
Comparison of Two Kinds of Two-Dimensional Shear Wave Elastography Techniques in the Evaluation of Jaundiced Infants Suspected of Biliary Atresia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrollment
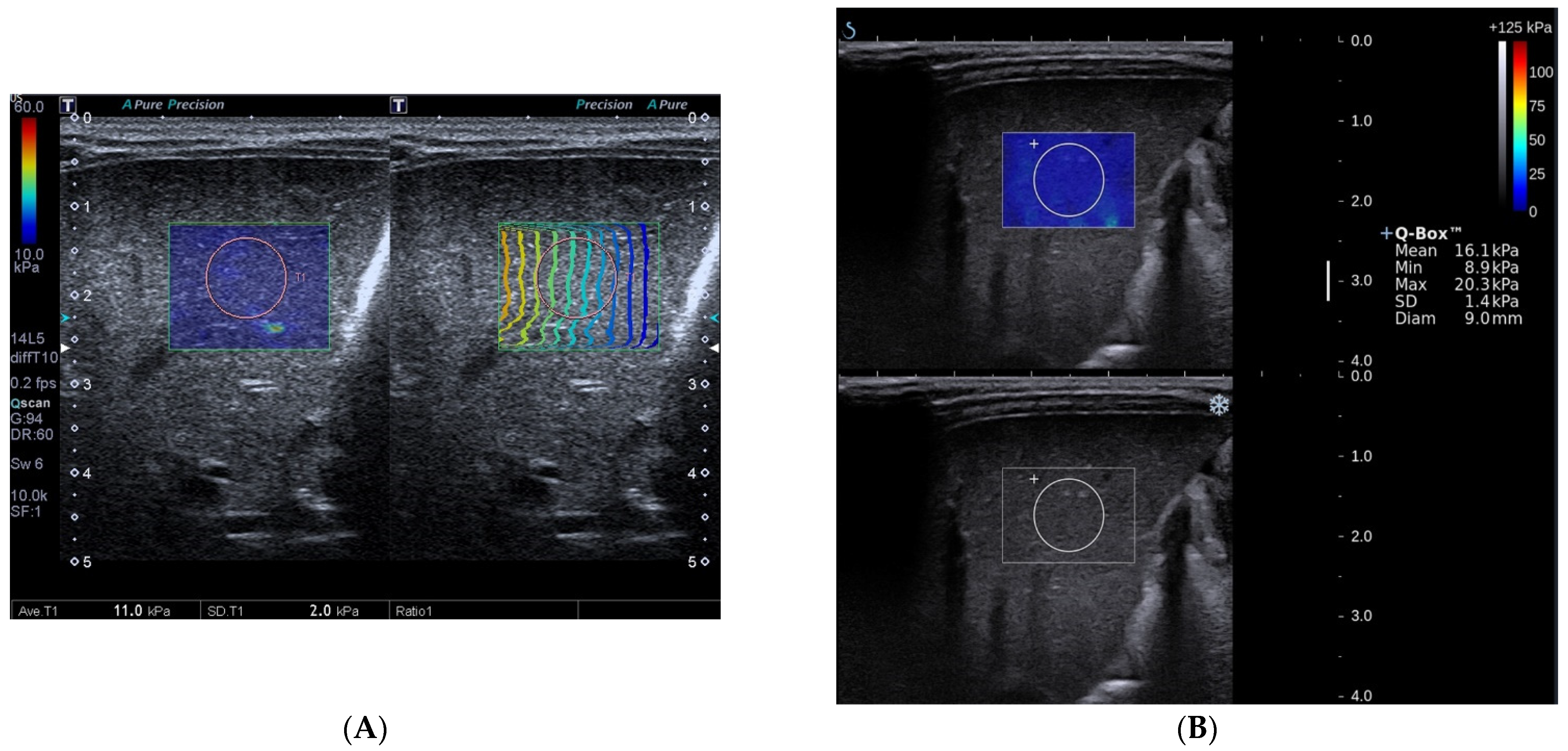
2.2. The Measurement of S-SWE
2.3. The Measurement of T-SWE
2.4. Liver Histopathology
2.5. Inter-Operator and Intra-Operator Error of T-SWE and S-SWE
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
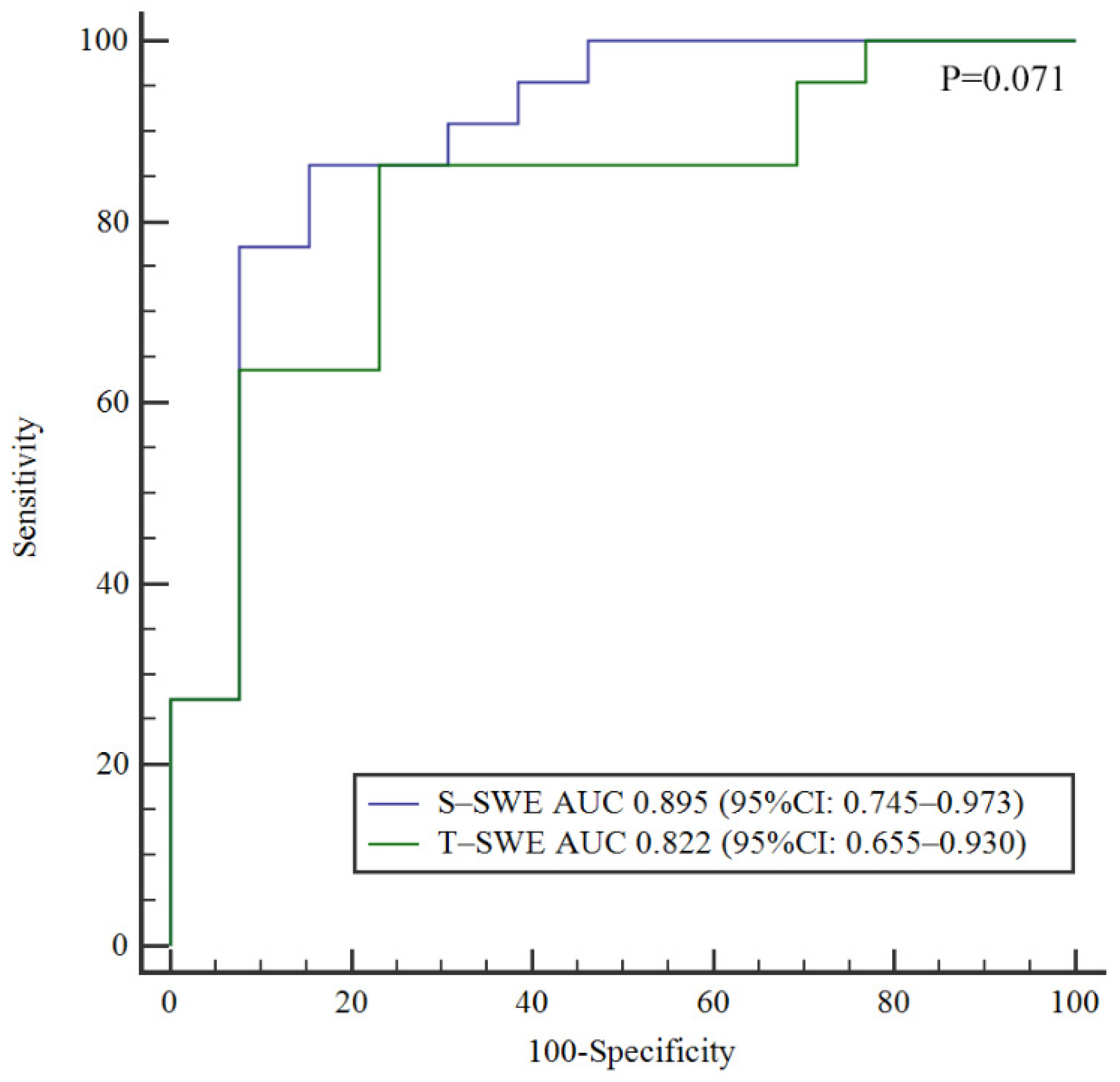
3.2. Diagnostic Performances of S-SWE and T-SWE
3.3. The Correlation between 2D-SWE Values and Serum Biochemical Tests
3.4. Inter- and Intra-Operator Error
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hartley, J.L.; Davenport, M.; Kelly, D.A. Biliary atresia. Lancet 2009, 374, 1704–1713. [Google Scholar] [CrossRef]
- Liu, Y.; Peng, C.; Wang, K.; Wu, D.; Yan, J.; Tu, W.; Chen, Y. The utility of shear wave elastography and serum biomarkers for diagnosing biliary atresia and predicting clinical outcomes. Eur. J. Pediatr. 2021, 181, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Liao, B.; Zhong, Z.; Zheng, Y.; Liu, B.; Shan, Q.; Xie, X.; Zhou, L. Supersonic shearwave elastography in the assessment of liver fibrosis for postoperative patients with biliary atresia. Sci. Rep. 2016, 6, 31057. [Google Scholar] [CrossRef]
- Thumar, V.; Squires, J.H.; Spicer, P.J.; Robinson, A.L.; Chan, S.S. Ultrasound Elastography Applications in Pediatrics. Ultrasound Q. 2018, 34, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Chen, H.; Xie, X.; Cao, Q.; Liao, B.; Jiang, H.; Shan, Q.; Zhong, Z.; Zhou, W.; Zhou, L. 2D shear wave elastography combined with age and serum biomarkers prior to kasai surgery predicts native liver survival of biliary atresia infants. J. Intern. Med. 2020, 288, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Du, L.; Zhou, J.; Li, Y.; Lei, J.; Liu, J.; Luo, Y. Diagnostic performance and prognostic value of elastography in patients with biliary atresia and after hepatic portoenterostomy: Protocol for a systematic review and meta-analysis. BMJ Open 2021, 11, e042129. [Google Scholar] [CrossRef]
