
Dynamic Changes of Platelet and Factors Related Dengue Haemorrhagic Fever: A Retrospective Study in Indonesian

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
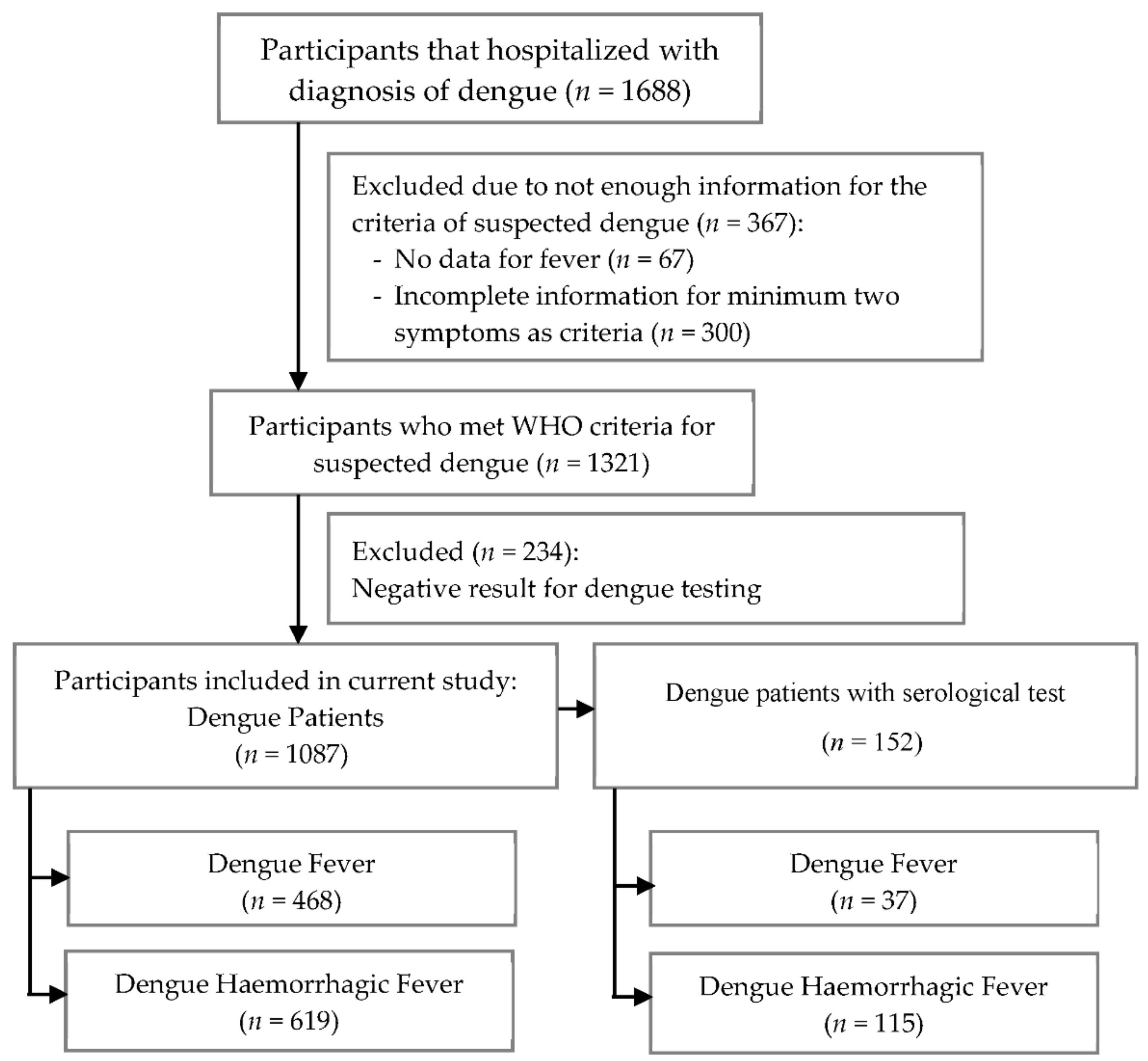
2.1. Population and Study Design
2.2. Definitions of Serum Biochemical Parameters
2.3. Statistical Analysis
3. Results
3.1. Demographics, Clinical Features, and Laboratory Data
3.2. Factors Associated with DHF
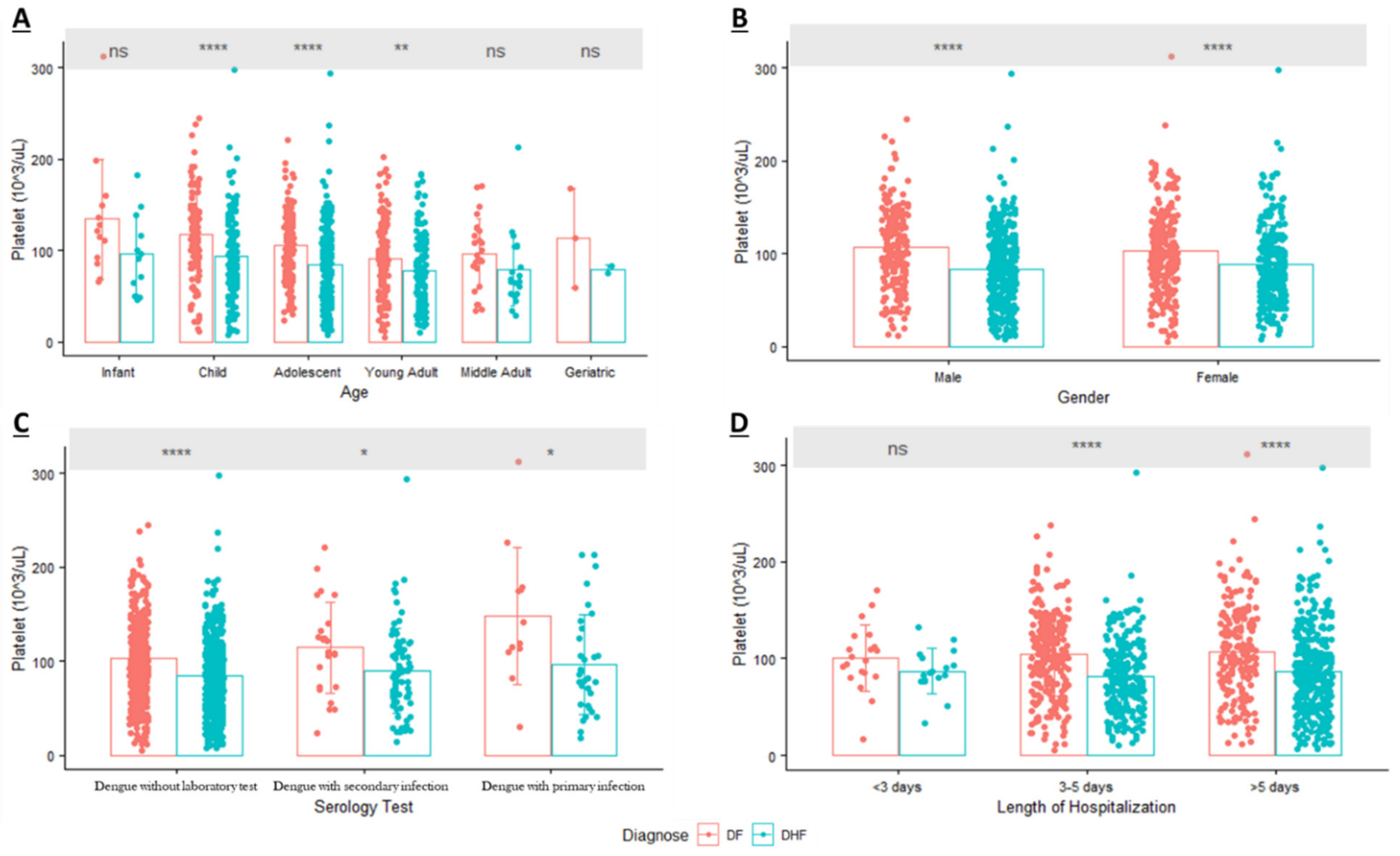
3.3. Evaluation of Platelet Profiles Related to DHF
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Messina, J.P.; Brady, O.J.; Golding, N.; Kraemer, M.U.G.; Wint, G.R.W.; Ray, S.E.; Pigott, D.M.; Shearer, F.M.; Johnson, K.; Earl, L.; et al. The current and future global distribution and population at risk of dengue. Nat. Microbiol. 2019, 4, 1508–1515. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue and Severe Dengue. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 14 December 2020).
