
Factors Associated with Delirium in COVID-19 Patients and Their Outcome: A Single-Center Cohort Study


 ,
,  ,
,  , ,
, ,  , ,
, ,  on behalf of the CSS-COVID-19 Group
on behalf of the CSS-COVID-19 Group
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Sample
2.2. Patient and Public Involvement
2.3. Data Collection
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Wilson, J.E.; Mart, M.F.; Cunningham, C.; Shehabi, Y.; Girard, T.D.; MacLullich, A.M.J.; Slooter, A.J.C.; Ely, E.W. Delirium. Nat. Rev. Dis. Primers 2020, 6, 90, Erratum in Nat. Rev. Dis. Primers 2020, 6, 94. [Google Scholar] [CrossRef] [PubMed]
- D’Ardes, D.; Carrarini, C.; Russo, M.; Dono, F.; Speranza, R.; Digiovanni, A.; Martinotti, G.; Di Iorio, A.; Onofrj, M.; Cipollone, F.; et al. Low molecular weight heparin in COVID-19 patients prevents delirium and shortens hospitalization. Neurol. Sci. 2021, 42, 1527–1530. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with com- parison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Shao, S.C.; Lai, C.C.; Chen, Y.H.; Chen, Y.C.; Hung, M.J.; Liao, S.C. Prevalence, incidence and mortality of delirium in patients with COVID-19: A systematic review and meta-analysis. Age Ageing 2021, 50, 1445–1453. [Google Scholar] [CrossRef]
- Pun, B.T.; Badenes, R.; Heras La Calle, G.; Orun, O.M.; Chen, W.; Raman, R.; Simpson, B.K.; Wilson-Linville, S.; Hinojal Olmedillo, B.; de la Cueva, A.V.; et al. COVID-19 Intensive Care International Study Group. Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): A multicentre cohort study. Lancet Respir. Med. 2021, 9, 239–250. [Google Scholar] [CrossRef]
- Lou, B.; Guo, J.; Liu, Y.; Xiong, C.; Shi, J.; Zhou, C. Prevalence, classification, risk factors and outcome impact of delirium in patients with COVID-19: A meta-analysis protocol for systematic review. BMJ Open 2021, 11, e048323. [Google Scholar] [CrossRef]
- O’Hanlon, S.; Inouye, S.K. Delirium: A missing piece in the COVID-19 pandemic puzzle. Age Ageing 2020, 49, 497–498. [Google Scholar] [CrossRef]
- Vabret, N.; Britton, G.J.; Gruber, C.; Hegde, S.; Kim, J.; Kuksin, M.; Levantovsky, R.; Malle, L.; Moreira, A.; Park, M.D.; et al. Sinai Immunology Review Project. Immunology of COVID-19: Current State of the Science. Immunity 2020, 52, 910–941. [Google Scholar] [CrossRef]
- Mirijello, A.; Zarrelli, M.; Miscio, G.; de Matthaeis, A.; Piscitelli, P.; Carbonelli, C.M.; Di Giorgio, A.; Inglese, M.; Ciliberti, G.L.; Marciano, C.; et al. Diagnosis of COVID-19 in Patients with Negative Nasopharyngeal Swabs: Reliability of Radiological and Clinical Diagnosis and Accuracy Versus Serology. Diagnostics 2021, 11, 386. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Bellelli, G.; Morandi, A.; Davis, D.H.; Mazzola, P.; Turco, R.; Gentile, S.; Ryan, T.; Cash, H.; Guerini, F.; Torpilliesi, T.; et al. Validation of the 4AT, a new instrument for rapid delirium screening: A study in 234 hospitalised older people. Age Ageing 2014, 43, 496–502, Erratum in Age Ageing 2015, 44, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipowski, Z.J. Delirium: Acute Confusional States; Oxford University Press: New York, NY, USA, 1990. [Google Scholar]
