
Radiomic Applications on Digital Breast Tomosynthesis of BI-RADS Category 4 Calcifications Sent for Vacuum-Assisted Breast Biopsy

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
- Detection of microcalcification at the most recent mammography.
- Microcalcifications classified by a radiologist as BI-RADS category 4.
- Execution of VABB in high-definition breast tomosynthesis.
- Histological examination of the specimens in our institution.
- Presence of a mass or an architectural distortion associated with microcalcification.
- Allergic reaction to the local anesthetic.
- Hemorrhagic diathesis or the impossibility of discontinuing an antiplatelet/anticoagulant therapy.
- Technical unfeasibility of the execution of VABB (not cooperative patients, thin breast, microcalcifications too close to the chest wall or near the skin or in the breast tissue of the axillary tails).
- B1 (Uninterpretable/Normal tissue only): indicates a core of normal tissue or an uninterpretable specimen, for example, due to an excessive crush artifact or composed of blood clots only.
- B2 (Benign lesion): indicates the presence of a benign abnormality such as fibroadenomas, fibrocystic changes, sclerosing adenosis, and duct ectasia.
- B3 (Lesion of uncertain malignant potential): indicates lesions that may provide benign histology in needle core biopsy (NCB) but are either known to show heterogeneity or to have an increased risk of associated malignancy (e.g., papillary lesions, radial scar/complex sclerosing lesion, lobular intraepithelial neoplasia, atypical epithelial proliferation of ductal type and phyllodes tumor).
