
Diagnostic Value of Fully Automated Artificial Intelligence Powered Coronary Artery Calcium Scoring from 18F-FDG PET/CT

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Material and Methods
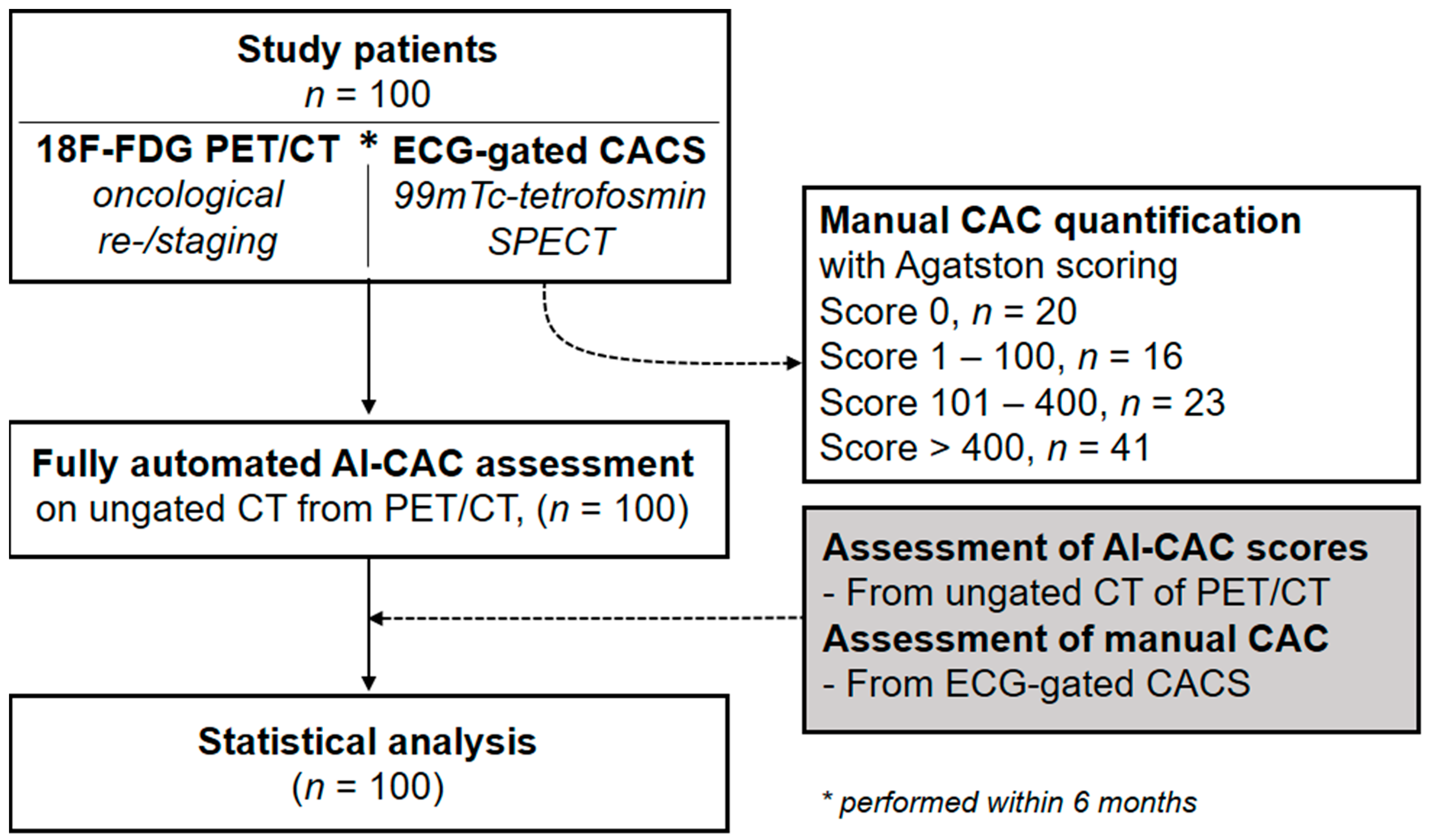
2.1. Study Population and Study Design
2.2. Whole Body 18F-FDG PET/CT Including Ungated CT
2.3. Fully Automated AI-CAC Scoring
2.4. Statistical Analysis
3. Results
3.1. Diagnostic Accuracy of AI-CACS for the Detection of Coronary Calcifications
3.2. Quantitative Agreement of AI-CACS with Manual CACS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| CAC | Coronary artery calcium |
| CACS | Coronary artery calcium scoring |
| CHD | Coronary heart disease |
| CT | Computed tomography |
| DL | Deep-learning |
| F18-FDG | F18-Fluorodeoxyglucose |
| MPI | Myocardial perfusion imaging |
| PET | Positron emission tomography |
| SPECT | Single-photon emission computed tomography |
| SUVmax | Maximum standardized uptake value |
References
- Haider, A.; Bengs, S.; Schade, K.; Wijnen, W.J.; Portmann, A.; Etter, D.; Fröhlich, S.; Warnock, G.I.; Treyer, V.; Burger, I.A.; et al. Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT. JCM 2020, 9, 2279. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, K.M.; Deng, L.; Bluethmann, S.M.; Zhou, S.; Trifiletti, D.M.; Jiang, C.; Kelly, S.; Zaorsky, N.G. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur. Heart J. 2019, 40, 3889–3897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, A.W.; Dardari, Z.A.; Blumenthal, R.S.; Dzaye, O.; Obisesan, O.H.; Uddin, S.M.I.; Nasir, K.; Blankstein, R.; Budoff, M.J.; Mortensen, M.B.; et al. Very High Coronary Artery Calcium (≥1000) and Association with Cardiovascular Disease Events, Non–Cardiovascular Disease Outcomes, and Mortality: Results from MESA. Circulation 2021, 143, 1571–1583. [Google Scholar] [CrossRef] [PubMed]
- Clerc, O.F.; Fuchs, T.A.; Stehli, J.; Benz, D.C.; Gräni, C.; Messerli, M.; Giannopoulos, A.A.; Buechel, R.R.; Lüscher, T.F.; Pazhenkottil, A.P.; et al. Non-invasive screening for coronary artery disease in asymptomatic diabetic patients: A systematic review and meta-analysis of randomised controlled trials. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 838–846. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Ulzheimer, S.; Halliburton, S.S.; Shanneik, K.; White, R.D.; Kalender, W.A. Coronary Artery Calcium: A Multi-institutional, Multimanufacturer International Standard for Quantification at Cardiac CT. Radiology 2007, 243, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Messerli, M.; Rengier, F.; Desbiolles, L.; Ehl, N.F.; Bauer, R.W.; Leschka, S.; Alkadhi, H.; Wildermuth, S.; Nähle, C.P. Impact of Advanced Modeled Iterative Reconstruction on Coronary Artery Calcium Quantification. Acad. Radiol. 2016, 23, 1506–1512. [Google Scholar] [CrossRef]
