
HCC or Something Else? Frequency of Various Benign and Malignant Etiologies in Cirrhotic Patients with Newly Detected Focal Liver Lesions in Relation to Different Clinical and Sonographic Parameters

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Demographic and Clinical Characteristics of Study Participants
2.2. History of Active Non-Hepatic Malignancy
2.3. Indications to Perform US
2.4. US and CEUS Examinations
2.5. Cross-Sectional Imaging
2.6. Histological Specimens
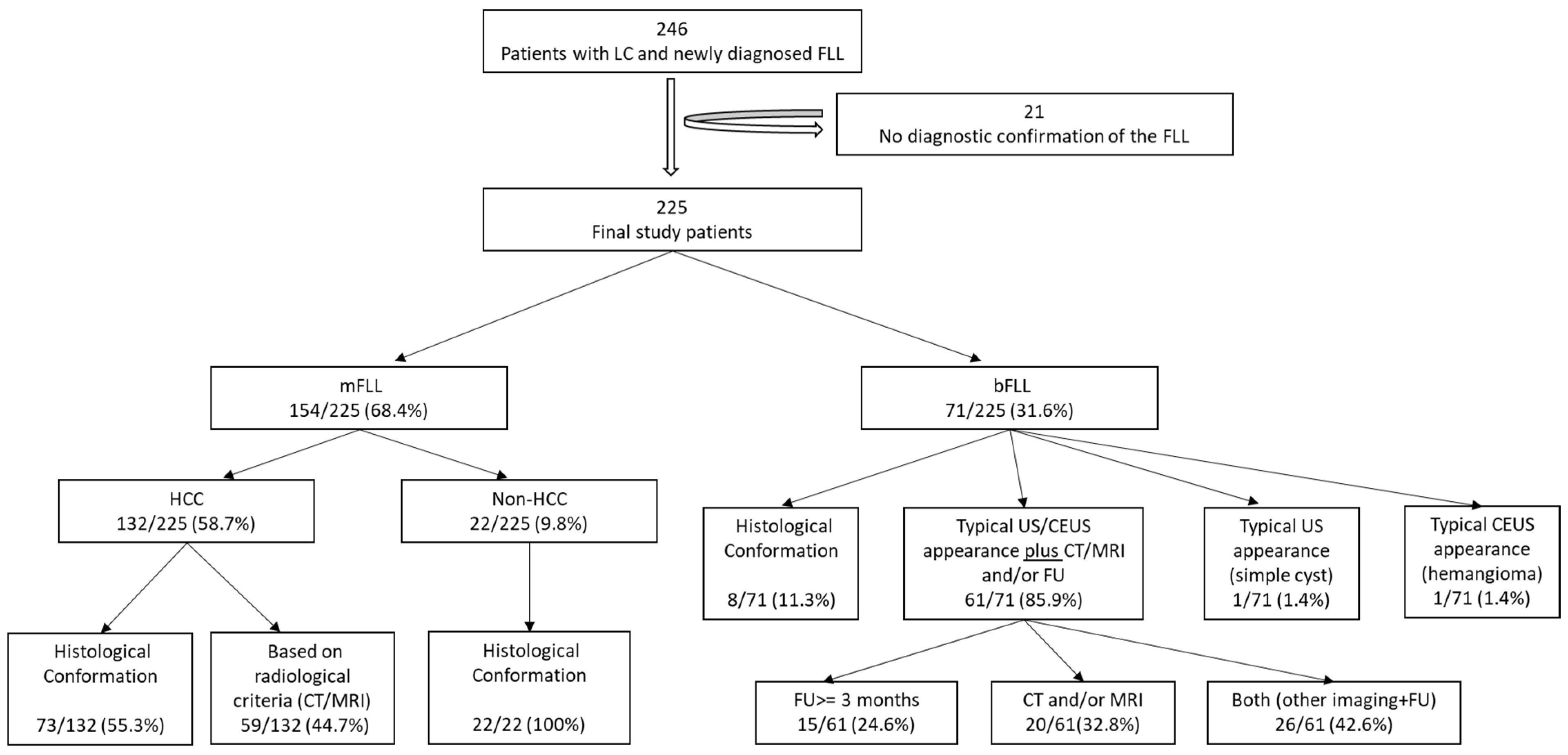
2.7. Diagnostic Confirmation of FLLs
2.8. Statistical Analysis
3. Results
3.1. Final Etiologies of the FLLs
3.2. Clinical Features
3.3. Laboratory Parameters
3.4. Sonographic Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AFP | Alpha-fetoprotein |
| AIH | Autoimmune hepatitis |
| APHE | Arterial phase hyperenhancement |
| bFLLs | Benign focal liver lesions |
| B-US | B-mode ultrasound |
| CEUS | Contrast enhanced ultrasound |
| CRC | Colorectal carcinoma |
| CT | Computer tomography |
| CTP | Child–Pugh–Turcotte |
| CUP | Cancer of unknown primary |
| DEGUM | German Society of Ultrasound in Medicine |
| EASL | European Association for the Study of the Liver |
| EFSUMB | European Federation of Societies for Ultrasound in Medicine and Biology |
| FDS | Fat deposition/sparing |
| FLLs | Focal liver lesions |
| FU | Follow-up |
| HBV | Hepatitis B virus |
| HCC | Hepatocellular carcinoma |
| HCV | Hepatitis C virus |
| ICC | Intrahepatic cholangiocarcinoma |
| LC | Liver cirrhosis |
| LI-RADS | Liver imaging reporting and data system |
| MELD-Na | Model of end-stage liver disease with sodium |
| mFLLs | Malignant focal liver lesions |
| MRI | Magnetic resonance imaging |
| NASH | Non-alcoholic steatohepatitis |
| NET | Neuroendocrine tumor |
| NHPMD | Non-hepatic primary malignant disease |
| PBC | Primary biliary cirrhosis |
| PSC | Primary sclerosing cholangitis |
| PVT | Portal vein thrombosis |
| RN | Regenerative nodule |
| SD | Standard deviation |
| TIV | Tumor in a vein |
| US | Ultrasound |
References
- Moon, A.M.; Singal, A.G.; Tapper, E.B. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 18, 2650–2666. [Google Scholar] [CrossRef] [PubMed]
- Pimpin, L.; Cortez-Pinto, H.; Negro, F.; Corbould, E.; Lazarus, J.V.; Webber, L.; Sheron, N. Burden of liver disease in Europe: Epidemiology and analysis of risk factors to identify prevention policies. J. Hepatol. 2018, 69, 718–735. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Huang, J.L.W.; George, J.; Huang, J.; Leung, C.; Eslam, M.; Chan, H.L.Y.; Ng, S.C. The changing epidemiology of liver diseases in the Asia-Pacific region. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 57–73. [Google Scholar] [CrossRef]
- EASL. Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Lampertico, P.; Nahon, P. Epidemiology and surveillance for hepatocellular carcinoma: New trends. J. Hepatol. 2020, 72, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Tang, A.; Santillan, C.; Sirlin, C. Cirrhotic liver: What’s that nodule? The LI-RADS approach. J. Magn. Reason. Imaging 2016, 43, 281–294. [Google Scholar] [CrossRef]