- B4 (Suspicious for malignancy): indicates apparently neoplastic cells contained within blood clots or adherent to the outer aspect of the sample or technical problems such as crushed or poorly fixed cores which contain probable carcinoma.
- B5 (Malignant): indicates unequivocal malignancy on NCB. Further categorization into in situ (B5a) and invasive malignancy (B5b) should be undertaken whenever possible.
- Benign group: 126 patients with category B2 addressed to imaging follow-up.
- Malignant group: 126 patients with category B3 (45 patients), B5a (63 patients), and B5b (18 patients) addressed to surgical excision.
2.2. Imaging Protocol
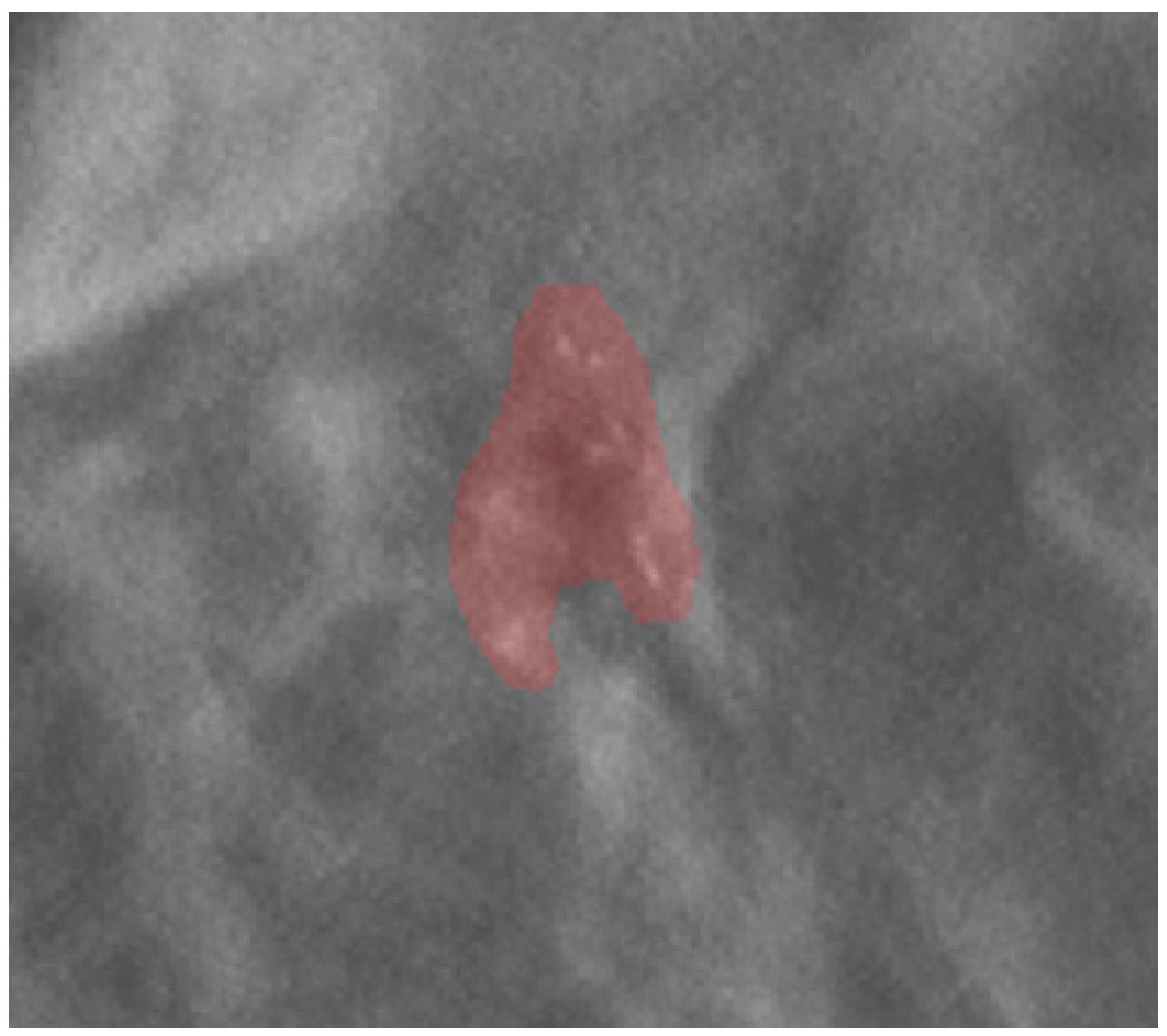
2.3. Image Segmentation and Feature Extraction
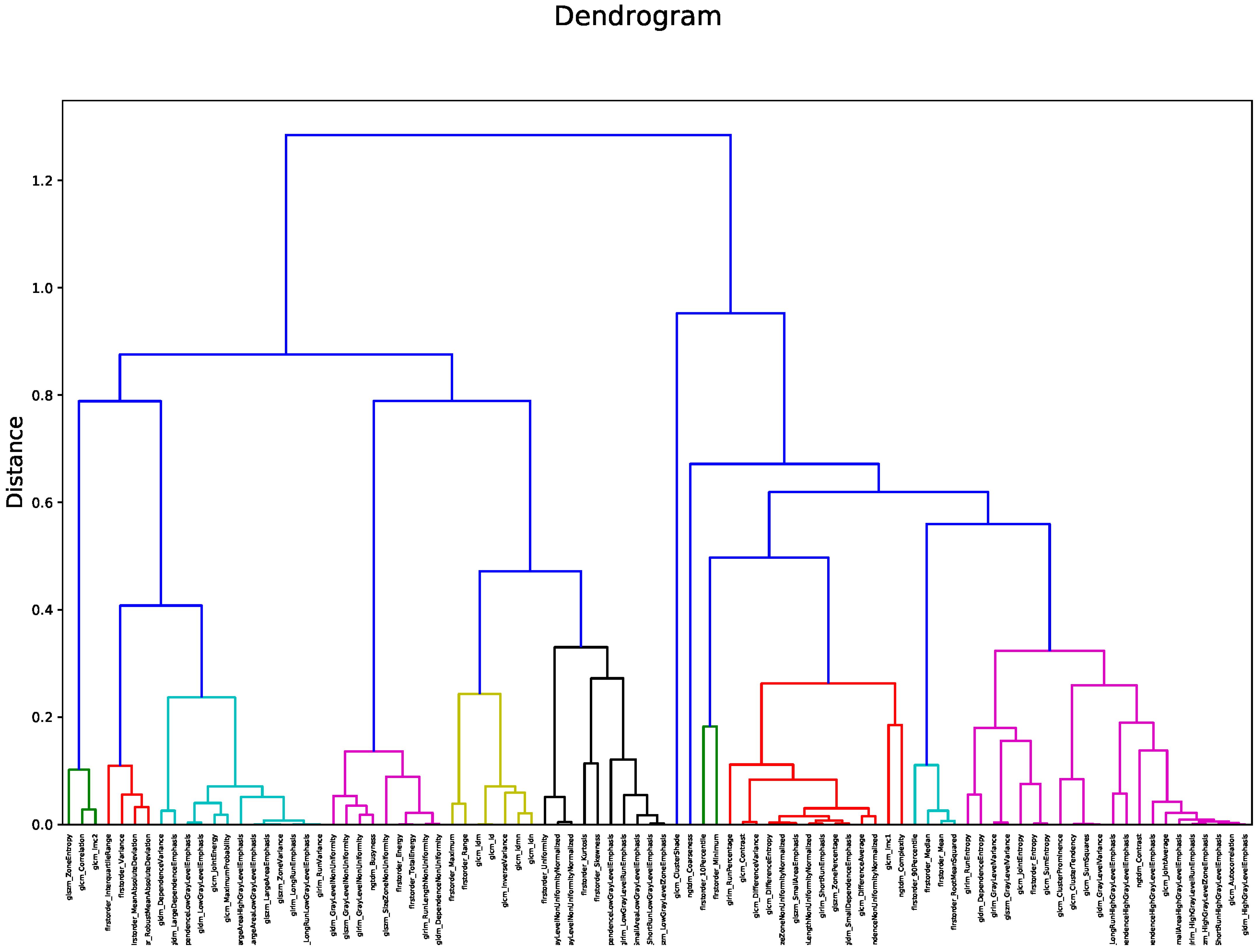
2.4. Feature Selection
2.5. Classification
3. Results
3.1. Features Selection
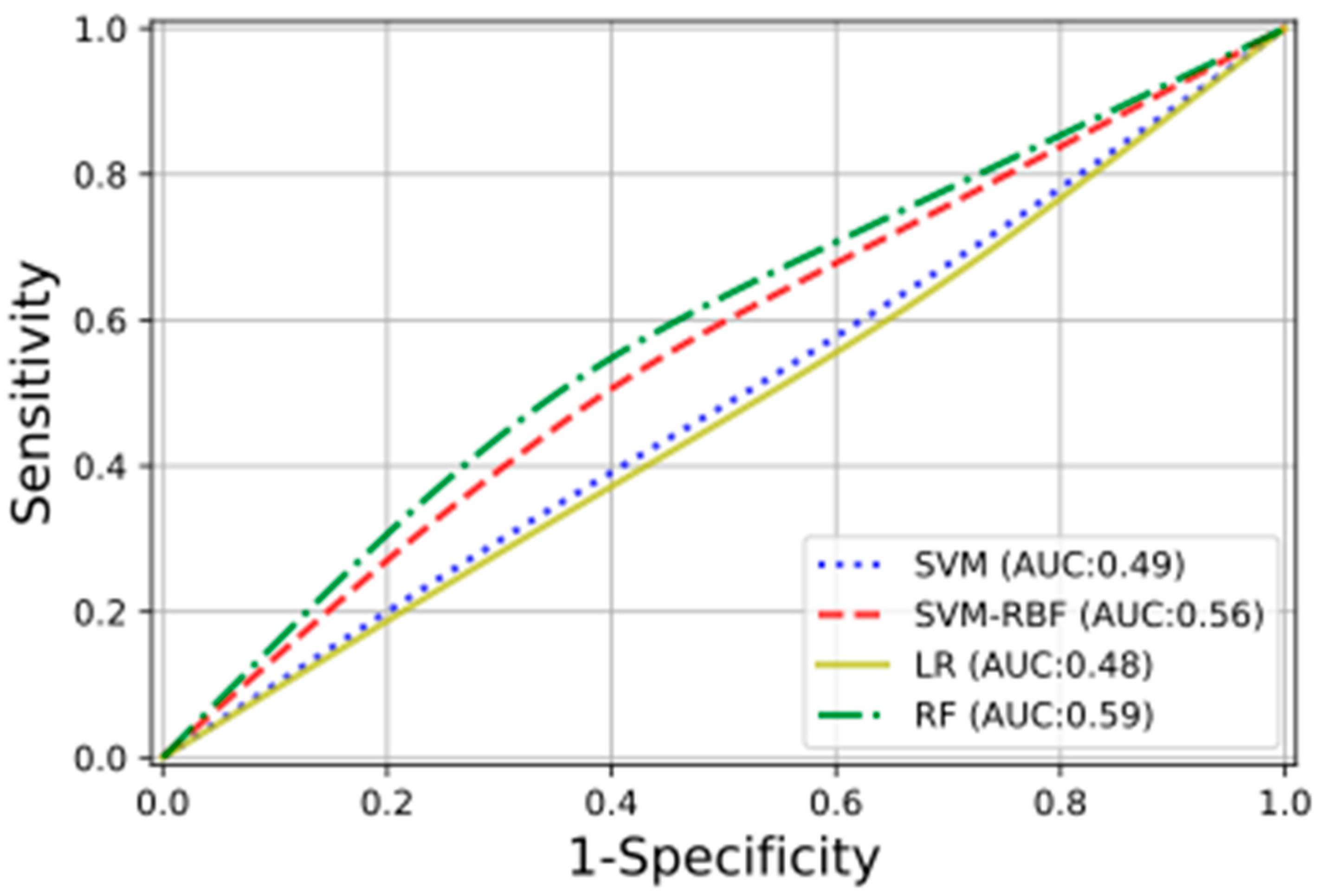
3.2. Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | area under the curve |
| BI-RADS | Breast Imaging Reporting and Data System |
| CI | confidence interval |
| CV | cross-validation |
| DBT | digital breast tomosynthesis |
| DCE-MRI | dynamic contrast-enhanced magnetic resonance imaging |
| DCIS | ductal carcinoma in situ |
| GLCM | gray level co-occurrence matrix |
| GLDM | gray level dependence matrix |
| GLRLM | gray level run length matrix |
| GLSZM | gray level size zone features |
| IBSI | Image Biomarker Standardization Initiative |
| LR | logistic regression |
| ML | machine-learning |
| NCB | needle core biopsy |
| NGTDM | neighboring gray tone difference matrix |
| RBF | radial basis function |
| RF | random forest |
