
Effects of Locally Delivered Minocycline Microspheres in Postmenopausal Female Patients with Periodontitis: A Clinical and Microbiological Study


 ,
,  , ,
, , 
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Slot, D.E.; Valkenburg, C.; Van der Weijden, G. Mechanical plaque removal of periodontal maintenance patients: A systematic review and network meta-analysis. J. Clin. Periodontol. 2020, 47, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Sedghi, L.M.; Bacino, M.; Kapila, Y.L. Periodontal disease: The good, the bad and the unknown. Front. Cell Infect. Microbiol. 2021, 11, 766944. [Google Scholar] [CrossRef]
- Bartold, P.M.; Van Dyke, T.E. Periodontitis: A host-mediated disruption of microbial homeostasis. Unlearning learned concepts. Periodontol. 2000 2013, 62, 203–217. [Google Scholar] [CrossRef] [Green Version]
- Ahmed Zaki, A. The new classification of periodontal diseases. BDJ Team 2020, 7, 32–33. [Google Scholar] [CrossRef]
- Twardowski, S.E.; Wactawski-Wende, J. Relationship between periodontal disease, tooth loss, and osteoporosis. In Marcus and Feldman’s Osteoporosis, 5th ed.; Dempster, D., Cauley, J., Bouxsein, M., Cosman, F., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2021; pp. 1381–1392. [Google Scholar]
- Levin, V.A.; Jiang, X.; Kagan, R. Estrogen therapy for osteoporosis in the modern era. Osteoporos. Int. 2018, 29, 1049–1055. [Google Scholar] [CrossRef]
- Rachner, T.D.; Khosla, S.; Hofbauer, L.C. Osteoporosis: Now and the future. Lancet 2011, 377, 1276–1287. [Google Scholar] [CrossRef] [Green Version]
- Guss, J.D.; Horsfield, M.W.; Fontenele, F.F.; Sandoval, T.N.; Luna, M.; Apoorva, F.; Lima, S.F.; Bicalho, R.C.; Singh, A.; Ley, R.E.; et al. Alterations to the gut microbiome impair bone strength and tissue material properties. J. Bone Miner. Res. 2017, 32, 1343–1353. [Google Scholar] [CrossRef] [Green Version]
