
Clinicopathological Impact of the Spread through Air Space in Non-Small Cell Lung Cancer: A Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
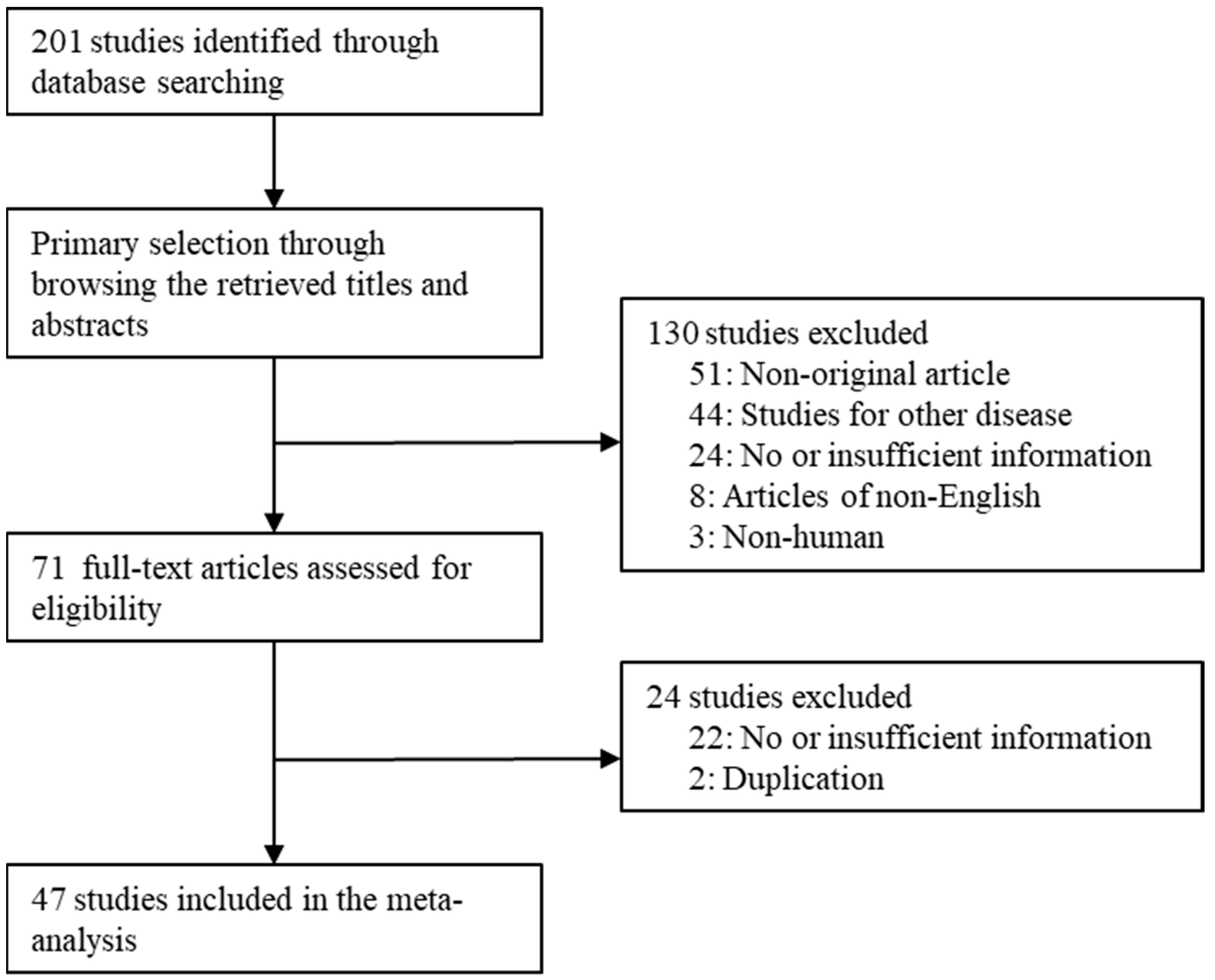
2.1. Published Studies Search and Selection Criteria
2.2. Data Extraction
2.3. Statistical Analyses
3. Results
3.1. Selection and Characteristics of the Studies
3.2. Estimated Rates of STAS in NSCLC
3.3. Correlation between STAS and Clinicopathological Characteristics in NSCLC
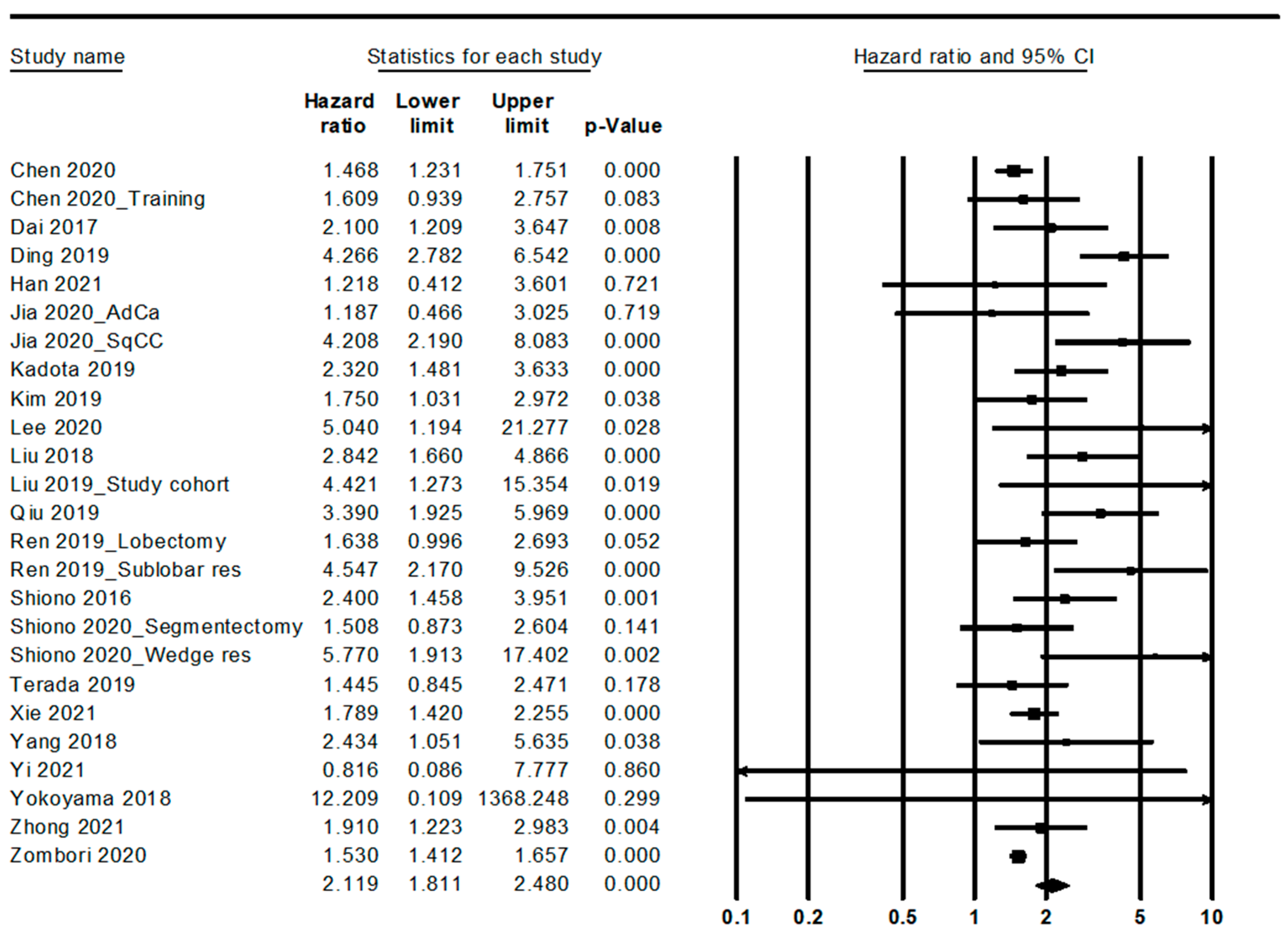
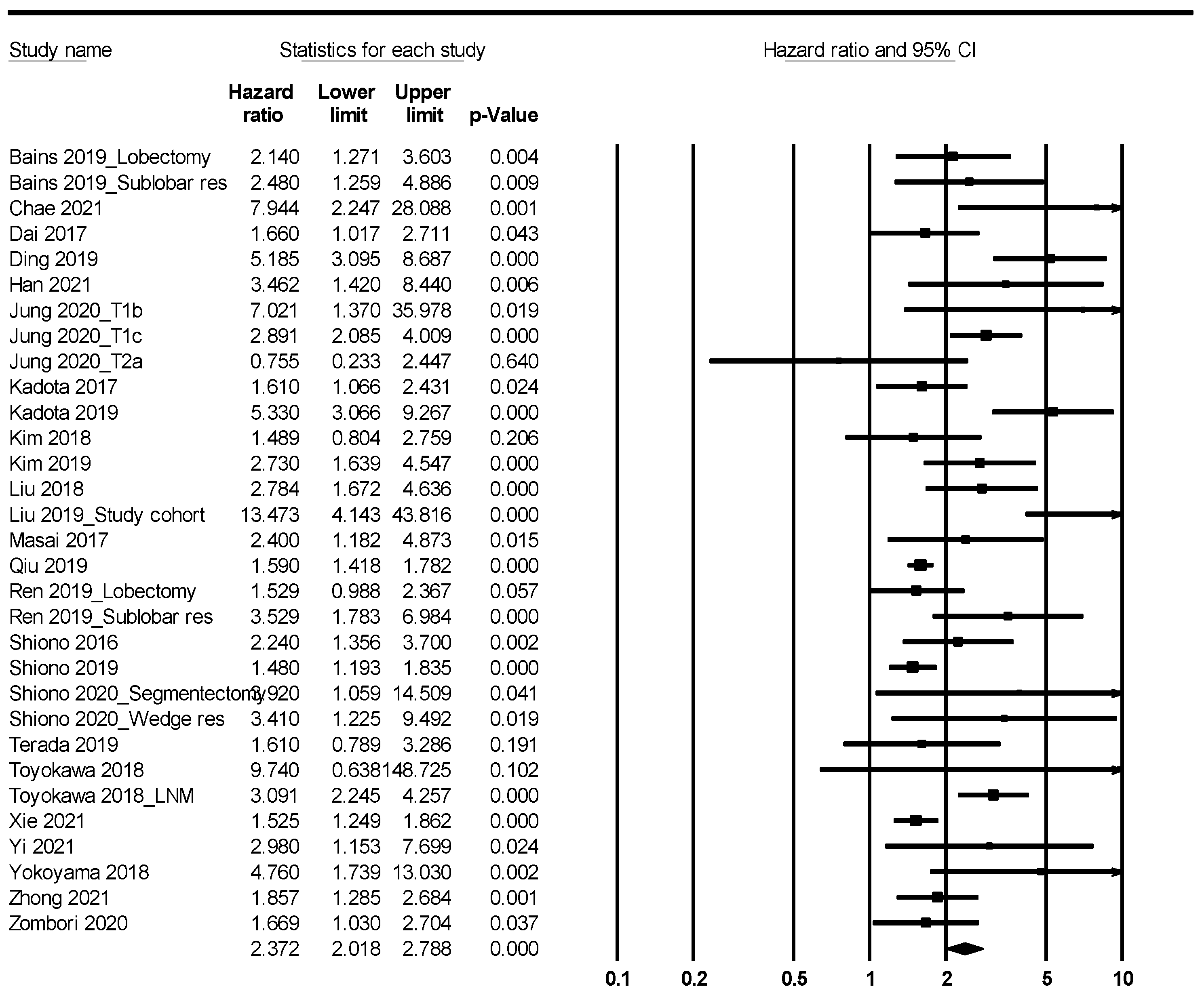
3.4. Prognosis of NSCLC with STAS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, W.A.; Ladanyi, M.; Van Schil, P.E.Y.; Scagliotti, G.V.; Bubendorf, L.; Bubendorf, L.; Kadota, K.; MacMahon, H.; Matsubara, D.; Russell, P.A.; et al. Tumours of the lung. In WHO Classification of the Lung, Pleura, Thymus and Heart. Thoracic Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021. [Google Scholar]
- Kadota, K.; Nitadori, J.I.; Sima, C.S.; Ujiie, H.; Rizk, N.P.; Jones, D.R.; Adusumilli, P.S.; Travis, W.D. Tumor spread through air spaces is an important pattern of invasion and impacts the frequency and location of recurrences after limited resection for small stage I lung adenocarcinomas. J. Thorac. Oncol. 2015, 10, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Aly, R.G.; Rekhtman, N.; Li, X.; Takahashi, Y.; Eguchi, T.; Tan, K.S.; Rudin, C.M.; Adusumilli, P.S.; Travis, W.D. Spread Through Air Spaces (STAS) Is Prognostic in Atypical Carcinoid, Large Cell Neuroendocrine Carcinoma, and Small Cell Carcinoma of the Lung. J. Thorac. Oncol. 2019, 14, 1583–1593. [Google Scholar] [CrossRef]
- Bains, S.; Eguchi, T.; Warth, A.; Yeh, Y.C.; Nitadori, J.I.; Woo, K.M.; Chou, T.Y.; Dienemann, H.; Muley, T.; Nakajima, J.; et al. Procedure-Specific Risk Prediction for Recurrence in Patients Undergoing Lobectomy or Sublobar Resection for Small (≤2 cm) Lung Adenocarcinoma: An International Cohort Analysis. J. Thorac. Oncol. 2019, 14, 72–86. [Google Scholar] [CrossRef] [Green Version]
- Onozato, M.L.; Kovach, A.E.; Yeap, B.Y.; Morales-Oyarvide, V.; Klepeis, V.E.; Tammireddy, S.; Heist, R.S.; Mark, E.J.; Dias-Santagata, D.; Iafrate, I.J.; et al. Tumor islands in resected early stage lung adenocarcinomas are associated with unique clinicopathologic and molecular characteristics and worse prognosis. Am. J. Surg. Pathol. 2013, 37, 287–294. [Google Scholar] [CrossRef] [Green Version]
- Warth, A.; Muley, T.; Kossakowski, C.A.; Goeppert, B.; Schirmacher, P.; Dienemann, H.; Weichert, W. Prognostic Impact of Intra-alveolar Tumor Spread in Pulmonary Adenocarcinoma. Am. J. Surg. Pathol. 2015, 39, 793–801. [Google Scholar] [CrossRef] [Green Version]
- Alvarez Moreno, J.C.; Aljamal, A.A.; Bahmad, B.F.; Febres-Aldana, C.A.; Rassaei, N.; Recine, M.; Poppiti, R. Correlation between spread through air spaces (STAS) and other clinicopathological parameters in lung cancer. Pathol. Res. Pract. 2021, 220, 153376. [Google Scholar] [CrossRef]
- Chae, M.; Jeon, J.H.; Chung, J.H.; Lee, S.Y.; Hwang, W.J.; Jung, W.; Hwang, Y.; Cho, S.; Kim, K.; Jheon, S. Prognostic significance of tumor spread through air spaces in patients with stage IA part-solid lung adenocarcinoma after sublobar resection. Lung Cancer 2021, 152, 21–26. [Google Scholar] [CrossRef]