- Gebhard, C.; Fiechter, M.; Fuchs, T.A.; Ghadri, J.R.; Herzog, B.A.; Kuhn, F.; Stehli, J.; Müller, E.; Kazakauskaite, E.; Gaemperli, O.; et al. Coronary artery calcium scoring: Influence of adaptive statistical iterative reconstruction using 64-MDCT. Int. J. Cardiol. 2013, 167, 2932–2937. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.C.; Abbas, A.; Tirr, E.; Alam, S.; Nicol, E.; Shambrook, J.; Schmitt, M.; Hughes, G.M.; Stirrup, J.; Holloway, B.; et al. Reporting incidental coronary, aortic valve and cardiac calcification on non-gated thoracic computed tomography, a consensus statement from the BSCI/BSCCT and BSTI. BJR 2021, 94, 20200894. [Google Scholar] [CrossRef]
- Schwyzer, M.; Martini, K.; Benz, D.C.; Burger, I.A.; Ferraro, D.A.; Kudura, K.; Treyer, V.; von Schulthess, G.K.; Kaufmann, P.A.; Huellner, M.W.; et al. Artificial intelligence for detecting small FDG-positive lung nodules in digital PET/CT: Impact of image reconstructions on diagnostic performance. Eur. Radiol. 2020, 30, 2031–2040. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Winkel, D.J.; Suryanarayana, V.R.; Ali, A.M.; Görich, J.; Buß, S.J.; Mendoza, A.; Schwemmer, C.; Sharma, P.; Schoepf, U.J.; Rapaka, S. Deep learning for vessel-specific coronary artery calcium scoring: Validation on a multi-centre dataset. Eur. Heart J.-Cardiovasc. Imaging 2021, 23, 846–854. [Google Scholar] [CrossRef]
- Eng, D.; Chute, C.; Khandwala, N.; Rajpurkar, P.; Long, J.; Shleifer, S.; Khalaf, M.H.; Sandhu, A.T.; Rodriguez, F.; Maron, D.J.; et al. Automated coronary calcium scoring using deep learning with multicenter external validation. npj Digit. Med. 2021, 4, 88. [Google Scholar] [CrossRef]
- van Velzen, S.G.M.; Lessmann, N.; Velthuis, B.K.; Bank, I.E.M.; Bongard, D.V.D.; Leiner, T.; de Jong, P.A.; Veldhuis, W.B.; Correa, A.; Terry, J.G.; et al. Deep Learning for Automatic Calcium Scoring in CT: Validation Using Multiple Cardiac CT and Chest CT Protocols. Radiology 2020, 295, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Vonder, M.; Zheng, S.; Dorrius, M.D.; van der Aalst, C.M.; de Koning, H.J.; Yi, J.; Yu, D.; Gratama, J.W.C.; Kuijpers, D.; Oudkerk, M. Deep Learning for Automatic Calcium Scoring in Population-Based Cardiovascular Screening. JACC Cardiovasc. Imaging 2021, 15, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Fiechter, M.; Roggo, A.; A Burger, I.; Bengs, S.; Treyer, V.; Becker, A.; Marȩdziak, M.; Haider, A.; Portmann, A.; Messerli, M.; et al. Association between resting amygdalar activity and abnormal cardiac function in women and men: A retrospective cohort study. Eur. Heart J.-Cardiovasc. Imaging 2019, 20, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Gräni, C.; Vontobel, J.; Benz, D.C.; Bacanovic, S.; Giannopoulos, A.A.; Messerli, M.; Grossmann, M.; Gebhard, C.; Pazhenkottil, A.P.; Gaemperli, O.; et al. Ultra-low-dose coronary artery calcium scoring using novel scoring thresholds for low tube voltage protocols—A pilot study. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1362–1371. [Google Scholar] [CrossRef]