- Das, M.; Cronin, O.; Keohane, D.M.; Cormac, E.M.; Nugent, H.; Nugent, M.; Molloy, C.; O’Toole, P.W.; Shanahan, F.; Molloy, M.G.; et al. Gut microbiota alterations associated with reduced bone mineral density in older adults. Rheumatology 2019, 58, 2295–2304. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Xie, Z.; Sun, J.; Huang, S.; Chen, Y.; Li, C.; Sun, X.; Xia, B.; Tian, L.; Guo, C.; et al. Gut microbiome reveals specific dysbiosis in primary osteoporosis. Front. Cell Infect. Microbiol. 2020, 10, 160. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Xu, S.; Zhang, B.; Xiao, C.; Chen, Z.; Si, F.; Fu, J.; Lin, X.; Zheng, G.; Yu, G.; et al. Gut microbiota and metabolite alterations associated with reduced bone mineral density or bone metabolic indexes in postmenopausal osteoporosis. Aging 2020, 12, 8583–8604. [Google Scholar] [CrossRef] [PubMed]
- Deepa, D.; Jain, G. Assessment of periodontal health status in postmenopausal women visiting dental hospital from in and around Meerut city: Cross-sectional observational study. J. Midlife Health 2016, 7, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Mazur, I.; Dilbarkhanov, B.; Kuracha, X.; Novoshytskyy, V.; Suprunovych, I.; Zhakipbekov, K. Periodontal status and bone metabolism in women in reproductive and postmenopausal periods. Horm. Mol. Biol. Clin. Investig. 2020, 41, 20200011. [Google Scholar] [CrossRef] [PubMed]
- George, C.N.; Canuas-Landero, V.; Theodoulou, E.; Muthana, M.; Wilson, C.; Ottewell, P. Oestrogen and zoledronic acid driven changes to the bone and immune environments: Potential mechanisms undelying the differential anti-tumour effects of zoledronic acid in pre- and post-menopausal conditions. J. Bone Oncol. 2020, 15, 100317. [Google Scholar] [CrossRef]
- Ayed, M.S.; Alsharif, A.F.; Divakar, D.D.; Jhugroo, C.; Alosaimi, B.; Mustafa, M. Evaluating the possible association between systemic osteoporosis and periodontal disease progression in postmenopausal women. Dis. Mon. 2019, 65, 193–215. [Google Scholar] [CrossRef]
- Brennan, R.M.; Genco, R.J.; Hovey, K.M.; Trevisan, M.; Wactawski-Wende, J. Clinical attachment loss, systemic bone density, and subgingival calculus in postmenopausal women. J. Periodontol. 2007, 78, 2104–2111. [Google Scholar] [CrossRef]
- Pereira, F.M.; Rodrigues, V.P.; de Oliveira, A.E.; Brito, L.M.; Lopes, F.F. Association between periodontal changes and osteo-porosis in postmenopausal women. Climacteric 2015, 18, 311–315. [Google Scholar] [CrossRef]
