
miR-146a-5p, miR-223-3p and miR-142-3p as Potential Predictors of Major Adverse Cardiac Events in Young Patients with Acute ST Elevation Myocardial Infarction—Added Value over Left Ventricular Myocardial Work Indices

 ,
, 
 and
and
Abstract
:1. Introduction
1.1. Myocardial Work Indices
1.2. microRNAs
2. Materials and Methods
2.1. Study Population
2.2. Echocardiography
Myocardial Work Analysis
- Global work index (GWI)—the area within the global LV pressure–strain loop (calculated from mitral valve closure to mitral valve opening), representing the total LV work performed in a single cardiac cycle.
- Global constructive work (GCW)—the myocardial work performed during the shortening of a myocardial segment in systole and during lengthening in isovolumic relaxation, representing the total work contributing to the pump function.
- Global wasted work (GWW)—the negative myocardial work performed during the lengthening of a myocardial segment in systole or during shortening in isovolumic relaxation, and which therefore does not contribute to LV ejection.
- Global work efficiency (GWE)—the sum of the constructive work in all LV segments, divided by the sum of the constructive and wasted work in all LV segments; it is expressed as a percentage: GCW/(GCW + GWW).
2.3. Blood Sample Collection and Storage
2.4. miRNA Isolation and Quantification
2.5. Coronary Angiography
2.6. Follow-Up and Outcomes
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Echocardiographic Parameters
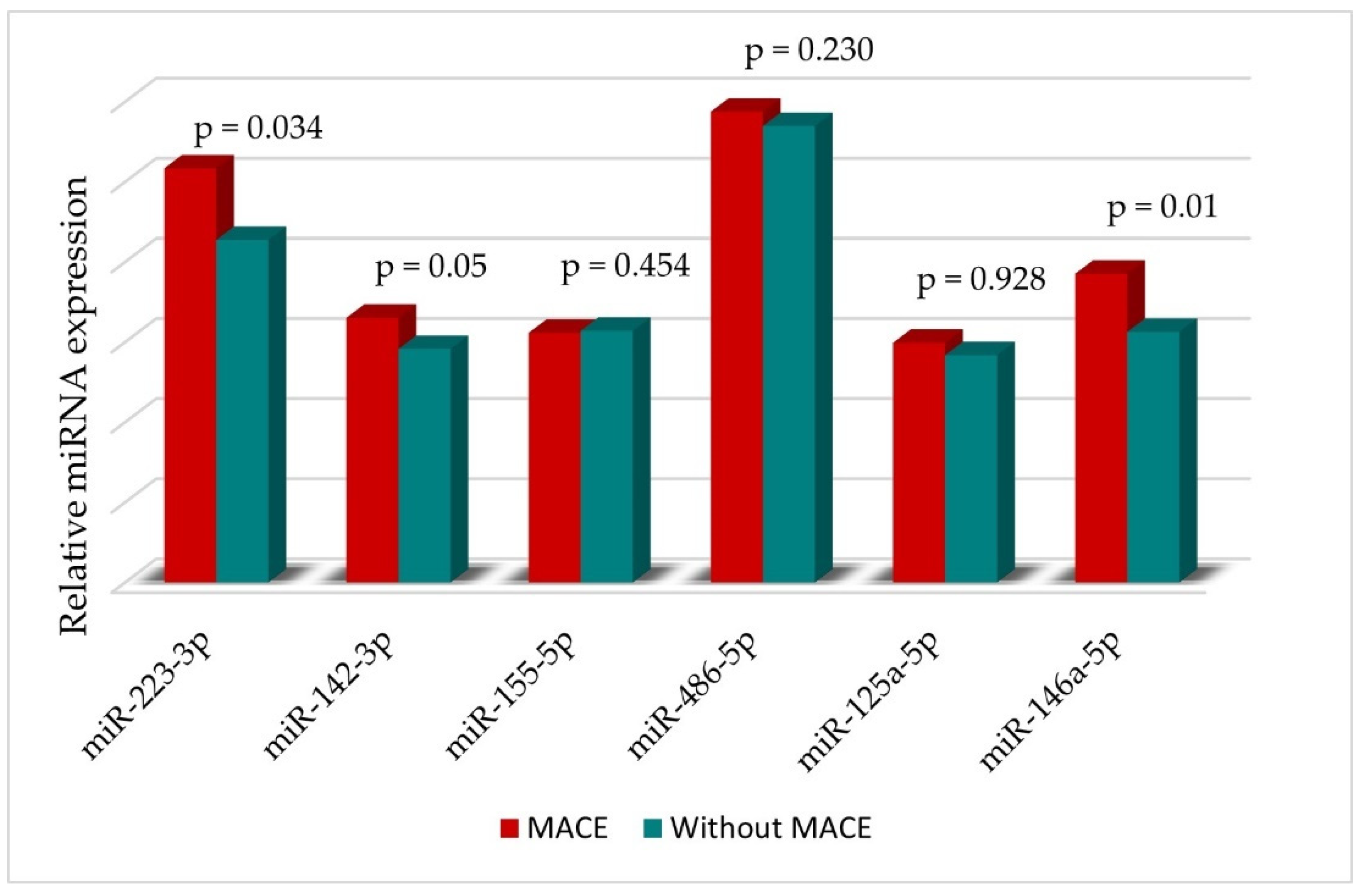
3.3. miRNAs
3.4. Clinical End Points—MACE
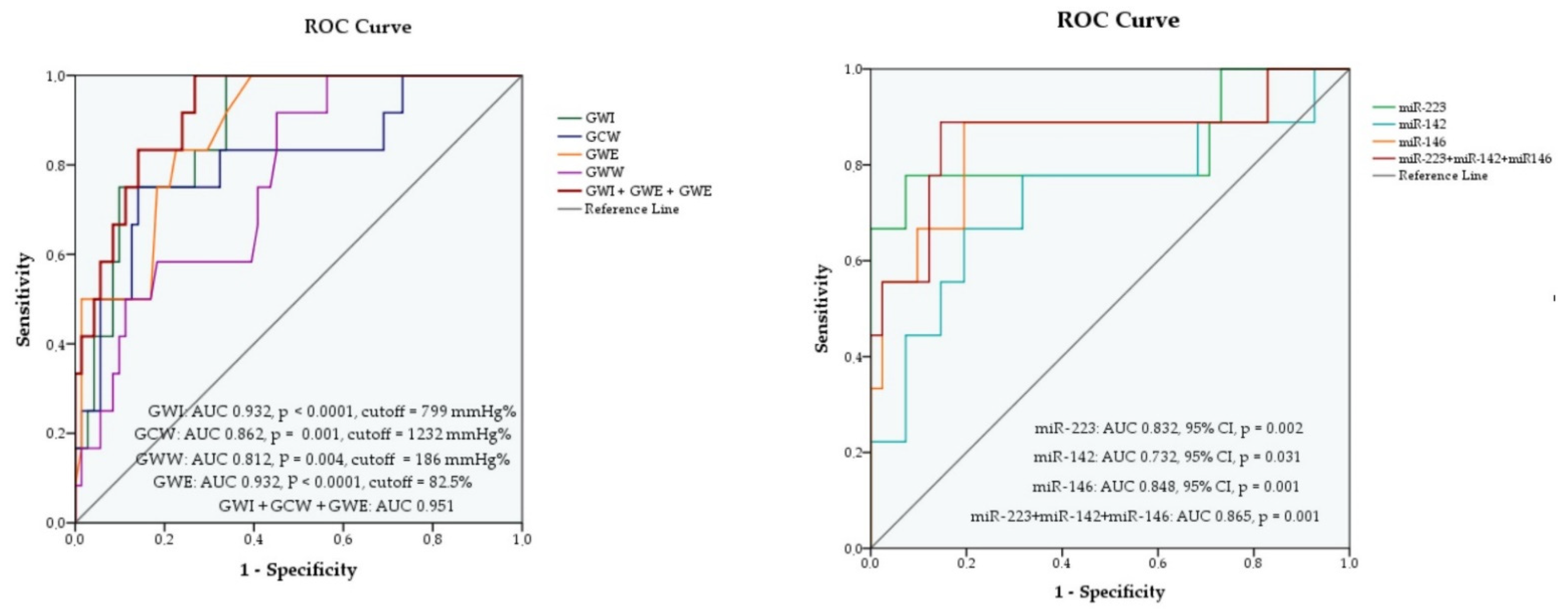
3.4.1. Myocardial Work Indices as Predictors of MACE
3.4.2. Association of miRNA Levels with Cardiovascular Outcome
3.4.3. Comparison between the Prognostic Power of Myocardial Work Indices and miRNAs
3.4.4. Incremental Prognostic Value of Circulating miRNAs over Myocardial Work Indices
4. Discussion
4.1. Myocardial Work Indices as MACE Predictors in STEMI
4.2. MIRNAs as MACE Predictors in STEMI
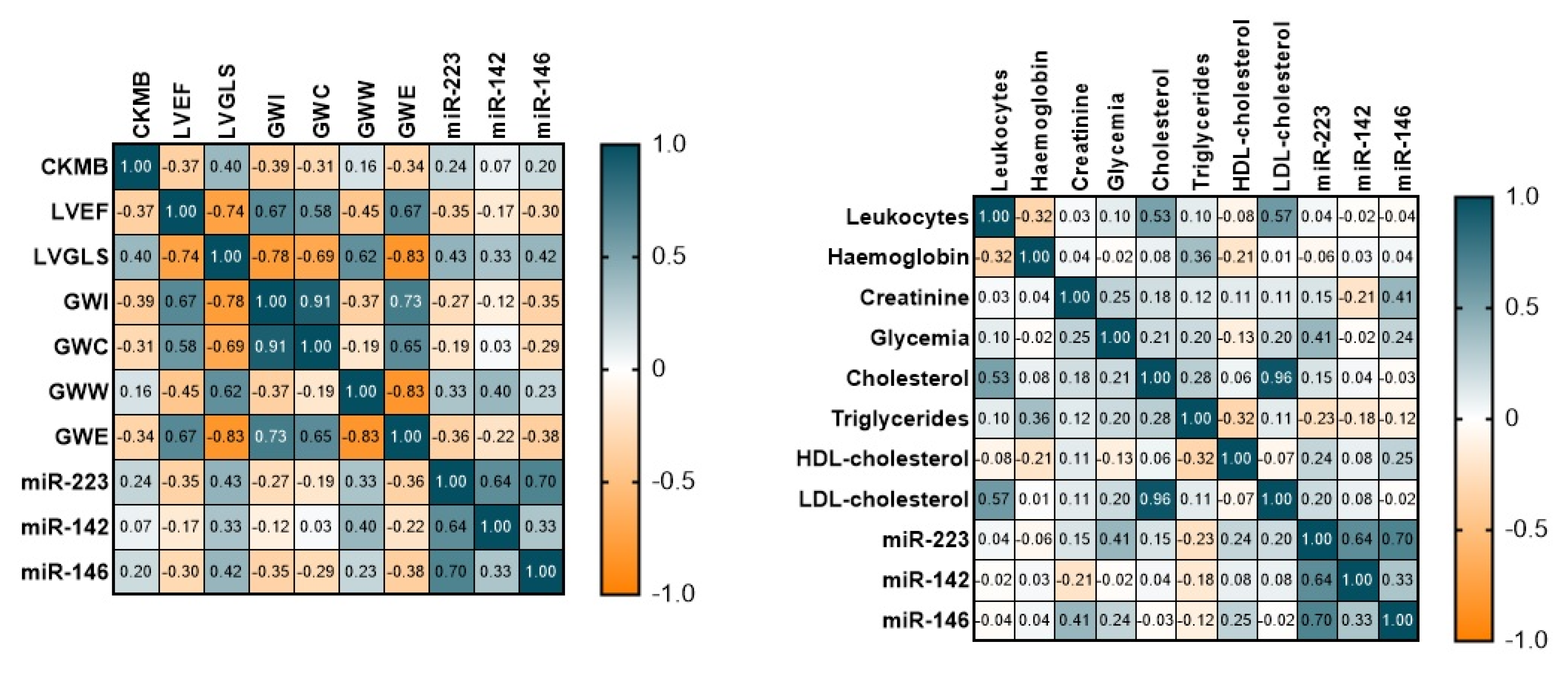
4.3. miRNAs and Myocardial Work Parameters
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACS | Acute Coronary Syndrome |
| AIC | Akaike information criterion |
| AMI | acute myocardial infarction |
| AUC | area under the curve |
| CAD | coronary artery disease |
| CI | confidence intervals |
| CK_MB | creatine kinase-MB |
| EDTA | ethylenediaminetetraacetic acid |
| GCW | global contraction work |
| GLS | global longitudinal strain |
| GWE | global work efficiency |
| GWI | global work index |
| GWW | global wasted work |
| HDL | high-density lipoprotein |
| LAD | left anterior descending artery |
| LCX | left circumflex artery |
| LDL | low-density lipoprotein |
| LV | left ventricular |
| LVEDV | LV end diastolic volume |
| LVEF | left ventricular ejection fraction |
| LVESV | LV end-systolic volume |
| MACE | major adverse cardiac events |
| MW | myocardial work |
| OR | odds ratio |
| PCI | percutaneous coronary intervention |
| RCA | right coronary artery |
| ROC | receiver operating characteristic |
| RT-PCR | reverse transcription polymerase chain reaction |
| STEMI | acute ST elevation myocardial infarction |
| WBC | white blood cells |
References
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality from Ischemic Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Nichols, M.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe--epidemiological update 2015. Eur. Heart. J. 2015, 36, 2696–2705. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Stouffer, G.A.; Kucharska-Newton, A.M.; Qamar, A.; Vaduganathan, M.; Pandey, A.; Porterfield, D.; Blankstein, R.; Rosamond, W.D.; Bhatt, D.L.; et al. Twenty Year Trends and Sex Differences in Young Adults Hospitalized with Acute Myocardial Infarction. Circulation 2019, 139, 1047–1056. [Google Scholar] [CrossRef]
