
Motor Fluctuations Development Is Associated with Non-Motor Symptoms Burden Progression in Parkinson’s Disease Patients: A 2-Year Follow-Up Study

 ,
,
Abstract
:1. Introduction
2. Material and Methods
3. Data Analysis
4. Standard Protocol Approvals, Registrations, and Patient Consents
5. Data Availability
6. Results
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
| Name (Last Name, First Name) | Location | Role | Contribution |
| Astrid Adarmes, Daniela | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Almeria, Marta | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Alonso Losada, Maria Gema | Hospital Álvaro Cunqueiro, Complejo Hospitalario Universitario de Vigo (CHUVI), Vigo, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Alonso Cánovas, Araceli | Hospital Universitario Ramón y Cajal, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Alonso Frech, Fernando | Hospital Universitario Clínico San Carlos, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Alonso Redondo, Ruben | Hospital Universitario Lucus Augusti (HULA), Lugo, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Aneiros Díaz, Ángel | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Álvarez, Ignacio | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Álvarez Sauco, María | Hospital General Universitario de Elche, Elche, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Arnáiz, Sandra | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Arribas, Sonia | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Ascunce Vidondo, Arancha | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Aguilar, Miquel | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Ávila Rivera, Maria Asunción | Consorci Sanitari Integral, Hospital General de L’Hospitalet, L’Hospitalet de Llobregat, Barcelona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Bernardo Lambrich, Noemí | Hospital de Tortosa Verge de la Cinta (HTVC), Tortosa, Tarragona, Spain | Site investigator | Evaluation of participants and/or data management |
| Bejr-Kasem, Helena | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Blázquez Estrada, Marta | Hospital Universitario Central de Asturias, Oviedo, Spain | Site investigator | Evaluation of participants and/or data management |
| Botí González, Maria Ángeles | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Borrué, Carmen | Hospital Infanta Sofía, Madrid, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Buongiorno, Maria Teresa | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Nurse study coordinator |
| Cabello González, Carolina | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Scheduling of evaluations |
| Cabo López, Iria | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Caballol, Nuria | Consorci Sanitari Integral, Hospital Moisés Broggi, Sant Joan Despí, Barcelona, Spain. | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Cámara Lorenzo, Ana | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator | Nurse study coordinator |
| Canfield Medina, Héctor | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Evaluation of participants and/or data management |
| Carrillo, Fátima | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Carrillo Padilla, Francisco José | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Casas, Elena | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Catalán, Maria José | Hospital Universitario Clínico San Carlos, Madrid, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Clavero, Pedro | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Cortina Fernández, A | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Coordination of blood extractions |
| Cosgaya, Marina | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Cots Foraster, Anna | Institut d’Assistència Sanitària (IAS)-Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| Crespo Cuevas, Ane | Hospital del Mar, Barcelona, Spain. | Site investigator | Evaluation of participants and/or data management |
| Cubo, Esther | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| De Deus Fonticoba, Teresa | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Nurse study coordinator Evaluation of participants and/or data management |
| De Fábregues-Boixar, Oriol | Hospital Universitario Vall d’Hebron, Barcelona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Díez Fairen, M | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Dotor García-Soto, Julio | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator/PI | Evaluation of participants and/or data management |
