
Bile Acids in Intrahepatic Cholestasis of Pregnancy

 , ,
, ,  and
and
Abstract
1. Introduction
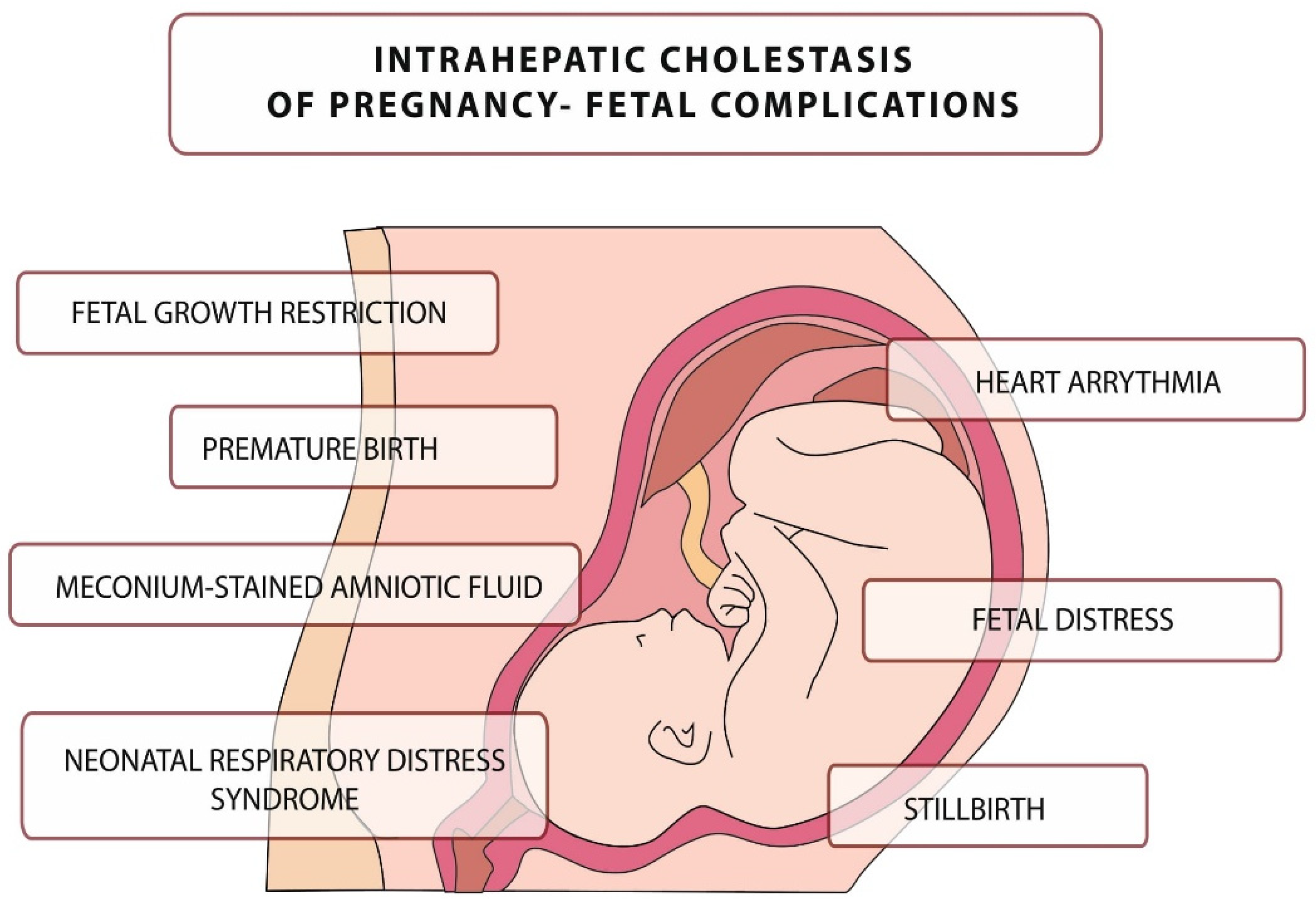
2. Pathophysiology, Etiology, and Complications of ICP
3. Bile Acids
3.1. Synthesis and Enterohepatic Circulation of Bile Acids
3.2. The Biological Role of Bile Acids
- constitute the main important mechanism for the elimination of excess cholesterol through their synthesis and subsequent fecal excretion.
