
The Effect of Varying Interval Definitions on the Prevalence of SARS-CoV-2 Reinfections: A Retrospective Cross-Sectional Cohort Study


Abstract
:1. Introduction
2. Methods
2.1. Setting, Study Design and Participants
2.2. Assays
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gousseff, M.; Penot, P.; Gallay, L.; Batisse, D.; Benech, N.; Bouiller, K.; Collarino, R.; Conrad, A.; Slama, D.; Joseph, C.; et al. Clinical recurrences of COVID-19 symptoms after recovery: Viral relapse, reinfection or inflammatory rebound? J. Infect. 2020, 81, 816–846. [Google Scholar] [CrossRef] [PubMed]
- Dao, T.L.; Hoang, V.T.; Gautret, P. Recurrence of SARS-CoV-2 viral RNA in recovered COVID-19 patients: A narrative review. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Overbaugh, J. Understanding protection from SARS-CoV-2 by studying reinfection. Nat Med. 2020, 26, 1680–1681. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Hung, I.F.; Ip, J.D.; Chu, A.W.; Chan, W.M.; Tam, A.R.; Fong, C.H.; Yuan, S.; Tsoi, H.W.; Ng, A.C.; et al. Coronavirus Disease 2019 (COVID-19) Re-infection by a Phylogenetically Distinct Severe Acute Respiratory Syndrome Coronavirus 2 Strain Confirmed by Whole Genome Sequencing. Clin. Infect. Dis. 2021, 73, e2946–e2951. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Bhoyar, R.C.; Jain, A.; Srivastava, S.; Upadhayay, R.; Imran, M.; Jolly, B.; Divakar, M.K.; Sharma, D.; Sehgal, P.; et al. Asymptomatic Reinfection in 2 Healthcare Workers from India with Genetically Distinct Severe Acute Respiratory Syndrome Coronavirus 2. Clin. Infect. Dis. 2021, 73, e2823–e2825. [Google Scholar] [CrossRef] [PubMed]