- Yang, J.; Biery, D.W.; Singh, A.; Divakaran, S.; DeFilippis, E.M.; Wu, W.Y.; Klein, J.; Hainer, J.; Ramsis, M.; Natarajan, P.; et al. Risk Factors and Outcomes of Very Young Adults Who Experience Myocardial Infarction: The Partners YOUNG-MI Registry. Am. J. Med. 2020, 133, 605–612 e1. [Google Scholar]
- Divakaran, S.; Singh, A.; Biery, D.; Yang, J.; DeFilippis, E.M.; Collins, B.L.; Ramsis, M.; Qamar, A.; Hainer, J.; Klein, J.; et al. Diabetes Is Associated with Worse Long-term Outcomes in Young Adults After Myocardial Infarction: The Partners YOUNG-MI Registry. Diabetes Care 2020, 43, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Yandrapalli, S.; Nabors, C.; Goyal, A.; Aronow, W.S.; Frishman, W.H. Modifiable Risk Factors in Young Adults with First Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Li, Z.; Vittinghoff, E.; Sun, Y.; Pletcher, M.J. Trends in rate of acute myocardial infarction among patients aged <30 years. Nat. Rev. Cardiol. 2018, 15, 119. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Ni, L.; Liu, K.; Gao, X.; Yang, J.; Zhang, X.; Ye, Y.; Dong, Q.; Fu, R.; Sun, H.; et al. Clinical Characteristics, Prognosis, and Gender Disparities in Young Patients with Acute Myocardial Infarction. Front. Cardiovasc. Med. 2021, 8, 720378. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.; Backhaus, S.J.; Stiermaier, T.; Eitel, I. Prognostic utility of global longitudinal strain in myocardial infarction. World J. Cardiol. 2018, 10, 35–37. [Google Scholar] [CrossRef]
- Smiseth, O.A.; Torp, H.; Opdahl, A.; Haugaa, K.H.; Urheim, S. Myocardial strain imaging: How useful is it in clinical decision making? Eur. Heart J. 2016, 37, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Ersboll, M.; Valeur, N.; Mogensen, U.M.; Andersen, M.J.; Moller, J.E.; Hassager, C.; Sogaard, P.; Kober, L. Relationship between left ventricular longitudinal deformation and clinical heart failure during admission for acute myocardial infarction: A two-dimensional speckle-tracking study. J. Am. Soc. Echocardiogr. 2012, 25, 1280–1289. [Google Scholar] [CrossRef]
- Woo, J.S.; Kim, W.S.; Yu, T.K.; Ha, S.J.; Kim, S.Y.; Bae, J.H.; Kim, K.S. Prognostic value of serial global longitudinal strain measured by two-dimensional speckle tracking echocardiography in patients with ST-segment elevation myocardial infarction. Am. J. Cardiol. 2011, 108, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Dahle, G.O.; Stangeland, L.; Moen, C.A.; Salminen, P.R.; Haaverstad, R.; Matre, K.; Grong, K. The influence of acute unloading on left ventricular strain and strain rate by speckle tracking echocardiography in a porcine model. Am. J. Physiol. Heart Circ. Physiol. 2016, 310, H1330–H1339. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef]
- Hubert, A.; Le Rolle, V.; Leclercq, C.; Galli, E.; Samset, E.; Casset, C.; Mabo, P.; Hernandez, A.; Donal, E. Estimation of myocardial work from pressure-strain loops analysis: An experimental evaluation. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1372–1379. [Google Scholar] [CrossRef]
- Verbeke, J.; Calle, S.; Kamoen, V.; De Buyzere, M.; Timmermans, F. Prognostic value of myocardial work and global longitudinal strain in patients with heart failure and functional mitral regurgitation. Int. J. Cardiovasc. Imaging 2022, 38, 803–812. [Google Scholar] [CrossRef]