- Hawkins, M.; Sockalingam, S.; Bonato, S.; Rajaratnam, T.; Ravindran, M.; Gosse, P.; Sheehan, K.A. A rapid review of the pathoetiology, presentation, and management of delirium in adults with COVID-19. J. Psychosom. Res. 2021, 141, 110350. [Google Scholar] [CrossRef] [PubMed]
- Slooter, A.J.C.; Otte, W.M.; Devlin, J.W.; Arora, R.C.; Bleck, T.P.; Claassen, J.; Duprey, M.S.; Ely, E.W.; Kaplan, P.W.; Latronico, N.; et al. Updated nomenclature of delirium and acute encephalopathy: Statement of ten Societies. Intensive Care Med. 2020, 46, 1020–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilotto, A.; Benussi, A.; Libri, I.; Masciocchi, S.; Poli, L.; Premi, E.; Alberici, A.; Baldelli, E.; Bonacina, S.; Brambilla, L.; et al. COVID-19 impact on consecutive neurological patients admitted to the emergency department. J. Neurol. Neurosurg. Psychiatry 2021, 92, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Benussi, A.; Pilotto, A.; Premi, E.; Libri, I.; Giunta, M.; Agosti, C.; Alberici, A.; Baldelli, E.; Benini, M.; Bonacina, S.; et al. Clinical characteristics and outcomes of inpatients with neurologic disease and COVID-19 in Brescia, Lombardy, Italy. Neurology 2020, 95, e910–e920. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, H.; Zhang, Z.; Liang, W.; Zhang, T.; Tong, Z.; Guo, X.; Qi, X. Risk factors for mortality of coronavirus disease 2019 (COVID-19) patients during the early outbreak of COVID-19: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 5069–5083. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Huang, I.; Lim, M.A.; Yonas, E.; Vania, R.; Kuswardhani, R.A.T. Delirium and Mortality in Coronavirus Disease 2019 (COVID-19)—A Systematic Review and Meta-analysis. Arch. Gerontol. Geriatr. 2021, 95, 104388. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. ISARIC4C investigators. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Ali, N. Elevated level of C-reactive protein may be an early marker to predict risk for severity of COVID-19. J. Med. Virol. 2020, 92, 2409–2411. [Google Scholar] [CrossRef]
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-lymphocyte ratio on admission to predict the sever- ity and mortality of COVID-19 patients: A meta-analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.; Helfand, B.K.I.; Gou, R.Y.; Gartaganis, S.L.; Webb, M.; Moccia, J.M.; Bruursema, S.N.; Dokic, B.; McCulloch, B.; Ring, H.; et al. Delirium in Older Patients With COVID-19 Presenting to the Emergency Department. JAMA Netw. Open 2020, 3, e2029540. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, A.; Adamis, D.; Treolar, A.; Martin, F. C-reactive protein levels predict incidence of and recovery from delirium. Age Ageing 2007, 36, 222–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasunilashorn, S.M.; Dillon, S.T.; Inouye, S.K.; Ngo, L.H.; Fong, T.G.; Jones, R.N.; Travison, T.G.; Schmitt, E.M.; Alsop, D.C.; Freedman, S.D.; et al. High C-Reactive Protein Predicts Delirium Incidence, Duration, and Feature Severity After Major Non-cardiac Surgery. J. Am. Geriatr. Soc. 2017, 65, e109–e116. [Google Scholar] [CrossRef]
- Dillon, S.T.; Vasunilashorn, S.M.; Ngo, L.; Otu, H.H.; Inouye, S.K.; Jones, R.N.; Alsop, D.C.; Kuchel, G.A.; Metzger, E.D.; Arnold, S.E.; et al. Higher C-Reactive Protein Levels Predict Postoperative Delirium in Older Patients Undergoing Major Elective Sur- gery: A Longitudinal Nested Case-Control Study. Biol. Psychiatry 2017, 81, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Saini, A.; Oh, T.H.; Ghanem, D.A.; Castro, M.; Butler, M.; Sin Fai Lam, C.C.; Posporelis, S.; Lewis, G.; David, A.S.; Rogers, J.P. Inflammatory and blood gas markers of COVID-19 delirium compared to non-COVID-19 delirium: A cross-sectional study. Aging Ment. Health 2021, 1–8. [Google Scholar] [CrossRef]
- Kealy, J.; Murray, C.; Griffin, E.W.; Lopez-Rodriguez, A.B.; Healy, D.; Tortorelli, L.S.; Lowry, J.P.; Watne, L.O.; Cunningham, C. Acute Inflammation Alters Brain Energy Metabolism in Mice and Humans: Role in Suppressed Spontaneous Activity, Impaired Cognition, and Delirium. J. Neurosci. 2020, 40, 5681–5696. [Google Scholar] [CrossRef]
- Tremblay, M.E.; Madore, C.; Bordeleau, M.; Tian, L.; Verkhratsky, A. Neuropathobiology of COVID-19: The Role for Glia. Front. Cell. Neurosci. 2020, 14, 592214. [Google Scholar] [CrossRef]
- Boldrini, M.; Canoll, P.D.; Klein, R.S. How COVID-19 Affects the Brain. JAMA Psychiatry 2021, 78, 682–683. [Google Scholar] [CrossRef]
- Khan, B.A.; Perkins, A.J.; Prasad, N.K.; Shekhar, A.; Campbell, N.L.; Gao, S.; Wang, S.; Khan, S.H.; Marcantonio, E.R.; Twigg, H.L., 3rd; et al. Biomarkers of Delirium Duration and Delirium Severity in the ICU. Crit. Care Med. 2020, 48, 353–361. [Google Scholar] [CrossRef]


{kind=link}
| Total (N = 214) | Without Delirium (N = 168) | With Delirium (N = 46) | |
|---|---|---|---|
| Age at admission: mean (SD) | 67.88 (15.05) | 64.32 (14.43) | 80.89 (8.89) |
| Age class (N, %) | |||
| <50 | 29 (13.6%) | 29 (17.3%) | 0 (0.0%) |
| 50–59 | 32 (15.0%) | 31 (18.5%) | 1 (2.2%) |
| 60–69 | 44 (20.6%) | 40 (23.8%) | 4 (8.7%) |
| 70–79 | 59 (27.6%) | 43 (25.6%) | 16 (34.8%) |
| ≥80 | 50 (23.4%) | 25 (14.9%) | 25 (54.3%) |
| Male gender (N, %) | 118 (55.1%) | 97 (57.7%) | 21 (45.7%) |
| Education (years) | |||
| ≤5 | 88 (41.5%) | 55 (33.1%) | 33 (71.7%) |
| 6–8 | 55 (25.9%) | 48 (28.9%) | 7 (15.2%) |
| >8 | 69 (32.5%) | 63 (38.0%) | 6 (13.0%) |
| Smokers (N, %) | 44 (27.2%) | 40 (30.5%) | 4 (12.9%) |