- Tillett, R.L.; Sevinsky, J.R.; Hartley, P.D.; Kerwin, H.; Crawford, N.; Gorzalski, A.; Laverdure, C.; Verma, S.C.; Rossetto, C.C.; Jackson, R.D.; et al. Genomic evidence for reinfection with SARS-CoV-2: A case study. Lancet Infect. Dis. 2021, 21, 52–58. [Google Scholar] [CrossRef]
- Sciscent, B.Y.; Eisele, C.D.; Ho, L.; King, S.D.; Jain, R.; Golamari, R.R. COVID-19 reinfection: The role of natural immunity, vaccines, and variants. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Okhuese, A.V. Estimation of the Probability of Reinfection With COVID-19 by the Susceptible-Exposed-Infectious-Removed-Undetectable-Susceptible Model. JMIR Public Health Surveill. 2020, 6, e19097. [Google Scholar] [CrossRef] [PubMed]
- Malkov, E. Simulation of coronavirus disease 2019 (COVID-19) scenarios with possibility of reinfection. Chaos Solitons Fractals 2020, 139, 110296. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Brito, A.F.; Trubin, P.; Lu, P.; Wong, P.; Alpert, T.; Peña-Hernández, M.A.; Haynes, W.; Kamath, K.; Liu, F.; et al. Case Study: Longitudinal immune profiling of a SARS-CoV-2 reinfection in a solid organ transplant recipient. medRxiv 2021. [Google Scholar] [CrossRef]
