
The ETS Homologous Factor (EHF) Represents a Useful Immunohistochemical Marker for Predicting Prostate Cancer Metastasis

 ,
,  , , , ,
, , , ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Prostate Samples Collection
2.2. Immunohistochemistry
2.3. Bioinformatics Analysis
2.4. Statistical Analysis
3. Results
3.1. Prostate Lesions Classification
According to the GG, lesions were classified as follows: 15.9% GG1 (Gleason score ≤ 6), 9.4% GG2 (Gleason score 3 + 4), 16.5% GG3 (Gleason score 4 + 3), 21.5% GG4 (Gleason score 4 + 4), and 8.1% GG5 (Gleason score ≥ 9). No specific association was observed between the GG and the occurrence of metastasis. In all patients who underwent prostatectomy during the follow-up (n = 12), histological analysis confirmed the GG value of the first diagnosis (i.e., the highest GG value obtained in the biopsies).
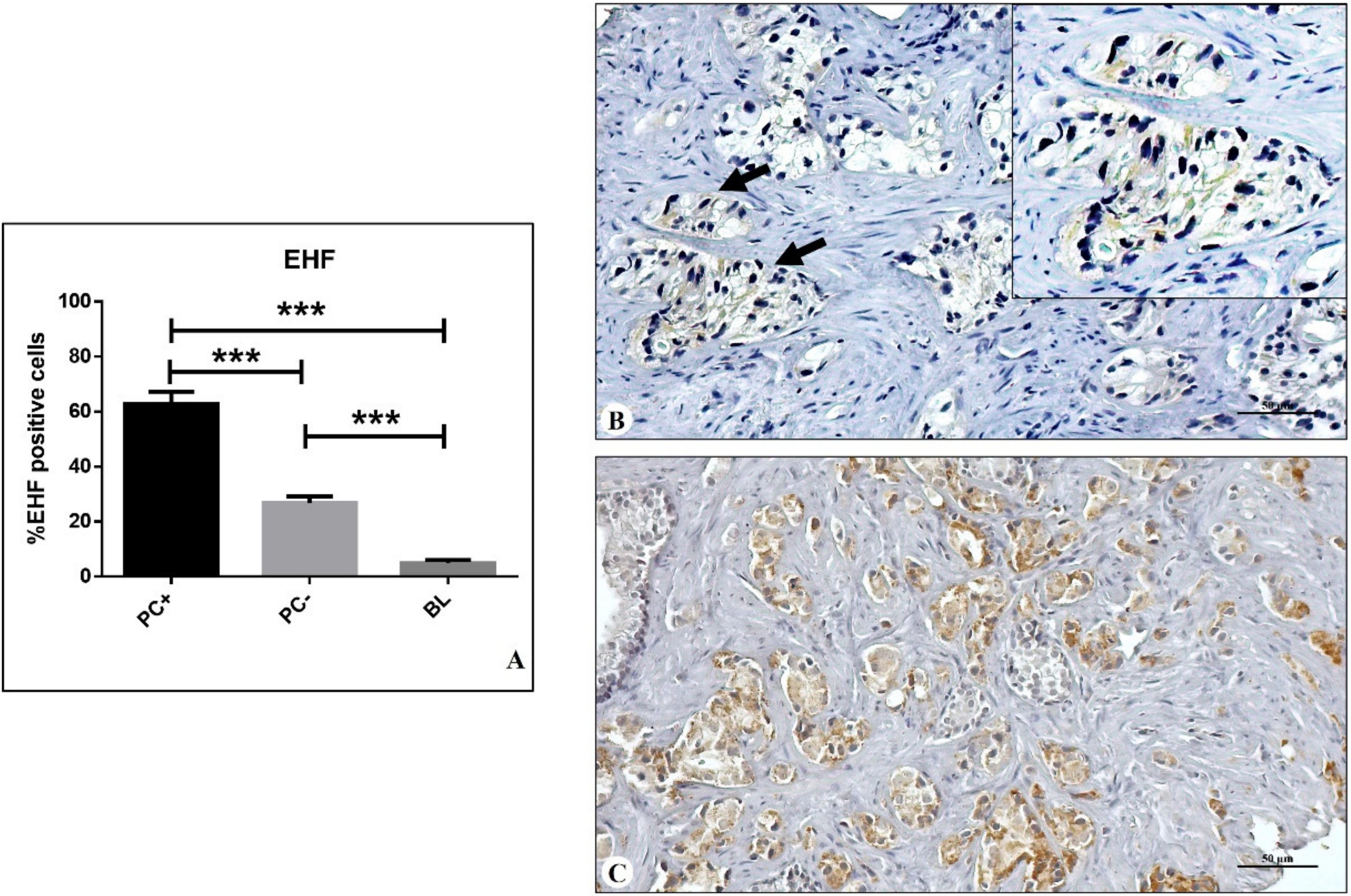
3.2. EHF Expression
3.3. Bioinformatics Analysis
3.4. Risk of Prostate Metastasis Formation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLO-BOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading Committee. The 2014 International Society of urological pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Beyer, K.; Moris, L.; Lardas, M.; Haire, A.; Barletta, F.; Scuderi, S.; Vradi, E.; Gandaglia, G.; Omar, M.I.; MacLennan, S.; et al. Diagnostic and prognostic factors in patients with prostate cancer: A systematic review protocol. BMJ Open 2021, 11, e040531. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part B: Prostate and Bladder Tumours. Eur. Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef]
- Kweldam, C.F.; van Leenders, G.J.; van der Kwast, T. Grading of prostate cancer: A work in progress. Histopathology 2019, 74, 146–160. [Google Scholar] [CrossRef]
- Urbano, N.; Scimeca, M.; Tolomeo, A.; Dimiccoli, V.; Bonanno, E.; Schillaci, O. Novel Biological and Molecular Characterization in Radiopharmaceutical Preclinical Design. J. Clin. Med. 2021, 10, 4850. [Google Scholar] [CrossRef]
- Mapelli, S.N.; Albino, D.; Mello-Grand, M.; Shinde, D.; Scimeca, M.; Bonfiglio, R.; Bonanno, E.; Chiorino, G.; Garcia-Escudero, R.; Catapano, C.V.; et al. A Novel Prostate Cell Type-Specific Gene Signature to Interrogate Prostate Tumor Differentiation Status and Monitor Therapeutic Response (Running Title: Phenotypic Classification of Prostate Tumors). Cancers 2020, 12, 176. [Google Scholar] [CrossRef]
- Kai, K.; Dittmar, R.; Sen, S. Secretory microRNAs as biomarkers of cancer. Semin. Cell Dev. Biol. 2018, 78, 22–36. [Google Scholar] [CrossRef]
- Hu, D.; Cao, Q.; Tong, M.; Ji, C.; Li, Z.; Huang, W.; Jin, Y.; Tong, G.; Wang, Y.; Li, P.; et al. A novel defined risk signature based on pyroptosis-related genes can predict the prognosis of prostate cancer. BMC Med. Genom. 2022, 15, 1–17. [Google Scholar] [CrossRef]
