
Perceived Stress in Hepatitis C Virus Infected Patients under the DAA-Based Therapy

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schaefer, M.; Capuron, L.; Friebe, A.; Diez-Quevedo, C.; Robaeys, G.; Neri, S.; Foster, G.R.; Kautz, A.; Forton, D.; Pariante, C.M. Hepatitis C infection, antiviral treatment and mental health: A European expert consensus statement. J. Hepatol. 2012, 57, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Nevola, R.; Lus, G.; Restivo, L.; Guerrera, B.; Romano, C.; Zampino, R.; Rinaldi, L.; Sellitto, A.; Giordano, M.; et al. Chronic hepatitis C virus infection and neurological and psychiatric disorders: An overview. World J. Gastroenterol. 2015, 21, 2269–2280. [Google Scholar] [CrossRef] [PubMed]
- Danilescu, C.M.; Sandulescu, D.L.; Pirlog, M.C.; Streba, C.T.; Rogoveanu, I. Depressive and Anxious Symptoms in Hepatitis C Virus Infected Patients Receiving DAA-Based Therapy. Diagnostics 2021, 11, 2237. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; Brook, R.A.; Kleinman, N.L.; Corey-Lisle, P. The impact of hepatitis C virus infection on work absence, productivity, and healthcare benefit costs. Hepatology 2010, 52, 436–442. [Google Scholar] [CrossRef]
- Pascual-Argente, N.; Puig-Junoy, J.; Llagostera-Punzano, A. Non-healthcare costs of hepatitis C: A systematic review. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 19–30. [Google Scholar] [CrossRef]
- Omland, L.H.; Osler, M.; Jepsen, P.; Krarup, H.; Weis, N.; Christensen, P.B.; Roed, C.; Sørensen, H.T.; Obel, N. Socioeconomic status in HCV infected patients—risk and prognosis. Clin. Epidemiol. 2013, 5, 163–172. [Google Scholar] [CrossRef]
- Meffre, C.; Le, S.Y.; Delarocque-Astagneau, E.; Dubois, F.; Antona, D.; Lemasson, J.-M.; Warszawski, J.; Steinmetz, J.; Coste, D.; Meyer, J.-F.; et al. Prevalence of hepatitis B and hepatitis C virus infections in France in 2004: Social factors are important predictors after adjusting for known risk factors. J. Med. Virol. 2010, 82, 546–555. [Google Scholar] [CrossRef]
- Menzin, J.; White, L.A.; Nichols, C.; Deniz, B. The economic burden of advanced liver disease among patients with hepatitis C virus: A large state Medicaid perspective. BMC Health Serv. Res. 2012, 12, 459. [Google Scholar] [CrossRef]
- Razavi, H.; ElKhoury, A.C.; Elbasha, E.; Estes, C.; Pasini, K.; Poynard, T.; Kumar, R. Chronic hepatitis C virus (HCV) disease burden and cost in the United States. Hepatology 2013, 57, 2164–2170. [Google Scholar] [CrossRef]
- Fontana, R.J.; Hussain, K.B.; Schwartz, S.M.; Moyer, C.A.; Su, G.L.; Lok, A.S.F. Emotional distress in chronic hepatitis C patients not receiving antiviral therapy. J. Hepatol. 2002, 36, 401–407. [Google Scholar] [CrossRef]