- Perez, G.; Banon, T.; Gazit, S.; Moshe, S.; Wortsman, B.J.; Grupel, D.; Peretz, A.; Tov, A.B.; Chodick, G.; Mizrahi-Reuveni, M.; et al. A 1 to 1000 SARS-CoV-2 reinfection proportion in members of a large healthcare provider in Israel: A preliminary report. medRxiv 2021. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Coyle, P.; Malek, J.A.; Ahmed, A.A.; Mohamoud, Y.A.; Younuskunju, S.; Ayoub, H.H.; Kanaani, Z.A.; Kuwari, E.A.; et al. SARS-CoV-2 reinfection in a cohort of 43,000 antibody-positive individuals followed for up to 35 weeks. medRxiv 2021. [Google Scholar] [CrossRef]
- Murillo-Zamora, E.; Mendoza-Cano, O.; Delgado-Enciso, I.; Hernandez-Suarez, C.M. Predictors of severe symptomatic laboratory-confirmed SARS-CoV-2 reinfection. Public Health 2021, 193, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Rhoads, D.; Peaper, D.R.; She, R.C.; Nolte, F.S.; Wojewoda, C.M.; Anderson, N.W.; Pritt, B.S. College of American Pathologists (CAP) Microbiology Committee Perspective: Caution Must Be Used in Interpreting the Cycle Threshold (Ct) Value. Clin. Infect. Dis. 2021, 72, e685–e686. [Google Scholar] [CrossRef] [PubMed]
- Tomassini, S.; Kotecha, D.; Bird, P.W.; Folwell, A.; Biju, S.; Tang, J.W. Setting the criteria for SARS-CoV-2 reinfection - six possible cases. J. Infect. 2021, 82, 282–327. [Google Scholar] [CrossRef] [PubMed]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widders, A.; Broom, A.; Broom, J. SARS-CoV-2: The viral shedding vs infectivity dilemma. Infect. Dis. Health 2020, 25, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rijksinstituut Voor Volksgezondheid en Milieu. Varianten van Het Coronavirus SARS-CoV-2. Available online: https://www.rivm.nl/coronavirus-covid-19/virus/varianten (accessed on 1 October 2021).
