
End-to-End Deep Learning Approach for Perfusion Data: A Proof-of-Concept Study to Classify Core Volume in Stroke CT

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
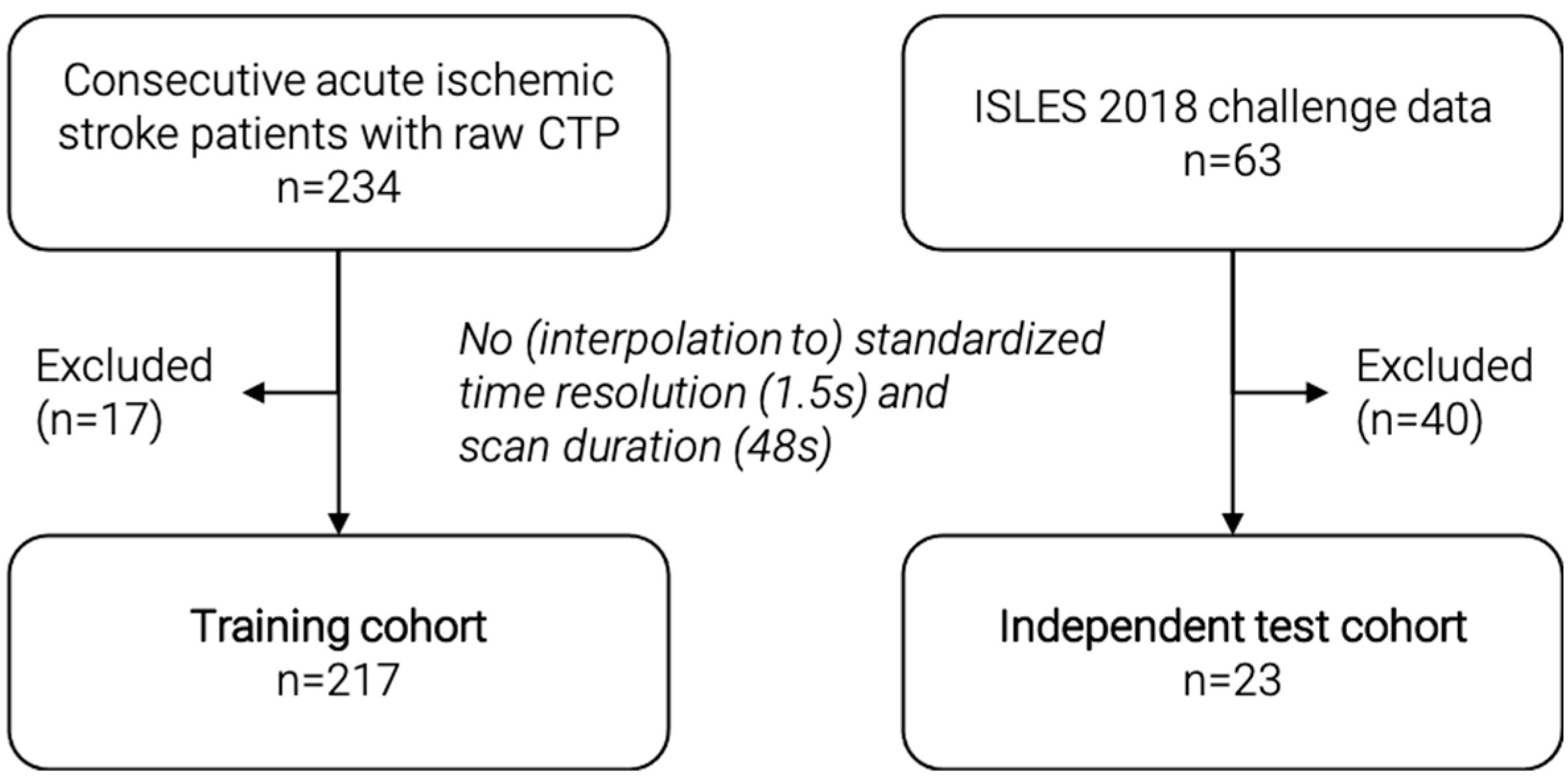
2.1. Study Population, Image Acquisition and Core Volumetry
2.2. Preprocessing, Batch Generation, and Data Augmentation
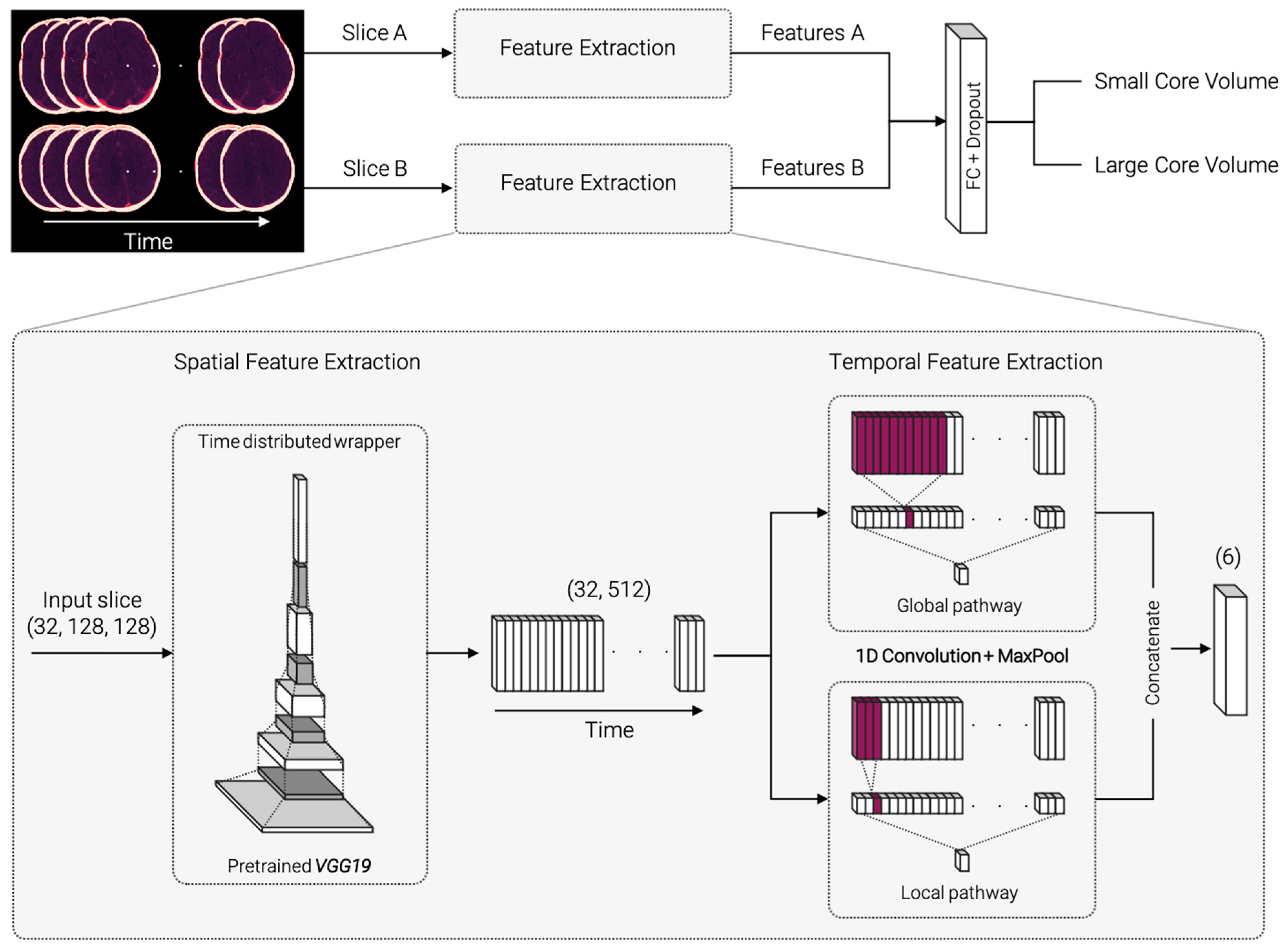
2.3. Network Architecture
2.4. Training, Validation and Testing
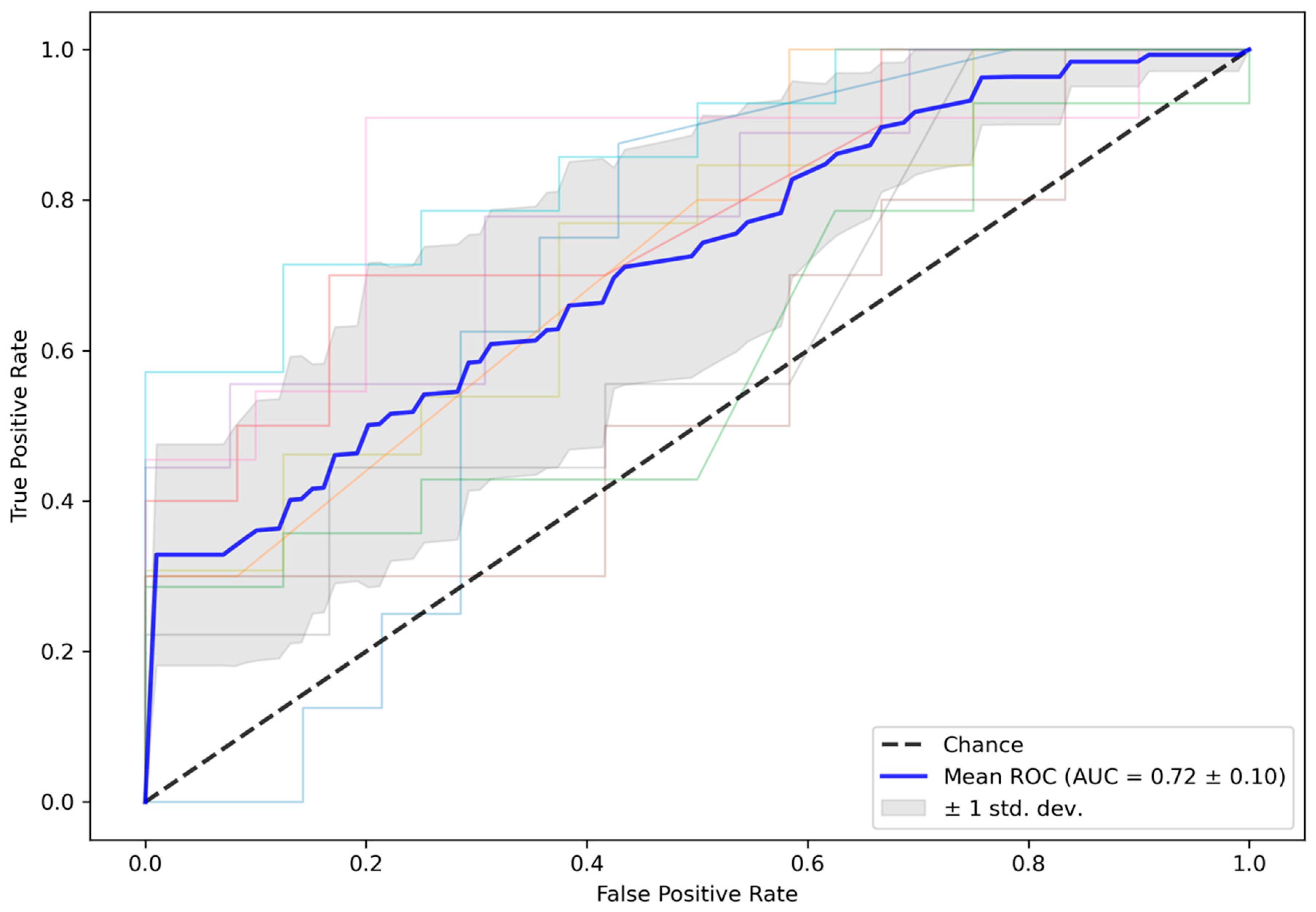
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van der Worp, H.B.; van Gijn, J. Acute Ischemic Stroke. N. Engl. J. Med. 2007, 357, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Chalet, L.; Boutelier, T.; Christen, T.; Raguenes, D.; Debatisse, J.; Eker, O.F.; Becker, G.; Nighoghossian, N.; Cho, T.-H.; Canet-Soulas, E.; et al. Clinical Imaging of the Penumbra in Ischemic Stroke: From the Concept to the Era of Mechanical Thrombectomy. Front. Cardiovasc. Med. 2022, 9, 438. [Google Scholar] [CrossRef] [PubMed]
- Allmendinger, A.M.; Tang, E.R.; Lui, Y.W.; Spektor, V. Imaging of Stroke: Part 1, Perfusion CT--Overview of Imaging Technique, Interpretation Pearls, and Common Pitfalls. AJR Am. J. Roentgenol. 2012, 198, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Merino, J.G.; Warach, S. Imaging of Acute Stroke. Nat. Rev. Neurol. 2010, 6, 560–571. [Google Scholar] [CrossRef]
- Ingrisch, M.; Sourbron, S. Tracer-Kinetic Modeling of Dynamic Contrast-Enhanced MRI and CT: A Primer. J. Pharm. Pharm. 2013, 40, 281–300. [Google Scholar] [CrossRef]
- Sourbron, S.; Dujardin, M.; Makkat, S.; Luypaert, R. Pixel-by-Pixel Deconvolution of Bolus-Tracking Data: Optimization and Implementation. Phys. Med. Biol. 2007, 52, 429–447. [Google Scholar] [CrossRef]