| Erro, Elena | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Escalante, Sonia | Hospital de Tortosa Verge de la Cinta (HTVC), Tortosa, Tarragona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Estelrich Peyret, Elena | Institut d’Assistència Sanitària (IAS)-Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| Fernández Guillán, Noelia | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Gámez, Pedro | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Gallego, Mercedes | Hospital La Princesa, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| García Caldentey, Juan | Centro Neurológico Oms 42, Palma de Mallorca, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| García Campos, Cristina | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| García Moreno, Jose Manuel | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator/PI (until MAR/21) | Coordination at the center Evaluation of participants and/or data management |
| Gastón, Itziar | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Gómez Garre, María del Pilar | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Genetic studies coordination |
| Gómez Mayordomo, Víctor | Hospital Clínico San Carlos, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| González Aloy, Javier | Institut d’Assistència Sanitària (IAS)-Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| González Aramburu, Isabel | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator | Evaluation of participants and/or data management |
| González Ardura, Jessica | Hospital Universitario Lucus Augusti (HULA), Lugo, Spain | Site investigator/PI (until FEB/21) | Evaluation of participants and/or data management |
| González García, Beatriz | Hospital La Princesa, Madrid, Spain | Site investigator | Nurse study coordinator |
| González Palmás, Maria Josefa | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator | Evaluation of participants and/or data management |
| González Toledo, Gabriel Ricardo | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator | Evaluation of participants and/or data management |
| Golpe Díaz, Ana | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Laboratory analysis coordination |
| Grau Solá, Mireia | Consorci Sanitari Integral, Hospital Moisés Broggi, Sant Joan Despí, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Guardia, Gemma | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Hernández Vara, Jorge | Hospital Universitario Vall d’Hebron, Barcelona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Horta Barba, Andrea | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Idoate Calderón, Daniel | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigaor | neuropsychologist; evaluation of participants |
| Infante, Jon | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Jesús, Silvia | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Kulisevsky, Jaime | Hospital de Sant Pau, Barcelona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Kurtis, Mónica | Hospital Ruber Internacional, Madrid, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Labandeira, Carmen | Hospital Álvaro Cunqueiro, Complejo Hospitalario Universitario de Vigo (CHUVI), Vigo, Spain | Site investigator | Evaluation of participants and/or data management |
| Labrador Espinosa, Miguel Ángel | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Neuroimaging data analysis |
| Lacruz, Francisco | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Lage Castro, Melva | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator | Evaluation of participants and/or data management |
| Lastres Gómez, Sonia | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Legarda, Inés | Hospital Universitario Son Espases, Palma de Mallorca, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| López Ariztegui, Nuria | Complejo Hospitalario de Toledo, Toledo, Spain | Site investigator/PI | Evaluation of participants and/or data management |
| López Díaz, Luis Manuel | Hospital Da Costa de Burela, Lugo, Spain | Site investigator | Evaluation of participants and/or data management |
| López Domínguez, Daniel | Institut d’Assistència Sanitària (IAS)-Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| López Manzanares, Lydia | Hospital La Princesa, Madrid, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| López Seoane, Balbino | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Lucas del Pozo, Sara | Hospital Universitario Vall d’Hebron, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Macías, Yolanda | Fundación Hospital de Alcorcón, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Mata, Marina | Hospital Infanta Sofía, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Martí Andres, Gloria | Hospital Universitario Vall d’Hebron, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Martí, Maria José | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Martínez Castrillo, Juan Carlos | Hospital Universitario Ramón y Cajal, Madrid, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Martinez-Martin, Pablo | Centro Nacional de Epidemiología y CIBERNED, Instituto de Salud Carlos III. Madrid | Collaborator in statistical and methods analysis | Methods and statistical reviewer |
