
Prevalence of Gestational Diabetes in preCOVID-19 and COVID-19 Years and Its Impact on Pregnancy: A 5-Year Retrospective Study


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
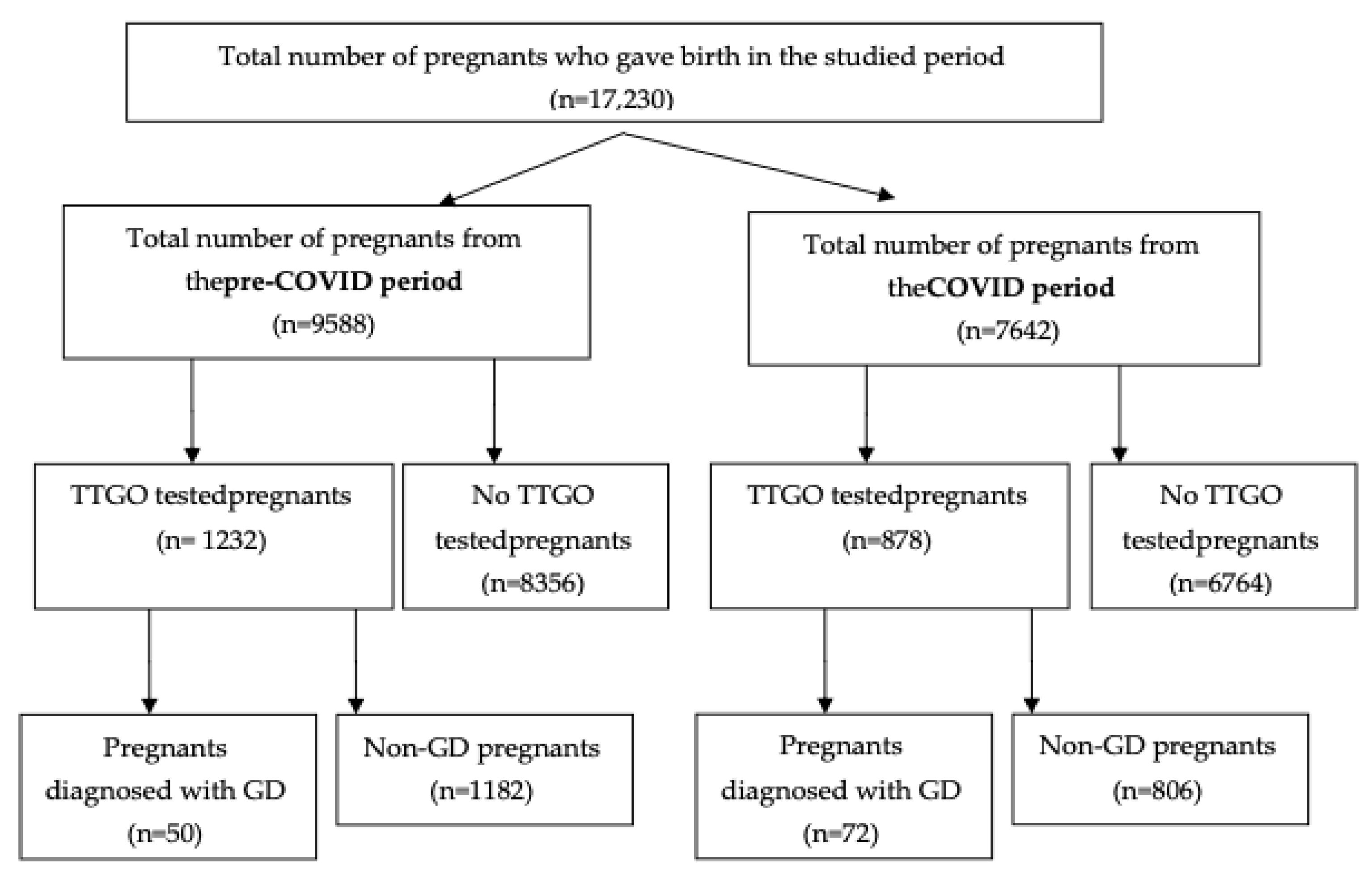
2.1. Objects and Collection
2.2. Procedures
2.3. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiefari, E.; Quaresima, P.; Visconti, F.; Mirabelli, M.; Brunetti, A. Gestational diabetes and fetal overgrowth: Time to rethink screening guidelines. Lancet Diabetes Endocrinol. 2020, 8, 561–562. [Google Scholar] [CrossRef]
- Han, Y.; Tong, M.; Jin, L.; Yu, J.; Meng, W.; Ren, A. Maternal age at pregnancy and risk for gestational diabetes mellitus among Chinese women with singleton pregnancies. Int. J. Diabetes Dev. Ctries. 2020, 41, 114–120. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes—2017. J. Clin. Appl. Res. Educ. 2017, 35, 5. [Google Scholar]
- Chu, S.Y.; Callaghan, W.M.; Kim, S.Y.; Schmid, C.H.; Lau, J.; England, L.J.; Dietz, P.M. Maternal Obesity and Risk of Gestational Diabetes Mellitus. Diabetes Care 2007, 30, 2070–2076. [Google Scholar] [CrossRef] [Green Version]
- Melchior, H.; Kurch-Bek, D.; Mund, M. The Prevalence of Gestational Diabetes. Dtsch. Arztebl. Int. 2017, 114, 412–418. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, R.L.; Wall, C.R.; Bloomfield, F.H. Prevalence of gestational diabetes according to commonly used data sources: An observational study. BMC Pregnancy Childbirth 2019, 19, 349. [Google Scholar] [CrossRef] [Green Version]
- Ogurtsova, K.; Da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- López-de-Andrés, A.; Perez-Farinos, N.; Hernández-Barrera, V.; Palomar-Gallego, M.A.; Carabantes-Alarcón, D.; Zamorano-León, J.J.; Miguel-Diez, D.; Jimenez-Garcia, R. A population-based study of diabetes during pregnancy in Spain (2009–2015): Trends in incidence, obstetric interventions, and pregnancy outcomes. J. Clin. Med. 2020, 9, 582. [Google Scholar] [CrossRef] [Green Version]
- Mackin, S.T.; Nelson, S.M.; Kerssens, J.J.; Wood, R.; Wild, S.; Colhoun, H.M.; Leese, G.P.; Philip, S.; Lindsay, R.S. Diabetes and pregnancy: National trends over a 15 year period. Diabetologia 2018, 61, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Introduction: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S1–S2. [Google Scholar] [CrossRef]
- Li, G.; Wei, T.; Ni, W.; Zhang, A.; Zhang, J.; Xing, Y.; Xing, Q. Incidence and risk factors of gestational diabetes mellitus: A prospective cohort study in Qingdao, China. Front. Endocrinol. 2020, 11, 636. [Google Scholar] [CrossRef] [PubMed]
- Garabedian, C.; Deruelle, P. Delivery (timing, route, peripartum glycemic control) in women with gestational diabetes mellitus. Diabetes Metab. 2010, 36, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.L. Malformations in infants of diabetic mothers. Teratology 1982, 25, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Kucera, J. Rate and type of congenital anomalies among offspring of diabetic women. J. Reprod. Med. 1971, 7, 73–82. [Google Scholar]