- Galina, P.; Alexopoulou, E.; Mentessidou, A.; Mirilas, P.; Zellos, A.; Lykopoulou, L.; Patereli, A.; Salpasaranis, K.; Kelekis, N.L.; Zarifi, M. Diagnostic accuracy of two-dimensional shear wave elastography in detecting hepatic fibrosis in children with autoimmune hepatitis, biliary atresia and other chronic liver diseases. Pediatr. Radiol. 2021, 51, 1358–1368. [Google Scholar] [CrossRef]
- Kim, J.R.; Suh, C.H.; Yoon, H.M.; Lee, J.S.; Cho, Y.A.; Jung, A.Y. The diagnostic performance of shear-wave elastography for liver fibrosis in children and adolescents: A systematic review and diagnostic meta-analysis. Eur. Radiol. 2018, 28, 1175–1186. [Google Scholar] [CrossRef]
- Chen, H.; Zhou, L.; Liao, B.; Cao, Q.; Jiang, H.; Zhou, W.; Wang, G.; Xie, X. Two-Dimensional Shear Wave Elastography Predicts Liver Fibrosis in Jaundiced Infants with Suspected Biliary Atresia: A Prospective Study. Korean J. Radiol. 2021, 22, 959–969. [Google Scholar] [CrossRef]
- Popa, A.; Șirli, R.; Popescu, A.; Bâldea, V.; Lupușoru, R.; Bende, F.; Cotrău, R.; Sporea, I. Ultrasound-Based Quantification of Fibrosis and Steatosis with a New Software Considering Transient Elastography as Reference in Patients with Chronic Liver Diseases. Ultrasound Med. Biol. 2021, 47, 1692–1703. [Google Scholar] [CrossRef]
- Boo, Y.A.; Chang, M.H.; Jeng, Y.M.; Peng, S.F.; Hsu, W.M.; Lin, W.H.; Chen, H.L.; Ni, Y.H.; Hsu, H.Y.; Wu, J.F. Diagnostic Performance of Transient Elastography in Biliary Atresia among Infants with Cholestasis. Hepatol. Commun. 2021, 5, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Peng, Y.; Liu, W.; Yang, L.; Zhang, J. Does Supersonic Shear Wave Elastography Help Differentiate Biliary Atresia from Other Causes of Cholestatic Hepatitis in Infants Less than 90 Days Old? Compared with Grey-Scale US. BioMed Res. Int. 2019, 2019, 9036362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, L.Y.; Jiang, H.; Shan, Q.Y.; Chen, D.; Lin, X.N.; Liu, B.X.; Xie, X.Y. Liver stiffness measurements with supersonic shear wave elastography in the diagnosis of biliary atresia: A comparative study with grey-scale US. Eur. Radiol. 2017, 27, 3474–3484. [Google Scholar] [CrossRef] [PubMed]