- European Centre for Disease Prevention and Control. Surveillance Definitions for COVID-19. 15 March 2021. Stockholm: ECDC. 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/surveillance-definitions (accessed on 16 February 2022).
- Centers for Disease Control and Prevention. Investigative Criteria for Suspected Cases of SARS-CoV-2 Reinfection (ICR). Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/invest-criteria.html (accessed on 26 September 2021).
- Rijksinstituut voor Volksgezondheid en Milieu. COVID-19 Richtlijn. Available online: https://lci.rivm.nl/richtlijnen/covid-19 (accessed on 1 October 2021).
- Rijksoverheid. Coronavirus Tijdlijn. 2020. Available online: https://www.rijksoverheid.nl/onderwerpen/coronavirus-tijdlijn (accessed on 19 October 2021).


{kind=link}
{kind=link}
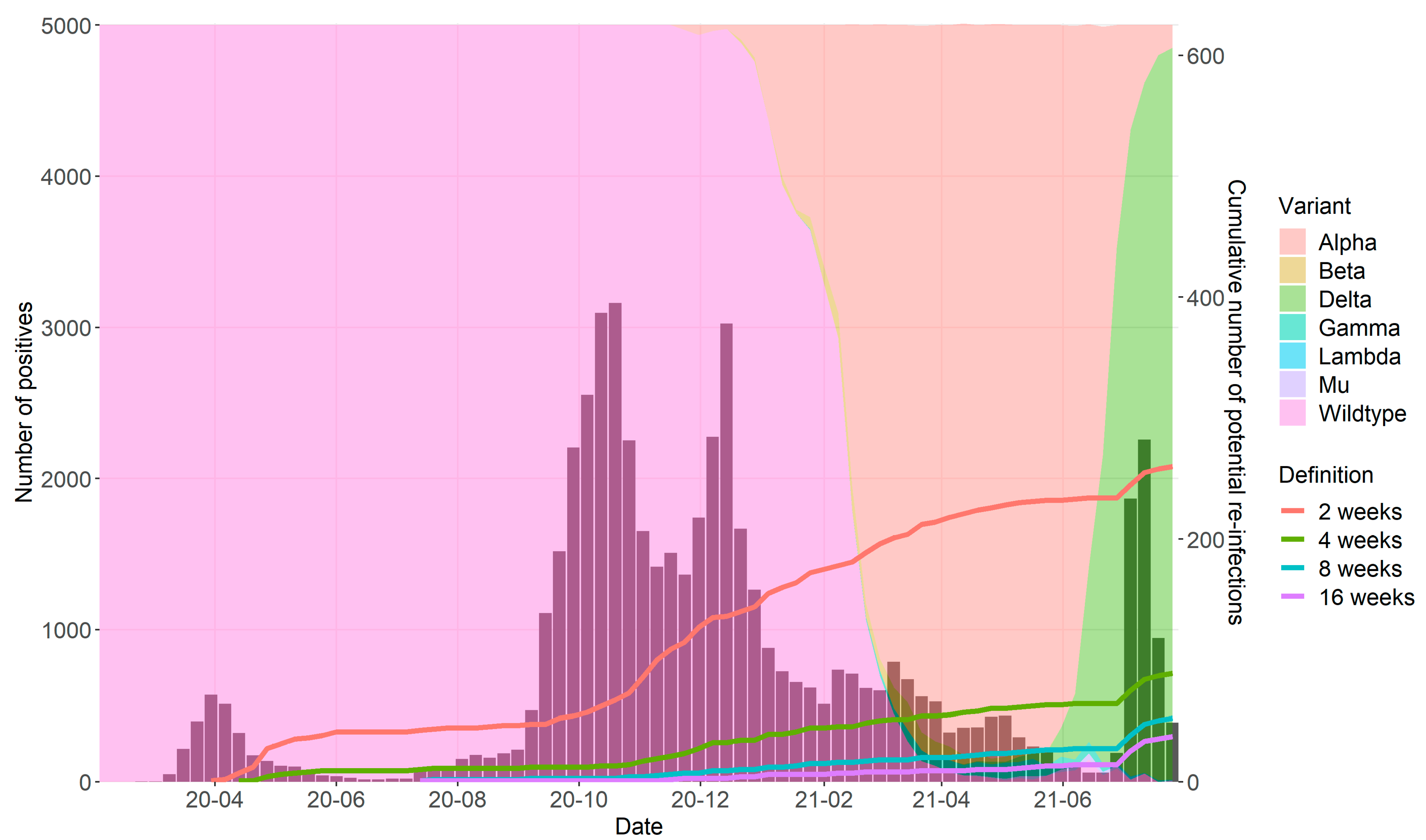
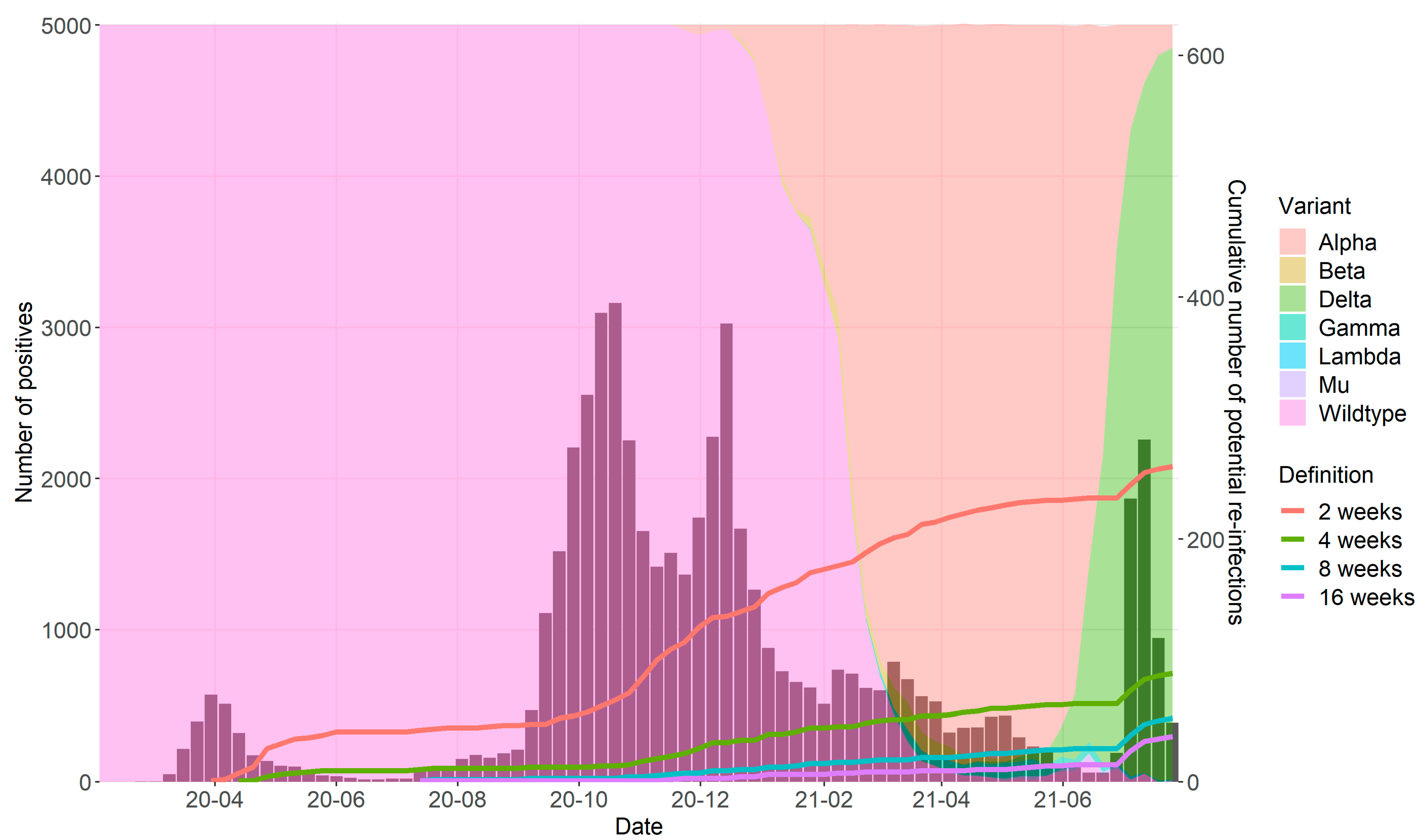
| Definition | Number of Reinfections (%) | Median Age [IQR] (Years) | Median Cp-Value [IQR] First Positive Test | Median Cp-Value [IQR] Second Positive Test |
|---|---|---|---|---|
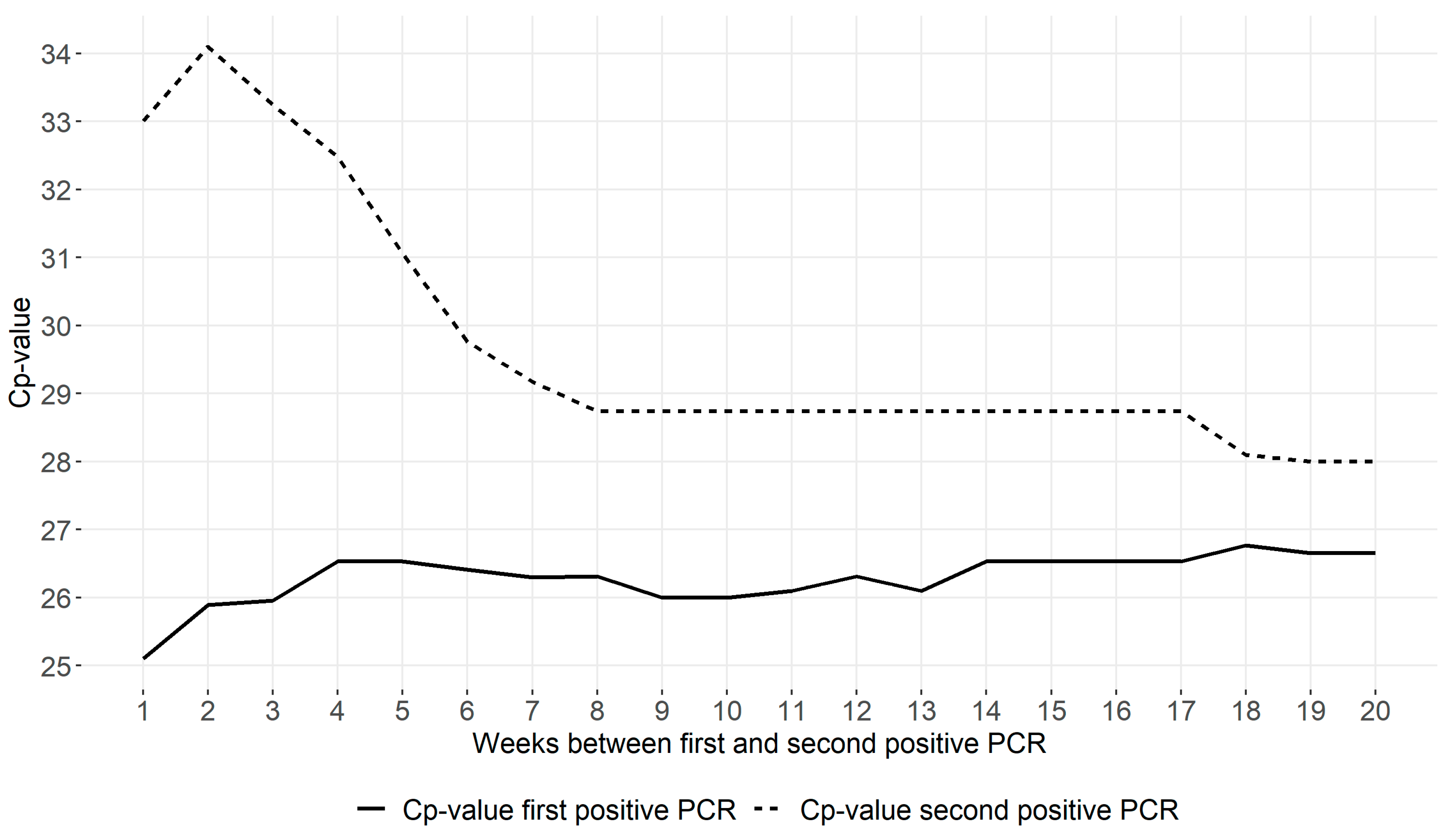
| 2 weeks | 260 (0.52%) | 69.0 [33.5] | 25.9 [7.5] | 34.1 [6.1] |
| 4 weeks | 89 (0.19%) | 53.0 [50.0] | 26.5 [8.5] | 32.5 [8.1] |
| 8 weeks | 52 (0.11%) | 30.0 [34.0] | 26.3 [8.8] | 28.7 [8.1] |