| ROI | region of interest |
| SVM | support vector machine |
| VABB | vacuum-assisted breast biopsy |
References
- Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN). Breast Cancer Screening. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 797–798. [Google Scholar] [CrossRef][Green Version]
- Løberg, M.; Lousdal, M.L.; Bretthauer, M.; Kalager, M. Benefits and harms of mammography screening. Breast Cancer Res. 2015, 17, 63. [Google Scholar] [CrossRef]
- Jørgensen, K.J.; Bewley, S.; Jatoi, I.; Lauby-Secretan, B.; Loomis, D.; Straif, K.; Fitzgerald, S.P. Breast-Cancer Screening—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2015, 373, 1478–1479. [Google Scholar] [CrossRef]
- De González, A.B.; Reeves, G. Mammographic screening before age 50 years in the UK: Comparison of the radiation risks with the mortality benefits. Br. J. Cancer 2005, 93, 590–596. [Google Scholar] [CrossRef][Green Version]
- Distante, V.; Frigerio, A.; Naldoni, C.; Paci, E.; Ponti, A. On the opportunity of extending service screening by mammography to women of 40–49 and 70–74 years of age. Epidemiol. Prev. 2007, 31, 15–22. [Google Scholar]
- Gajdos, C.; Tartter, P.I.; Bleiweiss, I.J.; Hermann, G.; De Csepel, J.; Estabrook, A.; Rademaker, A.W. Mammographic Appearance of Nonpalpable Breast Cancer Reflects Pathologic Characteristics. Ann. Surg. 2002, 235, 246–251. [Google Scholar] [CrossRef]