- Harapan, H.; Michie, A.; Mudatsir, M.; Sasmono, R.T.; Imrie, A. Epidemiology of dengue hemorrhagic fever in Indonesia: Analysis of five decades data from the National Disease Surveillance. BMC Res. Notes 2019, 12, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utama, I.M.S.; Lukman, N.; Sukmawati, D.D.; Alisjahbana, B.; Alam, A.; Murniati, D.; Utama, I.; Puspitasari, D.; Kosasih, H.; Laksono, I.; et al. Dengue viral infection in Indonesia: Epidemiology, diagnostic challenges, and mutations from an observational cohort study. PLoS Negl. Trop. Dis. 2019, 13, e0007785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasmono, R.T.; Sutjianto, A.; Santoso, M.S.; Sriwedari, K.; Yohan, B.; Mayasanti, E.; Hayati, R.F.; Denis, D. Molecular epidemiology of dengue in North Kalimantan, a province with the highest incidence rates in Indonesia in 2019. Infect. Genet. Evol. 2021, 95, 105036. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.H.; Wu, W.C.; Lai, Y.C.; Tsai, P.J.; Perng, G.C.; Lin, Y.S.; Yeh, T.M. Dengue virus nonstructural protein 1 activates platelets via Toll-like receptor 4, leading to thrombocytopenia and hemorrhage. PLoS Pathog. 2019, 15, e1007625. [Google Scholar] [CrossRef] [Green Version]
- Kularatnam, G.A.M.; Jasinge, E.; Gunasena, S.; Samaranayake, D.; Senanayake, M.P.; Wickramasinghe, V.P. Evaluation of biochemical and haematological changes in dengue fever and dengue hemorrhagic fever in Sri Lankan children: A prospective follow up study. BMC Pediatrics 2019, 19, 87. [Google Scholar] [CrossRef] [Green Version]
- Lam, P.K.; Ngoc, T.V.; Thu Thuy, T.T.; Hong Van, N.T.; Nhu Thuy, T.T.; Hoai Tam, D.T.; Dung, N.M.; Hanh Tien, N.T.; Thanh Kieu, N.T.; Simmons, C.; et al. The value of daily platelet counts for predicting dengue shock syndrome: Results from a prospective observational study of 2301 Vietnamese children with dengue. PLoS Negl. Trop. Dis. 2017, 11, e0005498. [Google Scholar] [CrossRef]
- World Health Organization. Handbook for Clinical Management of Dengue; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. Dengue Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Huang, H.-S.; Hsu, C.-C.; Ye, J.-C.; Su, S.-B.; Huang, C.-C.; Lin, H.-J. Predicting the mortality in geriatric patients with dengue fever. Medicine 2017, 96, e7878. [Google Scholar] [CrossRef]
- Mallhi, T.H.; Khan, A.H.; Sarriff, A.; Adnan, A.S.; Khan, Y.H. Determinants of mortality and prolonged hospital stay among dengue patients attending tertiary care hospital: A cross-sectional retrospective analysis. BMJ Open 2017, 7, e016805. [Google Scholar] [CrossRef]
- Hsieh, C.-C.; Cia, C.-T.; Lee, J.-C.; Sung, J.-M.; Lee, N.-Y.; Chen, P.-L.; Kuo, T.-H.; Chao, J.-Y.; Ko, W.-C. A Cohort Study of Adult Patients with Severe Dengue in Taiwanese Intensive Care Units: The Elderly and APTT Prolongation Matter for Prognosis. PLoS Negl. Trop. Dis. 2017, 11, e0005270. [Google Scholar] [CrossRef]
- Lovera, D.; Martinez de Cuellar, C.; Araya, S.; Amarilla, S.; Gonzalez, N.; Aguiar, C.; Acuña, J.; Arbo, A. Clinical Characteristics and Risk Factors of Dengue Shock Syndrome in Children. Pediatric Infect. Dis. J. 2016, 35, 1294–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, J.; Hsu, J.P.; Yeo, T.W.; Leo, Y.S.; Lye, D.C. Diabetes, cardiac disorders and asthma as risk factors for severe organ involvement among adult dengue patients: A matched case-control study. Sci. Rep. 2017, 7, 39872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan American Health Organization. Dengue: Guidelines for Patient Care in the Region of the Americas, 2nd ed.; World Health Organization, Regional Office for the Americas: Washington, DC, USA, 2016. [Google Scholar]
- World Health Organization—Regional Office for South-East Asia. Comprehensive Guideline for Prevention and Control of Dengue and Dengue Haemorrhagic Fever; Revised and Expanded Edition; WHO Regional Office for South-East Asia: New Delhi, India, 2011. [Google Scholar]
- Ministry of Health Republic Indonesia. Guideline for Dengue Prevention and Control in Indonesia; Ministry of Health Republic Indonesia: Jakarta, Republic of Indonesia, 2017.
