
Testosterone Therapy and Diaphragm Performance in a Male Patient with COVID-19: A Case Report

 , , and
, , and 
Abstract
:1. Introduction
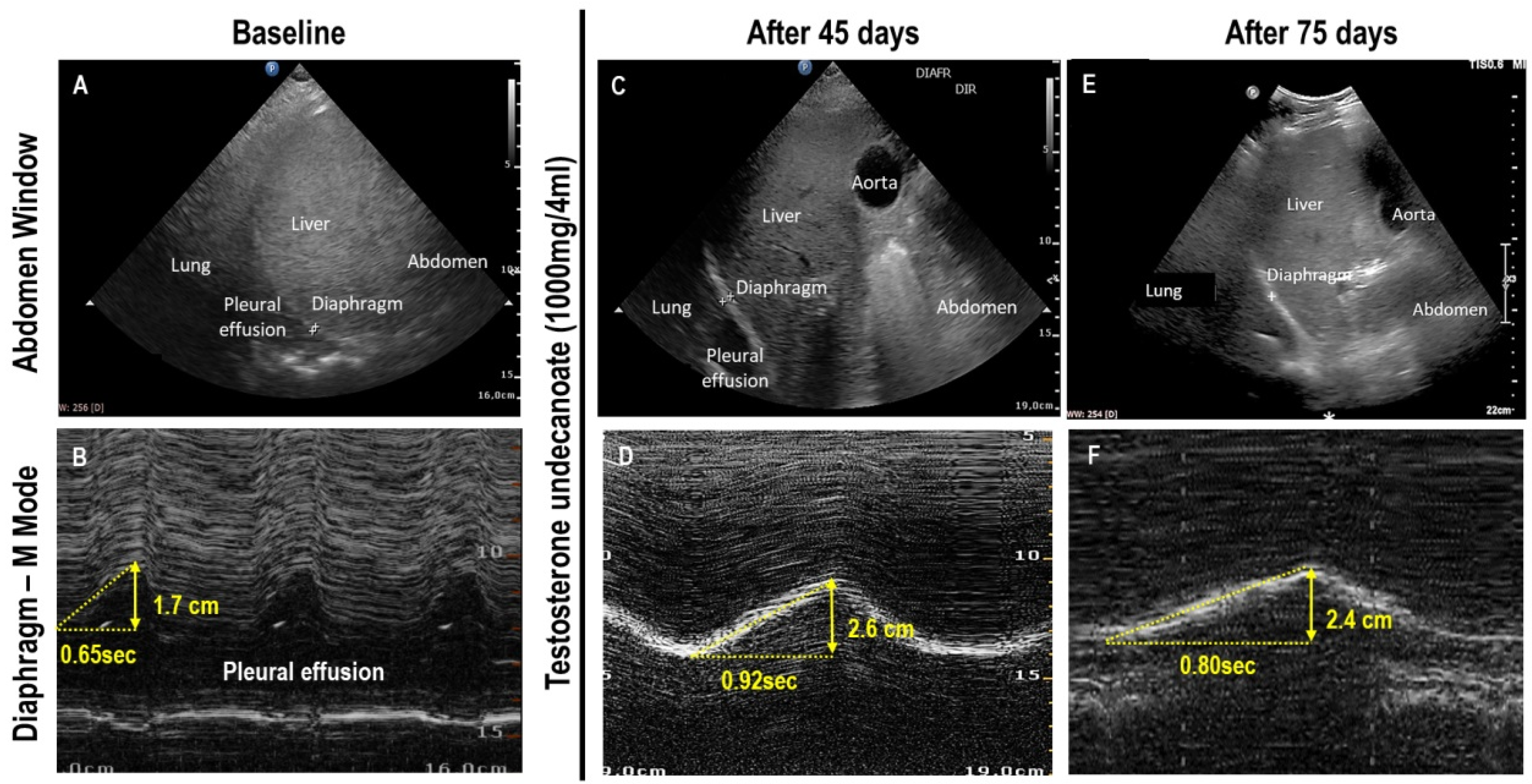
2. Case Study
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rastrelli, G.; Di Stasi, V.; Inglese, F.; Beccaria, M.; Garuti, M.; Di Costanzo, D.; Spreafico, F.; Greco, G.F.; Cervi, G.; Pecoriello, A.; et al. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology 2020, 9, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Camici, M.; Zuppi, P.; Lorenzini, P.; Scarnecchia, L.; Pinnetti, C.; Cicalini, S.; Nicastri, E.; Petrosillo, N.; Palmieri, F.; D’Offizi, G.; et al. Role of testosterone in SARS-CoV-2 infection: A key pathogenic factor and a biomarker for severe pneumonia. Int. J. Infect. Dis. 2021, 108, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Gröner, M.F.; de Carvalho, R.C.; Camillo, J.; Ferreira, P.R.A.; Fraietta, R. Effects of COVID-19 on male reproductive system. Int. Braz. J. Urol. 2021, 47, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.N.; Hussain, F.; Hashmi, S.K. Role of testosterone in COVID-19 patients—A double-edged sword? Med. Hypotheses 2020, 144, 110287. [Google Scholar] [CrossRef]
- Napolitano, L.; Barone, B.; Crocetto, F.; Capece, M.; La Rocca, R. The COVID-19 Pandemic: Is It A Wolf Consuming Fertility? Int. J. Fertil. Steril. 2020, 14, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Palkar, A.; Narasimhan, M.; Greenberg, H.; Singh, K.; Koenig, S.; Mayo, P.; Gottesman, E. Diaphragm Excursion-Time Index: A New Parameter Using Ultrasonography to Predict Extubation Outcome. Chest 2018, 153, 1213–1220. [Google Scholar] [CrossRef]
- Bax, F.; Lettieri, C.; Marini, A.; Pellitteri, G.; Surcinelli, A.; Valente, M.; Budai, R.; Patruno, V.; Gigli, G.L. Clinical and neurophysiological characterization of muscular weakness in severe COVID-19. Neurol. Sci. 2021, 42, 2173–2178. [Google Scholar] [CrossRef]
- Dalakas, M.C. Inflammatory myopathies: Update on diagnosis, pathogenesis and therapies, and COVID-19-related implications. Acta Myol. 2020, 39, 289–301. [Google Scholar] [CrossRef]
- Islam, B.; Ahmed, M.; Islam, Z.; Begum, S.M. Severe acute myopathy following SARS-CoV-2 infection: A case report and review of recent literature. Skelet. Muscle 2021, 11, 1–7. [Google Scholar] [CrossRef]
- Pasiakos, S.M.; Berryman, C.E.; Karl, J.P.; Lieberman, H.R.; Orr, J.S.; Margolis, L.M.; Caldwell, J.A.; Young, A.J.; Montano, M.A.; Evans, W.J.; et al. Effects of testosterone supplementation on body composition and lower-body muscle function during severe exercise- and diet-induced energy deficit: A proof-of-concept, single centre, randomised, double-blind, controlled trial. eBioMedicine 2019, 46, 411–422. [Google Scholar] [CrossRef]