- Jain, R.; Bajwa, T.; Roemer, S.; Huisheree, H.; Allaqaband, S.Q.; Kroboth, S.; Perez Moreno, A.C.; Tajik, A.J.; Khandheria, B.K. Myocardial work assessment in severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Hedwig, F.; Nemchyna, O.; Stein, J.; Knosalla, C.; Merke, N.; Knebel, F.; Hagendorff, A.; Schoenrath, F.; Falk, V.; Knierim, J. Myocardial Work Assessment for the Prediction of Prognosis in Advanced Heart Failure. Front. Cardiovasc. Med. 2021, 8, 691611. [Google Scholar] [CrossRef]
- Boe, E.; Russell, K.; Eek, C.; Eriksen, M.; Remme, E.W.; Smiseth, O.A.; Skulstad, H. Non-invasive myocardial work index identifies acute coronary occlusion in patients with non-ST-segment elevation-acute coronary syndrome. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Lustosa, R.P.; Butcher, S.C.; van der Bijl, P.; El Mahdiui, M.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Rocha De Lorenzo, A.; Knuuti, J.; Ajmone Marsan, N.; Bax, J.J.; et al. Global Left Ventricular Myocardial Work Efficiency and Long-Term Prognosis in Patients After ST-Segment-Elevation Myocardial Infarction. Circ. Cardiovasc. Imaging 2021, 14, e012072. [Google Scholar] [CrossRef] [PubMed]
- Butcher, S.C.; Lustosa, R.P.; Abou, R.; Marsan, N.A.; Bax, J.J.; Delgado, V. Prognostic implications of left ventricular myocardial work index in patients with ST-segment elevation myocardial infarction and reduced left ventricular ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Scarlatescu, A.I.; Micheu, M.M.; Popa-Fotea, N.M.; Dorobantu, M. MicroRNAs in Acute ST Elevation Myocardial Infarction-A New Tool for Diagnosis and Prognosis: Therapeutic Implications. Int. J. Mol. Sci. 2021, 22, 4799. [Google Scholar] [CrossRef]
- Plasterk, R.H. Micro RNAs in animal development. Cell 2006, 124, 877–881. [Google Scholar] [CrossRef]
- Cavarretta, E.; Frati, G. MicroRNAs in Coronary Heart Disease: Ready to Enter the Clinical Arena? Biomed. Res. Int. 2016, 2016, 2150763. [Google Scholar] [CrossRef]
- Wang, G.K.; Zhu, J.Q.; Zhang, J.T.; Li, Q.; Li, Y.; He, J.; Qin, Y.W.; Jing, Q. Circulating microRNA: A novel potential biomarker for early diagnosis of acute myocardial infarction in humans. Eur. Heart J. 2010, 31, 659–666. [Google Scholar] [CrossRef]
- Hsu, A.; Chen, S.J.; Chang, Y.S.; Chen, H.C.; Chu, P.H. Systemic approach to identify serum microRNAs as potential biomarkers for acute myocardial infarction. Biomed. Res. Int. 2014, 2014, 418628. [Google Scholar] [CrossRef]
- Van Empel, V.P.; De Windt, L.J.; da Costa Martins, P.A. Circulating miRNAs: Reflecting or affecting cardiovascular disease? Curr. Hypertens. Rep. 2012, 14, 498–509. [Google Scholar] [CrossRef]
- Kloosterman, W.P.; Plasterk, R.H. The diverse functions of microRNAs in animal development and disease. Dev. Cell 2006, 11, 441–450. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- Gilad, S.; Meiri, E.; Yogev, Y.; Benjamin, S.; Lebanony, D.; Yerushalmi, N.; Benjamin, H.; Kushnir, M.; Cholakh, H.; Melamed, N.; et al. Serum microRNAs are promising novel biomarkers. PLoS ONE 2008, 3, e3148. [Google Scholar] [CrossRef]
- Chen, X.; Ba, Y.; Ma, L.; Cai, X.; Yin, Y.; Wang, K.; Guo, J.; Zhang, Y.; Chen, J.; Guo, X.; et al. Characterization of microRNAs in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef]
- Landry, P.; Plante, I.; Ouellet, D.L.; Perron, M.P.; Rousseau, G.; Provost, P. Existence of a microRNA pathway in anucleate platelets. Nat. Struct. Mol. Biol. 2009, 16, 961–966. [Google Scholar] [CrossRef]