| McAfee, Darrian | University of Pennsylvania, Philadelphia | Collaborator in English style | English style reviewer |
| Meitín, Maria Teresa | Hospital Da Costa de Burela, Lugo, Spain | Site investigator | Evaluation of participants and/or data management |
| Menéndez González, Manuel | Hospital Universitario Central de Asturias, Oviedo, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Méndez del Barrio, Carlota | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Mendoza Plasencia, Zebenzui | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator | Evaluation of participants and/or data management |
| Mir, Pablo | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Miranda Santiago, Javier | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Morales Casado, Maria Isabel | Complejo Hospitalario de Toledo, Toledo, Spain. | Site investigator | Evaluation of participants and/or data management |
| Moreno Diéguez, Antonio | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Nogueira, Víctor | Hospital Da Costa de Burela, Lugo, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Novo Amado, Alba | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Novo Ponte, Sabela | Hospital Universitario Puerta de Hierro, Madrid, Spain. | Site investigator | Evaluation of participants and/or data management |
| Ordás, Carlos | Hospital Rey Juan Carlos, Madrid, Spain, Madrid, Spain. | Site investigator | Evaluation of participants and/or data management |
| Pagonabarraga, Javier | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Pareés, Isabel | Hospital Ruber Internacional, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Pascual-Sedano, Berta | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Pastor, Pau | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Pérez Fuertes, Aída | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Blood analysis |
| Pérez Noguera, Rafael | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Planas-Ballvé, Ana | Consorci Sanitari Integral, Hospital Moisés Broggi, Sant Joan Despí, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Planellas, Lluís | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator (until DEC/19) | Evaluation of participants and/or data management |
| Prats, Marian Ángeles | Institut d’Assistència Sanitària (IAS)-Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| Prieto Jurczynska, Cristina | Hospital Rey Juan Carlos, Madrid, Spain, Madrid, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Puente, Víctor | Hospital del Mar, Barcelona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Pueyo Morlans, Mercedes | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator | Evaluation of participants and/or data management |
| Puig Daví, Arnau | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Redondo, Nuria | Hospital La Princesa, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Rodríguez Méndez, Luisa | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Blood analysis |
| Rodríguez Pérez, Amparo Belén | Hospital General Universitario de Elche, Elche, Spain | Site investigator | Evaluation of participants and/or data management |
| Roldán, Florinda | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Neuroimaging studies |
| Ruíz de Arcos, María | Hospital Universitario Virgen Macarena, Sevilla, Spain. | Site investigator | Evaluation of participants and/or data management |
| Ruíz Martínez, Javier | Hospital Universitario Donostia, San Sebastián, Spain | Site investigator | Evaluation of participants and/or data management |
| Sánchez Alonso, Pilar | Hospital Universitario Puerta de Hierro, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Sánchez-Carpintero, Macarena | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Sánchez Díez, Gema | Hospital Universitario Ramón y Cajal, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Sánchez Rodríguez, Antonio | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator | Evaluation of participants and/or data management |
| Santacruz, Pilar | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Santos García, Diego | CHUAC, Complejo Hospitalario Universitario de A Coruña | Coordinator of the Project | Coordination of the COPPADIS-2015 |