- Fieselmann, A.; Kowarschik, M.; Ganguly, A.; Hornegger, J.; Fahrig, R. Deconvolution-Based CT and MR Brain Perfusion Measurement: Theoretical Model Revisited and Practical Implementation Details. J. Biomed. Imaging 2011, 2011, 1–20. [Google Scholar] [CrossRef]
- Bivard, A.; Levi, C.; Spratt, N.; Parsons, M. Perfusion CT in Acute Stroke: A Comprehensive Analysis of Infarct and Penumbra. Radiology 2013, 267, 543–550. [Google Scholar] [CrossRef] [Green Version]
- Lansberg, M.G.; Christensen, S.; Kemp, S.; Mlynash, M.; Mishra, N.; Federau, C.; Tsai, J.P.; Kim, S.; Nogueria, R.G.; Jovin, T.; et al. Computed Tomographic Perfusion to Predict Response to Recanalization in Ischemic Stroke. Ann. Neurol. 2017, 81, 849–856. [Google Scholar] [CrossRef]
- Alexandre, A.M.; Pedicelli, A.; Valente, I.; Scarcia, L.; Giubbolini, F.; D’Argento, F.; Lozupone, E.; Distefano, M.; Pilato, F.; Colosimo, C. May Endovascular Thrombectomy without CT Perfusion Improve Clinical Outcome? Clin. Neurol. Neurosurg. 2020, 198, 106207. [Google Scholar] [CrossRef]
- Van Cauwenberge, M.G.A.; Dekeyzer, S.; Nikoubashman, O.; Dafotakis, M.; Wiesmann, M. Can Perfusion CT Unmask Postictal Stroke Mimics? A Case-Control Study of 133 Patients. Neurology 2018, 91, e1918–e1927. [Google Scholar] [CrossRef]
- Becks, M.J.; Manniesing, R.; Vister, J.; Pegge, S.A.H.; Steens, S.C.A.; van Dijk, E.J.; Prokop, M.; Meijer, F.J.A. Brain CT Perfusion Improves Intracranial Vessel Occlusion Detection on CT Angiography. J. Neuroradiol. 