- World Health Organization. Dengue Haemorrhagic Fever: Diagnosis, Treatment, Prevention and Control, 2nd ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Sangkaew, S.; Ming, D.; Boonyasiri, A.; Honeyford, K.; Kalayanarooj, S.; Yacoub, S.; Dorigatti, I.; Holmes, A. Risk predictors of progression to severe disease during the febrile phase of dengue: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1014–1026. [Google Scholar] [CrossRef]
- Castilho, B.M.; Silva, M.T.; Freitas, A.R.R.; Fulone, I.; Lopes, L.C. Factors associated with thrombocytopenia in patients with dengue fever: A retrospective cohort study. BMJ Open 2020, 10, e035120. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.K.; Chanthavanich, P.; Limkittikul, K.; Lee, J.-S.; Sirivichayakul, C.; Lee, K.S.; Lim, S.-K.; Yoon, I.-K.; Hattasingh, W. Clinical and epidemiologic characteristics associated with dengue fever in 2011–2016 in Bang Phae district, Ratchaburi province, Thailand. PLoS Negl. Trop. Dis. 2021, 15, e0009513. [Google Scholar] [CrossRef] [PubMed]
- Malavige, G.N.; Ogg, G.S. Pathogenesis of vascular leak in dengue virus infection. Immunology 2017, 151, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Chuang, Y.-C.; Lin, Y.-S.; Liu, C.-C.; Liu, H.-S.; Liao, S.-H.; Shi, M.-D.; Lei, H.-Y.; Yeh, T.-M. Factors contributing to the disturbance of coagulation and fibrinolysis in dengue virus infection. J. Formos. Med. Assoc. 2013, 112, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Dengue Clinical Case Management (DCCM) E-Learning: Bleeding Manifestations in Patients with Dengue 2018; Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2018.
- Jayathilaka, D.; Gomes, L.; Jeewandara, C.; Jayarathna, G.S.B.; Herath, D.; Perera, P.A.; Fernando, S.; Wijewickrama, A.; Hardman, C.S.; Ogg, G.S.; et al. Role of NS1 antibodies in the pathogenesis of acute secondary dengue infection. Nat. Commun. 2018, 9, 5242. [Google Scholar] [CrossRef] [Green Version]
- Chaloemwong, J.; Tantiworawit, A.; Rattanathammethee, T.; Hantrakool, S.; Chai-Adisaksopha, C.; Rattarittamrong, E.; Norasetthada, L. Useful clinical features and hematological parameters for the diagnosis of dengue infection in patients with acute febrile illness: A retrospective study. BMC Hematol. 2018, 18, 20. [Google Scholar] [CrossRef]
- Ojha, A.; Nandi, D.; Batra, H.; Singhal, R.; Annarapu, G.K.; Bhattacharyya, S.; Seth, T.; Dar, L.; Medigeshi, G.R.; Vrati, S.; et al. Platelet activation determines the severity of thrombocytopenia in dengue infection. Sci. Rep. 2017, 7, 41697. [Google Scholar] [CrossRef]