- Ignee, A.; Weiper, D.; Schuessler, G.; Teuber, G.; Faust, D.; Dietrich, C.F. Sonographic characterisation of hepatocellular carcinoma at time of diagnosis. Z. Gastroenterol. 2005, 43, 289–294. [Google Scholar] [CrossRef]
- van der Pol, C.B.; Lim, C.S.; Sirlin, C.B.; McGrath, T.A.; Salameh, J.P.; Bashir, M.R.; Tang, A.; Singal, A.G.; Costa, A.F.; Fowler, K.; et al. Accuracy of the Liver Imaging Reporting and Data System in Computed Tomography and Magnetic Resonance Image Analysis of Hepatocellular Carcinoma or Overall Malignancy-A Systematic Review. Gastroenterology 2019, 156, 976–986. [Google Scholar] [CrossRef]
- Caraiani, C.; Boca, B.; Bura, V.; Sparchez, Z.; Dong, Y.; Dietrich, C. CT/MRI LI-RADS v2018 vs. CEUS LI-RADS v2017-Can Things Be Put Together? Biology 2021, 10, 412. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Dong, Y.; Kono, Y.; Caraiani, C.; Sirlin, C.B.; Cui, X.W.; Tang, A. LI-RADS ancillary features on contrast-enhanced ultrasonography. Ultrasonography 2020, 39, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Lyshchik, A.; Kono, Y.; Dietrich, C.F.; Jang, H.J.; Kim, T.K.; Piscaglia, F.; Vezeridis, A.; Willmann, J.K.; Wilson, S.R. Contrast-enhanced ultrasound of the liver: Technical and lexicon recommendations from the ACR CEUS LI-RADS working group. Abdom. Radiol. 2018, 43, 861–879. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Potthoff, A.; Helmberger, T.; Ignee, A.; Willmann, J.K.; Group, C.L.-R.W. Contrast-enhanced ultrasound: Liver Imaging Reporting and Data System (CEUS LI-RADS). Z. Gastroenterol. 2018, 56, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Lima, J.E.; Lichtenfels, E.; Barbosa, F.S.; Zettler, C.G.; Kulczynski, J.M. Prevalence study of metastases in cirrhotic livers. Hepatogastroenterology 2003, 50, 1490–1495. [Google Scholar]
- Lieber, M.M. The rare occurrence of metastatic carcinoma in the cirrhotic liver. Am. J. Med. Sci. 1957, 233, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Wallach, J.B.; Hyman, W.; Angrist, A.A. Metastasis to liver portal cirrhosis. Am. J. Clin. Pathol. 1953, 23, 989–993. [Google Scholar] [CrossRef]
- Seitz, K.; Greis, C.; Schuler, A.; Bernatik, T.; Blank, W.; Dietrich, C.F.; Strobel, D. Frequency of tumor entities among liver tumors of unclear etiology initially detected by sonography in the noncirrhotic or cirrhotic livers of 1349 patients. Results of the DEGUM multicenter study. Ultraschall Med. 2011, 32, 598–603. [Google Scholar] [CrossRef]
- Mahdi, Z.; Ettel, M.G.; Gonzalez, R.S.; Hart, J.; Alpert, L.; Fang, J.; Liu, N.; Hammer, S.T.; Panarelli, N.; Cheng, J.; et al. Metastases can occur in cirrhotic livers with patent portal veins. Diagn. Pathol. 2021, 16, 18. [Google Scholar] [CrossRef]
- Bartolotta, T.V.; Terranova, M.C.; Gagliardo, C.; Taibbi, A. CEUS LI-RADS: A pictorial review. Insights Imaging 2020, 11, 9. [Google Scholar] [CrossRef]
- Wills, M.; Harvey, C.J.; Kuzmich, S.; Afaq, A.; Lim, A.; Cosgrove, D. Characterizing benign liver lesions and trauma with contrast-enhanced ultrasound. Br. J. Hosp. Med. 2014, 75, 91–95. [Google Scholar] [CrossRef]