| Segundo Rodríguez, José Clemente | Complejo Hospitalario de Toledo, Toledo, Spain | Site investigator | Evaluation of participants and/or data management |
| Seijo, Manuel | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Sierra, María | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator | Evaluation of participants and/or data management |
| Solano, Berta | Institut d’Assistència Sanitària (IAS)-Instituí Cátala de la Salud. Girona, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Suárez Castro, Ester | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Evaluation of participants and/or data management |
| Tartari, Juan Pablo | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Valero, Caridad | Hospital Arnau de Vilanova, Valencia, Spain | Site investigator | Evaluation of participants and/or data management |
| Vargas, Laura | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Vela, Lydia | Fundación Hospital de Alcorcón, Madrid, Spain | Site investigator/PI | Coordination at the center Evaluation of participants and/or data management |
| Villanueva, Clara | Hospital Universitario Clínico San Carlos, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Vives, Bárbara | Hospital Universitario Son Espases, Palma de Mallorca, Spain | Site investigator | Evaluation of participants and/or data management |
References
- Bloem, B.R.; Okun, M.S.; Klein, C. Parkinson’s disease. Lancet 2021, 397, 2284–2303. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef]
- Schapira, A.; Chaudhuri, K.; Jenner, P. Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 435–450. [Google Scholar] [CrossRef]
- Seppi, K.; Ray Chaudhuri, K.; Coelho, M.; Fox, S.H.; Katzenschlager, R.; Lloret, S.P.; Weintraub, D.; Sampaio, C.; the Collaborators of the Parkinson’s Disease Update on Non-Motor Symptoms Study Group on behalf of the Movement Disorders Society Evidence-Based Medicine Committee. Update on treatments for non-motor symptoms of Parkinson’s disease—An evidence-based medicine review. Mov. Disord. 2019, 34, 180–198. [Google Scholar] [CrossRef] [Green Version]
- Chaudhuri, K.R.; Schapira, A.H. Non-motor symptoms of Parkinson’s disease: Dopaminergic pathophysiology and treatment. Lancet Neurol. 2009, 8, 464–474. [Google Scholar] [CrossRef]
- Mattay, V.; Tessitore, A.; Callicott, J.; Bertolino, A.; Goldberg, T.E.; Chase, T.N.; Hyde, T.M.; Weinberger, D.R. Dopaminergic modulation of cortical function in patients with Parkinson’s disease. Ann. Neurol. 2002, 51, 156–164. [Google Scholar] [CrossRef]
- Barone, P.; Scarzella, L.; Marconi, R.; Antonini, A.; Morgante, L.; Bracco, F.; Zappia, M.; Musch, B.; the Depression/Parkinson Italian Study Group. Pramipexole versus sertraline in the treatment of depression in Parkinson’s disease. A national multicenter parallel group randomized study. J. Neurol. 2006, 253, 601–607. [Google Scholar] [CrossRef]
- Fernández-Pajarín, G.; Sesar, Á.; Jiménez Martín, I.; Ares, B.; Castro, A. Continuous subcutaneous apomorphine infusion in the early phase of advanced Parkinson’s disease: A prospective study of 22 patients. Clin. Park. Relat. Disord. 2021, 6, 100129. [Google Scholar] [CrossRef]
- Trenkwalder, C.; Kies, B.; Rudzinska, M.; Fine, J.; Nikl, J.; Honczarenko, K.; Dioszeghy, P.; Hill, D.; Anderson, T.; Myllyla, V.; et al. Recover Study Group. Rotigotine effects on early morning motor function and sleep in Parkinson’s disease: A double-blind, randomized, placebo-controlled study (RECOVER). Mov. Disord. 2011, 26, 90–99. [Google Scholar] [CrossRef]
- Martinez-Castrillo, J.C.; Vela, L.; del Val, J.; Alonso-Canovas, A. Non-motor disorders and their correlation with dopamine: Can they be treated by currently available methods? Neurologist 2011, 17 (Suppl. 1), S9–S17. [Google Scholar] [CrossRef]
- Martínez-Fernández, R.; Schmitt, E.; Martinez-Martin, P.; Krack, P. The hidden sister of motor fluctuations in Parkinson’s disease: A review on non-motor fluctuations. Mov. Disord. 2016, 31, 1080–1094. [Google Scholar] [CrossRef]
- Witjas, T.; Kaphan, E.; Azulay, J.P.; Blin, O.; Ceccaldi, M.; Pouget, J.; Poncet, M.; Chérif, A.A. Non-motor fluctuations in Parkinson’s disease: Frequent and disabling. Neurology 2002, 59, 408–413. [Google Scholar] [CrossRef]
- Honig, H.; Antonini, A.; Martinez-Martin, P.; Forgacs, I.; Faye, G.C.; Fox, T.; Fox, K.; Mancini, F.; Canesi, M.; Odin, P.; et al. Intrajejunal levodopa infusion in Parkinson’s disease: A pilot multicenter study of effects on non-motor symptoms and quality of life. Mov. Disord. 2009, 24, 1468–1474. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Reddy, P.; Katzenschlager, R.; Antonini, A.; Todorova, A.; Odin, P.; Henriksen, T.; Martin, A.; Calandrella, D.; Rizos, A.; et al. EuroInf: A multicenter comparative observational study of apomorphine and levodopa infusion in Parkinson’s disease. Mov. Disord. 2015, 30, 510–516. [Google Scholar] [CrossRef]
