
2-[18F]FDG PET in the Management of Radioiodine Refractory Differentiated Thyroid Cancer in the Era of Thyrosin-Kinases Inhibitors: A Real-Life Retrospective Study


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. 2-[18F]FDGPET/CT Acquisition
2.2. Image Analysis
2.3. Laboratory Tests
2.4. Statistical Analysis
3. Results
3.1. First 2-[18F]FDGPET Scan Assessment
3.2. TKI Treatment
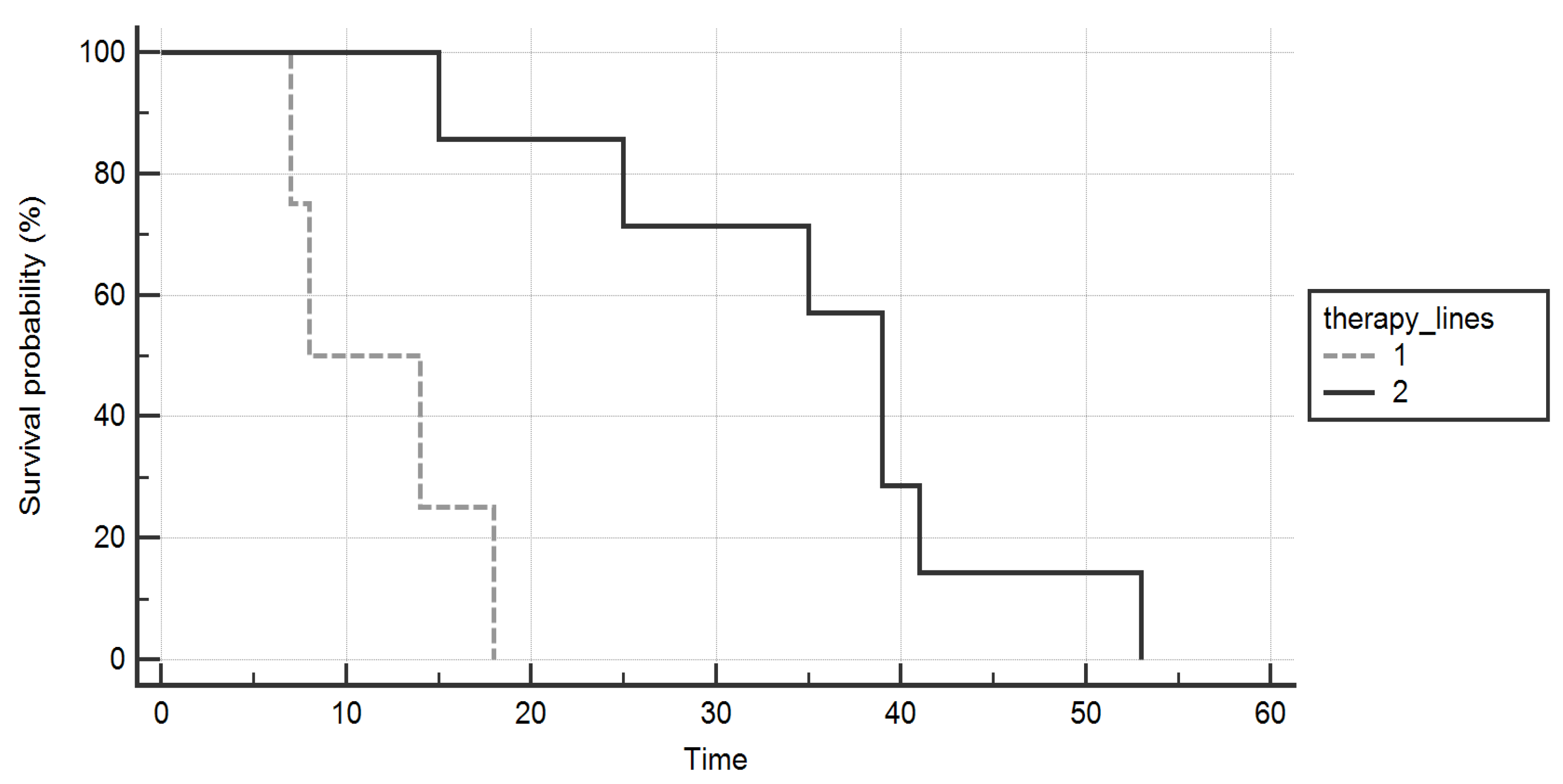
3.3. Overall Survival
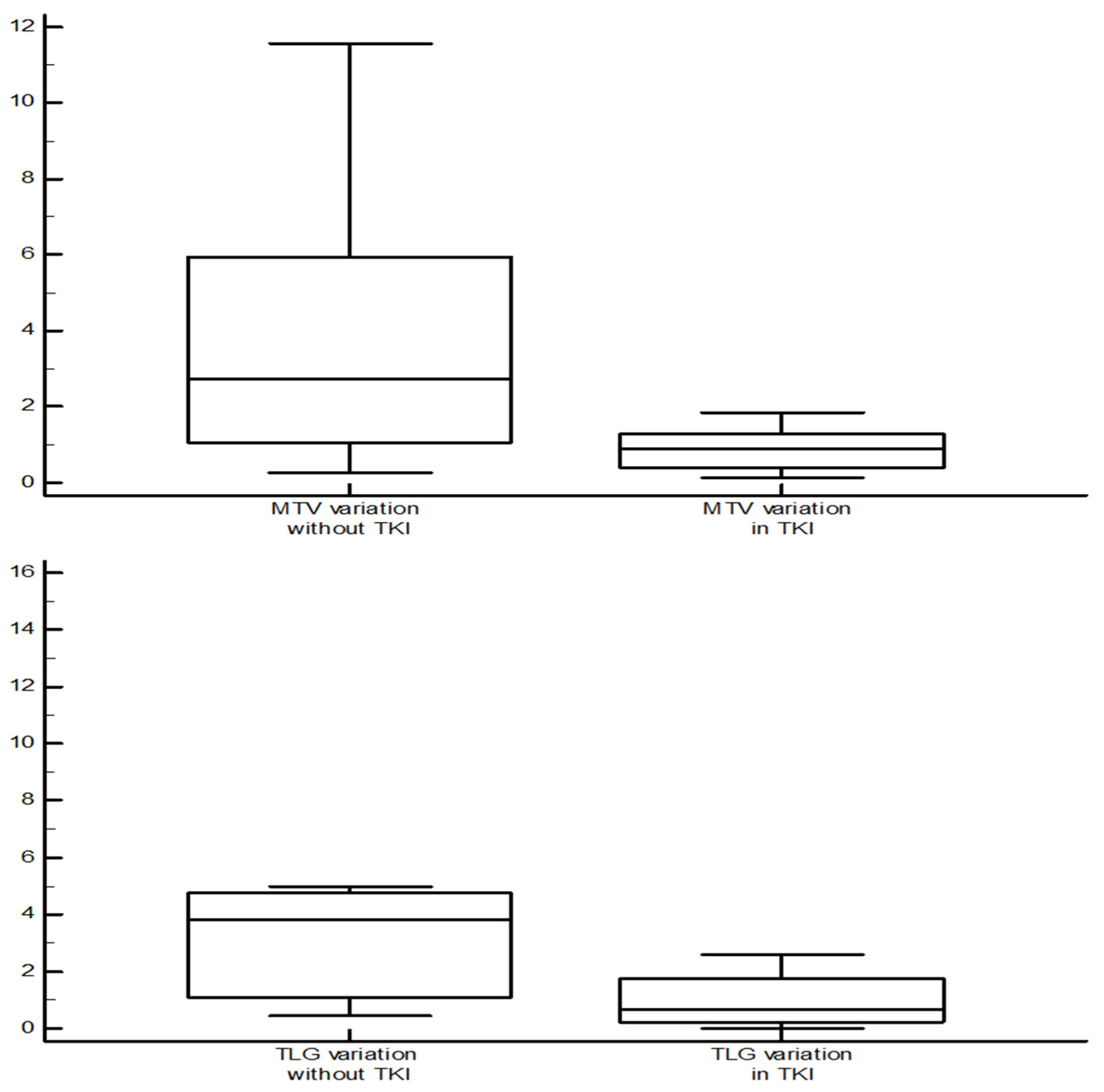
3.4. 2-[18F]FDGPET/CT Parameters Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tuttle, R.M.; Ahuja, S.; Avram, A.M.; Bernet, V.J.; Bourguet, P.; Daniels, G.H.; Dillehay, G.; Draganescu, C.; Flux, G.; Führer, D.; et al. Controversies, Consensus, and Collaboration in the Use of 131I Therapy in Differentiated Thyroid Cancer: A Joint Statement from the American Thyroid Association, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecular Imaging, and the European Thyroid Association. Thyroid 2019, 29, 461–470. [Google Scholar] [PubMed]
- Pacini, F.; Basolo, F.; Bellantone, R.; Boni, G.; Cannizzaro, M.A.; De Palma, M.; Durante, C.; Elisei, R.; Fadda, G.; Frasoldati, A.; et al. Italian consensus on diagnosis and treatment of differentiated thyroid cancer: Joint statements of six Italian societies. J. Endocrinol. Investig. 2018, 41, 849–876. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Iglesias, L.; Klain, M.; Pitoia, F.; Schlumberger, M.J. Radioactive iodine-refractory differentiated thyroid cancer: An uncommon but challenging situation. Arch. Endocrinol. Metab. 2017, 61, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Berdelou, A.; Borget, I.; Godbert, Y.; Nguyen, T.; Garcia, M.E.; Chougnet, C.N.; Ferru, A.; Buffet, C.; Chabre, O.; Huillard, O.; et al. Lenvatinib for the Treatment of Radioiodine-Refractory Thyroid Cancer in Real-Life Practice. Thyroid 2018, 28, 72–78. [Google Scholar] [CrossRef]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef]
- Brose, M.S.; Nutting, C.M.; Jarzab, B.; Elisei, R.; Siena, S.; Bastholt, L.; de la Fouchardiere, C.; Pacini, F.; Paschke, R.; Shong, Y.K.; et al. Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: A randomised, double-blind, phase 3 trial. Lancet 2014, 384, 319–328. [Google Scholar] [CrossRef]
- De Leo, S.; Di Stefano, M.; Persani, L.; Fugazzola, L.; Colombo, C. Lenvatinib as first-line treatment for advanced thyroid cancer: Long progression-free survival. Endocrine 2020, 72, 462–469. [Google Scholar] [CrossRef]