- Tucci, P.; Agostini, M.; Grespi, F.; Markert, E.K.; Terrinoni, A.; Vousden, K.H.; Muller, P.A.J.; Dötsch, V.; Kehrloesser, S.; Sayan, B.S.; et al. Loss of p63 and its microRNA-205 target results in enhanced cell migration and metastasis in prostate cancer. Proc. Natl. Acad. Sci. USA 2012, 109, 15312–15317. [Google Scholar] [CrossRef] [PubMed]
- Scimeca, M.; Bonfiglio, R.; Varone, F.; Ciuffa, S.; Mauriello, A.; Bonanno, E. Calcifications in prostate cancer: An active phe-nomenon mediated by epithelial cells with osteoblast-phenotype. Microsc. Res. Tech. 2018, 81, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Scimeca, M.; Urbano, N.; Rita, B.; Mapelli, S.N.; Catapano, C.V.; Carbone, G.M.; Ciuffa, S.; Tavolozza, M.; Schillaci, O.; Mauriello, A.; et al. Prostate Osteoblast-Like Cells: A Reliable Prognostic Marker of Bone Metastasis in Prostate Cancer Patients. Contrast Media Mol. Imaging 2018, 2018, 9840962. [Google Scholar] [CrossRef] [PubMed]
- Parol-Kulczyk, M.; Gzil, A.; Ligmanowska, J.; Grzanka, D. Prognostic significance of SDF-1 chemokine and its receptors CXCR4 and CXCR7 involved in EMT of prostate cancer. Cytokine 2022, 150, 155778. [Google Scholar] [CrossRef]
- Zheng, Y.; Li, P.; Huang, H.; Ye, X.; Chen, W.; Xu, G.; Zhang, F. Androgen receptor regulates eIF5A2 expression and promotes prostate cancer metastasis via EMT. Cell Death Discov. 2021, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lamouille, S.; Xu, J.; Derynck, R. Molecular mechanisms of epithelial–mesenchymal transition. Nat. Rev. Mol. Cell Biol. 2014, 15, 178–196. [Google Scholar] [CrossRef] [PubMed]
- Georgakopoulos-Soares, I.; Chartoumpekis, D.V.; Kyriazopoulou, V.; Zaravinos, A. EMT Factors and Metabolic Pathways in Cancer. Front. Oncol. 2020, 10, 499. [Google Scholar] [CrossRef]
- Cho, E.S.; Kang, H.E.; Kim, N.H.; Yook, J.I. Therapeutic implications of cancer epithelial-mesenchymal transition (EMT). Arch. Pharm. Res. 2019, 42, 14–24. [Google Scholar] [CrossRef]
- Gao, L.; Yang, T.; Zhang, S.; Liang, Y.; Shi, P.; Ren, H.; Hou, P.; Chen, M. EHF enhances malignancy by modulating AKT and MAPK/ERK signaling in non-small cell lung cancer cells. Oncol. Rep. 2021, 45, 102. [Google Scholar] [CrossRef]
- Gu, M.-L.; Zhou, X.-X.; Ren, M.-T.; Shi, K.-D.; Yu, M.-S.; Jiao, W.-R.; Wang, Y.-M.; Zhong, W.-X.; Ji, F. Blockage of ETS homologous factor inhibits the proliferation and invasion of gastric cancer cells through the c-Met pathway. World J. Gastroenterol. 2020, 26, 7497–7512. [Google Scholar] [CrossRef]
- Luk, I.Y.; Reehorst, C.M.; Mariadason, J.M. ELF3, ELF5, EHF and SPDEF Transcription Factors in Tissue Homeostasis and Cancer. Molecules 2018, 23, 2191. [Google Scholar] [CrossRef]
- Zhou, T.; Liu, J.; Xie, Y.; Yuan, S.; Guo, Y.; Bai, W.; Zhao, K.; Jiang, W.; Wang, H.; Wang, H.; et al. ESE3/EHF, a promising target of rosiglitazone, suppresses pancreatic cancer stemness by down-regulating CXCR4. Gut 2022, 71, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, K.; Endo, K.; Sakamoto, K.; Kayamori, K.; Ehata, S.; Ichikawa, J.; Ando, T.; Nakamura, R.; Kimura, Y.; Yoshizawa, K.; et al. EHF suppresses cancer pro-gression by inhibiting