- Grassi, L.; Satriano, J.; Serra, A.; Biancosino, B.; Zotos, S.; Sighinolfi, L.; Ghinelli, F. Emotional stress, psychosocial variables and coping associated with hepatitis C virus and human immunodeficiency virus infections in intravenous drug users. Psychother. Psychosom. 2002, 71, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Selye, H. A syndrome produced by diverse nocuous agents. Nature 1936, 138, 32. [Google Scholar] [CrossRef]
- Fink, G. Stress: Definition and history. In Encyclopedia of Neuroscience; Squire, L., Ed.; Elsevier Ltd.: Oxford, UK, 2009; pp. 549–555. [Google Scholar]
- Marcellin, P. Hepatitis C: The clinical spectrum of the disease. J. Hepatol. 1999, 31, 9–16. [Google Scholar] [CrossRef]
- Foster, G.R. Quality of life considerations for patients with chronic hepatitis C. J. Viral Hepat. 2009, 16, 605–611. [Google Scholar] [CrossRef]
- Baraldi, S.; Hepgul, N.; Mondelli, V.; Pariante, C.M. Symptomatic treatment of interferon-alpha-induced depression in hepatitis C: A systematic review. J. Clin. Psychopharmacol. 2012, 32, 531–543. [Google Scholar] [CrossRef]
- Cooper, C.M.; Godlewska, B.; Sharpley, A.L.; Barnes, E.; Cowen, P.J.; Harmer, C.J. Interferon-α induces negative biases in emotional processing in patients with hepatitis C virus infection: A preliminary study. Psychol. Med. 2018, 48, 998–1007. [Google Scholar] [CrossRef]
- Gheorghe, L.; Sporea, I.; Iacob, S.; Sirli, R.; Trifan, A.; Dobru, D.; Diculescu, M.; Stanciu, C.; Pascu, O.; Acalovschi, M.; et al. Position paper on treatment of hepatitis C in Romania, 2017. Part one. J. Gastrointest. Liver Dis. 2017, 26, 171–181. [Google Scholar] [CrossRef]
- Gheorghe, L.; Sporea, I.; Iacob, S.; Sirli, R.; Trifan, A.; Diculescu, M.; Stanciu, C.; Pascu, O.; Acalovschi, M.; Brisc, C.; et al. Position paper on treatment of hepatitis C in Romania, 2017. Part two. J. Gastrointest. Liver Dis. 2017, 26, 309–317. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef]
- Sănătăţii, M.; de Sănătate, C.N.d. Ordin Privind Modificarea şi Completarea Ordinului Ministrului Sănătăţii Publice şi al Preşedintelui Casei Naţionale de Asigurări de Sănătate nr. 1.301/500/2008 Pentru Aprobarea Protocoalelor Terapeutice Privind Prescrierea Medicamentelor Aferente Denumirilor Commune Internaţionale Prevăzute în Lista Cuprinzând Denumirile Commune Internaţionale Corespunzătoare Medicamentelor de care Beneficiază Asiguraţii, cu sau fără Contribuţie Personală, pe bază de Prescripţie Medicală, în Sistemul de Asigurări Sociale de Sănătate, Aprobată Prin Hotărârea Guvernului nr. 720/2008. Available online: http://www.ms.ro/wp-content/uploads/2017/03/Ordin-25.04.2017.pdf (accessed on 15 April 2021).