- Singh, S.; de Ronde, M.W.J.; Kok, M.G.M.; Beijk, M.A.; De Winter, R.J.; van der Wal, A.C.; Sondermeijer, B.M.; Meijers, J.C.M.; Creemers, E.E.; Pinto-Sietsma, S.J. MiR-223-3p and miR-122-5p as circulating biomarkers for plaque instability. Open Heart 2020, 7, e001223. [Google Scholar] [CrossRef]
- Hromadka, M.; Motovska, Z.; Hlinomaz, O.; Kala, P.; Tousek, F.; Jarkovsky, J.; Beranova, M.; Jansky, P.; Svoboda, M.; Krepelkova, I.; et al. MiR-126-3p and MiR-223-3p as Biomarkers for Prediction of Thrombotic Risk in Patients with Acute Myocardial Infarction and Primary Angioplasty. J. Pers. Med. 2021, 11, 508. [Google Scholar] [CrossRef]
- Qin, B.; Shu, Y.; Long, L.; Li, H.; Men, X.; Feng, L.; Yang, H.; Lu, Z. MicroRNA-142-3p Induces Atherosclerosis-Associated Endothelial Cell Apoptosis by Directly Targeting Rictor. Cell. Physiol. Biochem. 2018, 47, 1589–1603. [Google Scholar] [CrossRef]
- Tang, Q.J.; Lei, H.P.; Wu, H.; Chen, J.Y.; Deng, C.Y.; Sheng, W.S.; Fu, Y.H.; Li, X.H.; Lin, Y.B.; Han, Y.L.; et al. Plasma miR-142 predicts major adverse cardiovascular events as an intermediate biomarker of dual antiplatelet therapy. Acta. Pharmacol. Sin. 2019, 40, 208–215. [Google Scholar] [CrossRef]
- Su, Q.; Lv, X.; Ye, Z.; Sun, Y.; Kong, B.; Qin, Z.; Li, L. The mechanism of miR-142-3p in coronary microembolization-induced myocardiac injury via regulating target gene IRAK-1. Cell Death Dis. 2019, 10, 61. [Google Scholar] [CrossRef]
- Bao, M.H.; Xiao, Y.; Zhang, Q.S.; Luo, H.Q.; Luo, J.; Zhao, J.; Li, G.Y.; Zeng, J.; Li, J.M. Meta-Analysis of miR-146a Polymorphisms Association with Coronary Artery Diseases and Ischemic Stroke. Int. J. Mol. Sci. 2015, 16, 14305–14317. [Google Scholar] [CrossRef]
- Roldan, V.; Arroyo, A.B.; Salloum-Asfar, S.; Manzano-Fernandez, S.; Garcia-Barbera, N.; Marin, F.; Vicente, V.; Gonzalez-Conejero, R.; Martinez, C. Prognostic role of MIR146A polymorphisms for cardiovascular events in atrial fibrillation. Thromb. Haemost. 2014, 112, 781–788. [Google Scholar] [CrossRef]
- Niculescu, L.S.; Simionescu, N.; Sanda, G.M.; Carnuta, M.G.; Stancu, C.S.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; Simionescu, M.; et al. MiR-486 and miR-92a Identified in Circulating HDL Discriminate between Stable and Vulnerable Coronary Artery Disease Patients. PLoS ONE 2015, 10, e0140958. [Google Scholar] [CrossRef]
- Yang, K.; He, Y.S.; Wang, X.Q.; Lu, L.; Chen, Q.J.; Liu, J.; Sun, Z.; Shen, W.F. MiR-146a inhibits oxidized low-density lipoprotein-induced lipid accumulation and inflammatory response via targeting toll-like receptor 4. FEBS Lett. 2011, 585, 854–860. [Google Scholar] [CrossRef]
- Cheng, H.S.; Sivachandran, N.; Lau, A.; Boudreau, E.; Zhao, J.L.; Baltimore, D.; Delgado-Olguin, P.; Cybulsky, M.I.; Fish, J.E. MicroRNA-146 represses endothelial activation by inhibiting pro-inflammatory pathways. EMBO Mol. Med. 2013, 5, 1017–1034. [Google Scholar] [CrossRef]
- Dong, S.; Xiong, W.; Yuan, J.; Li, J.; Liu, J.; Xu, X. MiRNA-146a regulates the maturation and differentiation of vascular smooth muscle cells by targeting NF-kappaB expression. Mol. Med. Rep. 2013, 8, 407–412. [Google Scholar] [CrossRef]
- Bukauskas, T.; Mickus, R.; Cereskevicius, D.; Macas, A. Value of Serum miR-23a, miR-30d, and miR-146a Biomarkers in ST-Elevation Myocardial Infarction. Med. Sci. Monit. 2019, 25, 3925–3932. [Google Scholar] [CrossRef]
- Wang, J.; Wu, Q.; Yu, J.; Cao, X.; Xu, Z. miR-125a-5p inhibits the expression of NLRP3 by targeting CCL4 in human vascular smooth muscle cells treated with ox-LDL. Exp. Ther. Med. 2019, 18, 1645–1652. [Google Scholar] [CrossRef]