- Chen, D.; Wang, X.; Zhang, F.; Han, R.; Ding, Q.; Xu, X.; Shu, J.; Ye, F.; Shi, L.; Mao, Y.; et al. Could tumor spread through air spaces benefit from adjuvant chemotherapy in stage I lung adenocarcinoma? A multi-institutional study. Ther. Adv. Med. Oncol. 2020, 12, 1758835920978147. [Google Scholar] [CrossRef]
- Chen, D.; She, Y.; Wang, T.; Xie, H.; Li, J.; Jiang, G.; Chen, Y.; Zhang, L.; Xie, D.; Chen, C. Radiomics-based prediction for tumour spread through air spaces in stage I lung adenocarcinoma using machine learning. Eur. J. Cardiothorac. Surg. 2020, 58, 51–58. [Google Scholar] [CrossRef]
- Dai, C.; Xie, H.; Su, H.; She, Y.; Zhu, E.; Fan, Z.; Zhou, F.; Ren, Y.; Xie, D.; Zheng, H.; et al. Tumor Spread through Air Spaces Affects the Recurrence and Overall Survival in Patients with Lung Adenocarcinoma >2 to 3 cm. J. Thorac. Oncol. 2017, 12, 1052–1060. [Google Scholar] [CrossRef] [Green Version]
- Ding, Q.; Chen, D.; Wang, X.; Wen, J.; Chen, C.; Zhang, Y.; Xu, Z.; Chen, Y. Characterization of lung adenocarcinoma with a cribriform component reveals its association with spread through air spaces and poor outcomes. Lung Cancer 2019, 134, 238–244. [Google Scholar] [CrossRef]
- Han, Y.B.; Kim, H.; Mino-Kenudson, M.; Cho, S.; Kwon, H.J.; Lee, K.R.; Kwon, S.; Lee, J.; Kim, K.; Jheon, S.; et al. Tumor spread through air spaces (STAS): Prognostic significance of grading in non-small cell lung cancer. Mod. Pathol. 2021, 34, 549–561. [Google Scholar] [CrossRef]
- Hara, K.; Mizuguchi, S.; Okada, S.; Izumi, N.; Tsukioka, T.; Komatsu, H.; Ohsawa, M.; Inaba, M.; Shibata, T.; Nishiyama, N. Intensity of SLX predicts distance of tumor spread through alveolar spaces in stage I lung adenocarcinoma. Thorac. Cancer 2019, 10, 832–838. [Google Scholar] [CrossRef] [Green Version]
- Hu, S.Y.; Hsieh, M.S.; Hsu, H.H.; Tsai, T.M.; Chiang, X.H.; Tsou, K.C.; Liao, H.C.; Lin, M.W.; Chen, J.S. Correlation of tumor spread through air spaces and clinicopathological characteristics in surgically resected lung adenocarcinomas. Lung Cancer 2018, 126, 189–193. [Google Scholar] [CrossRef]
- Ikeda, T.; Kadota, K.; Yoshida, C.; Ishikawa, R.; Go, T.; Haba, R.; Yokomise, H. The epithelial-mesenchymal transition phenotype is associated with the frequency of tumor spread through air spaces (STAS) and a High risk of recurrence after resection of lung carcinoma. Lung Cancer 2021, 153, 49–55. [Google Scholar] [CrossRef]
- Jia, M.; Yu, S.; Yu, J.; Li, Y.; Gao, H.; Sun, P.L. Comprehensive analysis of spread through air spaces in lung adenocarcinoma and squamous cell carcinoma using the 8th edition AJCC/UICC staging system. BMC Cancer 2020, 20, 705. [Google Scholar] [CrossRef]
- Jung, W.; Chung, J.H.; Yum, S.; Kim, K.; Lee, C.T.; Jheon, S.; Cho, S. The differential prognostic impact of spread through air spaces in early-stage lung adenocarcinoma after lobectomy according to the pT descriptor. J. Thorac. Cardiovasc. Surg. 2022, 163, 277–284.e1. [Google Scholar] [CrossRef]
- Kadota, K.; Kushida, Y.; Katsuki, N.; Ishikawa, R.; Ibuki, E.; Motoyama, M.; Nii, K.; Yokomise, H.; Bandoh, S.; Haba, R. Tumor Spread Through Air Spaces Is an Independent Predictor of Recurrence-free Survival in Patients With Resected Lung Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2017, 41, 1077–1086. [Google Scholar] [CrossRef]