| BMI: mean (SD) | 26.97 (4.62) | 26.98 (4.59) | 26.89 (4.84) |
| Glasgow Coma Scale mean (SD) | 14.45 (2.06) | 14.71 (1.64) | 13.47 (3.00) |
| Fever at admission (N, %) | 154 (72.0%) | 128 (76.2%) | 26 (56.5%) |
| Comorbidity at admission (N, %) | |||
| Dementia | 33 (15.5%) | 9 (5.4%) | 24 (52.2%) |
| Chronic obstructive pulmonary disease | 23 (10.7%) | 17 (10.1%) | 6 (13.0%) |
| Diabetes | 40 (18.7%) | 27 (16.1%) | 13 (28.3%) |
| Atrial fibrillation | 29 (13.6%) | 21 (12.5%) | 8 (17.4%) |
| Arterial hypertension | 103 (48.1%) | 77 (45.8%) | 26 (56.5%) |
| Hypercholesterolemia | 17 (7.9%) | 16 (9.5%) | 1 (2.2%) |
| Tumor | 40 (18.7%) | 33 (19.6%) | 7 (15.2%) |
| Thyreopathy | 17 (7.9%) | 14 (8.3%) | 3 (6.5%) |
| Hypertriglyceridemia | 7 (3.3%) | 5 (3.0%) | 2 (4.3%) |
| Others | 140 (65.4%) | 99 (58.9%) | 41 (89.1%) |
| Charlson Index (without dementia) mean (SD) | 3.58 (2.40) | 3.15 (2.38) | 5.15 (1.71) |
| Use of psychotropic drugs (N, %) | 27 (12.6%) | 14 (8.3%) | 13 (28.3%) |
| Total (N = 214) ‡ | Without Delirium (N = 168) ‡ | With Delirium (N = 46) ‡ | |
|---|---|---|---|
| Red blood cells (RBC) millions/mcl | 4.58 (3.97, 5.09) | 4.68 (4.13, 5.14) | 4.09 (3.70, 4.83) |
| Hematocrit % | 40.25 (35.02, 43.98) | 40.80 (36.02, 44.08) | 36.25 (32.95, 42.95) |
| Hemoglobin g/dL | 13.30 (11.40, 14.50) | 13.40 (11.90, 14.70) | 11.80 (10.78, 13.72) |
| Mean corpuscular volume (MCV) fl | 87.80 (84.68, 91.12) | 87.30 (83.97, 91.03) | 89.20 (86.45, 91.82) |
| White blood cells (WBC) thousand/mcl | 6.39 (4.60, 9.04) | 5.92 (4.34, 8.10) | 8.29 (5.54, 11.18) |
| Neutrophils thousand/mcl | 4.54 (3.04, 7.68) | 4.19 (2.89, 6.39) | 6.61 (4.28, 9.27) |
| Lymphocytes thousand/mcl | 1.02 (0.73, 1.45) | 1.02 (0.77, 1.46) | 1.06 (0.68, 1.42) |
| Neutrophils-to-lymphocytes ratio (NLR) | 4.18 (2.52, 7.41) | 3.84 (2.40, 6.52) | 6.04 (3.19, 18.89) |
| Platelets thousand/mcl | 212.00 (159.25, 285.50) | 205.00 (153.25, 258.00) | 273.00 (197.50, 332.25) |
| International normalized ratio (INR) | 1.08 (1.04, 1.15) | 1.07 (1.03, 1.13) | 1.13 (1.06, 1.19) |
| Partial thromboplastin time (PTT) sec | 24.60 (22.90, 26.90) | 24.60 (22.90, 26.90) | 24.45 (22.10, 28.00) |
| Alkaline phosphatase UI/L | 74.00 (60.00, 101.50) | 71.00 (59.25, 96.75) | 85.00 (70.00, 121.00) |
| Total bilirubin mg/dL | 0.60 (0.40, 0.80) | 0.60 (0.40, 0.80) | 0.60 (0.40, 0.90) |
| Aspartate amino transferase (AST) UI/L | 33.00 (22.00, 48.00) | 33.00 (23.00, 48.00) | 32.00 (18.50, 47.50) |
| Alanine amino transferase (ALT) U/L | 30.00 (20.00, 48.00) | 32.50 (21.00, 51.00) | 24.00 (16.00, 38.00) |
| ɣ-glutamyl-transpeptidase (ɣ-GT) UI/L | 46.00 (22.75, 103.00) | 51.50 (23.00, 109.50) | 35.50 (17.25, 62.75) |
| Total proteins g/dL | 7.00 (6.40, 7.70) | 7.15 (6.50, 7.80) | 6.70 (6.10, 7.20) |
| Creatinine mg/dL | 0.90 (0.70, 1.10) | 0.80 (0.70, 1.10) | 1.10 (0.70, 1.60) |