- Gheorghe, L.; Csiki, I.E.; Iacob, S.; Gheorghe, C.; Smira, G.; Regep, L. The prevalence and risk factors of hepatitis C virus infection in adult population in Romania: A nationwide survey 2006–2008. J. Gastrointest. Liver Dis. 2010, 19, 373–379. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behavior. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Lee, E.H. Review of the Psychometric Evidence of the Perceived Stress Scale. Asian Nurs. Res. 2012, 6, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Mardare, I.; Bratu, E.C. Measuring Stress Methods and Tools. ACTA Med. Transilv. 2020, 25, 5–7. [Google Scholar] [CrossRef]
- Balgiu, B.A.; Sfeatcu, R.; Dumitrache, M.A.; Tribus, L. Construct validity and reliability of Perceived Stress Scale (PSS-14) in a Romanian sample of dental students. Int. J. Med. Dent. 2021, 25, 23–30. [Google Scholar]
- Sfeatcu, R.; Balgiu, B.A.; Parlatescu, I. New psychometric evidences on the Dental Environment Stress questionnaire among Romanian students. J. Edu. Health Promot. 2021, 10, 296. [Google Scholar]
- Keramat, F.; Mamani, M.; Torabian, S.; Aliparast Dostkohi, M. Assessment and Comparison of Health-Related Quality of Life in Chronic Hepatitis B and C Patients with Healthy Persons in Hamadan Province. Avicenna J. Clin. Med. 2013, 20, 151–159. [Google Scholar]
- Weissenborn, K.; Krause, J.; Bokemeyer, M.; Hecker, H.; Schuler, A.; Ennen, J.C.; Ahl, B.; Manns, M.P.; Boker, K.W. Hepatitis C virus infection affects the brain-evidence from psychometric studies and magnetic resonance spectroscopy. J. Hepatol. 2004, 41, 845–851. [Google Scholar] [CrossRef]
- McAndrews, M.P.; Farcnik, K.; Carlen, P.; Damyanovich, A.; Mrkonjic, M.; Jones, S.; Heathcote, E.J. Prevalence and significance of neurocognitive dysfunction in hepatitis C in the absence of correlated risk factors. Hepatology 2005, 41, 801–808. [Google Scholar] [CrossRef]
- Foster, G.R.; Goldin, R.D.; Thomas, H.C. Chronic hepatitis C virus infection causes a significant reduction in quality of life in the absence of cirrhosis. Hepatology 1998, 27, 209–212. [Google Scholar] [CrossRef]
- Castera, L.; Constant, A.; Bernard, P.H.; de Ledinghen, V.; Couzigou, P. Psychological impact of chronic hepatitis C: Comparison with other stressful life events and chronic diseases. World J. Gastroenterol. 2006, 12, 1545–1550. [Google Scholar] [CrossRef]
- Younossi, Z.; Kallman, J.; Kincaid, J. The effects of HCV infection and management on health-related quality of life. Hepatology 2007, 45, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Fabrazzo, M.; Zampino, R.; Vitrone, M.; Sampogna, G.; Del Gaudio, L.; Nunziata, D.; Agnese, S.; Santagata, A.; Durante-Mangoni, E.; Fiorillo, E. Effects of Direct-Acting Antiviral Agents on the Mental Health of Patients with Chronic Hepatitis C: A Prospective Observational Study. Brain Sci. 2020, 10, 483. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Montagnese, S.; Zanetto, A.; Turco, M.; De Rui, M.; Ferrarese, A.; Amodio, P.; Germani, G.; Senzolo, M.; Gambato, M.; et al. Neuropsychiatric performance and treatment of hepatitis C with direct-acting antivirals: A prospective study. BMJ Open Gastroenterol. 2017, 4, e000183. [Google Scholar] [CrossRef]