- Ursarescu, I.G.; Pasarin, L.; Solomon, S.M.; Cioloca, D.; Nitescu, D.C.; Boatca, M.; Martu, S. The effects of the adjunctive therapy with subantimicrobial doses of doxycycline in patients with osteoporosis and chronic periodontitis. Rom. J. Oral Rehabil. 2015, 7, 56–61. [Google Scholar]
- Greenstein, G. Local drug delivery in the treatment of periodontal diseases: Assessing the clinical significance of the results. J. Periodontol. 2006, 77, 565–578. [Google Scholar] [CrossRef]
- Garrido-Mesa, N.; Zarzuelo, A.; Gálvez, J. Minocycline: Far beyond an antibiotic. Br. J. Pharmacol. 2013, 169, 337–352. [Google Scholar] [CrossRef] [Green Version]
- Basegmez, C.; Berber, L.; Yalcin, F. Clinical and biochemical efficacy of minocycline in nonsurgical periodontal therapy: A randomized controlled pilot study. J. Clin. Pharmacol. 2011, 51, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Bala, I.; Hariharan, S.; Kumar, M.N. PLGA nanoparticles in drug delivery: The state of the art. Crit. Rev. Ther. Drug Carrier Syst. 2004, 21, 387–422. [Google Scholar] [CrossRef] [PubMed]
- Paquette, D.W. Minocycline microspheres: A complementary medical-mechanical model for the treatment of chronic periodontitis. Compend. Contin. Educ. Dent. 2002, 23, 15–21. [Google Scholar] [PubMed]
- Van Dyke, T.E.; Offenbacher, S.; Braswell, L.; Lessem, J. Enhancing the value of scaling and root-planing: Arestin clinical trial results. J. Int. Acad. Periodontol. 2002, 4, 72–76. [Google Scholar]
- Chackartchi, T.; Hamzani, Y.; Shapira, L.; Polak, D. Effect of subgingival mechanical debridement and local delivery of chlorhexidine gluconate chip or minocycline hydrochloride microspheres in patients enrolled in supportive periodontal therapy: A retrospective analysis. Oral Health Prev. Dent. 2019, 17, 167–171. [Google Scholar]
- Goodson, J.M.; Gunsolley, J.C.; Grossi, S.G.; Bland, P.S.; Otomo-Corgel, J.; Doherty, F.; Comiskey, J. Minocycline HCl microspheres reduce red-complex bacteria in periodontal disease therapy. J. Periodontol. 2007, 78, 1568–1579. [Google Scholar] [CrossRef] [Green Version]