- Wirth, L.J.; Tahara, M.; Robinson, B.; Francis, S.; Brose, M.S.; Habra, M.A.; Newbold, K.; Kiyota, N.; Dutcus, C.E.; Mathias, E.; et al. Treatment-emergent hypertension and efficacy in the phase 3 Study of (E7080) lenvatinib in differentiated cancer of the thyroid (SELECT). Cancer 2018, 124, 2365–2372. [Google Scholar] [CrossRef]
- Haddad, R.I.; Schlumberger, M.; Wirth, L.J.; Sherman, E.J.; Shah, M.H.; Robinson, B.; Dutcus, C.E.; Teng, A.; Gianoukakis, A.G.; Sherman, S.I. Incidence and timing of common adverse events in Lenvatinib-treated patients from the SELECT trial and their association with survival outcomes. Endocrine 2017, 56, 121–128. [Google Scholar] [CrossRef]
- Robinson, B.; Schlumberger, M.; Wirth, L.J.; Dutcus, C.E.; Song, J.; Taylor, M.H.; Kim, S.B.; Krzyzanowska, M.K.; Capdevila, J.; Sherman, S.I.; et al. Characterization of Tumor Size Changes over Time from the Phase 3 Study of Lenvatinib in Thyroid Cancer. J. Clin. Endocrinol. Metab. 2016, 101, 4103–4109. [Google Scholar] [CrossRef] [PubMed]
- Wassermann, J.; Bernier, M.O.; Spano, J.P.; Lepoutre-Lussey, C.; Buffet, C.; Simon, J.M.; Ménégaux, F.; Tissier, F.; Leban, M.; Leenhardt, L. Outcomes and Prognostic Factors in Radioiodine Refractory Differentiated Thyroid Carcinomas. Oncologist 2016, 21, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Song, E.; Kim, M.; Kim, E.Y.; Kim, B.H.; Shin, D.Y.; Kang, H.C.; Ahn, B.C.; Kim, W.B.; Shong, Y.K.; Jeon, M.J.; et al. Lenvatinib for Radioactive Iodine-Refractory Differentiated Thyroid Carcinoma and Candidate Biomarkers Associated with Survival: A Multicenter Study in Korea. Thyroid 2020, 30, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Lückerath, K.; Schmid, J.S.; Higuchi, T.; Kreissl, M.C.; Grelle, I.; Reiners, C.; Buck, A.K.; Lapa, C. Thyroglobulin fluctuations in patients with iodine-refractory differentiated thyroid carcinoma on lenvatinib treatment-initial experience. Sci. Rep. 2016, 6, 28081. [Google Scholar] [CrossRef]
- Manohar, P.M.; Beesley, L.J.; Bellile, E.L.; Worden, F.P.; Avram, A.M. Prognostic Value of FDG-PET/CT Metabolic Parameters in Metastatic Radioiodine-Refractory Differentiated Thyroid Cancer. Clin. Nucl. Med. 2018, 43, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Ahmaddy, F.; Burgard, C.; Beyer, L.; Koehler, V.F.; Bartenstein, P.; Fabritius, M.P.; Geyer, T.; Wenter, V.; Ilhan, H.; Spitzweg, C.; et al. 18F-FDG-PET/CT in Patients with Advanced, Radioiodine Refractory Thyroid Cancer Treated with Lenvatinib. Cancers 2021, 13, 317. [Google Scholar] [CrossRef]