- Dillman, J.R.; DiPaola, F.W.; Smith, S.J.; Barth, R.A.; Asai, A.; Lam, S.; Campbell, K.M.; Bezerra, J.A.; Tiao, G.M.; Trout, A.T. Prospective Assessment of Ultrasound Shear Wave Elastography for Discriminating Biliary Atresia from other Causes of Neonatal Cholestasis. J. Pediatr. 2019, 212, 60–65. [Google Scholar] [CrossRef]
- Leschied, J.R.; Dillman, J.R.; Bilhartz, J.; Heider, A.; Smith, E.A.; Lopez, M.J. Shear wave elastography helps differentiate biliary atresia from other neonatal/infantile liver diseases. Pediatr. Radiol. 2015, 45, 366–375. [Google Scholar] [CrossRef]
- Wu, J.F.; Lee, C.S.; Lin, W.H.; Jeng, Y.M.; Chen, H.L.; Ni, Y.H.; Hsu, H.Y.; Chang, M.H. Transient elastography is useful in diagnosing biliary atresia and predicting prognosis after hepatoportoenterostomy. Hepatology 2018, 68, 616–624. [Google Scholar] [CrossRef] [Green Version]
- Sandberg, J.K.; Sun, Y.; Ju, Z.; Liu, S.; Jiang, J.; Koci, M.; Rosenberg, J.; Rubesova, E.; Barth, R.A. Ultrasound shear wave elastography: Does it add value to gray-scale ultrasound imaging in differentiating biliary atresia from other causes of neonatal jaundice? Pediatr. Radiol. 2021, 51, 1654–1666. [Google Scholar] [CrossRef]
- Wang, X.; Qian, L.; Jia, L.; Bellah, R.; Wang, N.; Xin, Y.; Liu, Q. Utility of Shear Wave Elastography for Differentiating Biliary Atresia From Infantile Hepatitis Syndrome. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2016, 35, 1475–1479. [Google Scholar] [CrossRef] [Green Version]
- Goldschmidt, I.; Streckenbach, C.; Dingemann, C.; Pfister, E.D.; di Nanni, A.; Zapf, A.; Baumann, U. Application and limitations of transient liver elastography in children. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 109–113. [Google Scholar] [CrossRef]