2019, 46, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Wintermark, M.; Luby, M.; Bornstein, N.M.; Demchuk, A.; Fiehler, J.; Kudo, K.; Lees, K.R.; Liebeskind, D.S.; Michel, P.; Nogueira, R.G.; et al. International Survey of Acute Stroke Imaging Used to Make Revascularization Treatment Decisions. Int. J. Stroke 2015, 10, 759–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep Learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Szegedy, C.; Toshev, A.; Erhan, D. Deep Neural Networks for Object Detection. In Proceedings of the Advances in Neural Information Processing Systems, Lake Tahoe, NV, USA, 5–10 December 2013; Burges, C.J.C., Bottou, L., Welling, M., Ghahramani, Z., Weinberger, K.Q., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2013; Volume 26. [Google Scholar]
- Yang, G.; Yu, S.; Dong, H.; Slabaugh, G.; Dragotti, P.L.; Ye, X.; Liu, F.; Arridge, S.; Keegan, J.; Guo, Y.; et al. DAGAN: Deep De-Aliasing Generative Adversarial Networks for Fast Compressed Sensing MRI Reconstruction. IEEE Trans. Med. Imaging 2018, 37, 1310–1321. [Google Scholar] [CrossRef] [Green Version]
- Shen, D.; Wu, G.; Suk, H.-I. Deep Learning in Medical Image Analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [Green Version]
- Lai, M. Deep Learning for Medical Image Segmentation. arXiv 2015, arXiv:1505.02000. [Google Scholar]
- Ho, K.C.; Scalzo, F.; Sarma, K.V.; El-Saden, S.; Arnold, C.W. A Temporal Deep Learning Approach for MR Perfusion Parameter Estimation in Stroke. In Proceedings of the 2016 23rd International Conference on Pattern Recognition (ICPR), Cancun, Mexico, 4–8 December 2016; pp. 1315–1320. [Google Scholar]
- Ulas, C.; Das, D.; Thrippleton, M.J.; Valdés Hernández, M.D.C.; Armitage, P.A.; Makin, S.D.; Wardlaw, J.M.; Menze, B.H. Convolutional Neural Networks for Direct Inference of Pharmacokinetic Parameters: Application to Stroke Dynamic Contrast-Enhanced MRI. Front. Neurol. 2019, 9, 1147. [Google Scholar] [CrossRef] [Green Version]