- Sickles, E.A.; D’Orsi, C.J.; Bassett, L.W.; Appleton, M.C.; Berg, W.A.; Burnside, E.S.; Feig, S.A.; Gavenonis, S.C.; Newell, M.S.; Trinh, M.M. ACR BI-RADS® Mammography. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Bluekens, A.M.J.; Holland, R.; Karssemeijer, N.; Broeders, M.J.M.; Heeten, G.J.D. Comparison of Digital Screening Mammography and Screen-Film Mammography in the Early Detection of Clinically Relevant Cancers: A Multicenter Study. Radiology 2012, 265, 707–714. [Google Scholar] [CrossRef]
- Burnside, E.S.; Ochsner, J.E.; Fowler, K.J.; Fine, J.P.; Salkowski, L.R.; Rubin, D.L.; Sisney, G.A. Use of Microcalcification Descriptors in BI-RADS 4th Edition to Stratify Risk of Malignancy. Radiology 2007, 242, 388–395. [Google Scholar] [CrossRef]
- van Luijt, P.A.; Fracheboud, J.; Heijnsdijk, E.A.; Heeten, G.J.D.; de Koning, H.J. Nation-wide data on screening performance during the transition to digital mammography: Observations in 6 million screens. Eur. J. Cancer 2013, 49, 3517–3525. [Google Scholar] [CrossRef]
- Rosenberg, R.D.; Yankaskas, B.C.; Abraham, L.A.; Sickles, E.A.; Lehman, C.D.; Geller, B.M.; Carney, P.A.; Kerlikowske, K.; Buist, D.S.M.; Weaver, D.L.; et al. Performance Benchmarks for Screening Mammography. Radiology 2006, 241, 55–66. [Google Scholar] [CrossRef]
- Tagliafico, A.S.; Valdora, F.; Mariscotti, G.; Durando, M.; Nori, J.; La Forgia, D.; Rosenberg, I.; Caumo, F.; Gandolfo, N.; Houssami, N.; et al. An exploratory radiomics analysis on digital breast tomosynthesis in women with mammographically negative dense breasts. Breast 2018, 40, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Sakai, A.; Onishi, Y.; Matsui, M.; Adachi, H.; Teramoto, A.; Saito, K.; Fujita, H. A method for the automated classification of benign and malignant masses on digital breast tomosynthesis images using machine learning and radiomic features. Radiol. Phys. Technol. 