- Kadota, K.; Kushida, Y.; Kagawa, S.; Ishikawa, R.; Ibuki, E.; Inoue, K.; Go, T.; Yokomise, H.; Ishii, T.; Kadowaki, N.; et al. Limited Resection Is Associated With a Higher Risk of Locoregional Recurrence than Lobectomy in Stage I Lung Adenocarcinoma With Tumor Spread Through Air Spaces. Am. J. Surg. Pathol. 2019, 43, 1033–1041. [Google Scholar] [CrossRef]
- Kim, S.K.; Kim, T.J.; Chung, M.J.; Kim, T.S.; Lee, K.S.; Zo, J.I.; Shim, Y.M. Lung Adenocarcinoma: CT Features Associated with Spread through Air Spaces. Radiology 2018, 289, 831–840. [Google Scholar] [CrossRef]
- Kim, M.; Chung, Y.S.; Kim, K.A.; Shim, H.S. Prognostic factors of acinar- or papillary-predominant adenocarcinoma of the lung. Lung Cancer 2019, 137, 129–135. [Google Scholar] [CrossRef]
- Kimura, T.; Nakamura, H.; Omura, A.; Ike, A.; Hiroshima, T.; Maniwa, T.; Honma, K.; Higashiyama, M.; Okami, J. Novel imprint cytological classification is correlated with tumor spread through air spaces in lung adenocarcinoma. Lung Cancer 2020, 148, 62–68. [Google Scholar] [CrossRef]
- Koezuka, S.; Mikami, T.; Tochigi, N.; Sano, A.; Azuma, Y.; Makino, T.; Otsuka, H.; Matsumoto, K.; Shiraga, N.; Iyoda, A. Toward improving prognosis prediction in patients undergoing small lung adenocarcinoma resection: Radiological and pathological assessment of diversity and intratumor heterogeneity. Lung Cancer 2019, 135, 40–46. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, E.K.; Kim, M.; Shim, H.S. Genetic and clinicopathologic characteristics of lung adenocarcinoma with tumor spread through air spaces. Lung Cancer 2018, 123, 121–126. [Google Scholar] [CrossRef]
- Lee, M.A.; Kang, J.; Lee, H.Y.; Kim, W.; Shon, I.; Hwang, N.Y.; Kim, H.K.; Choi, Y.S.; Kim, J.; Zo, J.I.; et al. Spread through air spaces (STAS) in invasive mucinous adenocarcinoma of the lung: Incidence, prognostic impact, and prediction based on clinicoradiologic factors. Thorac. Cancer 2020, 11, 3145–3154. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, D.; Qiu, X.; Duan, S.; Zhang, Y.; Li, F.; Chen, C.; Zhou, Y.; Chen, Y. Relationship between MTA1 and spread through air space and their joint influence on prognosis of patients with stage I-III lung adenocarcinoma. Lung Cancer 2018, 124, 211–218. [Google Scholar] [CrossRef]
- Liu, A.; Hou, F.; Qin, Y.; Song, G.; Xie, B.; Xu, J.; Jiao, W. Predictive value of a prognostic model based on pathologic features in lung invasive adenocarcinoma. Lung Cancer 2019, 131, 14–22. [Google Scholar] [CrossRef]
- Lu, S.; Tan, K.S.; Kadota, K.; Eguchi, T.; Bains, S.; Rekhtman, N.; Adusumilli, P.S.; Travis, W.D. Spread through Air Spaces (STAS) Is an Independent Predictor of Recurrence and Lung Cancer-Specific Death in Squamous Cell Carcinoma. J. Thorac. Oncol. 2017, 12, 223–234. [Google Scholar] [CrossRef] [Green Version]
- Masai, K.; Sakurai, H.; Sukeda, A.; Suzuki, S.; Asakura, K.; Nakagawa, K.; Asamura, H.; Watanabe, S.I.; Motoi, N.; Hiraoka, N. Prognostic Impact of Margin Distance and Tumor Spread Through Air Spaces in Limited Resection for Primary Lung Cancer. J. Thorac. Oncol. 2017, 12, 1788–1797. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, N.; Yoshizawa, A.; Rokutan-Kurata, M.; Noguchi, M.; Teramoto, Y.; Sumiyoshi, S.; Kondo, K.; Sonobe, M.; Hamaji, M.; Menju, T.; et al. Prognostic significance of cribriform adenocarcinoma of the lung: Validation analysis of 1,057 Japanese patients with resected lung adenocarcinoma and a review of the literature. Transl. Lung Cancer Res. 2021, 10, 117–127. [Google Scholar] [CrossRef]