- Robben, D.; Boers, A.M.M.; Marquering, H.A.; Langezaal, L.L.C.M.; Roos, Y.B.W.E.M.; van Oostenbrugge, R.J.; van Zwam, W.H.; Dippel, D.W.J.; Majoie, C.B.L.M.; van der Lugt, A.; et al. Prediction of Final Infarct Volume from Native CT Perfusion and Treatment Parameters Using Deep Learning. Med. Image Anal. 2020, 59, 101589. [Google Scholar] [CrossRef]
- Chartrand, G.; Cheng, P.M.; Vorontsov, E.; Drozdzal, M.; Turcotte, S.; Pal, C.J.; Kadoury, S.; Tang, A. Deep Learning: A Primer for Radiologists. RadioGraphics 2017, 37, 2113–2131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakimelahi, R.; Yoo, A.J.; He, J.; Schwamm, L.H.; Lev, M.H.; Schaefer, P.W.; González, R.G. Rapid Identification of a Major Diffusion/Perfusion Mismatch in Distal Internal Carotid Artery or Middle Cerebral Artery Ischemic Stroke. BMC Neurol. 2012, 12, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kistler, M.; Bonaretti, S.; Pfahrer, M.; Niklaus, R.; Büchler, P. The Virtual Skeleton Database: An Open Access Repository for Biomedical Research and Collaboration. J. Med. Internet Res. 2013, 15, e2930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, O.; Menze, B.H.; von der Gablentz, J.; Häni, L.; Heinrich, M.P.; Liebrand, M.; Winzeck, S.; Basit, A.; Bentley, P.; Chen, L.; et al. ISLES 2015—A Public Evaluation Benchmark for Ischemic Stroke Lesion Segmentation from Multispectral MRI. Med. Image Anal. 2017, 35, 250–269. [Google Scholar] [CrossRef] [Green Version]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and Reliability of a Quantitative Computed Tomography Score in Predicting Outcome of Hyperacute Stroke before Thrombolytic Therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef]