- Chen, T.; Huang, Z.; Wang, L.; Wang, Y.; Wu, F.; Meng, S.; Wang, C. MicroRNA-125a-5p partly regulates the inflammatory response, lipid uptake, and ORP9 expression in oxLDL-stimulated monocyte/macrophages. Cardiovasc. Res. 2009, 83, 131–139. [Google Scholar] [CrossRef]
- Zhang, R.; Lan, C.; Pei, H.; Duan, G.; Huang, L.; Li, L. Expression of circulating miR-486 and miR-150 in patients with acute myocardial infarction. BMC Cardiovasc. Disord. 2015, 15, 51. [Google Scholar] [CrossRef]
- Du, F.; Yu, F.; Wang, Y.; Hui, Y.; Carnevale, K.; Fu, M.; Lu, H.; Fan, D. MicroRNA-155 deficiency results in decreased macrophage inflammation and attenuated atherogenesis in apolipoprotein E-deficient mice. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 759–767. [Google Scholar] [CrossRef]
- Eisenhardt, S.U.; Schmidt, Y.; Karaxha, G.; Iblher, N.; Penna, V.; Torio-Padron, N.; Stark, G.B.; Bannasch, H. Monitoring molecular changes induced by ischemia/reperfusion in human free muscle flap tissue samples. Ann. Plast. Surg. 2012, 68, 202–208. [Google Scholar] [CrossRef]
- Donners, M.M.; Wolfs, I.M.; Stoger, L.J.; van der Vorst, E.P.; Pottgens, C.C.; Heymans, S.; Schroen, B.; Gijbels, M.J.; de Winther, M.P. Hematopoietic miR155 deficiency enhances atherosclerosis and decreases plaque stability in hyperlipidemic mice. PLoS ONE 2012, 7, e35877. [Google Scholar] [CrossRef]
- Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of, Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging. 2016, 17, 412. [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Van der Bijl, P.; Kostyukevich, M.; El Mahdiui, M.; Hansen, G.; Samset, E.; Ajmone Marsan, N.; Bax, J.J.; Delgado, V. A Roadmap to Assess Myocardial Work: From Theory to Clinical Practice. JACC Cardiovasc. Imaging. 2019, 12, 2549–2554. [Google Scholar] [CrossRef]
- Mahdiui, M.E.; van der Bijl, P.; Abou, R.; de Paula Lustosa, R.; van der Geest, R.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Myocardial Work, an Echocardiographic Measure of Post Myocardial Infarct Scar on Contrast-Enhanced Cardiac Magnetic Resonance. Am. J. Cardiol. 2021, 151, 1–9. [Google Scholar] [CrossRef]
- Barbalata, T.; Moraru, O.E.; Stancu, C.S.; Devaux, Y.; Simionescu, M.; Sima, A.V.; Niculescu, L.S. Increased miR-142 Levels in Plasma and Atherosclerotic Plaques from Peripheral Artery Disease Patients with Post-Surgery Cardiovascular Events. Int. J. Mol. Sci. 2020, 21, 9600. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed]
- Poudel, I.; Tejpal, C.; Rashid, H.; Jahan, N. Major Adverse Cardiovascular Events: An Inevitable Outcome of ST-elevation myocardial infarction? A Literature Review. Cureus 2019, 11, e5280. [Google Scholar] [CrossRef]
- Guo, Y.; Yang, C.; Wang, X.; Pei, Z.; Zhu, H.; Meng, X.; Zhou, Z.; Lang, X.; Ning, S.; Zhang, R.; et al. Regional Myocardial Work Measured by Echocardiography for the Detection of Myocardial Ischemic Segments: A Comparative Study with Invasive Fractional Flow Reserve. Front. Cardiovasc. Med. 2022, 9, 813710. [Google Scholar] [CrossRef]
- Sabatino, J.; De Rosa, S.; Leo, I.; Strangio, A.; Spaccarotella, C.; Polimeni, A.; Sorrentino, S.; Di Salvo, G.; Indolfi, C. Prediction of Significant Coronary Artery Disease Through Advanced Echocardiography: Role of Non-invasive Myocardial Work. Front. Cardiovasc. Med. 2021, 8, 719603. [Google Scholar] [CrossRef]