- Qi, L.; Xue, K.; Cai, Y.; Lu, J.; Li, X.; Li, M. Predictors of CT Morphologic Features to Identify Spread Through Air Spaces Preoperatively in Small-Sized Lung Adenocarcinoma. Front. Oncol. 2021, 10, 548430. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Chen, D.; Liu, Y.; Duan, S.; Zhang, F.; Zhang, Y.; Li, F.; Chen, C.; Chen, Y. Relationship between stromal cells and tumor spread through air spaces in lung adenocarcinoma. Thorac. Cancer 2019, 10, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Xie, H.; Dai, C.; She, Y.; Su, H.; Xie, D.; Zheng, H.; Zhang, L.; Jiang, G.; Wu, C.; et al. Prognostic Impact of Tumor Spread Through Air Spaces in Sublobar Resection for 1A Lung Adenocarcinoma Patients. Ann. Surg. Oncol. 2019, 26, 1901–1908. [Google Scholar] [CrossRef]
- Shiono, S.; Yanagawa, N. Spread through air spaces is a predictive factor of recurrence and a prognostic factor in stage I lung adenocarcinoma. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 567–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiono, S.; Endo, M.; Suzuki, K.; Hayasaka, K.; Yanagawa, N. Spread through air spaces in lung cancer patients is a risk factor for pulmonary metastasis after surgery. J. Thorac. Dis. 2019, 11, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Shiono, S.; Endo, M.; Suzuki, K.; Yanagawa, N. Spread through air spaces affects survival and recurrence of patients with clinical stage IA non-small cell lung cancer after wedge resection. J. Thorac. Dis. 2020, 12, 2247–2260. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Jiang, L.; Zhuo, Z.; Luo, J.; Alai, G.; Shen, X.; Lin, Y. Impacts of thoracoscopic surgery and high grade histologic subtypes on spread through air spaces in small stage I lung adenocarcinomas. J. Cancer Res. Clin. Oncol. 2019, 145, 2375–2382. [Google Scholar] [CrossRef]
- Terada, Y.; Takahashi, T.; Morita, S.; Kashiwabara, K.; Nagayama, K.; Nitadori, J.I.; Anraku, M.; Sato, M.; Shinozaki-Ushiku, A.; Nakajima, J. Spread through air spaces is an independent predictor of recurrence in stage III (N2) lung adenocarcinoma. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 442–448. [Google Scholar] [CrossRef]
- Toyokawa, G.; Yamada, Y.; Tagawa, T.; Oda, Y. Significance of spread through air spaces in early-stage lung adenocarcinomas undergoing limited resection. Thorac. Cancer 2018, 9, 1255–1261. [Google Scholar] [CrossRef]
- Toyokawa, G.; Yamada, Y.; Tagawa, T.; Kinoshita, F.; Kozuma, Y.; Matsubara, T.; Haratake, N.; Takamori, S.; Akamine, T.; Hirai, F.; et al. Significance of Spread Through Air Spaces in Resected Lung Adenocarcinomas With Lymph Node Metastasis. Clin. Lung Cancer 2018, 19, 395–400.e1. [Google Scholar] [CrossRef]
- Vaghjiani, R.G.; Takahashi, Y.; Eguchi, T.; Lu, S.; Kameda, K.; Tano, Z.; Dozier, J.; Tan, K.S.; Jones, D.R.; Travis, W.D.; et al. Tumor Spread Through Air Spaces Is a Predictor of Occult Lymph Node Metastasis in Clinical Stage IA Lung Adenocarcinoma. J. Thorac. Oncol. 2020, 15, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Villalba, J.A.; Shih, A.R.; Sayo, T.M.S.; Kunitoki, K.; Hung, Y.P.; Ly, A.; Kem, M.; Hariri, L.P.; Muniappan, A.; Gaissert, H.A.; et al. Accuracy and Reproducibility of Intraoperative Assessment on Tumor Spread Through Air Spaces in Stage 1 Lung Adenocarcinomas. J. Thorac. Oncol. 2021, 16, 619–629. [Google Scholar] [CrossRef]