ETS1-mediated ZEB expression. Oncogenesis 2021, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Long, Z.; Deng, L.; Li, C.; He, Q.; He, Y.; Hu, X.; Cai, Y.; Gan, Y. Loss of EHF facilitates the development of treatment-induced neuroendocrine prostate cancer. Cell Death Dis. 2021, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Reehorst, C.M.; Nightingale, R.; Luk, I.Y.; Jenkins, L.; Koentgen, F.; Williams, D.S.; Darido, C.; Tan, F.; Anderton, H.; Chopin, M.; et al. EHF is essential for epidermal and colonic epithelial homeostasis, and suppresses Apc-initiated colonic tumorigenesis. Development 2021, 148, dev199542. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Guo, J.; Chen, L.; Luo, N.; Yang, W.; Qu, X. Knockdown of EHF inhibited the proliferation, invasion and tumor-igenesis of ovarian cancer cells. Mol. Carcinog. 2016, 55, 1048–1059. [Google Scholar] [CrossRef]
- Dallavalle, C.; Albino, D.; Civenni, G.; Merulla, J.; Ostano, P.; Mello-Grand, M.; Rossi, S.; Losa, M.; D’Ambrosio, G.; Sessa, F.; et al. MicroRNA-424 impairs ubiquitination to activate STAT3 and promote prostate tumor progression. J. Clin. Investig. 2016, 126, 4585–4602. [Google Scholar] [CrossRef]
- Civenni, G.; Albino, D.; Shinde, D.; Vázquez, R.; Merulla, J.; Kokanovic, A.; Mapelli, S.N.; Carbone, G.M.; Catapano, C.V. Transcriptional Reprogramming and Novel Therapeutic Approaches for Targeting Prostate Cancer Stem Cells. Front. Oncol. 2019, 9, 385. [Google Scholar] [CrossRef]
- Albino, D.; Civenni, G.; Rossi, S.; Mitra, A.; Catapano, C.V.; Carbone, G.M. The ETS factor ESE3/EHF represses IL-6 pre-venting STAT3 activation and expansion of the prostate cancer stem-like compartment. Oncotarget 2016, 7, 76756–76768. [Google Scholar] [CrossRef] [PubMed]
- Albino, D.; Civenni, G.; Dallavalle, C.; Roos, M.; Jahns, H.; Curti, L.; Rossi, S.; Pinton, S.; D’Ambrosio, G.; Sessa, F.; et al. Activation of the Lin28/let-7 Axis by Loss of ESE3/EHF Promotes a Tumorigenic and Stem-like Phenotype in Prostate Cancer. Cancer Res. 2016, 76, 3629–3643. [Google Scholar] [CrossRef]
- Longoni, N.; Kunderfranco, P.; Pellini, S.; Albino, D.; Mello-Grand, M.; Pinton, S.; D’Ambrosio, G.; Sarti, M.; Sessa, F.; Chiorino, G.; et al. Aberrant expression of the neuronal-specific protein DCDC2 promotes malignant pheno-types and is associated with prostate cancer progression. Oncogene 2013, 32, 2315–2324, 2324.e1–2324.e4. [Google Scholar] [CrossRef]
- Scimeca, M.; Anemona, L.; Granaglia, A.; Bonfiglio, R.; Urbano, N.; Toschi, N.; Santeusanio, G.; Schiaroli, S.; Mauriello, S.; Tancredi, V.; et al. Plaque calcification is driven by different mechanisms of mineralization associated with specific cardiovascular risk factors. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1330–1336. [Google Scholar] [CrossRef] [PubMed]
- Scimeca, M.; Bonfiglio, R.; Urbano, N.; Cerroni, C.; Anemona, L.; Montanaro, M.; Fazi, S.; Schillaci, O.; Mauriello, A.; Bonanno, E. Programmed death ligand 1 expression in prostate cancer cells is associated with deep changes of the tumor inflammatory infiltrate composition. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 297.e19–297.e31. [Google Scholar] [CrossRef] [PubMed]