- Lustosa, R.P.; Fortuni, F.; van der Bijl, P.; Mahdiui, M.E.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Knuuti, J.; Marsan, N.A.; Delgado, V.; Bax, J.J. Changes in Global Left Ventricular Myocardial Work Indices and Stunning Detection 3 Months After ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2021, 157, 15–21. [Google Scholar] [CrossRef]
- Meimoun, P.; Abdani, S.; Stracchi, V.; Elmkies, F.; Boulanger, J.; Botoro, T.; Zemir, H.; Clerc, J. Usefulness of Noninvasive Myocardial Work to Predict Left Ventricular Recovery and Acute Complications after Acute Anterior Myocardial Infarction Treated by Percutaneous Coronary Intervention. J. Am. Soc. Echocardiogr. 2020, 33, 1180–1190. [Google Scholar] [CrossRef]
- Navickas, R.; Gal, D.; Laucevicius, A.; Taparauskaite, A.; Zdanyte, M.; Holvoet, P. Identifying circulating microRNAs as biomarkers of cardiovascular disease: A systematic review. Cardiovasc. Res. 2016, 111, 322–337. [Google Scholar] [CrossRef]
- Solly, E.L.; Dimasi, C.G.; Bursill, C.A.; Psaltis, P.J.; Tan, J.T.M. MicroRNAs as Therapeutic Targets and Clinical Biomarkers in Atherosclerosis. J. Clin. Med. 2019, 8, 2199. [Google Scholar] [CrossRef] [PubMed]
- Barraclough, J.Y.; Joan, M.; Joglekar, M.V.; Hardikar, A.A.; Patel, S. MicroRNAs as Prognostic Markers in Acute Coronary Syndrome Patients-A Systematic Review. Cells 2019, 8, 1572. [Google Scholar] [CrossRef] [PubMed]
- Schirle, N.T.; Sheu-Gruttadauria, J.; MacRae, I.J. Structural basis for microRNA targeting. Science 2014, 346, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.E.; Hernandez, J.A.; Benito, R.; Gutierrez, N.C.; Garcia, J.L.; Hernandez-Sanchez, M.; Risueno, A.; Sarasquete, M.E.; Ferminan, E.; Fisac, R.; et al. Molecular characterization of chronic lymphocytic leukemia patients with a high number of losses in 13q14. PLoS ONE 2012, 7, e48485. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.; Qin, S.; Li, W.; Wu, W.; Yang, J.; Chu, M.; Li, X.; Huo, Y.; Schaer, G.L.; Wang, S.; et al. An Endocrine Genetic Signal Between Blood Cells and Vascular Smooth Muscle Cells: Role of MicroRNA-223 in Smooth Muscle Function and Atherogenesis. J. Am. Coll. Cardiol. 2015, 65, 2526–2537. [Google Scholar] [CrossRef]
- Willeit, P.; Zampetaki, A.; Dudek, K.; Kaudewitz, D.; King, A.; Kirkby, N.S.; Crosby-Nwaobi, R.; Prokopi, M.; Drozdov, I.; Langley, S.R.; et al. Circulating microRNAs as novel biomarkers for platelet activation. Circ. Res. 2013, 112, 595–600. [Google Scholar] [CrossRef]
- Barbalata, T.; Zhang, L.; Dulceanu, M.D.; Stancu, C.S.; Devaux, Y.; Sima, A.V.; Niculescu, L.S. Regulation of microRNAs in high-fat diet induced hyperlipidemic hamsters. Sci. Rep. 2020, 10, 20549. [Google Scholar] [CrossRef] [PubMed]
- Simionescu, N.; Niculescu, L.S.; Carnuta, M.G.; Sanda, G.M.; Stancu, C.S.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; Simionescu, M.; et al. Hyperglycemia Determines Increased Specific MicroRNAs Levels in Sera and HDL of Acute Coronary Syndrome Patients and Stimulates MicroRNAs Production in Human Macrophages. PLoS ONE 2016, 11, e0161201. [Google Scholar]
- Schulte, C.; Molz, S.; Appelbaum, S.; Karakas, M.; Ojeda, F.; Lau, D.M.; Hartmann, T.; Lackner, K.J.; Westermann, D.; Schnabel, R.B.; et al. miRNA-197 and miRNA-223 Predict Cardiovascular Death in a Cohort of Patients with Symptomatic Coronary Artery Disease. PLoS ONE 2015, 10, e0145930. [Google Scholar]