- Renvert, S.; Lessem, J.; Lindahl, C.; Svensson, M. Treatment of incipient peri-implant infections using topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement. J. Int. Acad. Periodontol. 2004, 6, 154–159. [Google Scholar]
- Teles, F.R.F.; Lynch, M.C.; Patel, M.; Torresyap, G.; Martin, L. Bacterial resistance to minocycline after adjunctive minocycline microspheres during periodontal maintenance: A randomized clinical trial. J. Periodontol. 2021, 92, 1222–1231. [Google Scholar] [CrossRef]
- Killeen, A.C.; Harn, J.A.; Erickson, L.M.; Yu, F.; Reinhardt, R.A. Local minocycline effect on inflammation and clinical attachment during periodontal maintenance: Randomized clinical Trial. J. Periodontol. 2016, 87, 1149–1157. [Google Scholar] [CrossRef]
- Tabenski, L.; Moder, D.; Cieplik, F.; Schenke, F.; Hiller, K.A.; Buchalla, W.; Schmalz, G.; Christgau, M. Antimicrobial photodynamic therapy vs. local minocycline in addition to non-surgical therapy of deep periodontal pockets: A controlled randomized clinical trial. Clin. Oral Investig. 2017, 21, 2253–2264. [Google Scholar] [CrossRef]
- Hernández-Vigueras, S.; Martínez-Garriga, B.; Sánchez, M.C.; Sanz, M.; Estrugo-Devesa, A.; Vinuesa, T.; López-Loópez, J.; Viñas, M. Oral microbiota, periodontal status, and osteoporosis in postmenopausal females. J. Periodontol. 2016, 87, 124–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
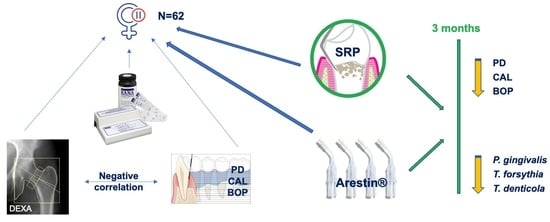
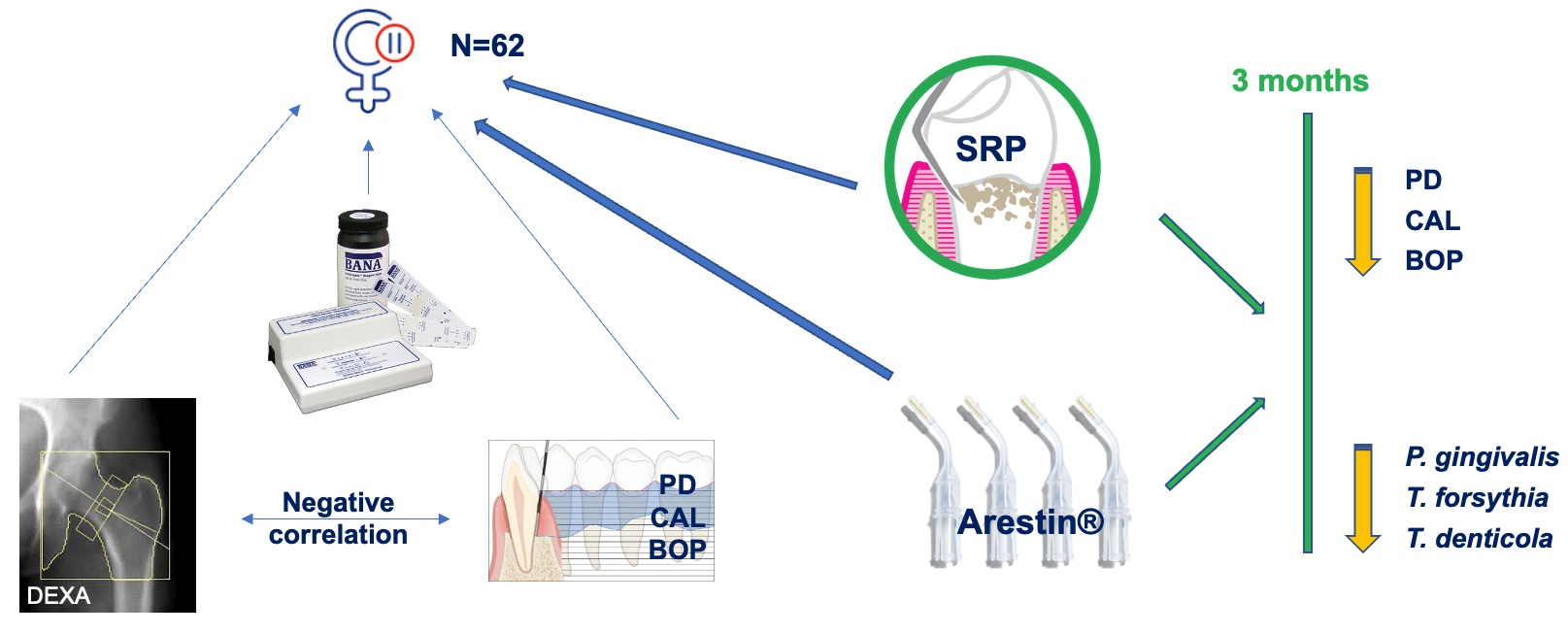
| Baseline (T0) | At 3 Months (T1) | |
|---|---|---|
| PD (mm) | 6.05 ± 0.36 | 5.12 ± 0.33 * |
| CAL (mm) | 5.11 ± 0.59 | 4.45 ± 0.57 * |
| BOP | 78.19 ± 5.00 | 11.54 ± 2.78 * |
| Baseline (T0) | At 3 Months (T1) | |
|---|---|---|
| Porphyromonas gingivalis | 84.78 ± 6.74 | 10.75 ± 3.55 * |
| Tannerella forsythia | 61.91 ± 13.40 | 8.44 ± 2.01 * |
| Treponema denticola | 39.72 ± 6.50 | 7.53 ± 1.20 * |
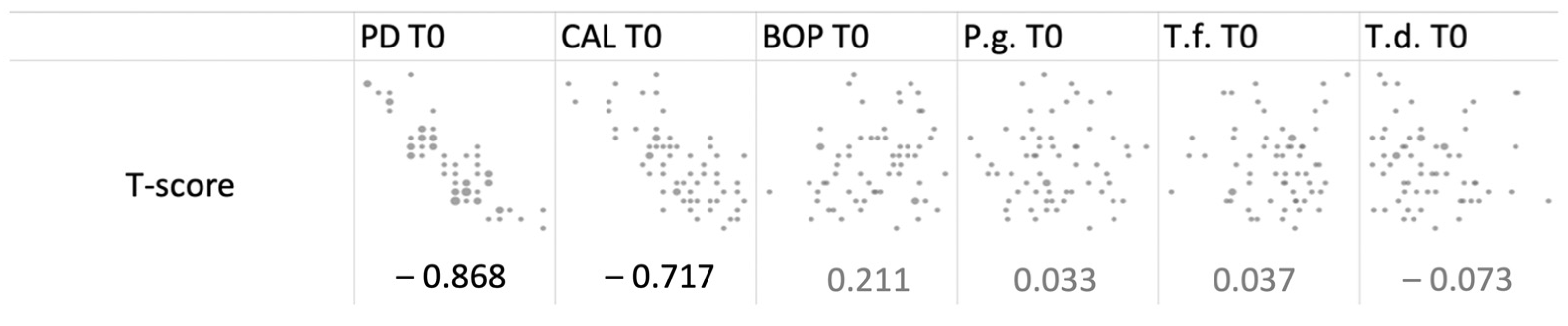
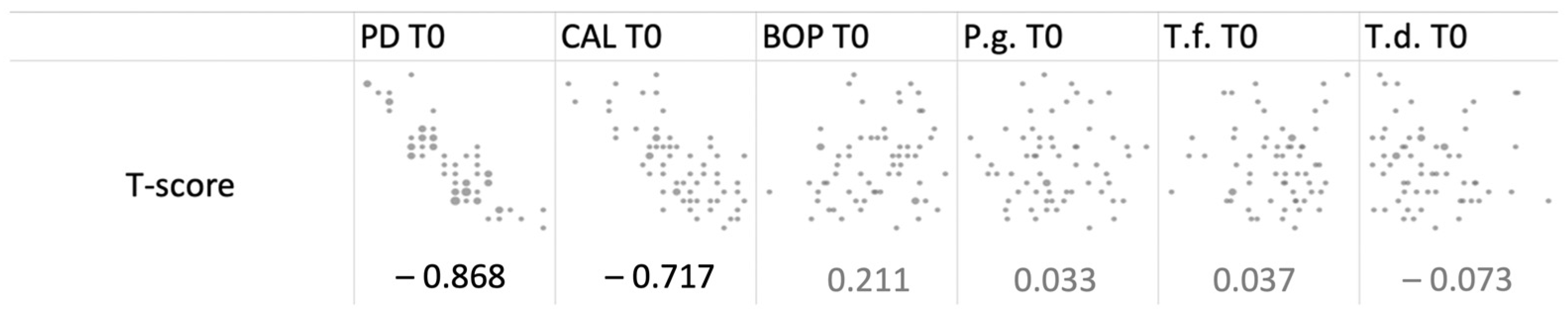
| PD T0 | CAL T0 | BOP T0 | P.g. T0 | T.f. T0 | T.d. T0 | |
|---|---|---|---|---|---|---|
| PD T0 | 0 | 0.000000 * | 0.152733 | 0.280677 | 0.376881 | 0.792804 |
| CAL T0 | 0 | 0.165768 | 0.487371 | 0.972045 | 0.399207 | |
| BOP T0 | 0 | 0.394453 | 0.433201 | 0.300487 | ||