- Valerio, L.; Guidoccio, F.; Giani, C.; Tardelli, E.; Puccini, G.; Puleo, L.; Minaldi, E.; Boni, G.; Elisei, R.; Volterrani, D. [18F]-FDG-PET/CT Correlates with the Response of Radiorefractory Thyroid Cancer to Lenvatinib and Patient Survival. J. Clin. Endocrinol. Metab. 2021, 106, 2355–2366. [Google Scholar] [CrossRef]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving Considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50 (Suppl. S1), 122S–150S. [Google Scholar] [CrossRef]
- Ora, M.; Nazar, A.H.; Pradhan, P.K.; Mishra, P.; Barai, S.; Arya, A.; Dixit, M.; Parashar, A.; Gambhir, S. The Utility of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Differentiated Thyroid Cancer Patients with Biochemical Recurrence and Negative Whole-Body Radioiodine Scintigraphy and Evaluation of the Possible Role of a Limited Regional Scan. Indian J. Nucl. Med. 2020, 35, 203–209. [Google Scholar]
- Chai, H.; Zhang, H.; Yu, Y.L.; Gao, Y.C. Optimal threshold of stimulated serum thyroglobulin level for 18F-FDG PET/CT imaging in patients with thyroid cancer. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2017, 37, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Masaki, C.; Sugino, K.; Saito, N.; Saito, Y.; Tanaka, T.; Ogimi, Y.; Maeda, T.; Osaku, T.; Akaishi, J.; Hames, K.Y.; et al. Lenvatinib induces early tumor shrinkage in patients with advanced thyroid carcinoma. Endocr. J. 2017, 64, 819–826. [Google Scholar] [CrossRef][Green Version]
- Kish, J.K.; Chatterjee, D.; Wan, Y.; Yu, H.T.; Liassou, D.; Feinberg, B.A. Lenvatinib and Subsequent Therapy for Radioactive Iodine-Refractory Differentiated Thyroid Cancer: A Real-World Study of Clinical Effectiveness in the United States. Adv. Ther. 2020, 37, 2841–2852. [Google Scholar] [CrossRef] [PubMed]
- Brilli, L.; Dalmiglio, C.; Pilli, T.; Barbato, F.; Maino, F.; Capezzone, M.; Cartocci, A.; Castagna, M.G. Improvement of Overall Survival Using TKIs as Salvage Therapy in Advanced Thyroid Carcinoma: Real-Life Data on a Single Center Experience. J. Clin. Med. 2021, 10, 384. [Google Scholar] [CrossRef] [PubMed]