- Her, Z.; Kam, Y.-W.; Gan, V.C.; Lee, B.; Thein, T.-L.; Tan, J.J.L.; Platform, S.I.I.; Lee, L.K.; Fink, K.; Lye, D.C.; et al. Severity of Plasma Leakage Is Associated With High Levels of Interferon γ–Inducible Protein 10, Hepatocyte Growth Factor, Matrix Metalloproteinase 2 (MMP-2), and MMP-9 During Dengue Virus Infection. J. Infect. Dis. 2017, 215, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Sahassananda, D.; Thanachartwet, V.; Chonsawat, P.; Wongphan, B.; Chamnanchanunt, S.; Surabotsophon, M.; Desakorn, V. Evaluation of Hematocrit in Adults with Dengue by a Laboratory Information System. J. Trop. Med. 2021, 2021, 8852031. [Google Scholar] [CrossRef] [PubMed]
- Wardhani, P.; Aryati, A.; Yohan, B.; Trimarsanto, H.; Setianingsih, T.Y.; Puspitasari, D.; Arfijanto, M.V.; Bramantono, B.; Suharto, S.; Sasmono, R.T. Clinical and virological characteristics of dengue in Surabaya, Indonesia. PLoS ONE 2017, 12, e0178443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ralapanawa, U.; Alawattegama, A.T.M.; Gunrathne, M.; Tennakoon, S.; Kularatne, S.A.M.; Jayalath, T. Value of peripheral blood count for dengue severity prediction. BMC Res. Notes 2018, 11, 400. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | DF (n = 468) | DHF (n = 619) | Total | p-Value | cOR | 95%CI | p-Value | Adjusted OR | 95%CI | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||||||
| Age (years), mean ± SD | 18.94 ± 13.36 | 17.92 ± 12.16 | 0.1894 | 0.994 | 0.984–1.003 | 0.1266 | 0.993 | 0.983–1.002 | |||
| Infant (<2 years old) | 13 | 2.78 | 12 | 1.94 | 25 (2.30) | 1 | 1 | ||||
| Child (2–12 years old) | 140 | 29.91 | 196 | 31.66 | 336 (30.91) | 0.3159 | 1.517 | 0.672–3.423 | 0.3133 | 1.523 | 0.672–3.451 |
| Adolescent (12–21 years old) | 144 | 30.77 | 220 | 35.54 | 364 (33.49) | 0.2241 | 1.655 | 0.735–3.729 | 0.2404 | 1.630 | 0.721–3.688 |
| Young Adult (21–45 years old) | 142 | 30.34 | 166 | 26.82 | 308 (28.33) | 0.5705 | 1.266 | 0.560–2.864 | 0.6005 | 1.245 | 0.548–2.826 |
| Middle Adult (45–65 years old) | 26 | 5.56 | 23 | 3.72 | 49 (4.51) | 0.9311 | 0.958 | 0.365–2.514 | 0.835 | 0.902 | 0.342–2.379 |
| Geriatric (>65 years old) | 3 | 0.64 | 2 | 0.32 | 5 (0.46) | 0.7441 | 0.722 | 0.102–5.095 | 0.6508 | 0.636 | 0.089–4.520 |
| Male Gender | 218 | 46.58 | 346 | 55.9 | 564 (51.89) | 0.0024 | 1.453 | 1.142–1.850 | 0.0017 | 1.473 | 1.156–1.877 |
| Length of Hospitalization (days), mean ± SD | 4.42 ± 1.35 | 4.85 ± 1.41 | <0.0001 | 1.260 | 1.150–1.380 | <0.0001 | 1.267 | 1.156–1.388 | |||
| Laboratory Confirmation Test | |||||||||||
| Dengue without laboratory test | 431 | 92.09 | 504 | 81.42 | 935 (86.02) | ||||||
| Dengue with laboratory test | 37 | 7.91 | 115 | 18.58 | 152 (13.98) | ||||||
| Primary Infection | 12 | 32.43 | 33 | 28.7 | 45 (29.61) | 0.6652 | 1 | 0.7782 | 1 | ||
| Secondary Infection | 25 | 67.57 | 82 | 71.3 | 107 (70.39) | 1.193 | 0.537–2.650 | 1.125 | 0.496–2.549 | ||