- Sattler, F.R.; Castaneda-Sceppa, C.; Binder, E.F.; Schroeder, E.T.; Wang, Y.; Bhasin, S.; Kawakubo, M.; Stewart, Y.; Yarasheski, K.E.; Ulloor, J.; et al. Testosterone and Growth Hormone Improve Body Composition and Muscle Performance in Older Men. J. Clin. Endocrinol. Metab. 2009, 94, 1991–2001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignozzi, L.; Cellai, I.; Santi, R.; Lombardelli, L.; Morelli, A.; Comeglio, P.; Filippi, S.; Logiodice, F.; Carini, M.; Nesi, G.; et al. Antiinflammatory effect of androgen receptor activation in human benign prostatic hyperplasia cells. J. Endocrinol. 2012, 214, 31–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamad, N.-V.; Wong, S.K.; Hasan, W.N.W.; Jolly, J.J.; Nur-Farhana, M.F.; Ima-Nirwana, S.; Chin, K.-Y. The relationship between circulating testosterone and inflammatory cytokines in men. Aging Male 2018, 22, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Vivier, E.; Dessap, A.M.; Dimassi, S.; Vargas, F.; Lyazidi, A.; Thille, A.W.; Brochard, L. Diaphragm ultrasonography to estimate the work of breathing during non-invasive ventilation. Intensiv. Care Med. 2012, 38, 796–803. [Google Scholar] [CrossRef]
- Viveiros, A.; Rasmuson, J.; Vu, J.; Mulvagh, S.L.; Yip, C.Y.Y.; Norris, C.M.; Oudit, G.Y. Sex differences in COVID-19: Candidate pathways, genetics of ACE2, and sex hormones. Am. J. Physiol. Circ. Physiol. 2021, 320, H296–H304. [Google Scholar] [CrossRef]
- Eshima, N.; Tokumaru, O.; Hara, S.; Bacal, K.; Korematsu, S.; Tabata, M.; Karukaya, S.; Yasui, Y.; Okabe, N.; Matsuishi, T. Sex- and Age-Related Differences in Morbidity Rates of 2009 Pandemic Influenza A H1N1 Virus of Swine Origin in Japan. PLoS ONE 2011, 6, e19409. [Google Scholar] [CrossRef]
- Bienvenu, L.A.; Noonan, J.; Wang, X.; Peter, K. Higher mortality of COVID-19 in males: Sex differences in immune response and cardiovascular comorbidities. Cardiovasc. Res. 2020, 116, 2197–2206. [Google Scholar] [CrossRef]
- Lucas, J.M.; Heinlein, C.; Kim, T.; Hernandez, S.A.; Malik, M.S.; True, L.D.; Morrissey, C.; Corey, E.; Montgomery, B.; Mostaghel, E.; et al. The Androgen-Regulated Protease TMPRSS2 Activates a Proteolytic Cascade Involving Components of the Tumor Microenvironment and Promotes Prostate Cancer Metastasis. Cancer Discov. 2014, 4, 1310–1325. [Google Scholar] [CrossRef] [Green Version]
- Tomlins, S.A.; Rhodes, D.R.; Perner, S.; Dhanasekaran, S.M.; Mehra, R.; Sun, X.-W.; Varambally, S.; Cao, X.; Tchinda, J.; Kuefer, R.; et al. Recurrent Fusion of TMPRSS2 and ETS Transcription Factor Genes in Prostate Cancer. Science 2005, 310, 644–648. [Google Scholar] [CrossRef]
- Muus, C.; The NHLBI LungMap Consortium; Luecken, M.D.; Eraslan, G.; Sikkema, L.; Waghray, A.; Heimberg, G.; Kobayashi, Y.; Vaishnav, E.D.; Subramanian, A.; et al. Single-cell meta-analysis of SARS-CoV-2 entry genes across tissues and demographics. Nat. Med. 2021, 27, 546–559. [Google Scholar] [CrossRef]
- Diaz-Arjonilla, M.; Schwarcz, M.; Swerdloff, R.S.; Wang, C. Obesity, low testosterone levels and erectile dysfunction. Int. J. Impot. Res. 2008, 21, 89–98. [Google Scholar] [CrossRef]