- Santos García, D.; Labandeira Guerra, C.; Yáñez Baña, R.; Cimas Hernando, M.I.; Cabo López, I.; Paz Gonález, J.M.; Alonso Losada, M.G.; González Palmás, M.J.; Martínez Miró, C. Safinamide Improves Non-Motor Symptoms Burden in Parkinson’s Disease: An Open-Label Prospective Study. Brain Sci. 2021, 11, 316. [Google Scholar] [CrossRef]
- Santos García, D.; Fernández-Pajarín, G.; Oropesa Ruíz, J.M.; Escamilla Sevilla, F.; Rahim López, R.R.A.; Muñoz Enríquez, J.G. Opicapone Improves Global Non-Motor Symptoms Burden in Parkinson´s Disease: An Open-label Prospective Study. Brain Sci. 2022, 12, 383. [Google Scholar] [CrossRef]
- Santos-García, D.; de Deus Fonticoba, T.; Suárez Castro, E.; Díaz, A.A.; McAfee, D.; Catalán, M.J.; Alonso-Frech, F.; Villanueva, C.; Jesús, S.; Mir, P.; et al. Non-motor symptom burden is strongly correlated to motor complications in patients with Parkinson’s disease. Eur. J. Neurol. 2020, 27, 1210–1223. [Google Scholar] [CrossRef]
- Santos García, D.; De Deus Fonticoba, T.; Paz González, J.M.; Bartolomé, C.C.; Aymerich, L.V.; Enríquez, J.G.M.; Suárez, E.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. Staging Parkinson’s Disease Combining Motor and Non-motor Symptoms Correlates with Disability and Quality of Life. Parkinsons Dis. 2021, 2021, 8871549. [Google Scholar]
- Santos García, D.; de Deus Fonticoba, T.; Cores, C.; Muñoz, G.; Paz González, J.M.; Martínez Miró, C.; Suárez, E.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. Predictors of clinically significant quality of life impairment in Parkinson’s disease. NPJ Parkinsons Dis. 2021, 7, 118. [Google Scholar] [CrossRef]
- Malaty, I.A.; Martinez-Martin, P.; Chaudhuri, K.R.; Odin, P.; Skorvanek, M.; Jimenez-Shahed, J.; Soileau, M.J.; Lindvall, S.; Domingos, J.; Jones, S.; et al. Does the 5-2-1 criteria identify patients with advanced Parkinson’s disease? Real-world screening accuracy and burden of 5-2-1-positive patients in 7 countries. BMC Neurol. 2022, 22, 35. [Google Scholar] [CrossRef]
- Santos García, D.; Jesús, S.; Aguilar, M.; Planellas, L.L.; Caldentey, J.G.; Caballol, N.; Legarda, I.; Hernández Vara, J.; Cabo, I.; Manzanares, L.L.; et al. COPPADIS-2015 (COhort of Patients with Parkinson’s DIsease in Spain, 2015): An ongoing global Parkinson’s disease project about disease progression with more than 1000 subjects included. Results from the baseline evaluation. Eur. J. Neurol. 2019, 26, 1399–1407. [Google Scholar] [CrossRef]
- Santos-García, D.; Mir, P.; Cubo, E.; Vela, L.; Rodríguez-Oroz, M.C.; Martí, M.J.; Arbelo, J.M.; Infante, J.; Kulisevsky, J.; Martínez-Martín, P.; et al. COPPADIS-2015 (COhort of Patients with Parkinson’s DIsease in Spain, 2015), a global--clinical evaluations, serum biomarkers, genetic studies and neuroimaging--prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol. 2016, 16, 26. [Google Scholar]
- Fahn, S.; Elton, R.L.; Members of the UPDRS Development Committee. Unified Parkinson’s Disease Rating Scale. In Recent Developments in Parkinson’s Disease; Fahn, S., Marsden, C.D., Calne, D.B., Goldstein, M., Eds.; Macmillan Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–164. [Google Scholar]
- Chaudhuri, K.R.; Martinez-Martin, P.; Brown, R.G.; Sethi, K.; Stocchi, F.; Odin, P.; Ondo, W.; Abe, K.; MacPhee, G.; MacMahon, D.; et al. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: Results from an international pilot study. Mov. Disord. 2007, 22, 1901–1911. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Kurtis, M.M.; Chaudhuri, K.R.; NMSS Validation Group. The impact of non-motor symptoms on health-related quality of life of patients with Parkinson’s disease. Mov. Disord. 2011, 26, 399–406. [Google Scholar] [CrossRef]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson´s Disease Questionnaire (PDQ-39): Development and validation of a Parkinson´s disease summary index score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Da Rocha, N.S.; Power, M.J.; Bushnell, D.M.; Fleck, M.P. The EUROHIS-QOL 8-item index: Comparative psychometric properties to its parent WHOQOL-BREF. Value Health 2012, 15, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Barone, P.; Antonini, A.; Colosimo, C.; Marconi, R.; Morgante, L.; Avarello, T.P.; Bottacchi, E.; Cannas, A.; Ceravolo, G.; Ceravolo, R.; et al. The PRIAMO study: A multicenter assessment of non-motor symptoms and their impact on quality of life in Parkinson’s disease. Mov. Disord. 2009, 24, 1641–1649. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Abe, K.; Bhattacharyya, K.B.; Bloem, B.R.; Carod-Artal, F.J.; Prakash, R.; Esselink, R.A.J.; Falup-Pecurariu, C.; Gallardo, M.; et al. International study on the psychometric attributes of the non-motor symptoms scale in Parkinson disease. Neurology 2009, 73, 1584–1591. [Google Scholar] [CrossRef]