| P.g. T0 | 0 | 0.842481 | 0.113247 | |||
| T.f. T0 | 0 | 0.039031 * | ||||
| T.d. T0 | 0 |
| PD T1 | CAL T1 | BOP T1 | P.g. T1 | T.f. T1 | T.d. T1 | |
|---|---|---|---|---|---|---|
| PD T1 | 0 | 0.000000 * | 0.971876 | 0.183483 | 0.217513 | 0.166559 |
| CAL T1 | 0 | 0.477021 | 0.623212 | 0.886567 | 0.450642 | |
| BOP T1 | 0 | 0.748079 | 0.253379 | 0.308013 | ||
| P.g. T1 | 0 | 0.307023 | 0.286488 | |||
| T.f. T1 | 0 | 0.828705 | ||||
| T.d. T1 | 0 |
| ΔPD | ΔCAL | ΔBOP | ΔP.g. | ΔT.f. | ΔT.d. | |
|---|---|---|---|---|---|---|
| ΔPD | 0 | 0.005746 * | 0.426438 | 0.907375 | 0.763760 | 0.683836 |
| ΔCAL | 0 | 0.030416 * | 0.828127 | 0.612912 | 0.345614 | |
| ΔBOP | 0 | 0.250398 | 0.504814 | 0.188132 | ||
| ΔP.g. | 0 | 0.320476 | 0.297842 | |||
| ΔT.f. | 0 | 0.038469 * | ||||
| ΔT.d. | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laza, G.-M.; Sufaru, I.-G.; Martu, M.-A.; Martu, C.; Diaconu-Popa, D.A.; Jelihovschi, I.; Martu, S. Effects of Locally Delivered Minocycline Microspheres in Postmenopausal Female Patients with Periodontitis: A Clinical and Microbiological Study. Diagnostics 2022, 12, 1310. https://doi.org/10.3390/diagnostics12061310
Laza G-M, Sufaru I-G, Martu M-A, Martu C, Diaconu-Popa DA, Jelihovschi I, Martu S. Effects of Locally Delivered Minocycline Microspheres in Postmenopausal Female Patients with Periodontitis: A Clinical and Microbiological Study. Diagnostics. 2022; 12(6):1310. https://doi.org/10.3390/diagnostics12061310
Chicago/Turabian StyleLaza, Georgeta-Maria, Irina-Georgeta Sufaru, Maria-Alexandra Martu, Cristian Martu, Diana Antonela Diaconu-Popa, Igor Jelihovschi, and Silvia Martu. 2022. "Effects of Locally Delivered Minocycline Microspheres in Postmenopausal Female Patients with Periodontitis: A Clinical and Microbiological Study" Diagnostics 12, no. 6: 1310. https://doi.org/10.3390/diagnostics12061310
APA StyleLaza, G.-M., Sufaru, I.-G., Martu, M.-A., Martu, C., Diaconu-Popa, D. A., Jelihovschi, I., & Martu, S. (2022). Effects of Locally Delivered Minocycline Microspheres in Postmenopausal Female Patients with Periodontitis: A Clinical and Microbiological Study. Diagnostics, 12(6), 1310. https://doi.org/10.3390/diagnostics12061310