- Engelmann, G.; Gebhardt, C.; Wenning, D.; Wühl, E.; Hoffmann, G.F.; Selmi, B.; Grulich-Henn, J.; Schenk, J.P.; Teufel, U. Feasibility study and control values of transient elastography in healthy children. Eur. J. Pediatr. 2012, 171, 353–360. [Google Scholar] [CrossRef]
- Franchi-Abella, S.; Corno, L.; Gonzales, E.; Antoni, G.; Fabre, M.; Ducot, B.; Pariente, D.; Gennisson, J.L.; Tanter, M.; Corréas, J.M. Feasibility and Diagnostic Accuracy of Supersonic Shear-Wave Elastography for the Assessment of Liver Stiffness and Liver Fibrosis in Children: A Pilot Study of 96 Patients. Radiology 2016, 278, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Tutar, O.; Beşer, Ö.F.; Adaletli, I.; Tunc, N.; Gulcu, D.; Kantarci, F.; Mihmanli, I.; Cokugras, F.C.; Kutlu, T.; Ozbay, G.; et al. Shear wave elastography in the evaluation of liver fibrosis in children. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Goodman, Z.D. Grading and staging systems for inflammation and fibrosis in chronic liver diseases. J. Hepatol. 2007, 47, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Nadebaum, D.P.; Nicoll, A.J.; Sood, S.; Gorelik, A.; Gibson, R.N. Variability of Liver Shear Wave Measurements Using a New Ultrasound Elastographic Technique. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2018, 37, 647–656. [Google Scholar] [CrossRef] [Green Version]
- Millonig, G.; Reimann, F.M.; Friedrich, S.; Fonouni, H.; Mehrabi, A.; Büchler, M.W.; Seitz, H.K.; Mueller, S. Extrahepatic cholestasis increases liver stiffness (FibroScan) irrespective of fibrosis. Hepatology 2008, 48, 1718–1723. [Google Scholar] [CrossRef]
- Guo, H.; Liao, M.; Jin, J.; Zeng, J.; Li, S.; Schroeder, D.R.; Zheng, J.; Zheng, R.; Chen, S. How intrahepatic cholestasis affects liver stiffness in patients with chronic hepatitis B: A study of 1197 patients with liver biopsy. Eur. Radiol. 2019, 30, 1096–1104. [Google Scholar] [CrossRef]
- Berzigotti, A.; De Gottardi, A.; Vukotic, R.; Siramolpiwat, S.; Abraldes, J.G.; García-Pagan, J.C.; Bosch, J. Effect of meal ingestion on liver stiffness in patients with cirrhosis and portal hypertension. PLoS ONE 2013, 8, e58742. [Google Scholar] [CrossRef] [Green Version]