- Dude, A.M.; Badreldin, N.; Schieler, A.; Yee, L.M. Periconception glycemic control and congenital anomalies in women with pregestational diabetes. BMJ Open Diabetes Res. Care 2021, 9, e001966. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Liu, Y.; Wu, H. Overexpression of circACTR2 in Gestational Diabetes Mellitus Predicts Intrauterine Death, Fetal Malformation, and Intrauterine Infection. Diabetes Metab. Syndr. Obes. 2021, 14, 4655. [Google Scholar] [CrossRef]
- Gasim, T. Gestational Diabetes Mellitus: Maternal and Perinatal Outcomes in 220 Saudi Women. Oman Med. J. 2012, 27, 140–144. [Google Scholar] [CrossRef]
- Kanguru, L.; Bezawada, N.; Hussein, J.; Bell, J. The burden of diabetes mellitus during pregnancy in low- and middle-income countries: A systematic review. Glob. Health Action 2014, 7, 23987. [Google Scholar] [CrossRef] [Green Version]
- Al-Hakeem, M.M. Pregnancy outcome of gestational diabetic mothers: Experience in a tertiary center. J. Fam. Community Med. 2006, 13, 55–59. [Google Scholar]
- Metzger, B.E.; Coustan, D.R.; Trimble, E.R. Hyperglycemia and adverse pregnancy outcomes. Clin. Chem. 2019, 65, 937–938. [Google Scholar] [CrossRef] [Green Version]
- Papageorghiou, A.T.; Deruelle, P.; Gunier, R.B.; Rauch, S.; García-May, P.K.; Mhatre, M.; Usman, M.A.; Abd-Elsalam, S.; Etuk, S.; Simmons, L.E.; et al. Preeclampsia and COVID-19: Results from the intercovid prospective longitudinal study. Am. J. Obstet. Gynecol. 2021, 225, 289.e1–289.e17. [Google Scholar] [CrossRef] [PubMed]
- Kc, K.; Shakya, S.; Zhang, H. Gestational Diabetes Mellitus and Macrosomia: A Literature Review. Ann. Nutr. Metab. 2015, 66 (Suppl. S2), 14–20. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.; Ibrahim, I.; Eltaher, F.; Beer, S.; Baagar, K.; Aboulfotouh, M.; Konje, J.C.; Abou-Samra, A.-B. Screening pregnant women in a high-risk population with WHO-2013 or NICE diagnostic criteria does not affect the prevalence of gestational diabetes. Sci. Rep. 2021, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Al-Rifai, R.H.; Abdo, N.M.; Paulo, M.S.; Saha, S.; Ahmed, L.A. Prevalence of Gestational Diabetes Mellitus in the Middle East and North Africa, 2000–2019: A Systematic Review, Meta-Analysis, and Meta-Regression. Front. Endocrinol. 2021, 12, 668447. [Google Scholar] [CrossRef]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; Vale, M.S.D.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women with and without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef]
- Li, Y.; Ren, X.; He, L.; Li, J.; Zhang, S.; Chen, W. Maternal age and the risk of gestational diabetes mellitus: A systematic review and meta-analysis of over 120 million participants. Diabetes Res. Clin. Pract. 2020, 162, 108044. [Google Scholar] [CrossRef]