- Hauser, R.A.; McDermott, M.P.; Messing, S. Factors associated with the development of motor fluctuations and dyskinesias in Parkinson disease. Arch. Neurol. 2006, 63, 1756–1760. [Google Scholar] [CrossRef]
- Ahlskog, J.E.; Muenter, M.D. Frequency of levodopa-related dyskinesias and motor fluctuations as estimated from the cumulative literature. Mov. Disord. 2001, 16, 448–458. [Google Scholar] [CrossRef]
- Barrachina-Fernández, M.; Maitín, A.M.; Sánchez-Ávila, C.; Romero, J.P. Wearable Technology to Detect Motor Fluctuations in Parkinson’s Disease Patients: Current State and Challenges. Sensors 2021, 21, 4188. [Google Scholar] [CrossRef]
- Stocchi, F.; Antonini, A.; Barone, P.; Tinazzi, M.; Zappia, M.; Onofrj, M.; Ruggieri, S.; Morgante, L.; Bonuccelli, U.; Lopiano, L.; et al. Early DEtection of wEaring off in Parkinson disease: The DEEP study. Parkinsonism Relat. Disord. 2014, 20, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Fox, S.H.; Katzenschlager, R.; Lim, S.Y.; Barton, B.; De Bie, R.M.A.; Seppi, K.; Coelho, M.; Sampaio, C.; Movement Disorder Society Evidence-Based Medicine Committee. International Parkinson and movement disorder society evidence-based medicine review: Update on treatments for the motor symptoms of Parkinson’s disease. Mov. Disord. 2018, 33, 1248–1266. [Google Scholar] [CrossRef]
- Antonini, A.; Barone, P.; Marconi, R.; Morgante, L.; Zappulla, S.; Pontieri, F.E.; Ramat, S.; Ceravolo, M.G.; Meco, G.; Cicarelli, G.; et al. The progression of non-motor symptoms in Parkinson’s disease and their contribution to motor disability and quality of life. J. Neurol. 2012, 259, 2621–2631. [Google Scholar] [CrossRef]
- Todorova, A.; Jenner, P.; Ray Chaudhuri, K. Non-motor parkinson’s: Integral to motor parkinson’s, yet often neglected. Pract. Neurol. 2014, 14, 310–322. [Google Scholar] [CrossRef]
- Fernandes, M.; Pierantozzi, M.; Stefani, A.; Cattaneo, C.; Bonizzoni, E.A.; Cerroni, R.; Mercuri, N.B.; Liguori, C. Frequency of Non-motor Symptoms in Parkinson’s Patients With Motor Fluctuations. Front. Neurol. 2021, 12, 678373. [Google Scholar] [CrossRef]
- Watanabe, H.; Saiki, H.; Chiu, S.W.; Yamaguchi, T.; Kashihara, K.; Tsuboi, Y.; Nomoto, M.; Hattori, N.; Maeda, T.; Shimo, Y.; et al. Real-World Non-motor Changes I Patients with Parkinson’s Disease and Motor Fluctuations: J-FIRST. Mov. Disord. Clin. Pract. 2020, 7, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Santos-García, D.; de Deus, T.; Cores, C.; Canfield, H.; Paz González, J.M.; Martínez Miró, C.; Valdés Aymerich, L.; Suárez, E.; Jesús, S.; Aguilar, M.; et al. Predictors of Global Non-Motor Symptoms Burden Progression in Parkinson’s Disease. Results from the COPPADIS Cohort at 2-Year Follow-Up. J. Pers. Med. 2021, 11, 626. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Schrag, A.; Weintraub, D.; Rizos, A.; Rodriguez-Blazquez, C.; Mamikonyan, E.; Martinez-Martin, P. The movement disorder society non-motor rating scale: Initial validation study. Mov. Disord. 2020, 35, 116–133. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chen, R.S.; Weng, Y.H.; Huang, Y.-Z.; Chen, C.C.; Hung, J.; Lin, Y.-Y. The severity progression of non-motor symptoms in Parkinson’s disease: A 6-year longitudinal study in Taiwanese patients. Sci. Rep. 2021, 11, 14781. [Google Scholar] [CrossRef]
- Ou, R.; Yang, J.; Cao, B.; Wei, Q.; Chen, K.; Chen, X.; Zhao, B.; Wu, Y.; Song, W.; Shang, H. Progression of non-motor symptoms in Parkinson’s disease among different age populations: A two-year follow-up study. J. Neurol. Sci. 2016, 360, 72–77. [Google Scholar] [CrossRef]
- Cilia, R.; Akpalu, A.; Sarfo, F.S.; Cham, M.; Amboni, M.; Cereda, E.; Fabbri, M.; Adjei, P.; Akassi, J.; Bonetti, A.; et al. The modern pre-levodopa era of Parkinson’s disease: Insights into motor complications from sub-Saharan Africa. Brain 2014, 137 Pt 10, 2731–2742. [Google Scholar] [CrossRef] [Green Version]
- Simuni, T.; Caspell-Garcia, C.; Coffey, C.S.; Weintraub, D.; Mollenhauer, B.; Lasch, S.; Tanner, C.M.; Jennings, D.; Kieburtz, K.; Chahine, L.M.; et al. Baseline prevalence and longitudinal evolution of non-motor symptoms in early Parkinson’s disease: The PPMI cohort. J. Neurol. Neurosurg. Psychiatry 2018, 89, 78–88. [Google Scholar] [CrossRef] [Green Version]