- Durcan, E.; Hatemi, I.; Sonsuz, A.; Canbakan, B.; Ozdemir, S.; Tuncer, M. The effect of direct antiviral treatment on the depression, anxiety, fatigue and quality-of-life in chronic hepatitis C patients. Eur. J. Gastroenterol. Hepatol. 2020, 32, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Abdo, A.A. Predicting antiviral treatment response in chronic hepatitis C: How accurate and how soon? J. Antimicrob. Chemother. 2003, 51, 487–491. [Google Scholar] [CrossRef][Green Version]
- Shiffman, M.L.; Di Bisceglie, A.D.; Lindsay, K.L.; Morishima, C.; Wright, E.C.; Everson, G.T.; Everhart, J.E. Peginterferon alfa-2a and ribavirin in patients with chronic hepatitis C who have failed prior treatment. Gastroenterology 2004, 126, 1015–1023. [Google Scholar] [CrossRef]
- Skolnik, A.A.; Noska, A.; Yakovchenko, V.; Tsai, J.; Jones, N.; Gifford, A.L.; McInnes, D.K. Experiences with interferon-free hepatitis C therapies: Addressing barriers to adherence and optimizing treatment outcomes. BMC Health Serv. Res. 2019, 19, 91. [Google Scholar] [CrossRef]
- Wright, C.; Cogger, S.; Hsieh, K.; Goutzamanis, S.; Hellard, M.; Higgs, P. “I’m obviously not dying so it’s not something I need to sort out today”: Considering hepatitis C treatment in the era of direct acting antivirals. Infect. Dis. Health 2019, 24, 58–66. [Google Scholar] [CrossRef]
- Spradling, P.R.; Zhong, Y.; Moorman, A.C.; Rupp, L.B.; Lu, M.; Gordon, S.C.; Teshale, E.H.; Schmidt, M.A.; Daida, Y.G.; Boscarino, J.A. Chronic Hepatitis Cohort Study (CHeCS) Investigators. Psychosocial Obstacles to Hepatitis C Treatment Initiation Among Patients in Care: A Hitch in the Cascade of Cure. Hepatol. Commun. 2020, 5, 400–411. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Romanian National Program of Interferon-Free Therapy | |
| Inclusion Criteria | Exclusion Criteria |
| fibrosis F3/F4 METAVIR; | decompensated cirrhosis (Child-Pugh > 6); |
| fibrosis F0-F2 METAVIR only for healthcare professionals; | liver cancers without transplant indication; |
| HCV-HIV or HCV-HBV coinfection; | liver cancers ablatively treated or resected less than 6 months after the intervention; |
| hepatocellular carcinoma (HCC); | liver cancers with post-surgery CT/MRI signs of activity/recurrence; |
| post-transplant patients (other than liver); | contraindications to Ombitasvirum + Paritaprevirum + Ritonavirum or Dasabuvirum. |
| patients with extrahepatic malignancies; | |
| patients with hematological neoplasms. | |