- Catalano, P.M.; Roman, N.M.; Tyzbir, E.D.; Merritt, A.O.; Driscoll, P.; Amini, S.B. Weight gain in women with gestational diabetes. Obstet. Gynecol. 1993, 81, 523–528. [Google Scholar]
- Kong, L.; Nilsson, I.A.; Gissler, M.; Lavebratt, C. Associations of Maternal Diabetes and Body Mass Index with Offspring Birth Weight and Prematurity. JAMA Pediatr. 2019, 173, 371–378. [Google Scholar] [CrossRef]
- Shah, A.; Stotland, N.E.; Cheng, Y.W.; Ramos, G.A.; Caughey, A.B. The association between body mass index and gestational diabetes mellitus varies by race/ethnicity. Am. J. Perinatol. 2011, 28, 515–520. [Google Scholar] [CrossRef] [Green Version]
- D’Ambrosio, V.; Brunelli, R.; Vena, F.; Di Mascio, D.; Marchetti, C.; Boccherini, C.; Piccioni, M.G.; Panici, P.B.; Giancotti, A. Metformin reduces maternal weight gain in obese pregnant women: A systematic review and meta-analysis of two randomized controlled trials. Diabetes/Metab. Res. Rev. 2019, 35, e3164. [Google Scholar] [CrossRef]
- Eskenazi, B.; Rauch, S.; Iurlaro, E.; Gunier, R.B.; Albertina, R.E.G.O.; Gravett, M.G.; Cavoretto, P.I.; Deruelle, P.; García-May, P.K.; Mhatre, M.; et al. Diabetes mellitus, maternal adiposity, and insulin-dependent gestational diabetes are associated with COVID-19 in pregnancy: The INTERCOVID Study. Am. J. Obstet. Gynecol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Schummers, L.; Hutcheon, J.A.; Hacker, M.R.; VanderWeele, T.J.; Williams, P.L.; McElrath, T.A.; Hernandez-Diaz, S. Absolute risks of obstetric outcomes risks by maternal age at first birth: A population-based cohort. Epidemiology 2018, 29, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, L.; Xiao, K.; Horswell, R.; Besse, J.; Johnson, J.; Ryan, D.H.; Hu, G. Increasing incidence of gestational diabetes mellitus in Louisiana, 1997–2009. J. Women’s Health 2012, 21, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Balsells, M.; Garcia-Patterson, A.; Gich, I.; Corcoy, R. Major congenital malformations in women with gestational diabetes mellitus: A systematic review and meta-analysis. Diabetes/Metab. Res. Rev. 2012, 28, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Mitrović, M.; Stojić, S.; Tešić, D.S.; Popović, Đ.; Rankov, O.; Tomić-Naglić, D.; Novaković-Paro, J.; Pejin, R.; Bulatović, S.; Todorović-Veljić, M.; et al. The impact of diabetes mellitus on the course and outcome of pregnancy during a 5-year follow-up. Vojnosanit. Pregl. 2014, 71, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.; Song, W.O. Prepregnancy body mass index is an independent risk factor for gestational hypertension, gestational diabetes, preterm labor, and small-and large-for-gestational-age infants. J. Matern.-Fetal Neonatal Med. 2015, 28, 1679–1686. [Google Scholar] [CrossRef]
- Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 190 Summary: Gestational Diabetes Mellitus. Obs. Gynecol. 2018, 131, 406–408. [Google Scholar] [CrossRef]


{kind=link}
| Total Births Per Year at Tested Patients | Total Births with GDM Per Year | % of GDM Births | |