- Xie, H.; Su, H.; Zhu, E.; Gu, C.; Zhao, S.; She, Y.; Ren, Y.; Xie, D.; Zheng, H.; Wu, C.; et al. Morphological Subtypes of Tumor Spread Through Air Spaces in Non-Small Cell Lung Cancer: Prognostic Heterogeneity and Its Underlying Mechanism. Front. Oncol. 2021, 11, 608353. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Yang, Y.; Ma, P.; Zheng, B.; Liu, W.; Zhang, Z.; Ding, N.; Liu, L.; Mao, Y.; Lv, N. Spread through air spaces predicts a worse survival in patients with stage I adenocarcinomas >2 cm after radical lobectomy. J. Thorac. Dis. 2018, 10, 5308–5317. [Google Scholar] [CrossRef] [PubMed]
- Yi, E.; Lee, J.H.; Jung, Y.; Chung, J.H.; Lee, Y.; Lee, S. Clinical implication of tumour spread through air spaces in pathological stage I lung adenocarcinoma treated with lobectomy. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, S.; Murakami, T.; Tao, H.; Onoda, H.; Hara, A.; Miyazaki, R.; Furukawa, M.; Hayashi, M.; Inokawa, H.; Okabe, K.; et al. Tumor Spread Through Air Spaces Identifies a Distinct Subgroup With Poor Prognosis in Surgically Resected Lung Pleomorphic Carcinoma. Chest 2018, 154, 838–847. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, Z.; Feng, H.; Xiao, F.; Shao, W.; Liang, C.; Sun, H.; Gu, X.; Liu, D. Predictive value of radiological features on spread through air space in stage cIA lung adenocarcinoma. J. Thorac. Dis. 2020, 12, 6494–6504. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Xu, Y.; Deng, J.; Wang, T.; Sun, X.; Chen, D.; Wu, C.; Hou, L.; Xie, H.; She, Y.; et al. Prognostic impact of tumour spread through air space in radiological subsolid and pure solid lung adenocarcinoma. Eur. J. Cardiothorac. Surg. 2021, 59, 624–632. [Google Scholar] [CrossRef]
- Zhuo, Y.; Feng, M.; Yang, S.; Zhou, L.; Ge, D.; Lu, S.; Liu, L.; Shan, F.; Zhang, Z. Radiomics nomograms of tumors and peritumoral regions for the preoperative prediction of spread through air spaces in lung adenocarcinoma. Transl. Oncol. 2020, 13, 100820. [Google Scholar] [CrossRef]
- Zombori, T.; Sejben, A.; Tiszlavicz, L.; Cserni, G.; Pálföldi, R.; Csada, E.; Furák, J. Architectural Grade Combined With Spread Through Air Spaces (STAS) Predicts Recurrence and is Suitable for Stratifying Patients Who Might Be Eligible for Lung Sparing Surgery for Stage I Adenocarcinomas. Pathol. Oncol. Res. 2020, 26, 2451–2458. [Google Scholar] [CrossRef]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Yusuf, S.; Peto, R.; Lewis, J.; Collins, R.; Sleight, P. Beta blockade during and after myocardial infarction: An overview of the randomized trials. Prog. Cardiovasc. Dis. 1985, 27, 335–371. [Google Scholar] [CrossRef]
- Shih, A.R.; Mino-Kenudson, M. Updates on spread through air spaces (STAS) in lung cancer. Histopathology 2020, 77, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Thunnissen, E.; Blaauwgeers, H.; de Cuba, E.; Yick, C.Y.; Flieder, D.B. Ex Vivo Artifacts and Histopathologic Pitfalls in the Lung. Arch. Pathol. Lab. Med. 2016, 140, 212–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, Q.; Wang, H.; Cui, H.; Wang, W.; Yang, G.; Qie, P.; Xun, X.; Han, S.; Liu, H. Meta-analysis of association between CT-based features and tumor spread through air spaces in lung adenocarcinoma. J. Cardiothorac. Surg. 2020, 15, 243. [Google Scholar] [CrossRef]