- BAs and phospholipids prevent cholesterol from precipitating in the gallbladder by dissolving cholesterol in the bile.
- they act as emulsifiers, increasing the availability of fats for pancreatic lipases, facilitating the digestion of triacylglycerols in the diet.
3.3. Bile Acids in the Fetus
3.4. Bile Acids in Physiological Pregnancy
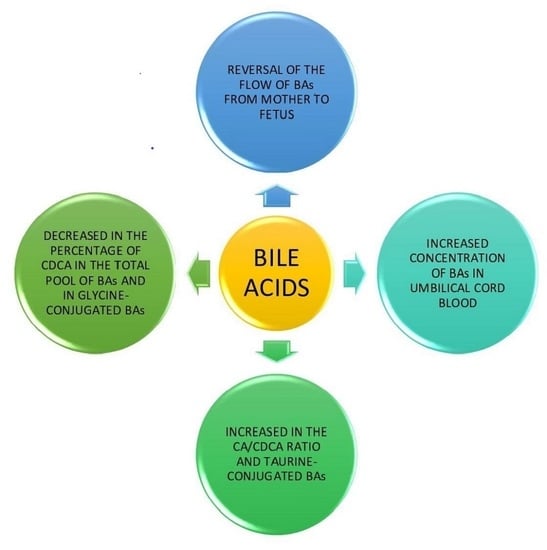
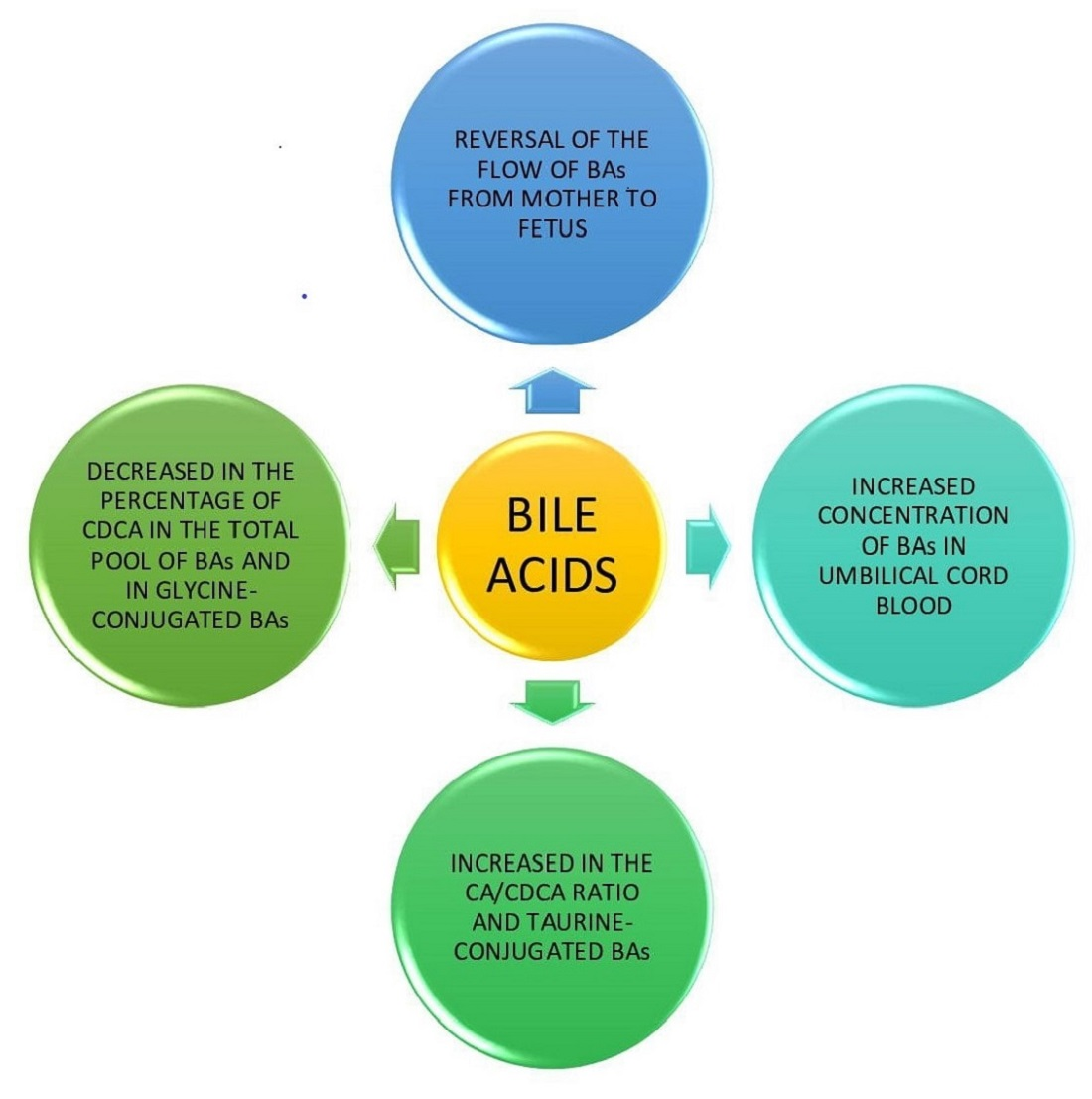
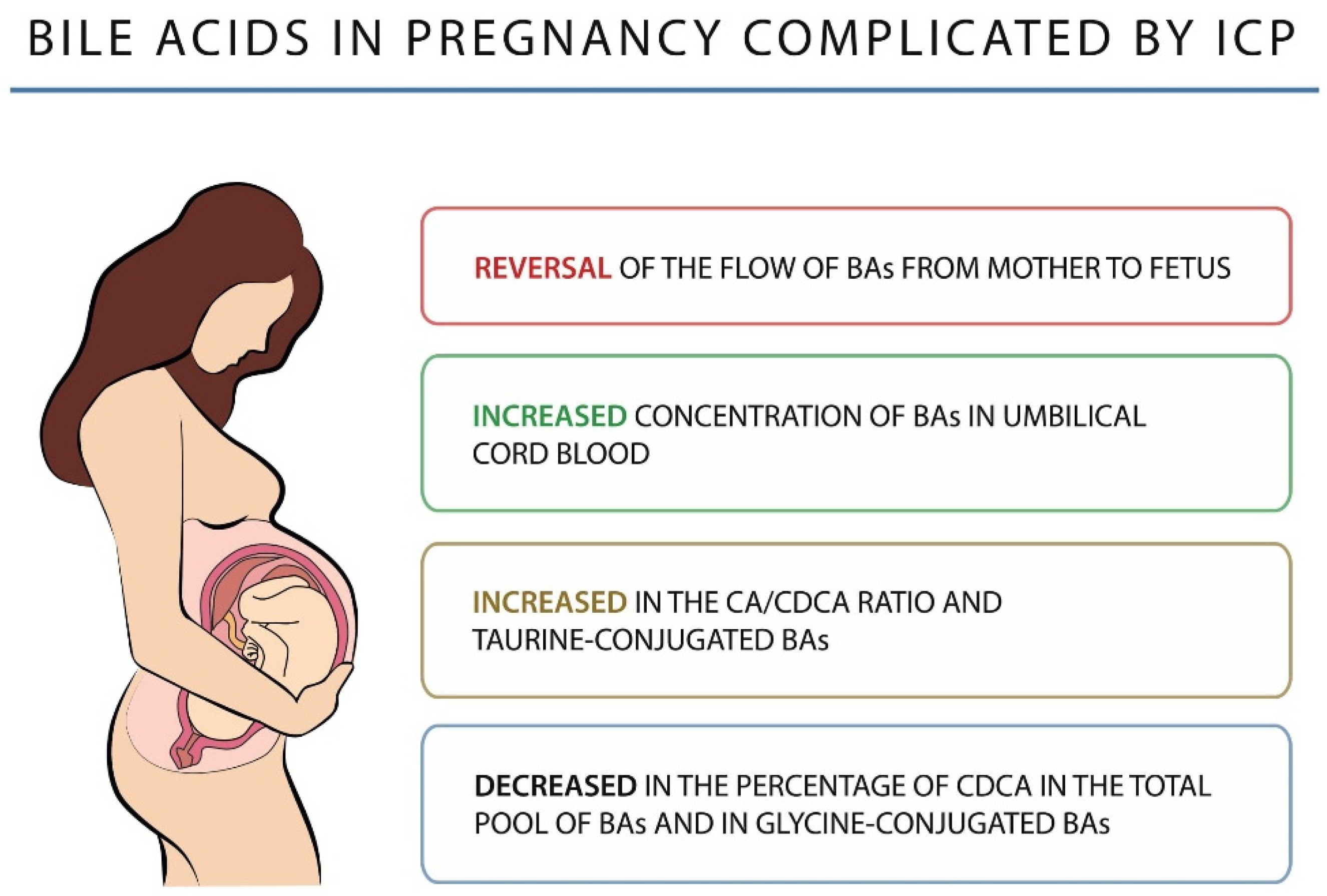
4. Bile Acids in Pregnancy Complicated by ICP
5. Management of ICP
- at the concentration of <40 µmol/L total bile acids, childbirth is recommended between 37 0/7 and 38 6/7 weeks of pregnancy.