| Symptom | DF (n = 468) | DHF (n = 619) | Total | p-Value | cOR | 95%CI | p-Value | Adjusted OR | 95%CI | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||||||
| Headache | 168 | 35.9 | 221 | 35.7 | 389 (35.79) | 0.9471 | 0.992 | 0.772–1.274 | 0.8255 | 1.029 | 0.797–1.329 |
| Rash | 11 | 2.35 | 13 | 2.1 | 24 (2.21) | 0.7797 | 0.891 | 0.395–2.006 | 0.9279 | 0.963 | 0.425–2.180 |
| Fatigue | 28 | 5.98 | 21 | 3.39 | 49 (4.51) | 0.0442 | 0.552 | 0.309–0.985 | 0.0381 | 0.54 | 0.302–0.967 |
| Diarrhea | 32 | 6.84 | 36 | 5.82 | 68 (6.26) | 0.4914 | 0.841 | 0.514–1.376 | 0.3638 | 0.795 | 0.484–1.305 |
| Gum Bleeding | 13 | 2.78 | 14 | 2.26 | 27 (2.48) | 0.5889 | 0.81 | 0.377–1.740 | 0.6416 | 0.833 | 0.386–1.799 |
| Nausea/Vomiting | 295 | 63.03 | 433 | 69.95 | 728 (66.97) | 0.0165 | 1.365 | 1.058–1.761 | 0.0134 | 1.385 | 1.070–1.792 |
| Abdominal Pain | 90 | 19.23 | 146 | 23.59 | 236 (21.71) | 0.085 | 1.296 | 0.965–1.742 | 0.0452 | 1.358 | 1.007–1.832 |
| Bone Pain | 30 | 6.41 | 28 | 4.52 | 58 (5.34) | 0.1726 | 0.692 | 0.407–1.175 | 0.2021 | 0.706 | 0.414–1.205 |
| Hemoptysis | 15 | 3.21 | 35 | 5.65 | 50 (4.6) | 0.0596 | 1.809 | 0.976–3.354 | 0.0657 | 1.790 | 0.963–3.329 |
| Leucopenia (WBC < 5000) | 281 | 73.75 | 303 | 73.72 | 584 (73.74) | 0.9922 | 0.998 | 0.727–1.370 | 0.8093 | 0.961 | 0.695–1.329 |
| High Hematocrit (HCT > 42) | 190 | 41.13 | 311 | 50.24 | 501 (46.35) | 0.003 | 1.446 | 1.133–1.844 | 0.0117 | 1.384 | 1.075–1.782 |
| Thrombocytopenia (PLT < 105) | 218 | 46.78 | 411 | 66.94 | 629 (58.24) | <0.0001 | 2.303 | 1.798–2.951 | <0.0001 | 2.412 | 1.873–3.106 |
| HCT > 42 & PLT < 50 | 28 | 6.01 | 72 | 11.73 | 100 (9.26) | 0.0016 | 2.077 | 1.319–3.271 | 0.0028 | 2.013 | 1.273–3.184 |
| Elevated SGPT (SGPT > 56) | 39 | 60.94 | 40 | 51.95 | 79 (56.03) | 0.285 | 0.693 | 0.354–1.357 | 0.1835 | 0.625 | 0.313–1.249 |
| Elevated SGOT (SGOT > 40) | 35 | 54.69 | 53 | 68.83 | 88 (62.41) | 0.0857 | 1.830 | 0.919–3.644 | 0.1545 | 1.666 | 0.825–3.364 |
| Variables (Unit), Mean ± SD | n | Dengue Fever | n | Dengue Hemorrhagic Fever | p-Value |
|---|---|---|---|---|---|
| Leucocytes (/mm3) | 381 | 4720 ± 4370 | 411 | 4340 ± 2720 | 0.435 |
| Hematocrit (%) | 462 | 40.68 ± 6.29 | 619 | 41.67 ± 6.04 | 0.0027 |
| Platelet (/mm3) | 466 | 104.73 ± 43.92 | 614 | 85.13 ± 41.48 | <0.0001 |
| Blood Glucose (mg/dL) | 55 | 111.60 + 38.12 | 80 | 109.84 ± 41.56 | 0.5863 |
| Hemoglobin (g/dL) | 346 | 14.17 + 2.01 | 385 | 14.43 ± 2.03 | 0.0487 |
| SGPT (U/L) | 64 | 83.54 ± 55.85 | 77 | 79.49 ± 70.26 | 0.1893 |
| SGOT (U/L) | 64 | 86.74 ± 62.68 | 77 | 121.16 ± 146.66 | 0.1992 |
| Creatinine (mg/dL) | 16 | 0.80 ± 0.32 | 36 | 0.83 ± 0.25 | 0.5922 |