- Leboulleux, S.; Schroeder, P.R.; Busaidy, N.L.; Auperin, A.; Corone, C.; Jacene, H.A.; Ewertz, M.E.; Bournaud, C.; Wahl, R.L.; Sherman, S.I.; et al. Assessment of the incremental value of recombinant thyrotropin stimulation before 2-[18F]-Fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography imaging to localize residual differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 2009, 94, 1310–1316. [Google Scholar] [CrossRef]
- Almeida, L.S.; Araújo, M.L.; Santos, A.O.; Montali da Assumpção, L.V.; Lima, M.L.; Ramos, C.D.; Zantut-Wittmann, D.E.; Etchebehere, E.C. Head-to-head comparison of F-18 FDG PET/CT in radioidine refractory thyroid cancer patients with elevated versus suppressed TSH levels a pilot study. Heliyon 2020, 6, e03450. [Google Scholar] [CrossRef]
- Ma, C.; Xie, J.; Lou, Y.; Gao, Y.; Zuo, S.; Wang, X. The role of TSH for 18F-FDG-PET in the diagnosis of recurrence and metastases of differentiated thyroid carcinoma with elevated thyroglobulin and negative scan: A meta-analysis. Eur. J. Endocrinol. 2010, 163, 177–183. [Google Scholar] [CrossRef]
- Carhill, A.A.; Litofsky, D.R.; Ross, D.S.; Jonklaas, J.; Cooper, D.S.; Brierley, J.D.; Ladenson, P.W.; Ain, K.B.; Fein, H.G.; Haugen, B.R.; et al. Long-Term Outcomes following Therapy in Differentiated Thyroid Carcinoma: NTCTCS Registry Analysis 1987–2012. J. Clin. Endocrinol. Metab. 2015, 100, 3270–3279. [Google Scholar] [CrossRef]
- Na, S.J.; Yoo, I.R.; O, J.H.; Lin, C.; Lin, Q.; Kim, S.H.; Chung, S.K. Diagnostic accuracy of (18)F-fluorodeoxyglucose positron emission tomography/computed tomography in differentiated thyroid cancer patients with elevated thyroglobulin and negative (131)I whole body scan: Evaluation by thyroglobulin level. Ann. Nucl. Med. 2012, 26, 26–34. [Google Scholar] [CrossRef]
- Albano, D.; Tulchinsky, M.; Dondi, F.; Mazzoletti, A.; Lombardi, D.; Bertagna, F.; Giubbini, R. Thyroglobulin doubling time offers a better threshold than thyroglobulin level for selecting optimal candidates to undergo localizing [18F]FDG PET/CT in non-iodine avid differentiated thyroid carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 461–468. [Google Scholar] [CrossRef]
- Harach, H.R.; Franssila, K.O. Thyroglobulin immunostaining in follicular thyroid carcinoma: Relationship to the degree of differentiation and cell type. Histopathology 1988, 13, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y. The role of 18F-FDG PET/CT in the follow-up of well-differentiated thyroid cancer with negative thyroglobulin but positive and/or elevated antithyroglobulin antibody. Nucl. Med. Commun. 2016, 37, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Nilubol, N.; Zhang, L.; Kebebew, E. Multivariate analysis of the relationship between male sex, disease-specific survival, and features of tumor aggressiveness in thyroid cancer of follicular cell origin. Thyroid 2013, 23, 695–702. [Google Scholar] [CrossRef]