- Gersak, M.M.; Badea, R.; Lenghel, L.M.; Vasilescu, D.; Botar-Jid, C.; Dudea, S.M. Influence of Food Intake on 2-D Shear Wave Elastography Assessment of Liver Stiffness in Healthy Subjects. Ultrasound Med. Biol. 2016, 42, 1295–1302. [Google Scholar] [CrossRef]
- Kutty, S.S.; Peng, Q.; Danford, D.A.; Fletcher, S.E.; Perry, D.; Talmon, G.A.; Scott, C.; Kugler, J.D.; Duncan, K.F.; Quiros-Tejeira, R.E.; et al. Increased hepatic stiffness as consequence of high hepatic afterload in the Fontan circulation: A vascular Doppler and elastography study. Hepatology 2014, 59, 251–260. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | BA (n = 22) | Non-BA (n = 13) | p Value |
|---|---|---|---|
| Age (days) | 61 (45–75) | 69 (50–87) | 0.330 |
| Male-to-female ratio | 16:6 | 10:3 | 0.557 |
| Total bilirubin level (μmol/L) | 189.2 (159.1–273.9) | 152.3 (108.1–188.9) | 0.013 |
| Direct bilirubin level (μmol/L) | 102.3 (90.2–147.1) | 86.1 (47.6–93.9) | 0.003 |
| Alanine aminotransferase level (U/L) | 134.0 (84.0–175.0) | 97.0 (49.0–163.0) | 0.231 |
| Aspartate aminotransferase level (U/L) | 214.0 (171.0–331.0) | 129.0 (79.0–334.0) | 0.201 |
| S-SWE value (kPa) | 14.0 (11.1–20.0) | 8.2 (7.1–9.7) | <0.001 |
| T-SWE value (kPa) | 11.0 (9.1–13.5) | 8.5 (6.5–9.2) | 0.002 |
| BA (n = 22) vs. Non-BA (n = 13) | F0-1 (n = 6) vs. F ≥ 2 (n = 15) | F0-2 (n = 12) vs. F ≥ 3 (n = 9) | F0-3 (n = 19) vs. F = 4(n = 2) | |
|---|---|---|---|---|
| S-SWE | ||||
| Cut-off value (kPa) | >10.2 | >13.0 | >14.0 | >27.3 |
| AUC | 0.895 (0.745–0.973) | 0.706 (0.469–0.881) | 0.676 (0.439–0.861) | 1.000 (0.839–1.000) |
| Sensitivity (%) | 77.3 (54.2–91.3) | 53.3 (27.4–77.7) | 55.6 (22.7–84.7) | 100.0 (19.8–100.0) |
| Specificity (%) | 84.6 (53.7–97.3) | 100.0 (51.7–100.0) | 83.3 (50.9–97.1) | 100.0 (79.1–100.0) |
| Accuracy (%) | 80.0 (63.8–90.3) | 66.7 (45.2–83.0) | 71.4 (49.8–86.4) | 100.0 (81.8–100.0) |
| PPV (%) | 89.5 (65.5–98.2) | 100.0 (59.8–100.0) | 71.4 (30.3–94.9) | 100.0 (19.8–100.0) |
| NPV (%) | 68.8 (41.5–87.9) | 46.2 (20.4–73.9) | 71.4 (42.0–90.4) | 100.0 (79.1–100.0) |