| Estimated glomerular filtration rate (eGFR), mL/mn | 86.00 (58.00, 108.75) | 90.00 (66.75, 110.00) | 61.50 (33.50, 97.25) |
| Glycemia mg/dL | 106.50 (85.00, 135.00) | 104.50 (85.00, 127.75) | 120.50 (92.00, 163.00) |
| Erythrocyte sedimentation rate (ESR) mm | 45.00 (30.00, 67.00) | 44.00 (29.75, 65.50) | 51.00 (42.00, 70.00) |
| Triglycerides mg/dL | 110.00 (88.50, 146.00) | 109.00 (84.00, 145.00) | 116.00 (106.25, 169.25) |
| Cholesterol mg/dL | 137.00 (111.50, 164.00) | 137.00 (112.00, 164.00) | 128.50 (105.00, 155.25) |
| Lactate-dehydrogenase (LDH) U/L | 243.00 (194.00, 318.50) | 250.50 (196.25, 326.75) | 227.00 (180.00, 287.00) |
| Creatine-phosphokinase CK U/L | 83.00 (46.00, 167.00) | 80.00 (50.00, 169.00) | 88.00 (36.00, 154.00) |
| Troponin pg/mL | 15.10 (8.00, 41.60) | 12.60 (7.40, 22.90) | 38.85 (16.12, 143.18) |
| D-dimer mg/mL | 764.00 (395.00, 2981.50) | 710.00 (393.50, 2136.25) | 2345.00 (505.00, 6021.00) |
| Procalcitonin µg/L | 0.14 (0.08, 0.31) | 0.12 (0.07, 0.27) | 0.23 (0.12, 0.42) |
| C-reactive protein (CRP) mg/dL | 4.93 (1.52, 11.05) | 3.59 (1.07, 9.04) | 10.70 5.73, 15.75) |
| Occurrence of Delirium | |||||
|---|---|---|---|---|---|
| Variable | N † | N Events ‡ | Hazard Ratio (95% Confidence Interval) | p-Value | p-Value Adjusted * |
| Age ^ | 214 | 46 | 1.11 (1.08–1.15) | 1.15 × 10−10 | 5.51 × 10−9 |
| Male gender | 214 | 46 | 0.67 (0.38–1.2) | 0.182434625 | 1 |
| Current/former smokers | 162 | 31 | 0.42 (0.15–1.21) | 0.107783665 | 1 |
| BMI ^ | 192 | 34 | 1.01 (1–1.02) | 0.041076706 | 1 |
| Glasgow Coma Scale ^ | 205 | 43 | 0.86 (0.79–0.93) | 0.00028387 | 0.013625766 |
| Fever | 214 | 46 | 0.43 (0.24–0.76) | 0.004144349 | 0.198928741 |
| Chronic obstructive pulmonary disease | 214 | 46 | 1.21 (0.51–2.87) | 6.60 × 10−1 | 1.00 |
| Diabetes | 214 | 46 | 1.99 (1.04–3.8) | 0.036791187 | 1 |
| Atrial fibrillation | 214 | 46 | 1.39 (0.65–2.97) | 0.402521663 | 1 |
| Arterial hypertension | 214 | 46 | 1.48 (0.83–2.66) | 0.184784901 | 1 |
| Hypercholesterolemia | 214 | 46 | 0.21 (0.03–1.54) | 0.125310853 | 1 |
| Neoplasia | 214 | 46 | 0.71 (0.32–1.59) | 0.401540797 | 1 |
| Thyreopathy | 214 | 46 | 0.91 (0.28–2.94) | 0.875627181 | 1 |
| Hypertriglyceridemia | 214 | 46 | 1.32 (0.32–5.47) | 0.705744187 | 1 |
| Other comorbidities | 214 | 46 | 5.32 (2.09–13.51) | 0.000439886 | 0.02111453 |
| Charlson Index (without dementia) ^ | 214 | 46 | 1.35 (1.2–1.53) | 6.39966 × 10−7 | 3.07184 × 10−5 |
| Use of psychotropic drugs | 214 | 46 | 3.58 (1.87–6.83) | 0.000112691 | 0.005409186 |
| Dementia | 213 | 46 | 11.21 (6.13–20.5) | 4.17 × 10−15 | 2.00 × 10−13 |
| Vit. D therapy | 214 | 46 | 4.28 (1.68–10.91) | 2.34 × 10−3 | 0.11250987 |
| Neutrophil/lymphocyte ratio § | 210 | 44 | 1.45 (1.21–1.73) | 4.87904 × 10−5 | 0.002341939 |
| Hematocrit § | 210 | 44 | 0.67 (0.43–1.03) | 0.067830978 | 1 |
| Hemoglobin § | 210 | 44 | 0.18 (0.05–0.69) | 0.012064584 | 0.579100049 |