- Hei, H.; Zhou, B.; Gong, W.; Zheng, C.; Qin, J. Male patients with papillary thyroid cancer have a higher risk of extranodal extension. Int. J. Clin. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients | Age | Sex | Histology | TKI | TSH * (mU/L) | fT4 ** (pg/mL) | Tg ** (ng/mL) | LT4 (µg/Week) | MTV * (cm3) | TLG* | OS (Months) | N° FDG-PET |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 63 | F | FTC | - | 0.89 | 14.2 | 2283.0 | 1050 | 1.56 | 6.88 | 35 | 6 |
| 2 | 77 | M | PTC | L | 0.03 | 22.2 | 1.1 | 900 | 126.67 | 700.48 | 53 | 4 |
| 3 | 79 | M | FTC | - | 0.01 | 22.4 | 20,583.2 | 1100 | 31.13 | 377.92 | 25 | 2 |
| 4 | 67 | M | FTC | S | 0.15 | 18.7 | 26.3 | 1050 | 25.00 | 314.17 | 39 | 5 |
| 5 | 71 | M | PTC | S | 0.06 | 18.8 | 2237.1 | 1125 | 3.27 | - | - | 4 |
| 6 | 70 | F | FTC | L | 0.02 | 22.1 | 2014.5 | 850 | 0.71 | 5.34 | - | 1 |
| 7 | 43 | M | FTC | S | 0.01 | 21.0 | 698.9 | 1400 | 7.25 | 45.96 | 41 | 5 |
| 8 | 76 | M | PTC | S | 0.17 | 15.1 | 532.4 | 1050 | 3.55 | 27.16 | 39 | 5 |
| 9 | 81 | M | HC+PTC | S | 2.44 | 12.3 | 1025.2 | 225 | 50.98 | - | 15 | 2 |
| 10 | 68 | F | FTC | S | 0.13 | 19.5 | 8853.3 | 650 | 4.04 | 22.99 | 14 | 2 |
| 11 | 53 | M | FTC | - | 4.70 | 10.5 | 5431.7 | 1050 | 1197.32 | 10,632.20 | 7 | 3 |
| 12 | 77 | F | FTC | S | 0.01 | 17.7 | 25,454.2 | 825 | 238.88 | 1748.60 | 8 | 1 |
| 13 | 76 | F | PDTC | - | 2.41 | 12.3 | 0.1 | 450 | 27.44 | 143.51 | 18 | 2 |
| 14 | 75 | M | PTC | - | 0.01 | 17.8 | 3.8 | 925 | 12.80 | 44.42 | - | 4 |
| Before the Study Period | At the Time of the First 18F-FDG PET Scan | During the Study Period | |
|---|---|---|---|
| 1 | sorafenib | no | lenvatinib |
| 2 | sorafenib | lenvatinib | lenvatinib |
| 3 | sorafenib | no | lenvatinib |
| 4 | sorafenib | sorafenib | lenvatinib |
| 5 | sorafenib | sorafenib | lenvatinib |
| 6 | lenvatinib | lenvatinib | - |
| 7 | sorafenib | sorafenib | lenvatinib |
| 8 | sorafenib | sorafenib | lenvatinib |
| 9 | sorafenib | sorafenib | lenvatinib |
| 10 | sorafenib | sorafenib | no |
| 11 | no | no | sorafenib |
| 12 | sorafenib | sorafenib | - |
| 13 | no | no | lenvatinib |
| 14 | no | no | lenvatinib |