- Lee, J.-G.; Kim, H.; Kang, H.; Koo, H.J.; Kang, J.-W.; Kim, Y.-H.; Yang, D.H. Fully Automatic Coronary Calcium Score Software Empowered by Artificial Intelligence Technology: Validation Study Using Three CT Cohorts. Korean J. Radiol. 2021, 22, 1764. [Google Scholar] [CrossRef] [PubMed]
- Sartoretti, T.; Gennari, A.G.; Sartoretti, E.; Skawran, S.; Maurer, A.; Buechel, R.R.; Messerli, M. Fully automated deep learning powered calcium scoring in patients undergoing myocardial perfusion imaging. J. Nucl. Cardiol. 2022. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiles, C.; Duan, F.; Gladish, G.; Ravenel, J.G.; Baginski, S.G.; Snyder, B.; Demello, S.; Desjardins, S.S.; Munden, R.F. Association of Coronary Artery Calcification and Mortality in the National Lung Screening Trial: A Comparison of Three Scoring Methods. Radiology 2015, 276, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Takx, R.A.; De Jong, P.; Leiner, T.; Oudkerk, M.; De Koning, H.; Mol, C.; Viergever, M.; Isgum, I. Automated Coronary Artery Calcification Scoring in Non-Gated Chest CT: Agreement and Reliability. PLoS ONE 2014, 9, e91239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mylonas, I.; Kazmi, M.; Fuller, L.; Dekemp, R.A.; Yam, Y.; Chen, L.; Beanlands, R.S.; Chow, B.J.W. Measuring coronary artery calcification using positron emission tomography-computed tomography attenuation correction images. Eur. Heart J.-Cardiovasc. Imaging 2012, 13, 786–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, C.; Vonder, M.; Pelgrim, G.J.; Rook, M.; Xie, X.; Alsurayhi, A.; van Ooijen, P.M.; van Bolhuis, J.N.; Oudkerk, M.; Dorrius, M.; et al. High-pitch dual-source CT for coronary artery calcium scoring: A head-to-head comparison of non-triggered chest versus triggered cardiac acquisition. J. Cardiovasc. Comput. Tomogr. 2021, 15, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Fan, R.; Shi, X.; Qian, Y.; Wang, Y.; Fan, L.; Chen, R.; Xiao, Y.; Liu, S. Optimized categorization algorithm of coronary artery calcification score on non-gated chest low-dose CT screening using iterative model reconstruction technique. Clin. Imaging 2018, 52, 287–291. [Google Scholar] [CrossRef]
- Yang, G.; Chen, Y.; Ning, X.; Sun, Q.; Shu, H.; Coatrieux, J.-L. Automatic coronary calcium scoring using noncontrast and contrast CT images. Med. Phys. 2016, 43, 2174. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female/Male | 34/66 |
|---|---|
| Age, years | 66 ± 11.4 (32–91) |
| Weight, kg | 74.2 ± 16.5 (46.8–140.0) |
| Height, cm | 169.8 ± 9.6 (135–200) |
| BMI, kg/m2 | 25.6 ± 5.2 (17.2–47.3) |
| Primary Tumor, n (%) | |
| Head and neck cancer | 11% |
| Lung or pleural cancer | 12% |
| Rectal or colon cancer | 13% |
| Esophageal cancer | 20% |
| Liver tumor | 5% |
| Breast cancer | 7% |
| Pancreatic and biliary cancer | 8% |
| Lymphoma | 4% |
| Others | 20% |