- at the concentration of 40–99 µmol/L total bile acids, childbirth is recommended between 36 0/7 and 37 0/7 weeks of pregnancy.
- at the concentration of >100 µmol/L total bile acids, childbirth is recommended in the 36 0/7 week of pregnancy, or earlier in the case of other events or emergency to either the fetus, mother, or both [110].
- contributes to the break-up of micelles in the intestines and reduces the rate of cholesterol absorption
- reduces hepatic synthesis and secretion of cholesterol,
- has a choleretic effect,
- has an anti-apoptotic effect,
- corrects the disturbed kinetics of transplacental bile acid transport in pregnancies complicated with intrahepatic cholestasis during pregnancy,
- reduces the concentration of primary bile acids in the umbilical cord blood and in the amniotic fluid.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Shan, D.; Dong, R.; Hu, Y. Current understanding of autophagy in intrahepatic cholestasis of pregnancy. Placenta 2021, 115, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Westbrook, R.H.; Dusheiko, G.; Williamson, C. Pregnancy and liver disease. J. Hepatol. 2016, 64, 933–945. [Google Scholar] [CrossRef] [PubMed]
- Piechota, J.; Jelski, W. Intrahepatic Cholestasis in Pregnancy: Review of the Literature. J. Clin. Med. 2020, 9, 1361. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, B.; Kimber-Trojnar, Ż.; Leszczyńska-Gorzelak, B.; Patro-Małysza, J.; Trojnar, M.; Oleszczuk, J. Treatment of obstetric cholestasis with polyunsaturated phosphatidylcholine and ursodeoxycholic acid. Ginekol. Pol. 2011, 82, 26–31. [Google Scholar]
- Panaitescu, A.M.; Popescu, M.R.; Ciobanu, A.M.; Gica, N.; Cimpoca-Raptis, B.A. Pregnancy Complications Can Foreshadow Future Disease—Long-Term Outcomes of a Complicated Pregnancy. Medicina 2021, 57, 1320. [Google Scholar] [CrossRef]
- Xiao, J.; Li, Z.; Song, Y.; Sun, Y.; Shi, H.; Chen, D.; Zhang, Y. Molecular Pathogenesis of Intrahepatic Cholestasis of Pregnancy. Can. J. Gastroenterol. Hepatol. 2021, 2021, 6679322. [Google Scholar] [CrossRef]
- Kondrackiene, J.; Kupcinskas, L. Intrahepatic cholestasis of pregnancy-current achievements and unsolved problems. World J. Gastroenterol. 2008, 14, 5781. [Google Scholar] [CrossRef]
- Stulic, M.; Culafic, D.; Boricic, I.; Stojkovic Lalosevic, M.; Pejic, N.; Jankovic, G.; Milovanovic, T.; Culafic-Vojinovic, V.; Vlaisavljevic, Z.; Culafic, M. Intrahepatic Cholestasis of Pregnancy: A Case Study of the Rare Onset in the First Trimester. Medicina 2019, 55, 454. [Google Scholar] [CrossRef]
- Huang, S.; Liu, Y.; Guo, N.; Liu, X.; Li, G.; Du, Q. Serum profiles of inflammatory cytokines associated with intrahepatic cholestasis of pregnancy. J. Matern. Fetal Neonatal Med. 2022, 1–10. [Google Scholar] [CrossRef]
- Varlas, V.N.; Bohîlțea, R.; Gheorghe, G.; Bostan, G.; Angelescu, G.A.; Penes, O.N.; Bors, R.G.; Cloțea, E.; Bacalbasa, N.; Diaconu, C.C. State of the Art in Hepatic Dysfunction in Pregnancy. Healthcare 2021, 9, 1481. [Google Scholar] [CrossRef]