- Bartha, Á.; Győrffy, B. TNMplot.com: A Web Tool for the Comparison of Gene Expression in Normal, Tumor and Metastatic Tissues. Int. J. Mol. Sci. 2021, 22, 2622. [Google Scholar] [CrossRef] [PubMed]
- Fossum, S.L.; Mutolo, M.J.; Yang, R.; Dang, H.; O’Neal, W.K.; Knowles, M.R.; Leir, S.-H.; Harris, A. Ets homologous factor regulates pathways controlling response to injury in airway epithelial cells. Nucleic Acids Res. 2014, 42, 13588–13598. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Li, J.; Guo, Y.; Wang, R.; Hua, L.; Gan, D.; Zhu, L.; Ma, P.; Yang, J.; Li, H.; et al. Ese-3 Inhibits the Proliferation, Migration, and Invasion of HaCaT Cells by Downregulating PSIP1 and NUCKS1. Ann. Clin. Lab. Sci. 2021, 51, 470–486. [Google Scholar] [PubMed]
- Saitoh, M. Involvement of partial EMT in cancer progression. J. Biochem. 2018, 164, 257–264. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| a | ||||
|---|---|---|---|---|
| ODDs RATIO | 95% CI | p | ||
| Lower | Upper | |||
| EHF30 | 0.381 | 0.296 | 0.491 | 0.001 |
| EHF40 | 45.043 | 5.62 | 361.27 | 0.001 |
| EHF50 | 42.000 | 8.49 | 207.86 | 0.001 |
| b | ||||
| ODDs RATIO | 95% CI | p | ||
| Lower | Upper | |||
| PSA * | 1.40 | 0.29 | 6.77 | 0.67 |
| GG ** | 7.31 | 0.72 | 74.48 | 0.09 |
| EHF *** | 50.19 | 5.90 | 427.12 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scimeca, M.; Montanaro, M.; Bonfiglio, R.; Anemona, L.; Agrò, E.F.; Asimakopoulos, A.D.; Bei, R.; Manzari, V.; Urbano, N.; Giacobbi, E.; et al. The ETS Homologous Factor (EHF) Represents a Useful Immunohistochemical Marker for Predicting Prostate Cancer Metastasis. Diagnostics 2022, 12, 800. https://doi.org/10.3390/diagnostics12040800
Scimeca M, Montanaro M, Bonfiglio R, Anemona L, Agrò EF, Asimakopoulos AD, Bei R, Manzari V, Urbano N, Giacobbi E, et al. The ETS Homologous Factor (EHF) Represents a Useful Immunohistochemical Marker for Predicting Prostate Cancer Metastasis. Diagnostics. 2022; 12(4):800. https://doi.org/10.3390/diagnostics12040800
Chicago/Turabian StyleScimeca, Manuel, Manuela Montanaro, Rita Bonfiglio, Lucia Anemona, Enrico Finazzi Agrò, Anastasios D. Asimakopoulos, Roberto Bei, Vittorio Manzari, Nicoletta Urbano, Erica Giacobbi, and et al. 2022. "The ETS Homologous Factor (EHF) Represents a Useful Immunohistochemical Marker for Predicting Prostate Cancer Metastasis" Diagnostics 12, no. 4: 800. https://doi.org/10.3390/diagnostics12040800
APA StyleScimeca, M., Montanaro, M., Bonfiglio, R., Anemona, L., Agrò, E. F., Asimakopoulos, A. D., Bei, R., Manzari, V., Urbano, N., Giacobbi, E., Servadei, F., Bonanno, E., Schillaci, O., & Mauriello, A. (2022). The ETS Homologous Factor (EHF) Represents a Useful Immunohistochemical Marker for Predicting Prostate Cancer Metastasis. Diagnostics, 12(4), 800. https://doi.org/10.3390/diagnostics12040800