| Our Study | |
| Inclusion Criteria | Exclusion Criteria |
| to be included in Romanian national program of interferon-free therapy; | refusal to participate in the study. |
| without neurologic and/or psychiatric disorder in the last 12 months. | |
| Group | Stage | PSS Score Level | ||
|---|---|---|---|---|
| Low | Moderate | High | ||
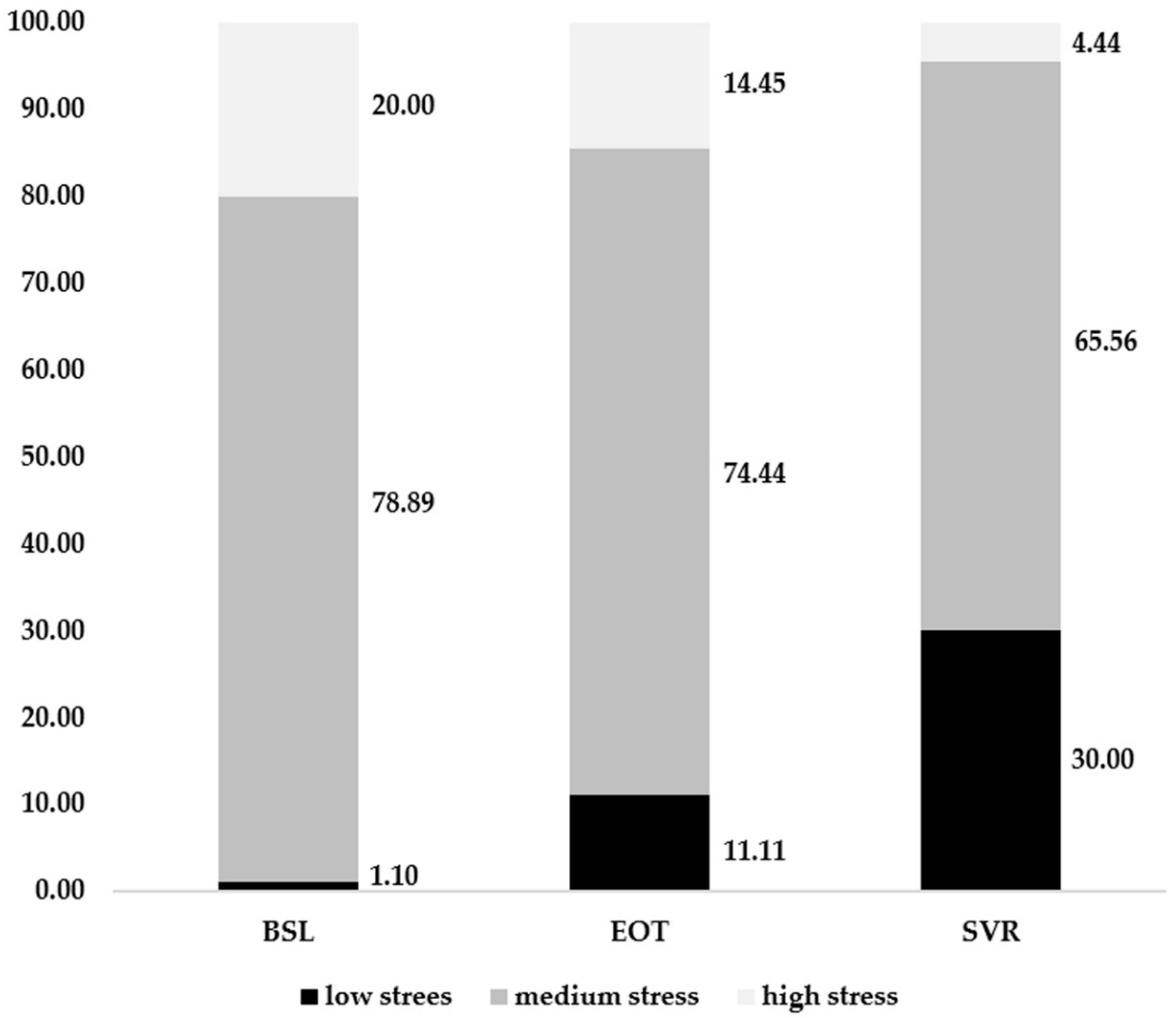
| Study lot n (%) | BSL | 1 (1.11) | 71 (78.89) | 18 (20.00) |
| EOT | 10 (11.11) | 67 (74.44) | 13 (14.44) | |
| SVR | 27 (30.00) | 59 (65.56) | 4 (4.44) | |
| Group | Stage | PSS Score Level | BSL/EOT | EOT/SVR | ||
|---|---|---|---|---|---|---|
| Low | Moderate | High | ||||
| Urban n (%) | BSL | 0 (0.00) | 33 (78.57) | 9 (21.43) | U = 1267.5 z = 2.102 p 1 = 0.036 | U = 1082 z = 0.599 p 1 = 0.549 |
| EOT | 9 (21.43) | 27 (64.29) | 6 (14.29) | |||
| SVR | 18 (42.86) | 23 (54.76) | 1 (2.08) | |||
| Rural n (%) | BSL | 1 (2.08) | 38 (79.17) | 9 (18.75) | ||
| EOT | 1 (2.08) | 40 (83.33) | 7 (14.58) | |||
| SVR | 9 (18.75) | 36 (75.00) | 3 (6.25) | |||
| Female n (%) | BSL | 1 (1.45) | 53 (76.81) | 15 (21.74) | U = 502.5 z = −2.121 p 1 = 0.034 | U = 1032.5 z = 2.941 p 1 = 0.003 |
| EOT | 8 (11.59) | 54 (78.26) | 7 (10.14) | |||
| SVR | 17 (24.64) | 48 (69.57) | 4 (5.80) | |||
| Male n (%) | BSL | 0 (0.00) | 18 (85.71) | 3 (14.29) | ||
| EOT | 2 (9.52) | 13 (61.90) | 6 (28.57) | |||
| SVR | 10 (47.62) | 11 (52.38) | 0 (0.00) | |||
| 35–55 n (%) | BSL | 0 (0.00) | 7 (58.33) | 5 (41.67) | χ2(2) = 0.301 p 2 = 0.860 | χ2(2) = 0.654 p 2 = 0.721 |
| EOT | 0 (0.00) | 9 (75.00) | 3 (25.00) | |||
| SVR | 4 (33.33) | 7 (58.33) | 1 (8.34) | |||
| 56–65 n (%) | BSL | 0 (0.00) | 35 (85.37) | 6 (14.63) | ||
| EOT | 5 (12.20) | 33 (80.49) | 3 (7.32) | |||
| SVR | 14 (34.14) | 24 (58.54) | 3 (7.32) | |||
| 66–80 n (%) | BSL | 1 (2.70) | 29 (78.38) | 7 (18.92) | ||
| EOT | 5 (13.51) | 25 (67.57) | 7 (18.92) | |||
| SVR | 9 (24.32) | 28 (75.68) | 0 (0.00) | |||
| Group | Stage | PSS Score Level | BSL/EOT | EOT/SVR | ||
|---|---|---|---|---|---|---|
| Low | Moderate | High | ||||
| 17–24.9 n (%) | BSL | 1 (4.17) | 17 (70.83) | 6 (25.00) | χ2(3) = 2.798 p 1 = 0.424 | χ2(3) = 3.347 p 1 = 0.341 |
| EOT | 2 (8.33) | 15 (62.50) | 7 (29.17) | |||
| SVR | 5 (20.83) | 18 (75.00) | 1 (4.17) | |||
| 25–29.9 n (%) | BSL | 0 (0.00) | 33 (80.49) | 8 (19.51) | ||
| EOT | 2 (4.88) | 35 (85.37) | 4 (9.76) | |||
| SVR | 16 (39.02) | 23 (56.10) | 2 (4.88) | |||
| 30–34.9 n (%) | BSL | 0 (0.00) | 17 (85.00) | 3 (15.00) | ||
| EOT | 5 (25.00) | 13 (65.00) | 2 (10.00) | |||
| SVR | 3 (15.00) | 16 (80.00) | 1 (5.00) | |||
| 35–39.9 n (%) | BSL | 0 (0.00) | 4 (80.00) | 1 (20.00) | ||
| EOT | 1 (20.00) | 4 (80.00) | 0 (0.00) | |||
| SVR | 3 (60.00) | 2 (40.00) | 0 (0.00) | |||