- Lin, Q.X.; Huang, W.W.; Shen, W.; Deng, X.S.; Tang, Z.Y.; Chen, Z.H.; Zhao, W.; Fan, H.Y. Intrahepatic Cholestasis of Pregnancy Increases Inflammatory Susceptibility in Neonatal Offspring by Modulating Gut Microbiota. Front. Immunol. 2022, 13, 889646. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Pan, Y.; Lin, C.; Zheng, Y.; Sun, H.; Zhang, H.; Wang, J.; Yuan, M.; Duan, T.; Du, Q.; et al. Bile acids evoke placental inflammation by activating Gpbar1/NF-κB pathway in intrahepatic cholestasis of pregnancy. J. Mol. Cell. Biol. 2016, 8, 530–541. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.A.; Nishio, A.; Hasan, S.; Wu, L.; Chie, L.; Rehermann, B.; T-Y Lau, D. A rare case of recurrent intrahepatic cholestasis of pregnancy with prolonged postpartum hepatic inflammation despite normalization of bile acid levels. Gastro Hep Adv. 2023, 2, 46–48. [Google Scholar] [CrossRef]
- Biberoglu, E.; Kirbas, A.; Daglar, K.; Kara, O.; Karabulut, E.; Yakut, H.I.; Danisman, N. Role of inflammation in intrahepatic cholestasis of pregnancy. J. Obstet. Gynaecol. Res. 2016, 42, 252–257. [Google Scholar] [CrossRef]
- Evangelakos, I.; Heeren, J.; Verkade, E.; Kuipers, F. Role of bile acids in inflammatory liver diseases. Semin. Immunopathol. 2021, 43, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Holtmann, T.M.; Inzaugarat, M.E.; Knorr, J.; Geisler, L.; Schulz, M.; Bieghs, V.; Frissen, M.; Feldstein, A.E.; Tacke, F.; Trautwein, C.; et al. Bile Acids Activate NLRP3 Inflammasome, Promoting Murine Liver Inflammation or Fibrosis in a Cell Type-Specific Manner. Cells 2021, 10, 2618. [Google Scholar] [CrossRef]
- Kawase, A.; Hatanaka, M.; Matsuda, N.; Shimada, H.; Iwaki, M. Slc25a39 and Slc25a40 Expression in Mice with Bile Duct Ligation or Lipopolysaccharide Treatment. Int. J. Mol. Sci. 2022, 23, 8573. [Google Scholar] [CrossRef] [PubMed]
- Wongjarupong, N.; Bharmal, S.; Lim, N. Never Too Soon: An Unusual Case of Intrahepatic Cholestasis of Pregnancy at Five Weeks Gestation. Cureus 2020, 12, e10540. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.; Kathirvel, R.; Mathur, M. Rare case of obstetric cholestasis presenting in the first trimester following in vitro fertilisation. BMJ Case Rep. 2021, 14, e244254. [Google Scholar] [CrossRef]
- Salame, A.A.; Jaffal, M.J.; Mouanness, M.A.; Nasser Eddin, A.R.; Ghulmiyyah, L.M. Unexplained First Trimester Intrahepatic Cholestasis of Pregnancy: A Case Report and Literature Review. Case Rep. Obstet. Gynecol. 2019, 2019, 4980610. [Google Scholar] [CrossRef]
- Hubschmann, A.G.; Orzechowski, K.M.; Berghella, V. Severe First Trimester Recurrent Intrahepatic Cholestasis of Pregnancy: A Case Report and Literature Review. AJP Rep. 2016, 6, 38–41. [Google Scholar]
- Mutlu, M.F.; Aslan, K.; Guler, I.; Mutlu, I.; Erdem, M.; Bozkurt, N.; Erdem, A. Two cases of first onset intrahepatic cholestasis of pregnancy associated with moderate ovarian hyperstimulation syndrome after IVF treatment and review of the literature. J. Obstet. Gynaecol. 2017, 37, 547. [Google Scholar] [CrossRef]