| Characteristic | Dengue Patients with Laboratory Test (n = 152) | ||
|---|---|---|---|
| p-Value | cOR | 95%CI | |
| Young Adult (21–45 years old) | 0.1449 | 7.378 | 0.502–108.349 |
| Male Gender | 0.8436 | 1.113 | 0.385–3.216 |
| Length of Hospitalization | 0.0018 | 1.883 | 1.264–2.803 |
| Fatigue | 0.8846 | 1.217 | 0.086–17.250 |
| Gum Bleeding | 0.0115 | 0.075 | 0.01–0.559 |
| Nausea/Vomiting | 0.6159 | 1.338 | 0.429–4.171 |
| Abdominal Pain | 0.6885 | 1.248 | 0.423–3.678 |
| High Hematocrit (Hct > 42) | 0.4428 | 1.574 | 0.494–5.016 |
| Thrombocytopenia (Plt < 100,000) | 0.0029 | 6.058 | 1.848–19.862 |
| Hct > 42 & Plt < 50 | 0.1746 | 0.3 | 0.053–1.707 |
| Hemoglobin | 0.0206 | 0.919 | 0.855–0.987 |
| Day of Hospitalization | n | Platelet Count of Dengue Fever | n | Platelet Count of Dengue Hemorrhagic Fever | p-Value | |
|---|---|---|---|---|---|---|
| Dengue Patients (n = 1087) | Day 1 | 466 | 104.73 ± 43.92 | 614 | 85.13 ± 41.48 | <0.0001 |
| Day 3 | 418 | 84.97 ± 40.34 | 564 | 64.93 ± 34.21 | <0.0001 | |
| Last Day | 409 | 113.17 ± 43.26 | 571 | 103.12 ± 40.50 | <0.0001 | |
| Dengue Patients with Serological Test (n = 152) | Day 1 | 37 | 125.32 ± 58.78 | 115 | 91.28 ± 47.45 | 0.0005 |
| Day 3 | 26 | 91.87 ± 35.36 | 86 | 74.57 ± 45.15 | 0.0151 | |
| Last Day | 36 | 111.09 ± 46.83 | 113 | 112.74 ± 45.11 | 0.7478 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faridah, I.N.; Dania, H.; Chen, Y.-H.; Supadmi, W.; Purwanto, B.D.; Heriyanto, M.J.; Aufa, M.A.; Chang, W.-C.; Perwitasari, D.A. Dynamic Changes of Platelet and Factors Related Dengue Haemorrhagic Fever: A Retrospective Study in Indonesian. Diagnostics 2022, 12, 950. https://doi.org/10.3390/diagnostics12040950
Faridah IN, Dania H, Chen Y-H, Supadmi W, Purwanto BD, Heriyanto MJ, Aufa MA, Chang W-C, Perwitasari DA. Dynamic Changes of Platelet and Factors Related Dengue Haemorrhagic Fever: A Retrospective Study in Indonesian. Diagnostics. 2022; 12(4):950. https://doi.org/10.3390/diagnostics12040950
Chicago/Turabian StyleFaridah, Imaniar Noor, Haafizah Dania, Yen-Hsu Chen, Woro Supadmi, Barkah Djaka Purwanto, Mochammad Junaidy Heriyanto, Mahda Adil Aufa, Wei-Chiao Chang, and Dyah Aryani Perwitasari. 2022. "Dynamic Changes of Platelet and Factors Related Dengue Haemorrhagic Fever: A Retrospective Study in Indonesian" Diagnostics 12, no. 4: 950. https://doi.org/10.3390/diagnostics12040950
APA StyleFaridah, I. N., Dania, H., Chen, Y.-H., Supadmi, W., Purwanto, B. D., Heriyanto, M. J., Aufa, M. A., Chang, W.-C., & Perwitasari, D. A. (2022). Dynamic Changes of Platelet and Factors Related Dengue Haemorrhagic Fever: A Retrospective Study in Indonesian. Diagnostics, 12(4), 950. https://doi.org/10.3390/diagnostics12040950