| 16 weeks | 37 (0.09%) | 24.0 [30.0] | 26.5 [8.8] | 28.7 [6.5] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Euser, S.M.; Weenink, T.; Prins, J.M.; Haverkort, M.; Manders, I.; van Lelyveld, S.; Herpers, B.L.; Sinnige, J.; Kalpoe, J.; Snijders, D.; et al. The Effect of Varying Interval Definitions on the Prevalence of SARS-CoV-2 Reinfections: A Retrospective Cross-Sectional Cohort Study. Diagnostics 2022, 12, 719. https://doi.org/10.3390/diagnostics12030719
Euser SM, Weenink T, Prins JM, Haverkort M, Manders I, van Lelyveld S, Herpers BL, Sinnige J, Kalpoe J, Snijders D, et al. The Effect of Varying Interval Definitions on the Prevalence of SARS-CoV-2 Reinfections: A Retrospective Cross-Sectional Cohort Study. Diagnostics. 2022; 12(3):719. https://doi.org/10.3390/diagnostics12030719
Chicago/Turabian StyleEuser, Sjoerd M., Tieme Weenink, Jan M. Prins, Milly Haverkort, Irene Manders, Steven van Lelyveld, Bjorn L. Herpers, Jan Sinnige, Jayant Kalpoe, Dominic Snijders, and et al. 2022. "The Effect of Varying Interval Definitions on the Prevalence of SARS-CoV-2 Reinfections: A Retrospective Cross-Sectional Cohort Study" Diagnostics 12, no. 3: 719. https://doi.org/10.3390/diagnostics12030719
APA StyleEuser, S. M., Weenink, T., Prins, J. M., Haverkort, M., Manders, I., van Lelyveld, S., Herpers, B. L., Sinnige, J., Kalpoe, J., Snijders, D., Cohen Stuart, J., Slijkerman Megelink, F., Kapteijns, E., den Boer, J., Wagemakers, A., & Souverein, D. (2022). The Effect of Varying Interval Definitions on the Prevalence of SARS-CoV-2 Reinfections: A Retrospective Cross-Sectional Cohort Study. Diagnostics, 12(3), 719. https://doi.org/10.3390/diagnostics12030719