| MCV § | 204 | 40 | 1.36 (0.88–2.1) | 0.160177209 | 1 |
| RBC § | 210 | 44 | 0.28 (0.01–9.86) | 0.480843162 | 1 |
| WBC § | 210 | 44 | 1.35 (1.02–1.79) | 0.03343282 | 1 |
| Neutrophils § | 210 | 44 | 1.11 (0.93–1.31) | 0.243821628 | 1 |
| Lymphocytes § | 210 | 44 | 0.22 (0.01–4.87) | 0.337755457 | 1 |
| Platelets § | 210 | 44 | 1.04 (1.01–1.07) | 0.002220278 | 0.106573321 |
| INR § | 194 | 38 | 6.74 (0.15–310.51) | 0.32861737 | 1 |
| PTT § | 194 | 38 | 1.13 (0.61–2.1) | 0.703355655 | 1 |
| ALT § | 205 | 43 | 0.95 (0.87–1.04) | 0.244626107 | 1 |
| Total bilirubin § | 202 | 41 | 2.81 (0.07–110.22) | 0.581749862 | 1 |
| Alkaline phosphatase § | 163 | 37 | 1.03 (0.98–1.08) | 0.23127989 | 1 |
| ɣ-GT § | 164 | 36 | 1 (0.97–1.03) | 0.820668706 | 1 |
| AST § | 205 | 43 | 0.97 (0.9–1.05) | 0.44704993 | 1 |
| Total proteins § | 203 | 41 | 0.03 (0–1.05) | 0.053086568 | 1 |
| Creatinine § | 206 | 43 | 1.05 (0.4–2.78) | 0.923433337 | 1 |
| e-GFR § | 202 | 42 | 0.9 (0.83–0.97) | 0.004767905 | 0.228859456 |
| Glycemia § | 204 | 42 | 1.06 (1.03–1.11) | 0.000990944 | 0.047565326 |
| ESR § | 149 | 25 | 1.1 (0.95–1.27) | 0.184748898 | 1 |
| Triglycerides § | 163 | 30 | 1.05 (0.99–1.11) | 0.11199928 | 1 |
| Cholesterol § | 163 | 30 | 0.97 (0.89–1.07) | 0.59449302 | 1 |
| LDH § | 155 | 31 | 0.99 (0.96–1.02) | 0.623247956 | 1 |
| CK § | 162 | 37 | 1 (0.99–1.02) | 0.856646053 | 1 |
| Troponin § | 101 | 24 | 1 (0.99–1.01) | 0.750801089 | 1 |
| D-dimer § | 119 | 25 | 1 (1–1) | 0.029007362 | 1 |
| Procalcitonin § | 118 | 24 | 1.75 (0.89–3.47) | 1.06 × 10−1 | 1 |
| CRP § | 207 | 43 | 2.26 (1.6–3.2) | 4.28496 × 10−6 | 0.000205678 |
| Occurrence of Delirium | ||
|---|---|---|
| Variable | Hazard Ratio (95% Confidence Interval) | p-Value |
| Age at admission ^ | 1.07 (1.03–1.11) | 0.0007 |
| Glasgow coma scale | 0.88 (0.8–0.98) | 0.0166 |
| Baseline CRP § | 1.06 (1.02–1.1) | 0.0015 |
| Dementia | 3.2 (1.38–7.38) | 0.0065 |
| Patients with Delirium (N = 46) | Patients without Delirium (N = 168) | p-Value | |
|---|---|---|---|
| Length of hospitalization (only survived patients days) (mean, SD) | 33.44 (12.63) | 24.64 (13.28) | Poisson model, p < 0.0001 |
| Admission to ICU (N, %) | 10/46 21.7% | 30/168 17.9% | Cox model Hazard Ratio = 1.26, p = 0.53 |
| Time to ICU admission (only patients admitted in ICU) days (mean, SD) | 10.60 (15.04) | 6.90 (7.40) | Poisson model, p < 0.0005 |
| Length of stay in ICU (only patients admitted in ICU) days (mean, SD) | 24.00 (4.24) | 24.00 (8.73) | Poisson model, p = 0.893 |
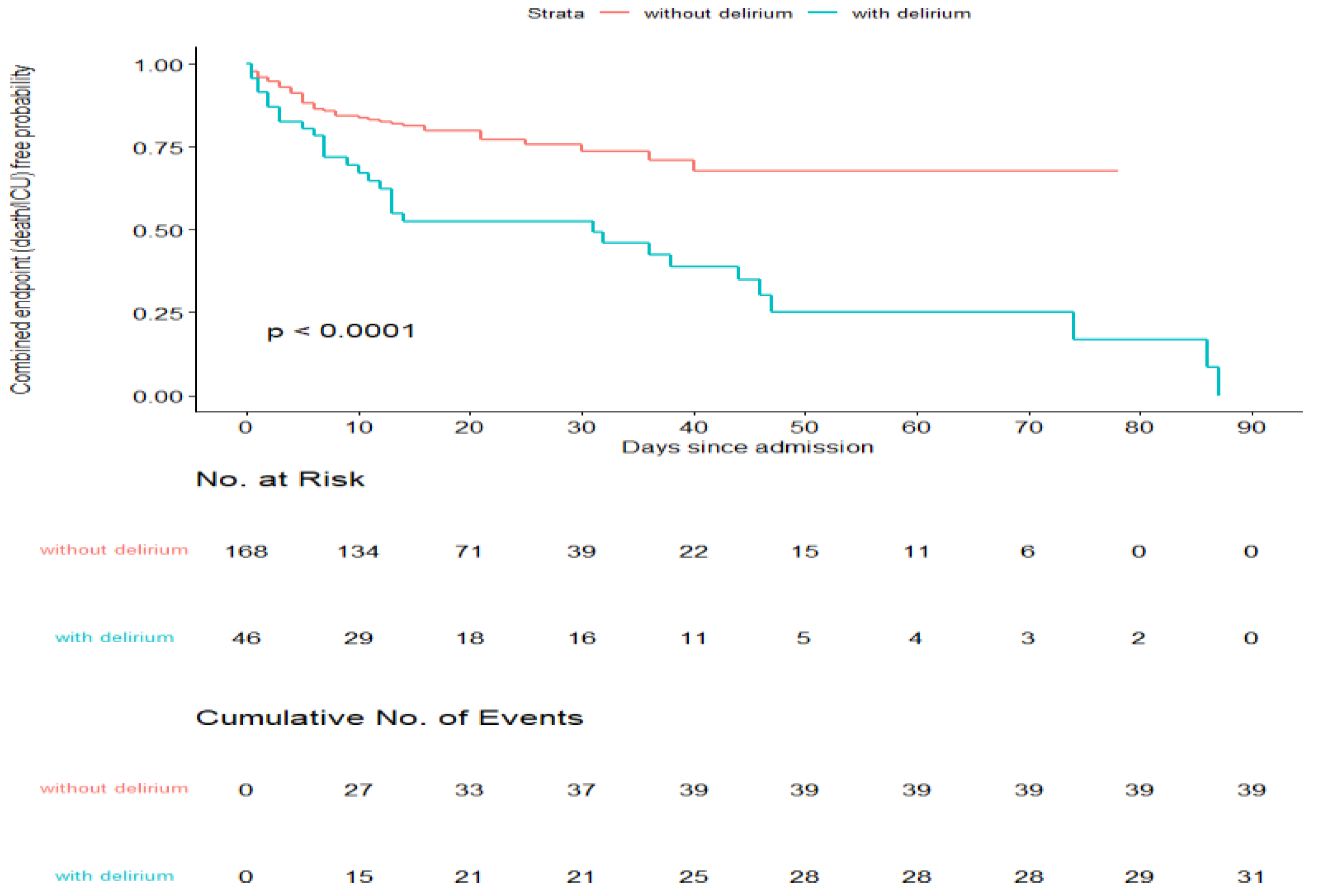
| In-hospital death (N, %) | 29/46 63.0% | 26/168 15.5% | Cox model Hazard Ratio = 8.27, p < 0.0001 |
| Combined Endpoint (Death/Admission to ICU) | |||||
|---|---|---|---|---|---|
| Variable | N † | N Events ‡ | Hazard Ratio (95% Confidence Interval) | p-Value | p-Value Adjusted * |
| Delirium (time dependent) | 214 | 70 | 5.12 (2.99–8.78) | 0.000000003 | 0.0000001 |