- Claudon, M.; Dietrich, C.F.; Choi, B.I.; Cosgrove, D.O.; Kudo, M.; Nolsøe, C.P.; Piscaglia, F.; Wilson, S.R.; Barr, R.G.; Chammas, M.C.; et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: A WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med. 2013, 34, 11–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heese, F.; Görg, C. Diagnostische Wertigkeit einer internistischen Referenzsonographie (DEGUM-Stufe 3). Ultraschall Med.-Eur. J. Ultrasound 2006, 27, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Kwon, H.J.; Lee, S.Y.; Park, H.J.; Kim, M.S.; Sohn, J.H.; Chung, E.C.; Park, H.W. Focal hepatic solid lesions incidentally detected on initial ultrasonography in 542 asymptomatic patients. Abdom. Radiol. 2016, 41, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Heller, E.; Görg, C. Focal liver lesions in patients with malignant haematological disease: Value of B-mode ultrasound in comparison to contrast-enhanced ultrasound—A retrospective study with N = 61 patients. Z. Gastroenterol. 2013, 51, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Safai Zadeh, E.; Baumgarten, M.A.; Dietrich, C.F.; Görg, C.; Neesse, A.; Trenker, C.; Alhyari, A. Frequency of synchronous malignant liver lesions initially detected by ultrasound in patients with newly diagnosed underlying non-hematologic malignant disease: A retrospective study in 434 patients. Z. Gastroenterol. 2022, 60, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Ajayi, F.; Jan, J.; Singal, A.G.; Rich, N.E. Racial and Sex Disparities in Hepatocellular Carcinoma in the USA. Curr. Hepatol. Rep. 2020, 19, 462–469. [Google Scholar] [CrossRef]
- Kanda, T.; Jiang, X.; Yokosuka, O. Androgen receptor signaling in hepatocellular carcinoma and pancreatic cancers. World J. Gastroenterol. 2014, 20, 9229–9236. [Google Scholar] [CrossRef]
- Mogahed, M.M.; Zytoon, A.A.; Essa, B.; Abdellatif, W.; Ghanem, N.; ElWakeel, B. Natural history of hepatic hemangiomas as a guide for surgical indication. Egypt. Liver J. 2020, 10, 56. [Google Scholar] [CrossRef]
- Grazioli, L.; Ambrosini, R.; Frittoli, B.; Grazioli, M.; Morone, M. Primary benign liver lesions. Eur. J. Radiol. 2017, 95, 378–398. [Google Scholar] [CrossRef]
- Al-Azzawi, Y.; Rouanet, E.; Hendrix, R.J.; Spaho, L.; Malik, H.; Devuni, D.; Szabo, G.; Barnard, G. Segmental Distribution of Hepatocellular Carcinoma Correlates with Microvascular Invasion in Liver Explants Undergoing Transplantation. J. Cancer Epidemiol. 2019, 2019, 8534372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cagin, Y.F.; Atayan, Y.; Erdogan, M.A.; Dagtekin, F.; Colak, C. Incidence and clinical presentation of portal vein thrombosis in cirrhotic patients. Hepatobiliary Pancreat. Dis. Int. 2016, 15, 499–503. [Google Scholar] [CrossRef]
- Carr, B.I.; Guerra, V.; Donghia, R. Portal Vein Thrombosis and Markers of Inflammation in Hepatocellular Carcinoma. J. Gastrointest. Cancer 2020, 51, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Lee, S.; An, C. Problematic lesions in cirrhotic liver mimicking hepatocellular carcinoma. Eur. Radiol. 2019, 29, 5101–5110. [Google Scholar] [CrossRef]