| Null Model-2 Log Likelihood | Full Model-2 Log Likelihood | Chi-Squared | DF | Significance Level | |
|---|---|---|---|---|---|
| MTV | 35.58 | 31.47 | 4.43 | 1 | p = 0.035 |
| TLG | 30.78 | 25.92 | 4.86 | 1 | p = 0.027 |
| TSH | 35.58 | 29.77 | 5.81 | 1 | p = 0.016 |
| fT4 | 35.58 | 31.59 | 3.99 | 1 | p = 0.046 |
| Tg | 35.58 | 32.58 | 2.99 | 1 | p = 0.083 |
| RAI dosage | 30.78 | 30.46 | 0.32 | 1 | p = 0.545 |
| AUC | Significance Level | Youden Index (J) | Associated Criterion | Sensitivity % | Specificity % | |
|---|---|---|---|---|---|---|
| MTV | 0.815 | 0.001 | 0.56 | >126.67 | 60 | 96 |
| TLG | 0.812 | 0.001 | 0.60 | >817.86 | 60 | 100 |
| TSH | 0.708 | 0.133 | 0.47 | >0.47 | 67 | 81 |
| fT4 | 0.763 | 0.010 | 0.54 | ≤17.68 | 100 | 54 |
| Tg | 0.675 | 0.145 | 0.48 | >1253.0 | 75 | 73 |
| RAI dosage | 0.563 | 0.793 | 0.37 | ≤500 | 100 | 37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gay, S.; Raffa, S.; De’Luca di Pietralata, A.; Bauckneht, M.; Vera, L.; Miceli, A.; Albertelli, M.; Morbelli, S.; Giusti, M.; Ferone, D. 2-[18F]FDG PET in the Management of Radioiodine Refractory Differentiated Thyroid Cancer in the Era of Thyrosin-Kinases Inhibitors: A Real-Life Retrospective Study. Diagnostics 2022, 12, 506. https://doi.org/10.3390/diagnostics12020506
Gay S, Raffa S, De’Luca di Pietralata A, Bauckneht M, Vera L, Miceli A, Albertelli M, Morbelli S, Giusti M, Ferone D. 2-[18F]FDG PET in the Management of Radioiodine Refractory Differentiated Thyroid Cancer in the Era of Thyrosin-Kinases Inhibitors: A Real-Life Retrospective Study. Diagnostics. 2022; 12(2):506. https://doi.org/10.3390/diagnostics12020506
Chicago/Turabian StyleGay, Stefano, Stefano Raffa, Anna De’Luca di Pietralata, Matteo Bauckneht, Lara Vera, Alberto Miceli, Manuela Albertelli, Silvia Morbelli, Massimo Giusti, and Diego Ferone. 2022. "2-[18F]FDG PET in the Management of Radioiodine Refractory Differentiated Thyroid Cancer in the Era of Thyrosin-Kinases Inhibitors: A Real-Life Retrospective Study" Diagnostics 12, no. 2: 506. https://doi.org/10.3390/diagnostics12020506
APA StyleGay, S., Raffa, S., De’Luca di Pietralata, A., Bauckneht, M., Vera, L., Miceli, A., Albertelli, M., Morbelli, S., Giusti, M., & Ferone, D. (2022). 2-[18F]FDG PET in the Management of Radioiodine Refractory Differentiated Thyroid Cancer in the Era of Thyrosin-Kinases Inhibitors: A Real-Life Retrospective Study. Diagnostics, 12(2), 506. https://doi.org/10.3390/diagnostics12020506