- Kameda, K.; Eguchi, T.; Lu, S.; Qu, Y.; Tan, K.S.; Kadota, K.; Adusumilli, P.S.; Travis, W.D. Implications of the Eighth Edition of the TNM Proposal: Invasive Versus Total Tumor Size for the T Descriptor in Pathologic Stage I-IIA Lung Adenocarcinoma. J. Thorac. Oncol. 2018, 13, 1919–1929. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Hao, J.; Qian, C.; Wang, H. Tumor Spread Through Air Spaces Is a Survival Predictor in Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2019, 20, e584–e591. [Google Scholar] [CrossRef]
- Liu, H.; Yin, Q.; Yang, G.; Qje, P. Prognostic Impact of Tumor Spread Through Air Spaces in Non-small Cell Lung Cancers: A Meta-Analysis Including 3564 Patients. Pathol. Oncol. Res. 2019, 25, 1303–1310. [Google Scholar] [CrossRef]
- Chen, D.; Mao, Y.; Wen, J.; She, Y.; Zhu, E.; Zhu, F.; Zhang, Y.; Fan, M.; Chen, C.; Chen, Y. Tumor Spread Through Air Spaces in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2019, 108, 945–954. [Google Scholar] [CrossRef]
- Sun, Y.; Yu, X.; Shi, X.; Hong, W.; Zhao, J.; Shi, L. Correlation of survival and EGFR mutation with predominant histologic subtype according to the new lung adenocarcinoma classification in stage IB patients. World J. Surg. Oncol. 2014, 12, 148. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.R.; Dong, Y.J.; Wu, H.B.; Liu, Z.C.; Zhou, L.J.; Su, D.; Chen, X.J.; Zhang, L.; Zhao, Y.L. Micropapillary: A component more likely to harbour heterogeneous EGFR mutations in lung adenocarcinomas. Sci. Rep. 2016, 6, 23755. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Author, Year | Location | Subtype | TNM Stage | Subgroup | No of Patients | STAS | |
|---|---|---|---|---|---|---|---|
| Present | Absent | ||||||
| Alvarez Moreno 2021 [7] | USA | NSCLC | I-III | 240 | 67 | 173 | |
| Bains 2019 [4] | USA | ADC | I | Lobectomy | 557 | 191 | 366 |
| ADC | I | Sublobar resection | 352 | 126 | 226 | ||
| Chae 2021 [8] | Korea | ADC | I | 115 | 20 | 95 | |
| Chen 2020 [9] | China | ADC | I | 3346 | 1082 | 2264 | |
| Chen 2020 [10] | China | ADC | I | Training cohort | 233 | 69 | 164 |
| ADC | I | Validation cohort | 112 | 50 | 62 | ||
| Dai 2017 [11] | China | NSCLC | I | 383 | 116 | 267 | |
| Ding 2019 [12] | China | ADC | I-III | 208 | 107 | 101 | |
| Han 2021 [13] | Korea | NSCLC | I-IV | NSCLC | 1869 | 765 | 1104 |
| ADC | I-IV | ADC | 1544 | 684 | 860 | ||
| Hara 2019 [14] | Japan | ADC | I | 108 | 32 | 76 | |
| Hu 2018 [15] | Taiwan | ADC | I-III | 500 | 134 | 366 | |
| Ikeda 2021 [16] | Japan | NSCLC | I-III | 636 | 282 | 354 | |
| Jia 2020 [17] | China | ADC | I-IV | ADC | 303 | 183 | 120 |
| SCC | I-IV | SCC | 121 | 39 | 82 | ||
| Jung 2020 [18] | Korea | ADC | I | 506 | 204 | 302 | |
| Kadota 2015 [2] | Japan | ADC | I | 411 | 155 | 256 | |
| Kadota 2017 [19] | Japan | SCC | I-IV | 216 | 87 | 129 | |
| Kadota 2019 [20] | Japan | ADC | I-IV | 735 | 247 | 488 | |
| Kim 2018 [21] | Korea | ADC | I-III | 276 | 92 | 184 | |
| Kim 2019 [22] | Korea | ADC | I-III | 301 | 154 | 147 | |
| Kimura 2020 [23] | Japan | ADC | ND | 164 | 29 | 135 | |
| Koezuka 2019 [24] | Japan | ADC | I-III | 64 | 18 | 46 | |
| Lee 2018 [25] | Korea | ADC | I-III | 316 | 160 | 156 | |
| Lee 2020 [26] | Korea | ADC | I-III | 119 | 86 | 33 | |
| Liu 2018 [27] | China | ADC | I-III | 208 | 107 | 101 | |
| Liu 2019 [28] | China | ADC | I-III | Study cohort | 289 | 143 | 146 |
| I-III | Validation cohort | 91 | 50 | 41 | |||
| Lu 2017 [29] | USA | SCC | I-III | 445 | 132 | 313 | |
| Masai 2017 [30] | Japan | NSCLC | ND | 508 | 76 | 432 | |