- Mohan, S.S.; Knuiman, M.; Divitini, M.L.; James, A.L.; Musk, A.W.; Handelsman, D.J.; Beilin, J.; Hunter, M.; Yeap, B.B. Higher serum testosterone and dihydrotestosterone, but not oestradiol, are independently associated with favourable indices of lung function in community-dwelling men. Clin. Endocrinol. 2015, 83, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, G.; Volterrani, M.; Iellamo, F.; Marazzi, G.; Massaro, R.; Miceli, M.; Mammi, C.; Piepoli, M.; Fini, M.; Rosano, G.M. Effect of Long-Acting Testosterone Treatment on Functional Exercise Capacity, Skeletal Muscle Performance, Insulin Resistance, and Baroreflex Sensitivity in Elderly Patients with Chronic Heart Failure: A Double-Blind, Placebo-Controlled, Randomized Study. J. Am. Coll. Cardiol. 2009, 54, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.F.; Zakai, N.A.; MacLehose, R.F.; Cowan, L.T.; Adam, T.J.; Alonso, A.; Lutsey, P.L. Association of Testosterone Therapy with Risk of Venous Thromboembolism among Men with and without Hypogonadism. JAMA Intern. Med. 2020, 180, 190. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline | After 45 Days | After 75 Days | |
|---|---|---|---|
| Diaphragm ultrasonography measurements | |||
| Thickness at expiration (cm) | 0.30 | 0.31 | 0.30 |
| Thickness at inspiration (cm) | 0.41 | 0.51 | 0.51 |
| Thickness fraction (%) | 37 | 67 | 70 |
| Excursion-time index during inspiration (cm/s) | 2.6 | 2.4 | 3.0 |
| Blood laboratory measurements | |||
| Total testosterone (ng/dL) | 9.3 | 212 | 332 |
| Bioavailable testosterone (ng/dL) | 5.8 | 129 | 196 |
| Sex hormone binding globulin (nmol/L) | 10.5 | 15.5 | 17.9 |
| Total prostate-specific antigen (ng/mL) | 0.5 | 0.5 | 0.4 |
| Free prostate-specific antigen (ng/mL) | 0.2 | 0.2 | 0.2 |
| C-reactive protein (mg/dL) | 6.6 | 5.4 | 2.2 |
| Ferritin (ng/mL) | 1996 | 1983 | 1041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martins, G.; Verdeal, J.C.R.; Tostes, H.; da Silva, A.R.O.; Tessarollo, B.; Rocha, N.N.; Rocco, P.R.M.; Silva, P.L. Testosterone Therapy and Diaphragm Performance in a Male Patient with COVID-19: A Case Report. Diagnostics 2022, 12, 535. https://doi.org/10.3390/diagnostics12020535
Martins G, Verdeal JCR, Tostes H, da Silva ARO, Tessarollo B, Rocha NN, Rocco PRM, Silva PL. Testosterone Therapy and Diaphragm Performance in a Male Patient with COVID-19: A Case Report. Diagnostics. 2022; 12(2):535. https://doi.org/10.3390/diagnostics12020535
Chicago/Turabian StyleMartins, Gloria, Juan Carlos Rosso Verdeal, Helio Tostes, Alice Ramos Oliveira da Silva, Bernardo Tessarollo, Nazareth Novaes Rocha, Patricia Rieken Macedo Rocco, and Pedro Leme Silva. 2022. "Testosterone Therapy and Diaphragm Performance in a Male Patient with COVID-19: A Case Report" Diagnostics 12, no. 2: 535. https://doi.org/10.3390/diagnostics12020535
APA StyleMartins, G., Verdeal, J. C. R., Tostes, H., da Silva, A. R. O., Tessarollo, B., Rocha, N. N., Rocco, P. R. M., & Silva, P. L. (2022). Testosterone Therapy and Diaphragm Performance in a Male Patient with COVID-19: A Case Report. Diagnostics, 12(2), 535. https://doi.org/10.3390/diagnostics12020535