| Age at admission ^ | 214 | 70 | 1.05 (1.03–1.08) | 0.000000237 | 0.0000116 |
| Male gender | 214 | 70 | 1.05 (0.65–1.69) | 0.837643647 | 1.0000000 |
| Current/former smokers | 162 | 50 | 1.12 (0.59–2.13) | 0.722477102 | 1.0000000 |
| BMI ^ | 192 | 58 | 1.01 (1–1.01) | 0.121131099 | 1.0000000 |
| Glasgow Coma Scale ^ | 205 | 65 | 0.86 (0.8–0.93) | 0.000145628 | 0.0071358 |
| Fever | 214 | 70 | 0.69 (0.42–1.13) | 0.142083876 | 1.0000000 |
| Chronic Pulmonary Obstructive Disease | 214 | 70 | 2.15 (1.19–3.88) | 0.011525366 | 0.5647430 |
| Diabetes | 214 | 70 | 1.39 (0.8–2.41) | 0.246348210 | 1.0000000 |
| Atrial fibrillation | 214 | 70 | 1.65 (0.91–2.97) | 0.096134852 | 1.0000000 |
| Arterial hypertension | 214 | 70 | 1.7 (1.05–2.76) | 0.030715219 | 1.0000000 |
| Hypercholesterolemia | 214 | 70 | 0.47 (0.15–1.5) | 0.200883917 | 1.0000000 |
| Tumor | 214 | 70 | 1.74 (1.02–2.95) | 0.041879511 | 1.0000000 |
| Thyreopathy | 214 | 70 | 1.19 (0.51–2.76) | 0.684096031 | 1.0000000 |
| Hypertriglyceridemia | 214 | 70 | 0.79 (0.19–3.21) | 0.738138639 | 1.0000000 |
| Other comorbidities | 214 | 70 | 2.65 (1.45–4.84) | 0.001604357 | 0.0786135 |
| Charlson Index (without dementia) ^ | 214 | 70 | 1.28 (1.16–1.41) | 0.000000394 | 0.0000193 |
| Use of psychotropic drugs | 214 | 70 | 1.78 (0.97–3.25) | 0.062649518 | 1.0000000 |
| Dementia | 213 | 69 | 2.36 (1.39–4.03) | 0.001521415 | 0.0745493 |
| Vit. D therapy | 214 | 70 | 1.21 (0.38–3.85) | 0.750983797 | 1.0000000 |
| Neutrophil/lymphocyte ratio § | 210 | 67 | 1.57 (1.37–1.81) | 0.000000000 | 0.0000000 |
| Hematocrit § | 210 | 67 | 0.62 (0.44–0.89) | 0.009681733 | 0.4744049 |
| Hemoglobin § | 210 | 67 | 0.15 (0.05–0.45) | 0.000721321 | 0.0353447 |
| MCV § | 204 | 62 | 1.24 (0.89–1.73) | 0.202686714 | 1.0000000 |
| RBC § | 210 | 67 | 0.07 (0–1.61) | 0.096831372 | 1.0000000 |
| WBC § | 210 | 67 | 1.55 (1.24–1.94) | 0.000139079 | 0.0068149 |
| Neutrophils § | 210 | 67 | 1.22 (1.09–1.37) | 0.000454567 | 0.0222738 |
| Lymphocytes § | 210 | 67 | 0.99 (0.54–1.8) | 0.972133027 | 1.0000000 |
| Platelets § | 210 | 67 | 1 (0.98–1.03) | 0.880538484 | 1.0000000 |
| INR § | 194 | 60 | 10.95 (0.63–189.64) | 0.099877021 | 1.0000000 |
| PTT § | 194 | 60 | 1.52 (0.96–2.41) | 0.075694508 | 1.0000000 |
| ALT § | 205 | 65 | 1.01 (0.97–1.04) | 0.702865821 | 1.0000000 |
| Total bilirubin § | 202 | 62 | 3.29 (0.19–55.53) | 0.408924418 | 1.0000000 |
| Alkaline phosphatase § | 163 | 52 | 1.05 (1.01–1.09) | 0.014802566 | 0.7253258 |
| ɣ-GT § | 164 | 53 | 1.01 (0.99–1.03) | 0.329223790 | 1.0000000 |
| AST § | 205 | 65 | 1.02 (1–1.05) | 0.071553567 | 1.0000000 |
| Total proteins § | 203 | 63 | 0.02 (0–0.3) | 0.005466919 | 0.2678790 |
| Creatinine § | 206 | 65 | 1.36 (0.81–2.3) | 0.250416795 | 1.0000000 |
| e-GFR § | 202 | 65 | 0.89 (0.83–0.95) | 0.000202712 | 0.0099329 |