2020, 13, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Son, J.; Lee, S.E.; Kim, E.-K.; Kim, S. Prediction of breast cancer molecular subtypes using radiomics signatures of synthetic mammography from digital breast tomosynthesis. Sci. Rep. 2020, 10, 21566. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Zhao, Y.; Ji, Y.; Guo, X.; Jian, X.; Liu, P.; Wu, S. Breast Cancer Molecular Subtype Prediction by Mammographic Radiomic Features. Acad. Radiol. 2019, 26, 196–201. [Google Scholar] [CrossRef]
- Zhou, J.; Tan, H.; Bai, Y.; Li, J.; Lu, Q.; Chen, R.; Zhang, M.; Feng, Q.; Wang, M. Evaluating the HER-2 status of breast cancer using mammography radiomics features. Eur. J. Radiol. 2019, 121, 108718. [Google Scholar] [CrossRef]
- Lei, C.; Wei, W.; Liu, Z.; Xiong, Q.; Yang, C.; Yang, M.; Zhang, L.; Zhu, T.; Zhuang, X.; Liu, C.; et al. Mammography-based radiomic analysis for predicting benign BI-RADS category 4 calcifications. Eur. J. Radiol. 2019, 121, 108711. [Google Scholar] [CrossRef]
- Chen, S.; Guan, X.; Shu, Z.; Li, Y.; Cao, W.; Dong, F.; Zhang, M.; Shao, G.; Shao, F. A New Application of Multimodality Radiomics Improves Diagnostic Accuracy of Nonpalpable Breast Lesions in Patients with Microcalcifications-Only in Mammography. Med. Sci. Monit. 2019, 25, 9786–9793. [Google Scholar] [CrossRef]
- Lindfors, K.K.; Boone, J.M.; Nelson, T.R.; Yang, K.; Kwan, A.L.C.; Miller, D.F. Dedicated Breast CT: Initial Clinical Experience. Radiology 2008, 246, 725–733. [Google Scholar] [CrossRef]
- Chaimeleon. Available online: https://chaimeleon.eu/ (accessed on 18 April 2021).