- Guo, J.F.; Zhang, Y.; Zheng, Q.X.; Zhang, Y.; Zhou, H.H.; Cui, L.M. Association between elevated plasma microRNA-223 content and severity of coronary heart disease. Scand. J. Clin. Lab. Investig. 2018, 78, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Raitoharju, E.; Lyytikainen, L.P.; Levula, M.; Oksala, N.; Mennander, A.; Tarkka, M.; Klopp, N.; Illig, T.; Kahonen, M.; Karhunen, P.J.; et al. miR-21, miR-210, miR-34a, and miR-146a/b are up-regulated in human atherosclerotic plaques in the Tampere Vascular Study. Atherosclerosis 2011, 219, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Satoh, M.; Minami, Y.; Tabuchi, T.; Itoh, T.; Nakamura, M. Expression of miR-146a/b is associated with the Toll-like receptor 4 signal in coronary artery disease: Effect of renin-angiotensin system blockade and statins on miRNA-146a/b and Toll-like receptor 4 levels. Clin. Sci. 2010, 119, 395–405. [Google Scholar] [CrossRef]
- Oerlemans, M.I.; Mosterd, A.; Dekker, M.S.; de Vrey, E.A.; van Mil, A.; Pasterkamp, G.; Doevendans, P.A.; Hoes, A.W.; Sluijter, J.P. Early assessment of acute coronary syndromes in the emergency department: The potential diagnostic value of circulating microRNAs. EMBO Mol. Med. 2012, 4, 1176–1185. [Google Scholar] [CrossRef]
- Diehl, P.; Fricke, A.; Sander, L.; Stamm, J.; Bassler, N.; Htun, N.; Ziemann, M.; Helbing, T.; El-Osta, A.; Jowett, J.B.; et al. Microparticles: Major transport vehicles for distinct microRNAs in circulation. Cardiovasc. Res. 2012, 93, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Xue, T.; Pan, Q.; Hu, Y.; Wu, Q.; Liu, Q.; Wang, X.; Liu, A.; Liu, J.; Zhu, H.; et al. MicroRNA-146a Serves as a Biomarker for Adverse Prognosis of ST-Segment Elevation Myocardial Infarction. Cardiovasc. Ther. 2021, 2021, 2923441. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population (n = 50) | MACE (n = 9) | Without MACE (n = 41) | p Value | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Age (years) | 44.7 ± 5.62 | 44 ± 3.78 | 45 ± 5.98 | 0.99 |
| Systolic blood pressure (mmHg) | 119.54 ± 16.66 | 120.44 ± 20.35 | 119.34 ± 16.03 | 0.859 |
| Cardiovascular risk factors | ||||
| Smoking | 86% | 77.8% | 87% | 0.370 |
| Obesity | 22% | 0% | 24.2% | 0.109 |
| Hypertension | 46% | 33.3% | 48.8% | 0.321 |
| Dyslipidaemia | 75.6% | 77.8% | 82.9% | 0.517 |
| Diabetes | 17.1% | 11.1% | 12.2% | 0.707 |
| Metabolic syndrome | 12.2% | 40% | 17.6% | 0.248 |
| Clinical presentation | ||||
| Killip class ≥2 | 17% | 77.7% | 4.8% | <0.0001 |
| Angiographic characteristics | ||||
| LAD | 48% | 77.8% | 41.5% | 0.069 |
| RCA | 48% | 77.8% | 41.5% | 0.67 |
| LCX | 24% | 0% | 29.3% | 0.092 |
| Multivessel CAD | 34.6% | 22.2% | 77.8% | 0.459 |
| Occluded artery | 53.8% | 66.7% | 33.3% | 0.713 |
| Symptom to balloon time | 6.6 ± 5.31 | 7.5 ± 5.44 | 6.55 ± 7.26 | 0.692 |
| Laboratory characteristics | ||||
| WBC count, × 103/mm3 | 11,260 ± 3628 | 16,088.89 ± 3417.39 | 13,807 ± 1711.6 | 0.695 |
| Haemoglobin, g/dL | 14.06 ± 1.44 | 13.41 ± 1.24 | 14.02 ± 2.81 | 0.411 |
| Creatinine (mg/dL) | 0.83 ± 0.23 | 0.90 ± 0.40 | 0.82 ± 0.17 | 0.38 |
| Glycaemia (mg/dL) | 118.02 ± 38.62 | 136.22 ± 48.41 | 108.69 ± 33.36 | 0.047 |
| Cholesterol (mg/dL) | 217.21 ± 64.36 | 199.40 ± 67.15 | 224.08 ± 52.61 | 0.347 |
| Triglycerides (mg/dL) | 202.37 ± 181.288 | 125.47 ± 72.66 | 151.61 ± 71.65 | 0.321 |
| HDL-cholesterol | 28.08 ± 11.95 | 26.47 ± 12.30 | 28.47 ± 12.01 | 0.482 |
| LDL-cholesterol | 159.30 ± 53.95 | 147.84 ± 63.52 | 162.09 ± 51.69 | 0.658 |
| Peak CK-MB (U/L) | 251.58 ± 211.26 | 479.67 ± 296.824 | 198.00 ± 144.125 | 0.022 |
| Population | MACE (n = 9) | Without MACE (n = 41) | p Value | |
|---|---|---|---|---|
| 2D LVEDV (mL) | 102.74 ± 24.54 | 118.55 ± 29.43 | 99.26 ± 22.27 | 0.031 |
| 2D LVEDV (mL/mp) | 53.97 ± 12.6 | 64.18 ± 13.91 | 51.75 ± 11.28 | 0.06 |