| T-SWE | ||||
| Cut-off value (kPa) | >8.7 | >8.9 | >13.5 | >14.7 |
| AUC | 0.822 (0.655–0.930) | 0.811 (0.583–0.946) | 0.704 (0.467–0.880) | 1.000 (0.839–1.000) |
| Sensitivity (%) | 86.4 (64.0–96.4) | 80.0 (51.4–94.7) | 33.3 (9.0–69.1) | 100.0 (19.8–100.0) |
| Specificity (%) | 76.9 (46.0–93.8) | 83.3 (36.5–99.1) | 100.0 (69.9–100.0) | 100.0 (79.1–100.0) |
| Accuracy (%) | 82.9 (66.9–92.3) | 81.0 (59.4–92.9) | 71.4 (49.8–86.4) | 100.0 (81.8–100.0) |
| PPV (%) | 86.4 (64.0–96.4) | 92.3 (62.1–99.6) | 100.0 (31.0–100.0) | 100.0 (19.8–100.0) |
| NPV (%) | 76.9 (46.0–93.8) | 62.5 (25.9–89.8) | 66.7 (41.2–85.6) | 100.0 (79.1–100.0) |
| p value * | 0.071 | 0.211 | 0.619 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, W.; Liang, J.; Shan, Q.; Chen, H.; Gao, P.; Cao, Q.; Wang, G.; Xie, X.; Zhou, L. Comparison of Two Kinds of Two-Dimensional Shear Wave Elastography Techniques in the Evaluation of Jaundiced Infants Suspected of Biliary Atresia. Diagnostics 2022, 12, 1092. https://doi.org/10.3390/diagnostics12051092
Zhou W, Liang J, Shan Q, Chen H, Gao P, Cao Q, Wang G, Xie X, Zhou L. Comparison of Two Kinds of Two-Dimensional Shear Wave Elastography Techniques in the Evaluation of Jaundiced Infants Suspected of Biliary Atresia. Diagnostics. 2022; 12(5):1092. https://doi.org/10.3390/diagnostics12051092
Chicago/Turabian StyleZhou, Wenying, Jinyu Liang, Quanyuan Shan, Huadong Chen, Pengfei Gao, Qinghua Cao, Guotao Wang, Xiaoyan Xie, and Luyao Zhou. 2022. "Comparison of Two Kinds of Two-Dimensional Shear Wave Elastography Techniques in the Evaluation of Jaundiced Infants Suspected of Biliary Atresia" Diagnostics 12, no. 5: 1092. https://doi.org/10.3390/diagnostics12051092
APA StyleZhou, W., Liang, J., Shan, Q., Chen, H., Gao, P., Cao, Q., Wang, G., Xie, X., & Zhou, L. (2022). Comparison of Two Kinds of Two-Dimensional Shear Wave Elastography Techniques in the Evaluation of Jaundiced Infants Suspected of Biliary Atresia. Diagnostics, 12(5), 1092. https://doi.org/10.3390/diagnostics12051092