| Glycemia § | 204 | 64 | 1.05 (1.02–1.08) | 0.002704169 | 0.1325043 |
| ESR § | 149 | 42 | 1.08 (0.96–1.2) | 0.184670429 | 1.0000000 |
| Triglycerides § | 163 | 49 | 1 (0.95–1.05) | 0.994884031 | 1.0000000 |
| Cholesterol § | 163 | 49 | 0.93 (0.86–1.01) | 0.087372174 | 1.0000000 |
| LDH § | 155 | 45 | 1.03 (1.02–1.05) | 0.000171386 | 0.0083979 |
| CK § | 162 | 55 | 1 (0.99–1.02) | 0.578550518 | 1.0000000 |
| Troponin § | 101 | 29 | 1 (1–1) | 0.033795411 | 1.0000000 |
| D-dimer § | 119 | 35 | 1 (1–1) | 0.000014371 | 0.0007042 |
| Procalcitonin § | 118 | 38 | 1.02 (0.49–2.16) | 0.949739846 | 1.0000000 |
| CRP § | 207 | 65 | 2.37 (1.76–3.19) | 0.000000013 | 0.0000006 |
| Model A | Model B | |||
|---|---|---|---|---|
| Variable | Hazard Ratio (95% Confidence Interval) | p-Value | Hazard Ratio (95% Confidence Interval) | p-Value |
| Neutrophils-to-lymphocytes ratio § | 1.03 (1.01–1.05) | 0.001443974 | 1.03 (1.01–1.05) | 0.001066611 |
| Baseline CRP § | 1.07 (1.03–1.1) | 0.000282734 | 1.06 (1.02–1.1) | 0.001314788 |
| Charlson Index (without dementia) | 1.21 (1.07–1.36) | 0.001655282 | 1.22 (1.08–1.38) | 0.000977608 |
| Delirium | 3.81 (2.15–6.73) | 4.25597 × 10−6 | ||
| Hyperactive delirium (=15) | 2.09 (0.64–6.83) | 0.2199668 | ||
| Hypoactive delirium (N = 21) | 5.95 (2.85–12.42) | 2.05376 × 10−6 | ||
| Mixed delirium (N = 11) | 3.02 (1.08–8.46) | 0.03588895 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Giorgio, A.; Mirijello, A.; De Gennaro, C.; Fontana, A.; Alboini, P.E.; Florio, L.; Inchingolo, V.; Zarrelli, M.; Miscio, G.; Raggi, P.; et al. Factors Associated with Delirium in COVID-19 Patients and Their Outcome: A Single-Center Cohort Study. Diagnostics 2022, 12, 544. https://doi.org/10.3390/diagnostics12020544
Di Giorgio A, Mirijello A, De Gennaro C, Fontana A, Alboini PE, Florio L, Inchingolo V, Zarrelli M, Miscio G, Raggi P, et al. Factors Associated with Delirium in COVID-19 Patients and Their Outcome: A Single-Center Cohort Study. Diagnostics. 2022; 12(2):544. https://doi.org/10.3390/diagnostics12020544
Chicago/Turabian StyleDi Giorgio, Annabella, Antonio Mirijello, Clara De Gennaro, Andrea Fontana, Paolo Emilio Alboini, Lucia Florio, Vincenzo Inchingolo, Michele Zarrelli, Giuseppe Miscio, Pamela Raggi, and et al. 2022. "Factors Associated with Delirium in COVID-19 Patients and Their Outcome: A Single-Center Cohort Study" Diagnostics 12, no. 2: 544. https://doi.org/10.3390/diagnostics12020544
APA StyleDi Giorgio, A., Mirijello, A., De Gennaro, C., Fontana, A., Alboini, P. E., Florio, L., Inchingolo, V., Zarrelli, M., Miscio, G., Raggi, P., Marciano, C., Antonioni, A., De Cosmo, S., Aucella, F., Greco, A., Carella, M., Copetti, M., & Leone, M. A., on behalf of the CSS-COVID-19 Group. (2022). Factors Associated with Delirium in COVID-19 Patients and Their Outcome: A Single-Center Cohort Study. Diagnostics, 12(2), 544. https://doi.org/10.3390/diagnostics12020544