- Dong, Y.; Teufel, A.; Trojan, J.; Berzigotti, A.; Cui, X.W.; Dietrich, C.F. Contrast enhanced ultrasound in mixed hepatocellular cholangiocarcinoma: Case series and review of the literature. Dig. Liver Dis. 2018, 50, 401–407. [Google Scholar] [CrossRef]
- Walter, D.; Ferstl, P.; Waidmann, O.; Trojan, J.; Hartmann, S.; Schnitzbauer, A.A.; Zeuzem, S.; Kraywinkel, K. Cholangiocarcinoma in Germany: Epidemiologic trends and impact of misclassification. Liver Int. 2019, 39, 316–323. [Google Scholar] [CrossRef]
- Wilson, S.R.; Burns, P.N.; Kono, Y. Contrast-Enhanced Ultrasound of Focal Liver Masses: A Success Story. Ultrasound Med. Biol 2020, 46, 1059–1070. [Google Scholar] [CrossRef]
- Brancatelli, G.; Federle, M.P.; Blachar, A.; Grazioli, L. Hemangioma in the cirrhotic liver: Diagnosis and natural history. Radiology 2001, 219, 69–74. [Google Scholar] [CrossRef]
- Abd Alkhalik Basha, M.; Abd El Aziz El Sammak, D.; El Sammak, A.A. Diagnostic efficacy of the Liver Imaging-Reporting and Data System (LI-RADS) with CT imaging in categorising small nodules (10-20 mm) detected in the cirrhotic liver at screening ultrasound. Clin. Radiol. 2017, 72, 901-e1. [Google Scholar] [CrossRef]
- Allen, B.C.; Ho, L.M.; Jaffe, T.A.; Miller, C.M.; Mazurowski, M.A.; Bashir, M.R. Comparison of Visualization Rates of LI-RADS Version 2014 Major Features with IV Gadobenate Dimeglumine or Gadoxetate Disodium in Patients at Risk for Hepatocellular Carcinoma. AJR Am. J. Roentgenol. 2018, 210, 1266–1272. [Google Scholar] [CrossRef]
- An, C.; Park, S.; Chung, Y.E.; Kim, D.Y.; Kim, S.S.; Kim, M.J.; Choi, J.Y. Curative Resection of Single Primary Hepatic Malignancy: Liver Imaging Reporting and Data System Category LR-M Portends a Worse Prognosis. AJR Am. J. Roentgenol. 2017, 209, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, L.M.; Sofue, K.; Alagiyawanna, M.; Nilmini, V.; Muir, A.J.; Choudhury, K.R.; Semelka, R.C.; Bashir, M.R. Natural history of liver imaging reporting and data system category 4 nodules in MRI. Abdom. Radiol. 2016, 41, 1758–1766. [Google Scholar] [CrossRef] [PubMed]
- Cerny, M.; Bergeron, C.; Billiard, J.S.; Murphy-Lavallée, J.; Olivié, D.; Bérubé, J.; Fan, B.; Castel, H.; Turcotte, S.; Perreault, P.; et al. LI-RADS for MR Imaging Diagnosis of Hepatocellular Carcinoma: Performance of Major and Ancillary Features. Radiology 2018, 288, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Cha, D.I.; Jang, K.M.; Kim, S.H.; Kang, T.W.; Song, K.D. Liver Imaging Reporting and Data System on CT and gadoxetic acid-enhanced MRI with diffusion-weighted imaging. Eur. Radiol. 2017, 27, 4394–4405. [Google Scholar] [CrossRef] [PubMed]
- Channual, S.; Pahwa, A.; Sayre, J.; Beckett, K.R.; Lu, D.S.-K.; Raman, S.S. Performance of LI-RADS Criteria for Diagnosis of Pathologically Proven Hepatocellular Carcinoma Using Gd-EOB-DTPA, and Comparisons with the Japan Society of Hepatology 2010 Criteria. Available online: https://archive.rsna.org/2013/13044425.html (accessed on 19 April 2022).