- EuCanImage. Available online: https://eucanimage.eu/ (accessed on 18 April 2021).
- Perry, N.; Broeders, M.; de Wolf, C.; Törnberg, S.; Holland, R.; von Karsa, L. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition—summary document. Ann. Oncol. 2008, 19, 614–622. [Google Scholar] [CrossRef]
- Gisma. Available online: https://www.gisma.it/documenti/documenti_gisma/percorso-diagnostico-preoperatorio-GISMA-B3.pdf (accessed on 18 April 2021).
- Rageth, C.J.; O’Flynn, E.A.M.; Pinker-Domenig, K.; Kubik-Huch, R.A.; Mundinger, A.; Decker, T.; Tausch, C.; Dammann, F.; Baltzer, P.A.; Fallenberg, E.M.; et al. Second International Consensus Conference on lesions of uncertain malignant potential in the breast (B3 lesions). Breast Cancer Res. Treat. 2019, 174, 279–296. [Google Scholar] [CrossRef]
- Senonetwork. Available online: https://www.senonetwork.it/it/raccomandazioni/1-3798-1- (accessed on 18 April 2021).
- Pyradiomics. Available online: https://pyradiomics.readthedocs.io/en/latest/features.html (accessed on 18 April 2021).
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Tixier, F.; Le Rest, C.C.; Hatt, M.; Albarghach, N.; Pradier, O.; Metges, J.-P.; Corcos, L.; Visvikis, D. Intratumor Heterogeneity Characterized by Textural Features on Baseline 18F-FDG PET Images Predicts Response to Concomitant Radiochemotherapy in Esophageal Cancer. J. Nucl. Med. 2011, 52, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Yip, S.S.F.; Aerts, H.J.W.L. Applications and limitations of radiomics. Phys. Med. Biol. 2016, 61, R150–R166. [Google Scholar] [CrossRef]
- Leijenaar, R.T.; Nalbantov, G.; Carvalho, S.; Van Elmpt, W.J.; Troost, E.G.; Boellaard, R.; Aerts, H.J.; Gillies, R.J.; Lambin, P. The effect of SUV discretization in quantitative FDG-PET Radiomics: The need for standardized methodology in tumor texture analysis. Sci. Rep. 2015, 5, 11075. [Google Scholar] [CrossRef] [PubMed]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. JMLR 2011, 12, 2825–1830. [Google Scholar]
- Moons, K.G.M.; Kengne, A.P.; Woodward, M.; Royston, P.; Vergouwe, Y.; Altman, D.G.; Grobbee, D.E. Risk prediction models: I. Development, internal validation, and assessing the incremental value of a new (bio)marker. Heart 2012, 98, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis, 2nd ed.; Springer International Publishing: Cham, Switzeland, 2015. [Google Scholar]
- The Royal College of Pathologist. Available online: https://www.rcpath.org/uploads/assets/4b16f19c-f7bd-456c-b212f557f8040f66/G150-Non-op-reporting-breast-cancer-screening.pdf (accessed on 10 October 2021).
- Holland, R.; Stekhoven, J.S.; Hendriks, J.; Verbeek, A.; Mravunac, M. Extent, distribution, and mammographic/ histological correlations of breast ductal carcinoma in situ. Lancet 1990, 335, 519–522. [Google Scholar] [CrossRef]
- Berger, N.; Schwizer, S.D.; Varga, Z.; Rageth, C.J.; Frauenfelder, T.; Boss, A. Assessment of the extent of microcalcifications to predict the size of a ductal carcinoma in situ: Comparison between tomosynthesis and conventional mammography. Clin. Imaging 2016, 40, 1269–1273. [Google Scholar] [CrossRef]
- Pathology Reporting of Breast Disease. Published by the NHS Cancer Screening Programmes Jointly with The Royal College of Pathologists. Available online: www.rcpath.org (accessed on 16 July 2021).