| Nakajima 2021 [31] | Japan | ADC | I-III | 1057 | 384 | 673 | |
| Qi 2021 [32] | China | ADC | ND | 190 | 47 | 143 | |
| Qiu 2019 [33] | China | ADC | I-III | 192 | 107 | 85 | |
| Ren 2019 [34] | China | ADC | I | Lobectomy | 634 | 182 | 452 |
| I | Sublobar resection | 118 | 43 | 75 | |||
| Shiono 2016 [35] | Japan | ADC | I | 318 | 47 | 271 | |
| Shiono 2019 [36] | Japan | NSCLC | I | 848 | 139 | 709 | |
| Shiono 2020 [37] | Japan | ADC | I | 217 | 34 | 183 | |
| Song 2019 [38] | China | ADC | I | 277 | 86 | 191 | |
| Terada 2019 [39] | Japan | ADC | III | 76 | 46 | 30 | |
| Toyokawa 2018 [40] | Japan | ADC | I | 82 | 31 | 51 | |
| Toyokawa 2018 [41] | Japan | ADC | II-III | Lymph node metastasis | 63 | 46 | 17 |
| Vaghjiani 2020 [42] | USA | ADC | I-III | 809 | 350 | 459 | |
| Villalba 2021 [43] | USA | ADC | I | 100 | 43 | 57 | |
| Xie 2021 [44] | China | NSCLC | I-IV | 803 | 433 | 370 | |
| Yang 2018 [45] | China | ADC | I | 242 | 81 | 161 | |
| Yi 2021 [46] | Korea | ADC | I-II | 109 | 41 | 68 | |
| Yokoyama 2018 [47] | Japan | NSCLC | I-III | 35 | 21 | 14 | |
| Zhang 2020 [48] | China | ADC | I-III | 762 | 83 | 679 | |
| Zhong 2021 [49] | China | ADC | I | 620 | 167 | 453 | |
| Zhuo 2020 [50] | China | ADC | ND | 212 | 107 | 105 | |
| Zombori 2020 [51] | Hungary | ADC | I | 292 | 123 | 169 | |
| Number of Subset | Fixed Effect [95% CI] | Heterogeneity Test [p-Value] | Random Effect [95% CI] | Egger’s Test | |
|---|---|---|---|---|---|
| Overall | 53 | 0.367 [0.361, 0.374] | <0.001 | 0.368 [0.336, 0.401] | 0.905 |
| Squamous cell carcinoma | 3 | 0.331 [0.299, 0.365] | 0.025 | 0.338 [0.273, 0.411] | 0.735 |
| Adenocarcinoma | 43 | 0.366 [0.358, 0.373] | <0.001 | 0.374 [0.340, 0.409] | 0.599 |
| Lepidic predominant | 28 | 0.167 [0.151, 0.183] | <0.001 | 0.128 [0.092, 0.175] | 0.126 |
| Acinar predominant | 28 | 0.361 [0.347, 0.374] | <0.001 | 0.352 [0.312, 0.394] | 0.699 |
| Papillary predominant | 28 | 0.434 [0.414, 0.454] | <0.001 | 0.446 [0.392, 0.501] | 0.559 |
| Micropapillary predominant | 25 | 0.647 [0.614, 0.679] | <0.001 | 0.719 [0.652, 0.778] | 0.004 |
| Solid predominant | 28 | 0.465 [0.440, 0.491] | <0.001 | 0.567 [0.478, 0.652] | 0.073 |
| Mucinous predominant | 7 | 0.282 [0.190, 0.397] | 0.222 | 0.278 [0.169, 0.421] | 0.654 |
| Cribriform predominant | 3 | 0.365 [0.337, 0.394] | 0.605 | 0.365 [0.337, 0.394] | 0.642 |
| Colloid predominant | 1 | 0.167 [0.010, 0.806] | 1.000 | 0.167 [0.010, 0.806] | - |
| Number of Subset | Fixed Effect [95% CI] | Heterogeneity Test [p-Value] | Random Effect [95% CI] | Egger’s Test [p-Value] | Meta-Regression Test [p-Value] | |
|---|---|---|---|---|---|---|
| Age (mean) | ||||||
| STAS | 25 | 66.2 [66.0, 66.4] | <0.001 | 63.8 [61.6, 65.9] | 0.088 | 0.653 |
| Non-STAS | 25 | 68.1 [68.0, 68.2] | <0.001 | 63.0 [60.4, 65.4] | 0.032 | |
| Gender (Male) | ||||||
| STAS | 44 | 0.533 [0.521, 0.545] | <0.001 | 0.546 [0.514, 0.578] | 0.298 | 0.008 |
| Non-STAS | 44 | 0.489 [0.480, 0.497] | <0.001 | 0.484 [0.451, 0.516] | 0.748 | |
| Current/ex-Smoking | ||||||
| STAS | 39 | 0.465 [0.452, 0.478] | <0.001 | 0.475 [0.418, 0.532] | 0.951 | 0.236 |
| Non-STAS | 39 | 0.422 [0.412, 0.431] | <0.001 | 0.426 [0.369, 0.486] | 0.862 | |
| Tumor size (cm) | ||||||
| STAS | 20 | 1.91 [1.90, 1.92] | <0.001 | 2.45 [2.21, 2.69] | 0.175 | 0.092 |
| Non-STAS | 20 | 1.65 [1.64, 1.65] | <0.001 | 2.99 [2.52, 3.46] | 0.112 | |