- Choi, S.H.; Byun, J.H.; Kim, S.Y.; Lee, S.J.; Won, H.J.; Shin, Y.M.; Kim, P.N. Liver Imaging Reporting and Data System v2014 With Gadoxetate Disodium-Enhanced Magnetic Resonance Imaging: Validation of LI-RADS Category 4 and 5 Criteria. Investig. Radiol. 2016, 51, 483–490. [Google Scholar] [CrossRef]
- Fraum, T.J.; Tsai, R.; Rohe, E.; Ludwig, D.R.; Salter, A.; Nalbantoglu, I.; Heiken, J.P.; Fowler, K.J. Differentiation of Hepatocellular Carcinoma from Other Hepatic Malignancies in Patients at Risk: Diagnostic Performance of the Liver Imaging Reporting and Data System Version 2014. Radiology 2018, 286, 158–172. [Google Scholar] [CrossRef]
- Horvat, N.; Nikolovski, I.; Long, N.; Gerst, S.; Zheng, J.; Pak, L.M.; Simpson, A.; Zheng, J.; Capanu, M.; Jarnagin, W.R.; et al. Imaging features of hepatocellular carcinoma compared to intrahepatic cholangiocarcinoma and combined tumor on MRI using liver imaging and data system (LI-RADS) version 2014. Abdom. Radiol. 2018, 43, 169–178. [Google Scholar] [CrossRef]
- Joo, I.; Lee, J.M.; Lee, S.M.; Lee, J.S.; Park, J.Y.; Han, J.K. Diagnostic accuracy of liver imaging reporting and data system (LI-RADS) v2014 for intrahepatic mass-forming cholangiocarcinomas in patients with chronic liver disease on gadoxetic acid-enhanced MRI. J. Magn. Reson. Imaging 2016, 44, 1330–1338. [Google Scholar] [CrossRef]
- Kim, B.R.; Lee, J.M.; Lee, D.H.; Yoon, J.H.; Hur, B.Y.; Suh, K.S.; Yi, N.J.; Lee, K.B.; Han, J.K. Diagnostic Performance of Gadoxetic Acid-enhanced Liver MR Imaging versus Multidetector CT in the Detection of Dysplastic Nodules and Early Hepatocellular Carcinoma. Radiology 2017, 285, 134–146. [Google Scholar] [CrossRef]
- Kim, Y.Y.; An, C.; Kim, S.; Kim, M.J. Diagnostic accuracy of prospective application of the Liver Imaging Reporting and Data System (LI-RADS) in gadoxetate-enhanced MRI. Eur. Radiol. 2018, 28, 2038–2046. [Google Scholar] [CrossRef]
- Lee, S.E.; An, C.; Hwang, S.H.; Choi, J.Y.; Han, K.; Kim, M.J. Extracellular contrast agent-enhanced MRI: 15-min delayed phase may improve the diagnostic performance for hepatocellular carcinoma in patients with chronic liver disease. Eur. Radiol. 2018, 28, 1551–1559. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Qin, J.; Guo, R.; Xie, S.; Jiang, H.; Wang, X.; Kang, Z.; Wang, J.; Shan, H. Accuracy of the diagnostic evaluation of hepatocellular carcinoma with LI-RADS. Acta Radiol. 2018, 59, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Qi, Z.; Li, H. The Utility of LI-RADS v2014 to Characterize the Nodules Detected during Hepatocarcinogenesis in HBV-Related Liver Cirrhosis: A Comparative Study of MR Imaging and Pathology. Available online: http://archive.rsna.org/2016/16019077.html (accessed on 20 April 2022).