- Britt, K.L.; Cuzick, J.; Phillips, K.-A. Key steps for effective breast cancer prevention. Nat. Cancer 2020, 20, 417–436. [Google Scholar] [CrossRef]
- Pinker, K. Beyond Breast Density: Radiomic Phenotypes Enhance Assessment of Breast Cancer Risk. Radiology 2019, 290, 50–51. [Google Scholar] [CrossRef]
- Kontos, D.; Winham, S.J.; Oustimov, A.; Pantalone, L.; Hsieh, M.-K.; Gastounioti, A.; Whaley, D.H.; Hruska, C.B.; Kerlikowske, K.; Brandt, K.; et al. Radiomic Phenotypes of Mammographic Parenchymal Complexity: Toward Augmenting Breast Density in Breast Cancer Risk Assessment. Radiology 2019, 290, 41–49. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DBT-VABB Histopathologic Reports | |||
|---|---|---|---|
| B2 | B3 | B5a | B5b |
| 126 | 45 | 63 | 18 |
| Total 126 | Total 126 | ||
| Follow up | Surgical Excision | ||
| Classification Methods | Sensitivity | Specificity | Accuracy | AUC |
|---|---|---|---|---|
| Linear support vector classifier | 0.53 [0.50–0.56] | 0.45 [0.42–0.48] | 0.48 [0.46–0.50] | 0.49 [0.48–0.50] |
| Radial basis function support vector classifier | 0.57 [0.55–0.59] | 0.55 [0.53–0.57] | 0.56 [0.54–0.57] | 0.56 [0.55–0.57] |
| Logistic regression | 0.45 [0.41–0.49] | 0.50 [0.46–0.55] | 0.46 [0.45–0.48] | 0.48 [0.46–0.49] |
| Random forest | 0.56 [0.54–0.58] | 0.61 [0.59–0.63] | 0.58 [0.57–0.59] | 0.59 [0.57–0.60] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Favati, B.; Borgheresi, R.; Giannelli, M.; Marini, C.; Vani, V.; Marfisi, D.; Linsalata, S.; Moretti, M.; Mazzotta, D.; Neri, E. Radiomic Applications on Digital Breast Tomosynthesis of BI-RADS Category 4 Calcifications Sent for Vacuum-Assisted Breast Biopsy. Diagnostics 2022, 12, 771. https://doi.org/10.3390/diagnostics12040771
Favati B, Borgheresi R, Giannelli M, Marini C, Vani V, Marfisi D, Linsalata S, Moretti M, Mazzotta D, Neri E. Radiomic Applications on Digital Breast Tomosynthesis of BI-RADS Category 4 Calcifications Sent for Vacuum-Assisted Breast Biopsy. Diagnostics. 2022; 12(4):771. https://doi.org/10.3390/diagnostics12040771
Chicago/Turabian StyleFavati, Benedetta, Rita Borgheresi, Marco Giannelli, Carolina Marini, Vanina Vani, Daniela Marfisi, Stefania Linsalata, Monica Moretti, Dionisia Mazzotta, and Emanuele Neri. 2022. "Radiomic Applications on Digital Breast Tomosynthesis of BI-RADS Category 4 Calcifications Sent for Vacuum-Assisted Breast Biopsy" Diagnostics 12, no. 4: 771. https://doi.org/10.3390/diagnostics12040771
APA StyleFavati, B., Borgheresi, R., Giannelli, M., Marini, C., Vani, V., Marfisi, D., Linsalata, S., Moretti, M., Mazzotta, D., & Neri, E. (2022). Radiomic Applications on Digital Breast Tomosynthesis of BI-RADS Category 4 Calcifications Sent for Vacuum-Assisted Breast Biopsy. Diagnostics, 12(4), 771. https://doi.org/10.3390/diagnostics12040771