- Bugalho, P.; Ladeira, F.; Barbosa, R.; Marto, J.P.; Borbinha, C.; Da Conceição, L.; Salavisa, M.; Saraiva, M.; Meira, B.; Fernandes, M. Progression in Parkinson’s Disease: Variation in Motor and Non-motor Symptoms Severity and Predictors of Decline in Cognition, Motor Function, Disability, and Health-Related Quality of Life as Assessed by Two Different Methods. Mov. Disord. Clin. Pract. 2021, 8, 885–895. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| All Sample (N = 330) | nonMF at V2 (N = 239) | MF at V2 (N = 91) | p | |
|---|---|---|---|---|
| Males (%) | 58.8 | 59.8 | 56 | 0.308 |
| At V0 | ||||
| Age | 62.67 ± 8.7 | 63.41 ± 8.46 | 60.75 ± 9.06 | 0.012 |
| Years from symptoms onset | 4.13 ± 3.3 | 3.65 ± 3.09 | 5.36 ± 3.51 | <0.0001 |
| Time on levodopa therapy (months) | 18.99 ± 27.99 | 14.71 ± 24.37 | 29.65 ± 33.25 | <0.0001 |
| Daily dose of levodopa (mg/day) | 231.85 ± 257.89 | 175.74 ± 216.46 | 379.62 ± 298.07 | <0.0001 |
| DA equivalent daily dose (mg/day) | 152.77 ± 149.36 | 143.21 ± 148.24 | 177.96 ± 150.18 | 0.047 |
| LEDD (mg/day) | 437.71 ± 325.85 | 372.62 ± 283.4 | 609.1 ± 367.38 | <0.0001 |
| H&Y stage (OFF) | 0.277 | |||
| Stage from 1 to 3 | 99.7 | 100 | 98.8 | |
| Stage from 4 to 5 | 0.3 | 0 | 1.2 | |
| UPDRS-III (OFF) | 18.9 ± 9.54 | 17.57 ± 8.81 | 22.4 ± 10.51 | <0.0001 |
| UPDRS-IV | 0.71 ± 0.87 | 0.66 ± 0.79 | 0.86 ± 1.05 | 0.241 |
| FOGQ | 1.97 ± 3.13 | 1.56 ± 2.51 | 3.06 ± 4.19 | <0.0001 |
| Tremotic motor phenotype (%) | 55.5 | 59 | 46.2 | 0.024 |
| PD-CRS | 92.93 ± 15.17 | 92.32 ± 15.39 | 94.51 ± 14.55 | 0.205 |
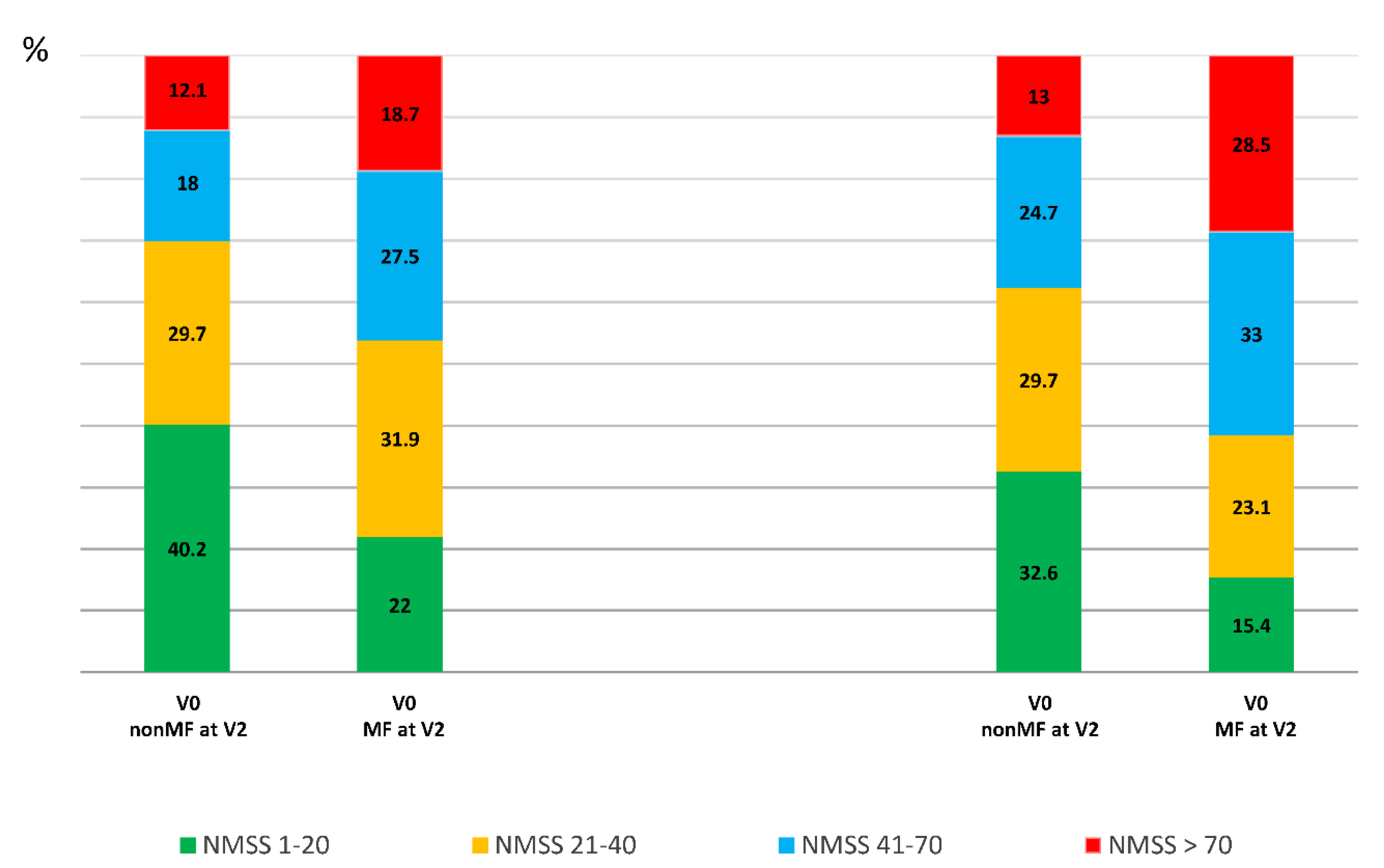
| NMSS | 37.62 ± 31.69 | 34.3 ± 29.07 | 46.34 ± 36.48 | 0.001 |
| BDI-II | 7.49 ± 6.63 | 6.98 ± 6.33 | 8.82 ± 7.22 | 0.037 |
| PDSS | 119.82 ± 23.36 | 122.41 ± 22.02 | 113.01 ± 25.45 | <0.0001 |
| QUIP-RS | 3.68 ± 7.44 | 2.72 ± 5.94 | 6.42 ± 10.15 | <0.0001 |
| NPI | 4.43 ± 6.62 | 4.22 ± 6.41 | 4.95 ± 7.13 | 0.381 |
| VAS–PAIN | 2.31 ± 2.8 | 2.22 ± 2.76 | 2.54 ± 2.91 | 0.363 |
| VASF–physical | 2.43 ± 2.57 | 2.27 ± 2.54 | 2.86 ± 2.61 | 0.050 |
| VASF–mental | 1.86 ± 2.45 | 1.75 ± 2.42 | 2.17 ± 2.51 | 0.084 |
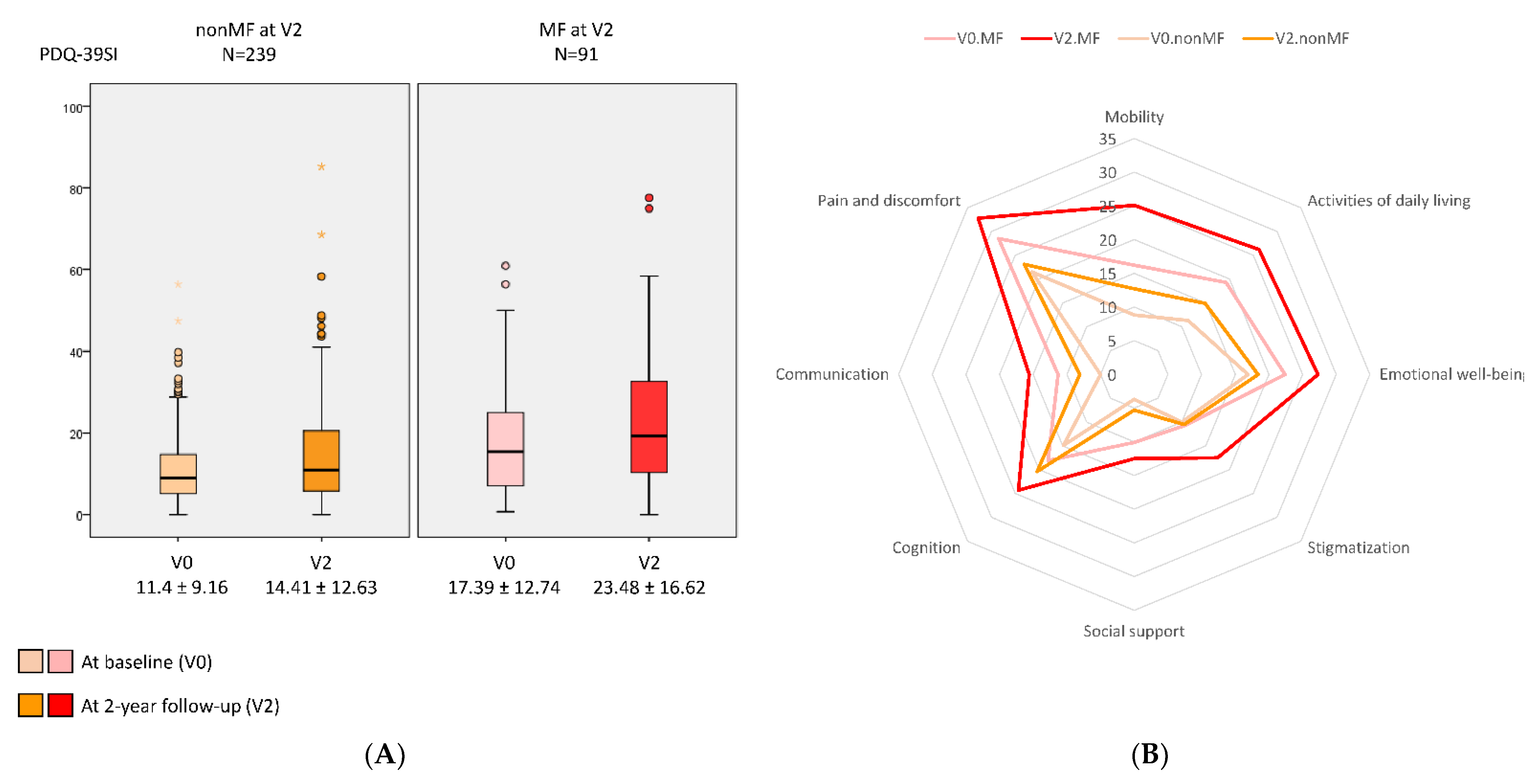
| PDQ-39SI | 13.08 ± 10.59 | 11.44 ± 9.16 | 17.39 ± 12.74 | <0.0001 |
| EUROHIS-QOL8 | 3.87 ± 0.51 | 3.92 ± 0.5 | 3.74 ± 0.49 | 0.006 |
| S&E-ADLS | 91.12 ± 8.04 | 92.05 ± 7.24 | 88.68 ± 9.45 | 0.001 |
| Change at V2 (V2 vs. V0) | ||||
| Daily dose of levodopa (mg/day) | +126.73 ± 190.01 | +113.37 ± 186.82 | +161.89 ± 208.83 | 0.021 |
| DA equivalent daily dose (mg/day) | +13.35 ± 188.95 | +6.32 ± 117.41 | +31.85 ± 306.18 | 0.288 |
| LEDD (mg/day) | +190.55 ± 278.38 | +158.22 ± 222.42 | +275.65 ± 377.62 | 0.008 |
| UPDRS-III (OFF) | +3.5 ± 9.73 | +2.11 ± 8.61 | +7.01 ± 11.46 | <0.0001 |
| UPDRS-IV | +1.02 ± 2.09 | +0.09 ± 1.03 | +3.5 ± 2.18 | <0.0001 |
| FOGQ | +1.37 ± 3.63 | +0.94 ± 3.18 | +2.52 ± 4.44 | 0.001 |
| PD-CRS | −0.9 ± 10.87 | −0.79 ± 11.49 | −1.19 ± 9.11 | 0.873 |
| NMSS | +8.91 ± 29.77 | +6.2 ± 25.8 | +16.03 ± 37.37 | 0.021 |
| BDI-II | +0.46 ± 7.16 | +0.33 ± 7.2 | +0.8 ± 7.07 | 0.463 |
| PDSS | +0.61 ± 23.46 | +1.05 ± 22.26 | −0.55 ± 26.42 | 0.654 |
| QUIP-RS | +0.79 ± 8.74 | +0.93 ± 7.45 | +0.42 ± 11.56 | 0.564 |
| NPI | +0.4 ± 8.45 | −0.23 ± 8.51 | +1.89 ± 8.15 | 0.270 |
| VAS–PAIN | +0.47 ± 3.15 | +0.33 ± 3.13 | +0.86 ± 3.17 | 0.109 |
| VASF–physical | +0.57 ± 2.84 | +0.42 ± 2.85 | +0.94 ± 2.79 | 0.216 |
| VASF–mental | +0.12 ± 2.75 | −0.07 ± 2.61 | +0.65 ± 3.04 | 0.062 |
| PDQ-39SI | +3.85 ± 10.18 | +3.01 ± 9.15 | +6.09 ± 12.28 | 0.005 |
| EUROHIS-QOL8 | −0.05 ± 0.56 | −0.03 ± 0.55 | −0.12 ± 0.58 | 0.249 |
| S&E-ADLS | −3.87 ± 9.73 | −3.4 ± 9.35 | −5.11 ± 10.62 | 0.177 |
| nonMF at V2 V0 | nonMF at V2 V2 | Cohen’s Test | p a | MF at V2 V0 | MF at V2 V2 | Cohen’s Test | p b | p c | p d | |
|---|---|---|---|---|---|---|---|---|---|---|
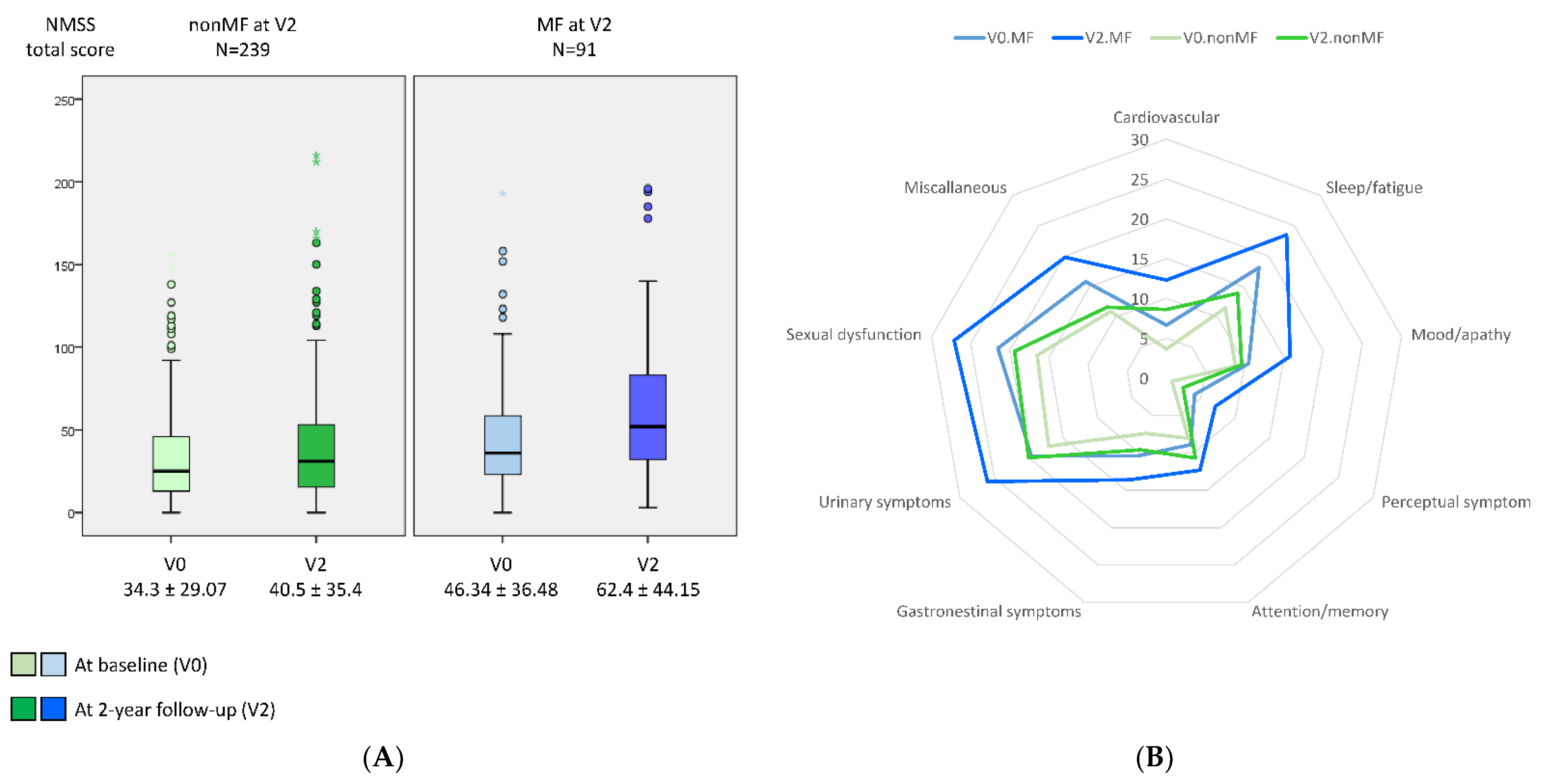
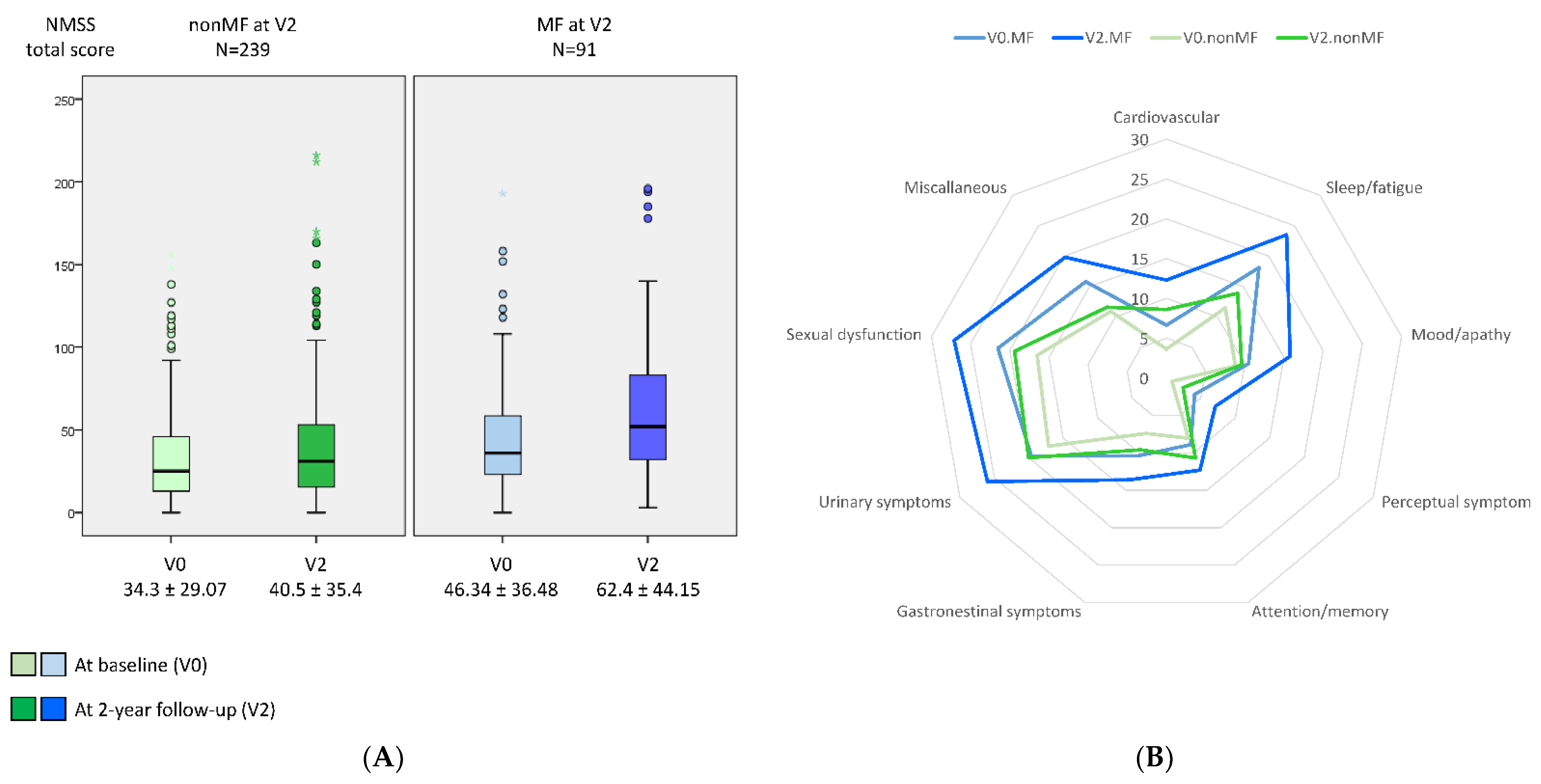
| NMSS | 34.3 ± 29.07 | 40.5 ± 35.4 | 0.33 | <0.0001 | 46.34 ± 36.48 | 62.37 ± 44.15 | 0.57 | 0.003 | 0.387 | 0.005 |
| Cardiovascular | 3.63 ± 7.35 | 8.66 ± 12.36 | 0.61 | <0.0001 | 6.63 ± 10.22 | 12.36 ± 13.78 | 0.54 | 0.002 | 0.973 | 0.240 |
| Sleep/fatigue | 11.52 ± 13.03 | 13.91 ± 15.09 | 0.24 | 0.024 | 18.09 ± 16.8 | 23.53 ± 18.47 | 0.39 | 0.027 | 0.069 | 0.104 |
| Mood/apathy | 8.86 ± 13.56 | 9.68 ± 15.51 | 0.09 | 0.101 | 10.51 ± 16 | 15.82 ± 18.13 | 0.46 | 0.012 | 0.090 | 0.261 |
| Perceptual symptoms | 0.87 ± 3.48 | 2.41 ± 8.09 | 0.31 | 0.002 | 4.17 ± 8.84 | 7.11 ± 16 | 0.31 | 0.080 | 0.672 | 0.105 |
| Attention/memory | 8.05 ± 12.6 | 10.75 ± 16.24 | 0.27 | 0.002 | 8.93 ± 11.51 | 12.36 ± 15.78 | 0.32 | 0.062 | 0.736 | 0.175 |