| 2D LVESV (mL) | 59.72 ± 20.91 | 81.77 ± 25.36 | 54.87 ± 16.55 | 0.013 |
| 2D LVESV (mL/mp) | 59.72 ± 20.91 | 81.77 ± 25.36 | 54.87 ± 16.55 | 0.013 |
| 2D EF (%) | 41.94 ± 7.07 | 32.88 ± 5.79 | 43 ± 6.6 | <0.0001 |
| 3D LVEDV (mL) | 113.46 ± 24.46 | 127.66 ± 28.48 | 110.34 ± 22.7 | 0.053 |
| 3D LVEDV (ml/mp) | 59.77 ± 13.02 | 69.24 ± 13.45 | 57.69 ± 12.36 | 0.016 |
| 3D LVESV (mL) | 65.74 ± 21.15 | 87 ± 25.91 | 61.07 ± 17.02 | 0.001 |
| 3D LVESV (mL/mp) | 34.67 ± 11.34 | 47.13 ± 12.73 | 31.93 ± 9.08 | <0.0001 |
| 3D LVEF (%) | 40.02 ± 8.05 | 33 ± 6.55 | 45.24 ± 6.5 | <0.0001 |
| LV GLS | −12.93 ± 2.2 | −8.85 ± 1.58 | −13.8 ± 2.8 | <0.0001 |
| LV mechanical dispersion | 72.57 ± 26.49 | 93.11 ± 29.36 | 68.06 ± 23.9 | 0.009 |
| E/e’ (LV filling pressure) | 8.2 ± 2.92 | 10.68 ± 2.01 | 7.59 ± 2.03 | <0.0001 |
| Myocardial work indices | ||||
| LV GWI, mmHg% | 1089.66 ± 318.97 | 1167.07 ± 295.67 | 737 ± 124.24 | <0.0001 |
| LV GCW, mmHg% | 1430.54 ± 325.37 | 1499.68 ± 304.01 | 1115.55 ± 224.06 | 0.001 |
| LV GWW, mmHg% | 193.14 ± 105.84 | 172.75 ± 96.3 | 286 ± 102.07 | 0.003 |
| LV GWE, % | 86.12 ± 6.55 | 87.95 ± 5.53 | 77.77 ± 3.8 | <0.0001 |
| p Value | Statistic log Likelihood Ratio | AIC | C-Statistic | Likelihood Ratio Test | |
|---|---|---|---|---|---|
| Model 1 (GWI + GCW + GWE) | p < 0.0001 | 27.577 | 44.07 | 0.938 (0.884–0.991) | |
| +miR 223-3p | p < 0.0001 | 33.064 | 40.53 | 0.9504 (0.909–0.991) | 0.0186 |
| +miR 142-3p | p = 0.0024 | 35.027 | 38.11 | 0.9504 (0.905–0.995) | 0.0048 |
| +miR 146a-5p | p < 0.0001 | 34.674 | 38.58 | 0.9603 (0.932–0.988) | 0.0062 |
| +miR 223-3p + miR 142-3p | p < 0.0001 | 37.049 | 38 | 0.9553 (0.9165–0.9942) | 0.0067 |
| +miR 142-3p + miR 146a-5p | p < 0.0001 | 42.719 | 31.19 | 0.975 (0.949–1.001)) | 0.0002 |
| +miR 223-3p + miR 146a-5p | p < 0.0001 | 34.934 | 40 | 0.960 (0.9329–0.9877) | 0.0216 |
| +miR 223 + miR-142 + miR-146 | p < 0.0001 | 44.068 | 31 | 0.9777 (0.952–1.003) | 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scărlătescu, A.I.; Barbălată, T.; Sima, A.V.; Stancu, C.; Niculescu, L.Ș.; Micheu, M.M. miR-146a-5p, miR-223-3p and miR-142-3p as Potential Predictors of Major Adverse Cardiac Events in Young Patients with Acute ST Elevation Myocardial Infarction—Added Value over Left Ventricular Myocardial Work Indices. Diagnostics 2022, 12, 1946. https://doi.org/10.3390/diagnostics12081946
Scărlătescu AI, Barbălată T, Sima AV, Stancu C, Niculescu LȘ, Micheu MM. miR-146a-5p, miR-223-3p and miR-142-3p as Potential Predictors of Major Adverse Cardiac Events in Young Patients with Acute ST Elevation Myocardial Infarction—Added Value over Left Ventricular Myocardial Work Indices. Diagnostics. 2022; 12(8):1946. https://doi.org/10.3390/diagnostics12081946
Chicago/Turabian StyleScărlătescu, Alina Ioana, Teodora Barbălată, Anca Volumnia Sima, Camelia Stancu, Loredan Ștefan Niculescu, and Miruna Mihaela Micheu. 2022. "miR-146a-5p, miR-223-3p and miR-142-3p as Potential Predictors of Major Adverse Cardiac Events in Young Patients with Acute ST Elevation Myocardial Infarction—Added Value over Left Ventricular Myocardial Work Indices" Diagnostics 12, no. 8: 1946. https://doi.org/10.3390/diagnostics12081946
APA StyleScărlătescu, A. I., Barbălată, T., Sima, A. V., Stancu, C., Niculescu, L. Ș., & Micheu, M. M. (2022). miR-146a-5p, miR-223-3p and miR-142-3p as Potential Predictors of Major Adverse Cardiac Events in Young Patients with Acute ST Elevation Myocardial Infarction—Added Value over Left Ventricular Myocardial Work Indices. Diagnostics, 12(8), 1946. https://doi.org/10.3390/diagnostics12081946