ease of doing various steps and its value as an educational tool |
| Wang et al. | 2021 | RCT | NCVideo 3D system | Not reported | Total: 242 HUVS: 117 SOM: 125 | HUVS: 7.7 ± 1.34 SOM:7.53 ± 1.28 | Total: 1 HUVS: 1 SOM: 0 | HUVS: 0.26 ± 0.2 SOM: 0.30 ± 0.2 | Not reported | Depth of field, visibility, detail understanding; knowledge retention; and educational value; preoperative BCVA and preoperative and postoperative IOP |
| Kelkar et al. | 2021 | Non-RCT | Artevo 800 | Not reported | Total: 343 HUVS: 100 SOM: 243 | HUVS: 8.4 ± 2.1 SOM: 6.5 ± 1.8 | Total: 8 HUVS: 2 SOM: 6 | SOM 0.40 ± 0.27 HUVS: 0.41 ± 0.34 | Not reported | Surgical parameters; binocular conversion, Difficulty with 3-D Heads up display group (low illumination, difficult depth perception) and surgeon workload score |
| Bedar et al. | 2021 | RS | Ngenuity 3D visualization system | Zeiss OPMI Visu160 | Total: 2000 HUVS: 1000 SOM: 1000 | HUVS: 11.84 ± 2.9 SOM: 11.73 ± 2.8 | Total: 15 HUVS: 7 SOM: 8 | Not reported | Not reported | None |
| Del Turco et al. | 2021 | RS | Ngenuity 3DVisualization System and Artevo 800 | Not reported | Total: 3286 HUVS: 1638 SOM: 1648 | Not reported | Total: 62 HUVS: 29 SOM: 33 | Not reported | Not reported | Comfort, visibility, image quality, maneuverability, teaching potential, depth perception, and simplicity of use |
| Nariai et al. | 2021 | RS | Ngenuity 3D visualization system | OMS800 Topcon | Total: 91 HUVS: 45 SOM: 46 | HUVS: CCC + PEA + I/A: 3.2 ± 1.16 SOM: CCC + PEA + I/A: 3.08 ± 0.94 | Total: 0 HUVS: 0 SOM: 0 | Not reported | Ocular surface illuminance HUVS: 5500 ± 2000 SOM: 1900 ± 1800 | None |
| Kelkar et al. | 2022 | Non-RCT | Artevo 800 | Zeiss Lumera 700 | Total: 203 HUVS: 80 SOM: 123 | HUVS: 8.07 ± 2.94 SOM: 7.45 ± 3.66 | Total: 0 HUVS: 0 SOM: 0 | SOM: 0.3 (0.2–0.48) HUVS: 0.3 (0.2–0.5) | Not reported | Cognitive load assessment (Heart Rate, Oxigen Saturation and SURG-TLX analysis) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ripa, M.; Kopsacheilis, N.; Kanellopoulou, K.; Nomikarios, M.; Motta, L. Three-Dimensional Heads-Up vs. Standard Operating Microscope for Cataract Surgery: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 2100. https://doi.org/10.3390/diagnostics12092100
Ripa M, Kopsacheilis N, Kanellopoulou K, Nomikarios M, Motta L. Three-Dimensional Heads-Up vs. Standard Operating Microscope for Cataract Surgery: A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(9):2100. https://doi.org/10.3390/diagnostics12092100
Chicago/Turabian StyleRipa, Matteo, Nikolaos Kopsacheilis, Kanellina Kanellopoulou, Mikes Nomikarios, and Lorenzo Motta. 2022. "Three-Dimensional Heads-Up vs. Standard Operating Microscope for Cataract Surgery: A Systematic Review and Meta-Analysis" Diagnostics 12, no. 9: 2100. https://doi.org/10.3390/diagnostics12092100
APA StyleRipa, M., Kopsacheilis, N., Kanellopoulou, K., Nomikarios, M., & Motta, L. (2022). Three-Dimensional Heads-Up vs. Standard Operating Microscope for Cataract Surgery: A Systematic Review and Meta-Analysis. Diagnostics, 12(9), 2100. https://doi.org/10.3390/diagnostics12092100