- Van Rossum, G.; Drake, F.L., Jr. Python Reference Manual; Centrum voor Wiskunde en Informatica Amsterdam: Amsterdam, The Netherlands, 1995. [Google Scholar]
- Beare, R.; Lowekamp, B.; Yaniv, Z. Image Segmentation, Registration and Characterization in R with SimpleITK. J. Stat. Softw. 2018, 86, 8. [Google Scholar] [CrossRef] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Abadi, M.; Agarwal, A.; Barham, P.; Brevdo, E.; Chen, Z.; Citro, C.; Corrado, G.S.; Davis, A.; Dean, J.; Devin, M.; et al. TensorFlow: Large-Scale Machine Learning on Heterogeneous Systems. arXiv 2016, arXiv:1603.04467. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2015, arXiv:1409.1556. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Li, F.-F. Imagenet: A Large-Scale Hierarchical Image Database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Almekhlafi, M.A.; Kunz, W.G.; Menon, B.K.; McTaggart, R.A.; Jayaraman, M.V.; Baxter, B.W.; Heck, D.; Frei, D.; Derdeyn, C.P.; Takagi, T.; et al. Imaging of Patients with Suspected Large-Vessel Occlusion at Primary Stroke Centers: Available Modalities and a Suggested Approach. Am. J. Neuroradiol. 2019, 40, 396–400. [Google Scholar] [CrossRef] [Green Version]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Austein, F.; Riedel, C.; Kerby, T.; Meyne, J.; Binder, A.; Lindner, T.; Huhndorf, M.; Wodarg, F.; Jansen, O. Comparison of Perfusion CT Software to Predict the Final Infarct Volume After Thrombectomy. Stroke 2016, 47, 2311–2317. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Validation Folds | Test Folds | Independent Test Cohort |