- Ronot, M.; Fouque, O.; Esvan, M.; Lebigot, J.; Aubé, C.; Vilgrain, V. Comparison of the accuracy of AASLD and LI-RADS criteria for the non-invasive diagnosis of HCC smaller than 3 cm. J. Hepatol. 2018, 68, 715–723. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | bFLLs | mFLLs |
|---|---|---|
| n | 71 | 154 |
| Disease Entity | RNs (25) Simple Cysts (22) Hemangiomas (14) FDS (5) Abscesses (2) Hematomas (2) Echinococcal Cysts (1) | HCC (132) |
| Metastases (11) | ||
| CUP (3) CRC (2) NET (2) Lymphoma (2) Gallbladder (1) Esophageal (1) | ||
| ICC (9) | ||
| Mixed HCC/ICC (1) | ||
| Angiosarcomas (1) |
| Etiology | n | Percentage |
|---|---|---|
| Alcohol | 124 | 55.1 |
| NASH | 34 | 15.1 |
| HCV | 28 | 12.4 |
| HBV | 11 | 4.9 |
| Hemochromatosis | 7 | 3.1 |
| AIH | 4 | 1.8 |
| PSC | 4 | 1.8 |
| PBC | 4 | 1.8 |
| Other * | 2 | 0.9 |
| Idiopathic | 7 | 3.1 |
| Group | bFLLs | HCC mFLLs | Non-HCC mFLLs | p-Value |
|---|---|---|---|---|
| n | 71 | 132 | 22 | |
| Age (years) | 61 ± 11 | 67 ± 9 | 66 ± 6 | <0.001 |
| Male (%) | 63 | 86 | 68 | 0.001 |
| History of Active NHPMD (%) | 7 (9.9) | 2 (1.5) | 12 (55) | <0.001 |
| CTP Stage: A/B/C (%) | 60/30/10 | 56/36/8 | 55/45/0 | 0.45 |
| MELD-Na Score | 12.9 ± 6.5 | 12.6 ± 6.2 | 12.2 ± 7.4 | 0.69 |
| Albumin (g/L) | 33.5 ± 7.7 | 33.1 ± 6.9 | 31.0 ± 6.3 | 0.31 |
| Platelet Count (×103/μL) | 152 ± 95 | 147 ± 82 | 155 ± 96 | 0.98 |
| AFP (ng/dL) | 5.3 ± 5.8 * | 2197 ± 9093 | 55 ± 173 # | <0.001 |
| Size of the Lesion (cm) | 2.2 ± 1.7 | 4.9 ± 3.0 | 5.3 ± 3.8 | <0.001 |
| Lobar Location: Right/Left/both (%) | 41/41/18 | 56/20/24 | 32/45/23 | 0.008 |
| Ascites: n (%) | 30 (42) | 50 (38) | 11 (50) | 0.52 |
| Splenomegaly: n (%) | 38 (54) ** | 63 (48) § | 7 (32) $ | 0.24 |
| Hypoechoic Echogenicity: n (%) | 50 (70) | 95 (9) | 17 (77) | 0.82 |
| Portal Vein Thrombosis (%) | 2 (2.8) | 20 (15.2) | 3 (13.6) | 0.03 |
| Clinical Background | Prevalence of mFLLs (%) | n | Year | Author |
|---|---|---|---|---|
| Incidental detection in asymptomatic patients | 0.6 | 542 | 2016 | Choi et al. [23] |
| Patients with synchronous hematological malignancies | 33.0 | 61 | 2013 | Heller et al. [24] |
| Patients with synchronous non-hematological malignancies | 59.4 | 434 | 2021 | Safai Zadeh et al. [25] |
| Patients with liver cirrhosis | 76.6 | 282 | 2011 | Seitz et al. [17] |
| Patients with liver cirrhosis | 68.4 | 228 | 2022 | Present Study |
| Study | n | Male (%) | Imaging Modality | Final Diagnosis | ||
|---|---|---|---|---|---|---|
| HCC (%) | Non-HCC mFLLs (%) | bFLLs (%) | ||||
| Abd Alkhalik Basha et al., 2017 [39] | 55 | 58 | CT | 34 (61.8) | 2 (3.6) | 19 (34.5) |
| Allen et al., 2018 [40] | 57 | NR | MRI | 36 (63.2) | NR | 21 (36.8) |
| An et al., 2017 [41] | 225 | 77 | MRI | 218 (96.9) | 7 (3.1) | 0 |