| Location (upper/middle lobe) | ||||||
| STAS | 11 | 0.646 [0.621, 0.671] | 0.079 | 0.648 [0.612, 0.682] | 0.722 | 0.078 |
| Non-STAS | 11 | 0.702 [0.684, 0.719] | 0.003 | 0.691 [0.658, 0.721] | 0.021 | |
| Visceral pleural invasion | ||||||
| STAS | 30 | 0.355 [0.341, 0.370] | <0.001 | 0.322 [0.275, 0.373] | 0.187 | <0.001 |
| Non-STAS | 30 | 0.202 [0.193, 0.212] | <0.001 | 0.177 [0.128, 0.239] | 0.478 | |
| Venous invasion | ||||||
| STAS | 23 | 0.352 [0.335, 0.370] | <0.001 | 0.301 [0.251, 0.356] | 0.093 | <0.001 |
| Non-STAS | 23 | 0.151 [0.140, 0.163] | <0.001 | 0.120 [0.080, 0.175] | 0.319 | |
| Lymphatic invasion | ||||||
| STAS | 20 | 0.495 [0.476, 0.514] | <0.001 | 0.391 [0.325, 0.461] | 0.005 | <0.001 |
| Non-STAS | 20 | 0.192 [0.180, 0.205] | <0.001 | 0.130 [0.092, 0.181] | 0.103 |
| Number of Subset | Fixed Effect [95% CI] | Heterogeneity Test [p-Value] | Random Effect [95% CI] | Egger’s Test [p-Value] | Meta-Regression Test [p-Value] | |
|---|---|---|---|---|---|---|
| ALK mutation | ||||||
| STAS | 7 | 0.125 [0.102, 0.152] | 0.504 | 0.125 [0.102, 0.152] | 0.894 | <0.001 |
| Non-STAS | 7 | 0.042 [0.030, 0.059] | <0.001 | 0.027 [0.011, 0.067] | 0.120 | |
| EGFR mutation | ||||||
| STAS | 13 | 0.464 [0.439, 0.489] | <0.001 | 0.438 [0.373, 0.506] | 0.421 | 0.058 |
| Non-STAS | 13 | 0.519 [0.500, 0.538] | <0.001 | 0.523 [0.473, 0.573] | 0.864 | |
| ROS1 rearrangement | ||||||
| STAS | 3 | 0.040 [0.023, 0.067] | 0.359 | 0.040 [0.023, 0.068] | 0.050 | 0.003 |
| Non-STAS | 3 | 0.008 [0.004, 0.018] | 0.315 | 0.009 [0.004, 0.020] | 0.966 | |
| KRAS mutation | ||||||
| STAS | 3 | 0.059 [0.039, 0.089] | 0.168 | 0.053 [0.029, 0.096] | 0.161 | 0.284 |
| Non-STAS | 3 | 0.033 [0.020, 0.053] | 0.301 | 0.033 [0.019, 0.056] | 0.375 |
| Number of Subset | Fixed Effect [95% CI] | Heterogeneity Test [p-Value] | Random Effect [95% CI] | Egger’s Test [p-Value] | |
|---|---|---|---|---|---|
| Overall survival | 25 | 1.684 [1.584, 1.791] | <0.001 | 2.119 [1.811, 2.480] | 0.001 |
| Adenocarcinoma | 21 | 1.656 [1.552, 1.766] | <0.001 | 2.093 [1.756, 2.496] | 0.005 |
| Squamous cell carcinoma | 1 | 4.208 [2.190, 8.083] | 1.000 | 4.208 [2.190, 8.083] | - |
| Recurrence-free survival | 31 | 1.888 [1.763, 2.023] | <0.001 | 2.372 [2.018, 2.788] | <0.001 |
| Adenocarcinoma | 25 | 2.028 [1.869, 2.200] | <0.001 | 2.633 [2.145, 3.232] | <0.001 |
| Squamous cell carcinoma | 1 | 1.610 [1.066, 2.431] | 1.000 | 1.610 [1.066, 2.431] | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyo, J.-S.; Kim, N.Y. Clinicopathological Impact of the Spread through Air Space in Non-Small Cell Lung Cancer: A Meta-Analysis. Diagnostics 2022, 12, 1112. https://doi.org/10.3390/diagnostics12051112
Pyo J-S, Kim NY. Clinicopathological Impact of the Spread through Air Space in Non-Small Cell Lung Cancer: A Meta-Analysis. Diagnostics. 2022; 12(5):1112. https://doi.org/10.3390/diagnostics12051112
Chicago/Turabian StylePyo, Jung-Soo, and Nae Yu Kim. 2022. "Clinicopathological Impact of the Spread through Air Space in Non-Small Cell Lung Cancer: A Meta-Analysis" Diagnostics 12, no. 5: 1112. https://doi.org/10.3390/diagnostics12051112
APA StylePyo, J.-S., & Kim, N. Y. (2022). Clinicopathological Impact of the Spread through Air Space in Non-Small Cell Lung Cancer: A Meta-Analysis. Diagnostics, 12(5), 1112. https://doi.org/10.3390/diagnostics12051112