|---|---|---|---|
| 2017 | 433 | 12 | 2.77 |
| 2018 | 447 | 13 | 2.91 |
| 2019 | 352 | 25 | 7.10 |
| 2020 | 371 | 29 | 7.82 |
| 2021 | 507 | 43 | 8.48 |
| Number | % | |
|---|---|---|
| Parity | ||
| Nulliparous | 65 | 53.27 |
| Pluripare | 39 | 31.96 |
| More than 2 births | 18 | 14.75 |
| Age groups | ||
| ≤20 years | 0 (0.00) | |
| 21–30 years | 44 | 36.07 |
| 31–40 years | 76 | 62.30 |
| >40 years | 2 | 1.64 |
| Obesity | ||
| Normoponderal | 51 | 41.80 |
| Grade I obesity | 48 | 39.34 |
| Grade II obesity | 19 | 15.57 |
| Morbid Obesity | 4 | 3.29 |
| Number | % | |
|---|---|---|
| Type of birth | ||
| Natural Delivery | 16 | 13.11 |
| Cesarean Delivery | 106 | 86.89 |
| Newborn weight at birth | ||
| <2000 g | 3 | 2459 |
| 2000–2500 g | 2 | 1.634 |
| 2500–3000 g | 17 | 13.93 |
| 3000–3500 g | 39 | 31.962 |
| 3500–4000 g | 30 | 24.590 |
| 4000–5000 g | 30 | 24.590 |
| >5000 g | 1 | 0.819 |
| Apgar Score (IA) | ||
| 6 | 11 | 9.016 |
| 7 | 26 | 21.311 |
| 9 | 85 | 69.672 |
| Malformed fetuses | 2 | 1.639 |
| Variable | PreCOVID (n = 50) | COVID (n = 72) | p Test, sig |
|---|---|---|---|
| HGB (g/dL) | 11.18 ± 1.48 | 10.92 ± 1.38 | 0.291 t, is |
| HCT (%) | 34.1 (7.44) | 32.6 (6.7) | 0.378 M-W, is |
| WBC (×10³/qL) | 12.1 (5.31) | 11.5 (3.46) | 0.306 M-W, is |
| Blood sugar level (mg/dL) | 103.0 (35.5) | 101.5 (32.75) | 0.613 M-W, is |
| Fetal weight (g) | 3400 (950) | 3575 (912.5) | 0.771 M-W, is |
| Apgar score | 9 (1) | 9 (1) | 0.213 M-W, is |
| HTAIS | 17 (34%) | 19 (26.4%) | 0.365 Chi2, is |
| Newborn pathology | 41 (82%) | 50 (69.4%) | 0.141 Chi2, is |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chelu, S.; Bernad, E.; Craina, M.; Neamtu, R.; Mocanu, A.G.; Vernic, C.; Chiriac, V.D.; Tomescu, L.; Borza, C. Prevalence of Gestational Diabetes in preCOVID-19 and COVID-19 Years and Its Impact on Pregnancy: A 5-Year Retrospective Study. Diagnostics 2022, 12, 1241. https://doi.org/10.3390/diagnostics12051241
Chelu S, Bernad E, Craina M, Neamtu R, Mocanu AG, Vernic C, Chiriac VD, Tomescu L, Borza C. Prevalence of Gestational Diabetes in preCOVID-19 and COVID-19 Years and Its Impact on Pregnancy: A 5-Year Retrospective Study. Diagnostics. 2022; 12(5):1241. https://doi.org/10.3390/diagnostics12051241
Chicago/Turabian StyleChelu, Sorina, Elena Bernad, Marius Craina, Radu Neamtu, Adelina Geanina Mocanu, Corina Vernic, Veronica Daniela Chiriac, Larisa Tomescu, and Claudia Borza. 2022. "Prevalence of Gestational Diabetes in preCOVID-19 and COVID-19 Years and Its Impact on Pregnancy: A 5-Year Retrospective Study" Diagnostics 12, no. 5: 1241. https://doi.org/10.3390/diagnostics12051241
APA StyleChelu, S., Bernad, E., Craina, M., Neamtu, R., Mocanu, A. G., Vernic, C., Chiriac, V. D., Tomescu, L., & Borza, C. (2022). Prevalence of Gestational Diabetes in preCOVID-19 and COVID-19 Years and Its Impact on Pregnancy: A 5-Year Retrospective Study. Diagnostics, 12(5), 1241. https://doi.org/10.3390/diagnostics12051241