| Burke et al., 2016 [42] | 30 | NR | MRI | 20 (66.7) | NR | 10 (33.3) |
| Cerny et al., 2018 [43] | 275 | 74 | MRI | 113 (41.1) | 10 (3.6) | 152 (55.3) |
| Cha et al., 2017 [44] | 445 | 72 | CT + MRI | 397 (89.2) | 31 (7.0) | 17 (3.8) |
| Channual et al., 2014 [45] | 131 | NR | MRI | 116 (88.5) | NR | NR |
| Choi et al., 2016 [46] | 379 | 84 | MRI | 327 (86.3) | 9 (2.4) | 43 (11.3) |
| Fraum et al., 2018 [47] | 220 | 74 | CT + MRI | 136 (61.8) | 42 (19.1) | 42 (19.1) |
| Horvat et al., 2018 [48] | 102 | 54 | MRI | 51 (50.0) | 51 (50.0) | 0 |
| Joo et al., 2016 [49] | 106 | 79 | MRI | 71 (67.0) | 35 (33.0) | 0 |
| Kim et al., 2017 [50] | 112 | 69 | CT + MRI | 75 (67.0) | 0 | 37 (33.0) |
| Kim et al., 2018 [51] | 202 | 83 | MRI | 129 (63.9) | 6 (3.0) | 67 (33.1) |
| Lee et al., 2018 [52] | 133 | 75 | MRI | 107 (80.4) | 3 (2.3) | 23 (17.3) |
| Liu et al., 2018 [53] | 297 | 86 | CT + MRI | 178 (59.9) | 13 (4.4) | 106 (35.6) |
| Qi et al., 2016 [54] | 192 | NR | MRI | 138 (71.9) | 0 | 54 (28.1) |
| Ronot et al., 2017 [55] | 595 | 81 | CT + MRI | 341 (57.3) | 8 (1.3) | NR |
| Seitz et al., 2011 [17] | 282 | 80 | CT + MRI + US + CEUS | 216 (76.6) | 21 (7.4) | 42 (14.9) |
| Present Study | 225 | 77 | CT + MRI + US + CEUS | 132 (58.7) | 22 (9.8) | 71 (31.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhyari, A.; Görg, C.; Alakhras, R.; Dietrich, C.F.; Trenker, C.; Safai Zadeh, E. HCC or Something Else? Frequency of Various Benign and Malignant Etiologies in Cirrhotic Patients with Newly Detected Focal Liver Lesions in Relation to Different Clinical and Sonographic Parameters. Diagnostics 2022, 12, 2079. https://doi.org/10.3390/diagnostics12092079
Alhyari A, Görg C, Alakhras R, Dietrich CF, Trenker C, Safai Zadeh E. HCC or Something Else? Frequency of Various Benign and Malignant Etiologies in Cirrhotic Patients with Newly Detected Focal Liver Lesions in Relation to Different Clinical and Sonographic Parameters. Diagnostics. 2022; 12(9):2079. https://doi.org/10.3390/diagnostics12092079
Chicago/Turabian StyleAlhyari, Amjad, Christian Görg, Raed Alakhras, Christoph Frank Dietrich, Corrina Trenker, and Ehsan Safai Zadeh. 2022. "HCC or Something Else? Frequency of Various Benign and Malignant Etiologies in Cirrhotic Patients with Newly Detected Focal Liver Lesions in Relation to Different Clinical and Sonographic Parameters" Diagnostics 12, no. 9: 2079. https://doi.org/10.3390/diagnostics12092079
APA StyleAlhyari, A., Görg, C., Alakhras, R., Dietrich, C. F., Trenker, C., & Safai Zadeh, E. (2022). HCC or Something Else? Frequency of Various Benign and Malignant Etiologies in Cirrhotic Patients with Newly Detected Focal Liver Lesions in Relation to Different Clinical and Sonographic Parameters. Diagnostics, 12(9), 2079. https://doi.org/10.3390/diagnostics12092079