| Per Patient | Per Coronary Artery | ||||
|---|---|---|---|---|---|
| All Patients | LM | LAD | RCX | RCA | |
| Sensitivity | 85.0% (77.2–92.8%) | 74.5% (62.5–86.5%) | 82.0% (73.4–91.0%) | 64.2% (51.2–77.1%) | 61.7% (49.4–74.0%) |
| Specificity | 90.0% (76.9–100%) | 79.6% (68.3–90.9%) | 100% (100–100%) | 95.7% (90.0–100%) | 95.0% (88.2–100%) |
| Diagnostic accuracy | 86.0% (77.6–92.1%) | 77.0% (67.5–84.8%) | 87.0% (78.8–92.9%) | 79.0% (69.7–86.5%) | 75.0% (65.3–83.1%) |
| PPV | 97.1% (93.2–100%) | 79.2% (67.7–90.7%) | 100% (100–100%) | 94.4% (87.0–100%) | 94.9% (88.0–100%) |
| NPV | 60.0% (42.5–77.5%) | 75.0% (63.2–86.8%) | 67.5% (53.0–82.0%) | 70.3% (59.1–81.5%) | 62.3% (50.1–74.4%) |
| Total, n | 100 | 100 | 100 | 100 | 100 |
| True positive, n | 68 | 38 | 60 | 34 | 37 |
| False negative, n | 12 | 13 | 13 | 19 | 23 |
| True negative, n | 18 | 39 | 27 | 45 | 38 |
| False positive, n | 2 | 10 | 0 | 2 | 2 |
| Manual CACS | AI-CACS | Total | Underestimation a | Overestimation a | Concordance a | |||
|---|---|---|---|---|---|---|---|---|
| 0 | 1–100 | 101–400 | >400 | |||||
| 0 | 18 | 2 | 0 | 0 | 20 | - | 2 (10.0%) | 18 (90.0%) |
| 1–100 | 11 | 5 | 0 | 0 | 16 | 11 (68.8%) | 0 | 5 (31.2%) |
| 101–400 | 1 | 17 | 5 | 0 | 23 | 18 (78.3%) | 0 | 5 (21.7%) |
| >400 | 0 | 4 | 9 | 28 | 41 | 13 (31.7%) | - | 28 (68.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morf, C.; Sartoretti, T.; Gennari, A.G.; Maurer, A.; Skawran, S.; Giannopoulos, A.A.; Sartoretti, E.; Schwyzer, M.; Curioni-Fontecedro, A.; Gebhard, C.; et al. Diagnostic Value of Fully Automated Artificial Intelligence Powered Coronary Artery Calcium Scoring from 18F-FDG PET/CT. Diagnostics 2022, 12, 1876. https://doi.org/10.3390/diagnostics12081876
Morf C, Sartoretti T, Gennari AG, Maurer A, Skawran S, Giannopoulos AA, Sartoretti E, Schwyzer M, Curioni-Fontecedro A, Gebhard C, et al. Diagnostic Value of Fully Automated Artificial Intelligence Powered Coronary Artery Calcium Scoring from 18F-FDG PET/CT. Diagnostics. 2022; 12(8):1876. https://doi.org/10.3390/diagnostics12081876
Chicago/Turabian StyleMorf, Claudia, Thomas Sartoretti, Antonio G. Gennari, Alexander Maurer, Stephan Skawran, Andreas A. Giannopoulos, Elisabeth Sartoretti, Moritz Schwyzer, Alessandra Curioni-Fontecedro, Catherine Gebhard, and et al. 2022. "Diagnostic Value of Fully Automated Artificial Intelligence Powered Coronary Artery Calcium Scoring from 18F-FDG PET/CT" Diagnostics 12, no. 8: 1876. https://doi.org/10.3390/diagnostics12081876
APA StyleMorf, C., Sartoretti, T., Gennari, A. G., Maurer, A., Skawran, S., Giannopoulos, A. A., Sartoretti, E., Schwyzer, M., Curioni-Fontecedro, A., Gebhard, C., Buechel, R. R., Kaufmann, P. A., Huellner, M. W., & Messerli, M. (2022). Diagnostic Value of Fully Automated Artificial Intelligence Powered Coronary Artery Calcium Scoring from 18F-FDG PET/CT. Diagnostics, 12(8), 1876. https://doi.org/10.3390/diagnostics12081876