| Gastrointestinal symptoms | 7.41 ± 10.67 | 9.61 ± 11.95 | 0.32 | <0.0001 | 10.42 ± 14.81 | 13.64 ± 15.02 | 0.31 | 0.168 | 0.852 | 0.580 |
| Urinary symptoms | 17.45 ± 19.77 | 20.09 ± 21.92 | 0.21 | 0.035 | 19.63 ± 20.42 | 26 ± 23.95 | 0.43 | 0.042 | 0.923 | 0.532 |
| Sexual dysfunction | 16.58 ± 25.16 | 19.4 ± 26.65 | 0.14 | 0.119 | 21.55 ± 28.26 | 27.1 ± 27.55 | 0.24 | 0.128 | 0.980 | 0.082 |
| Miscellaneous | 10.96 ± 13.06 | 11.68 ± 12.83 | 0.07 | 0.945 | 15.84 ± 16.16 | 19.84 ± 16 | 0.34 | <0.0001 | 0.058 | 0.060 |
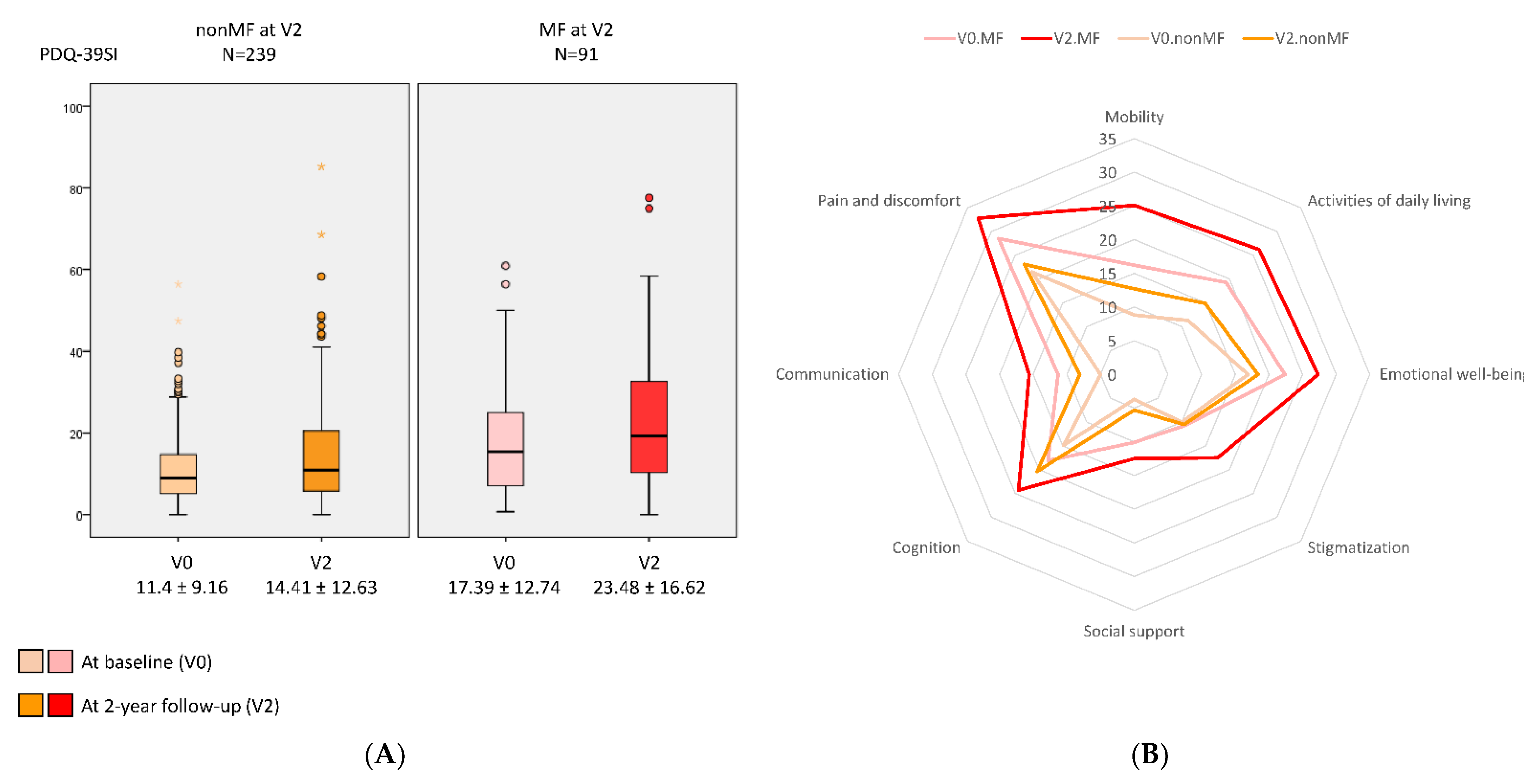
| PDQ-39SI | 11.4 ± 9.16 | 14.41 ± 12.63 | 0.46 | <0.0001 | 17.39 ± 12.74 | 23.48 ± 16.62 | 0.65 | <0.0001 | 0.397 | 0.002 |
| Mobility | 8.84 ± 12.67 | 12.76 ± 15.86 | 0.42 | <0.0001 | 16.2 ± 18.23 | 25.11 ± 22.48 | 0.69 | <0.0001 | 0.034 | N. A. |
| Activities of daily living | 11.35 ± 13.19 | 14.98 ± 26.2 | 0.32 | 0.006 | 19.35 ± 19.34 | 26.2 ± 21.37 | 0.46 | 0.002 | 0.224 | 0.271 |
| Emotional well-being | 16.91 ± 17.25 | 18.41 ± 21.8 | 0.15 | 0.167 | 22.36 ± 20.74 | 27.38 ± 24.33 | 0.35 | 0.089 | 0.852 | 0.576 |
| Stigmatization | 10.03 ± 16.81 | 10.5 ± 18.63 | 0.05 | 0.477 | 10.7 ± 14.64 | 17.5 ± 22.91 | 0.46 | 0.002 | 0.032 | N. A. |
| Social support | 3.76 ± 10.59 | 5.3 ± 12.77 | 0.17 | 0.074 | 10.06 ± 17.04 | 12.59 ± 21.46 | 0.16 | 0.396 | 0.861 | 0.224 |
| Cognition | 14.94 ± 15.84 | 20.4 ± 18.11 | 0.49 | <0.0001 | 18.05 ± 16.82 | 24.3 ± 22.43 | 0.42 | 0.027 | 0.833 | 0.424 |
| Communication | 5.01 ± 9.05 | 8.19 ± 14.68 | 0.33 | <0.0001 | 11.34 ± 17.09 | 15.64 ± 19.42 | 0.26 | 0.056 | 0.574 | 0.387 |
| Pain and discomfort | 20.65 ± 18.82 | 23.97 ± 22.12 | 0.16 | 0.071 | 28.55 ± 20.01 | 32.87 ± 24.33 | 0.30 | 0.015 | 0.432 | 0.039 |
| EUROHIS-QOL8 | 3.92 ± 0.5 | 3.89 ± 0.57 | −0.07 | 0.699 | 3.74 ± 0.49 | 2.62 ± 0.54 | −0.21 | 0.120 | 0.109 | 0.030 |
| Quality of life | 3.96 ± 0.67 | 3.82 ± 0.77 | −0.17 | 0.047 | 3.82 ± 0.61 | 3.57 ± 0.75 | −0.44 | 0.005 | 0.148 | 0.281 |
| Health status | 3.4 ± 0.82 | 3.46 ± 0.87 | +0.22 | 0.116 | 3.13 ± 0.81 | 3.11 ± 0.88 | −0.12 | 0.903 | 0.071 | 0.266 |
| Energy | 3.99 ± 0.73 | 3.9 ± 0.84 | −0.14 | 0.322 | 3.64 ± 0.81 | 3.49 ± 3.83 | −0.19 | 0.318 | 0.249 | 0.002 |
| Autonomy for ADL | 3.82 ± 0.81 | 3.82 ± 0.85 | 0.00 | 0.967 | 3.57 ± 0.81 | 3.44 ± 0.79 | −0.25 | 0.372 | 0.136 | 0.058 |
| Self-esteem | 3.9 ± 0.71 | 3.95 ± 0.76 | +0.04 | 0.449 | 3.8 ± 0.73 | 3.69 ± 0.77 | −0.10 | 0.078 | 0.003 | N. A. |
| Social relationships | 4.12 ± 0.61 | 4.03 ± 3.72 | −0.15 | 0.046 | 3.97 ± 0.67 | 3.82 ± 0.75 | −0.24 | 0.052 | 0.115 | 0.069 |
| Economic capacity | 3.93 ± 0.81 | 3.89 ± 0.78 | −0.06 | 0.795 | 3.81 ± 0.74 | 3.64 ± 0.83 | −0.28 | 0.080 | 0.115 | 0.821 |
| Habitat | 4.29 ± 0.61 | 4.27 ± 0.64 | −0.04 | 0.485 | 4.21 ± 0.72 | 4.24 ± 0.64 | +0.07 | 0.759 | 0.466 | 0.359 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos-García, D.; de Deus Fonticoba, T.; Bartolomé, C.C.; Painceiras, M.J.F.; Castro, E.S.; Canfield, H.; Miró, C.M.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. Motor Fluctuations Development Is Associated with Non-Motor Symptoms Burden Progression in Parkinson’s Disease Patients: A 2-Year Follow-Up Study. Diagnostics 2022, 12, 1147. https://doi.org/10.3390/diagnostics12051147
Santos-García D, de Deus Fonticoba T, Bartolomé CC, Painceiras MJF, Castro ES, Canfield H, Miró CM, Jesús S, Aguilar M, Pastor P, et al. Motor Fluctuations Development Is Associated with Non-Motor Symptoms Burden Progression in Parkinson’s Disease Patients: A 2-Year Follow-Up Study. Diagnostics. 2022; 12(5):1147. https://doi.org/10.3390/diagnostics12051147
Chicago/Turabian StyleSantos-García, Diego, Teresa de Deus Fonticoba, Carlos Cores Bartolomé, Maria J. Feal Painceiras, Ester Suárez Castro, Héctor Canfield, Cristina Martínez Miró, Silvia Jesús, Miquel Aguilar, Pau Pastor, and et al. 2022. "Motor Fluctuations Development Is Associated with Non-Motor Symptoms Burden Progression in Parkinson’s Disease Patients: A 2-Year Follow-Up Study" Diagnostics 12, no. 5: 1147. https://doi.org/10.3390/diagnostics12051147
APA StyleSantos-García, D., de Deus Fonticoba, T., Bartolomé, C. C., Painceiras, M. J. F., Castro, E. S., Canfield, H., Miró, C. M., Jesús, S., Aguilar, M., Pastor, P., Planellas, L., Cosgaya, M., Caldentey, J. G., Caballol, N., Legarda, I., Hernández-Vara, J., Cabo, I., Manzanares, L. L., Aramburu, I. G., ... COPPADIS Study Group. (2022). Motor Fluctuations Development Is Associated with Non-Motor Symptoms Burden Progression in Parkinson’s Disease Patients: A 2-Year Follow-Up Study. Diagnostics, 12(5), 1147. https://doi.org/10.3390/diagnostics12051147