| F2 n (%) | BSL | 0 (0.00) | 3 (100.00) | 0 (0.00) | χ2(2) = 2.202 p 1 = 0.333 | χ2(2) = 0.908 p 1 = 0.635 |
| EOT | 0 (0.00) | 3 (100.00) | 0 (0.00) | |||
| SVR | 1 (33.33) | 2 (66.67) | 0 (0.00) | |||
| F3 n (%) | BSL | 0 (0.00) | 29 (85.29) | 5 (14.71) | ||
| EOT | 4 (11.76) | 23 (67.65) | 7 (20.59) | |||
| SVR | 9 (26.47) | 23 (67.65) | 2 (5.88) | |||
| F4 n (%) | BSL | 1 (1.89) | 39 (73.58) | 13 (24.53) | ||
| EOT | 6 (11.32) | 41 (77.36) | 6 (11.32) | |||
| SVR | 17 (32.08) | 34 (64.15) | 2 (3.77) | |||
| Friedman | Pairwise Comparisons (p) | Median PSS Score | ||||||
|---|---|---|---|---|---|---|---|---|
| (χ2, p) | BSL-EOT | BSL-SVR | EOT-SVR | BSL | EOT | SVR | ||
| Gender | Female | 10.587; p = 0.005 | 0.090 | 0.007 | 1.000 | 31 | 29 | 27 |
| Male | 10.927; p = 0.004 | 1 | 0.041 | 0.006 | 31 | 31 | 21 | |
| Residence | Rural | 3.326; p = 0.190 | n/a | n/a | n/a | 31 | 30 | 28 |
| Urban | 16.738; p < 0.0005 | 0.076 | <0.0005 | 0.243 | 33 | 29.5 | 22 | |
| Age group (years) | 30–55 | 2.913; p = 0.023 | n/a | n/a | n/a | 34.5 | 31 | 26.5 |
| 56–65 | 9.713; p = 0.008 | 1 | 0.015 | 0.039 | 31 | 30 | 25 | |
| 66–80 | 5.348; p = 0.069 | n/a | n/a | n/a | 31 | 29 | 28 | |
| BMI (kg/m2) | 17–24.9 | 1.780; p = 0.411 | n/a | n/a | n/a | 32 | 30 | 28 |
| 25–29.9 | 9.686; p = 0.008 | 0.739 | 0.009 | 0.205 | 31 | 30 | 25 | |
| 30–34.9 | 4.430; p = 0.109 | n/a | n/a | n/a | 31 | 29 | 27.5 | |
| 35–39.9 | 7.444; p = 0.024 | 0.246 | 0.034 | 1 | 33 | 27 | 17 | |
| Fibrosis degree | F2 | 0.667; p = 0.717 | n/a | n/a | n/a | 29 | 31 | 28 |
| F3 | 2.800; p = 0.247 | n/a | n/a | n/a | 30 | 29.5 | 28 | |
| F4 | 14.539; p = 0.001 | 0.156 | 0.001 | 0.217 | 33 | 30 | 26 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danilescu, C.M.; Ionescu, M.; Sandulescu, D.L.; Pirlog, M.C.; Streba, C.T.; Rogoveanu, I. Perceived Stress in Hepatitis C Virus Infected Patients under the DAA-Based Therapy. Diagnostics 2022, 12, 1177. https://doi.org/10.3390/diagnostics12051177
Danilescu CM, Ionescu M, Sandulescu DL, Pirlog MC, Streba CT, Rogoveanu I. Perceived Stress in Hepatitis C Virus Infected Patients under the DAA-Based Therapy. Diagnostics. 2022; 12(5):1177. https://doi.org/10.3390/diagnostics12051177
Chicago/Turabian StyleDanilescu, Claudia Monica, Mihaela Ionescu, Daniela Larisa Sandulescu, Mihail Cristian Pirlog, Costin Teodor Streba, and Ion Rogoveanu. 2022. "Perceived Stress in Hepatitis C Virus Infected Patients under the DAA-Based Therapy" Diagnostics 12, no. 5: 1177. https://doi.org/10.3390/diagnostics12051177
APA StyleDanilescu, C. M., Ionescu, M., Sandulescu, D. L., Pirlog, M. C., Streba, C. T., & Rogoveanu, I. (2022). Perceived Stress in Hepatitis C Virus Infected Patients under the DAA-Based Therapy. Diagnostics, 12(5), 1177. https://doi.org/10.3390/diagnostics12051177