|---|---|---|
| 0.75 (0.11) | 0.72 (0.10) | 0.61 |
| Full Model | Global Feature Extractor Alone | Local Feature Extractor Alone |
|---|---|---|
| 0.72 (0.10) | 0.63 (0.14) | 0.65 (0.13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mittermeier, A.; Reidler, P.; Fabritius, M.P.; Schachtner, B.; Wesp, P.; Ertl-Wagner, B.; Dietrich, O.; Ricke, J.; Kellert, L.; Tiedt, S.; et al. End-to-End Deep Learning Approach for Perfusion Data: A Proof-of-Concept Study to Classify Core Volume in Stroke CT. Diagnostics 2022, 12, 1142. https://doi.org/10.3390/diagnostics12051142
Mittermeier A, Reidler P, Fabritius MP, Schachtner B, Wesp P, Ertl-Wagner B, Dietrich O, Ricke J, Kellert L, Tiedt S, et al. End-to-End Deep Learning Approach for Perfusion Data: A Proof-of-Concept Study to Classify Core Volume in Stroke CT. Diagnostics. 2022; 12(5):1142. https://doi.org/10.3390/diagnostics12051142
Chicago/Turabian StyleMittermeier, Andreas, Paul Reidler, Matthias P. Fabritius, Balthasar Schachtner, Philipp Wesp, Birgit Ertl-Wagner, Olaf Dietrich, Jens Ricke, Lars Kellert, Steffen Tiedt, and et al. 2022. "End-to-End Deep Learning Approach for Perfusion Data: A Proof-of-Concept Study to Classify Core Volume in Stroke CT" Diagnostics 12, no. 5: 1142. https://doi.org/10.3390/diagnostics12051142
APA StyleMittermeier, A., Reidler, P., Fabritius, M. P., Schachtner, B., Wesp, P., Ertl-Wagner, B., Dietrich, O., Ricke, J., Kellert, L., Tiedt, S., Kunz, W. G., & Ingrisch, M. (2022). End-to-End Deep Learning Approach for Perfusion Data: A Proof-of-Concept Study to Classify Core Volume in Stroke CT. Diagnostics, 12(5), 1142. https://doi.org/10.3390/diagnostics12051142