- Mikucka-Niczyporuk, A.; Pierzynski, P.; Lemancewicz, A.; Kosinski, P.; Charkiewicz, K.; Knas, M.; Kacerovsky, M.; Blachnio-Zabielska, A.; Laudanski, P. Role of sphingolipids in the pathogenesis of intrahepatic cholestasis. Prostaglandins Other Lipid Mediat. 2020, 147, 106399. [Google Scholar] [CrossRef] [PubMed]
- Manzotti, C.; Casazza, G.; Stimac, T.; Nikolova, D.; Gluud, C. Total serum bile acids or serum bile acid profile, or both, for the diagnosis of intrahepatic cholestasis of pregnancy. Cochrane Database Syst. Rev. 2019, 7, CD012546. [Google Scholar] [CrossRef] [PubMed]
- Yurtcu, N.; Caliskan, C.S.; Guvey, H.; Celik, S.; Hatirnaz, S.; Tinelli, A. Predictive and Diagnostic Value of Serum Adipokines in Pregnant Women with Intrahepatic Cholestasis. Int. J. Environ. Res. Public Health 2022, 19, 2254. [Google Scholar] [CrossRef]
- Berg, B.; Helm, G.; Petersohn, L.; Tryding, N. Cholestasis of pregnancy. Clinical and laboratory studies. Acta Obstet. Gynecol. Scand. 1986, 65, 107–113. [Google Scholar] [CrossRef]
- Brites, D.; Rodrigues, C.M.; van-Zeller, H.; Brito, A.; Silva, R. Relevance of serum bile acid profile in the diagnosis of intrahepatic cholestasis of pregnancy in an high incidence area: Portugal. Eur. J. Obstet. Gynecol. Reprod. Biol. 1998, 80, 31–38. [Google Scholar] [CrossRef]
- Hagenbeck, C.; Hamza, A.; Kehl, S.; Maul, H.; Lammert, F.; Keitel, V.; Hütten, M.C.; Pecks, U. Management of Intrahepatic Cholestasis of Pregnancy: Recommendations of the Working Group on Obstetrics and Prenatal Medicine-Section on Maternal Disorders. Geburtshilfe Frauenheilkd. 2021, 81, 922–939. [Google Scholar] [CrossRef]
- Heinonen, S.; Kirkinen, P. Pregnancy outcome with intrahepatic cholestasis. Obstet. Gynecol. 1999, 94, 189–193. [Google Scholar]
- Marschall, H.U.; Shemer, E.W.; Ludvigsson, J.F.; Stephansson, O. Intrahepatic cholestasis of pregnancy and associated hepatobiliary disease: A population-based cohort study. Hepatology 2013, 58, 1385–1391. [Google Scholar] [CrossRef]
- Gonzalez, M.C.; Reyes, H.; Arrese, M.; Figueroa, D.; Lorca, B.; Andresen, M.; Segovia, N.; Molina, C.; Arce, S. Intrahepatic cholestasis of pregnancy in twin pregnancies. J. Hepatol. 1989, 9, 84–90. [Google Scholar] [CrossRef]
- Koivurova, S.; Hartikainen, A.L.; Karinen, L.; Gissler, M.; Hemminki, E.; Martikainen, H.; Tuomivaara, L.; Järvelin, M.R. The course of pregnancy and delivery and the use of maternal healthcare services after standard IVF in Northern Finland 1990. Hum. Reprod. 2002, 17, 2897–2903. [Google Scholar] [CrossRef] [PubMed]
- Floreani, A.; Gervasi, M.T. New Insights on Intrahepatic Cholestasis of Pregnancy. Clin. Liver Dis. 2016, 20, 177. [Google Scholar] [CrossRef]
- Pařízek, A.; Dušková, M.; Vítek, L.; Šrámková, M.; Hill, M.; Adamcová, K.; Šimják, P.; Černý, A.; Kordová, Z.; Vráblíková, H.; et al. The role of steroid hormones in the development of intrahepatic cholestasis of pregnancy. Physiol. Res. 2015, 64, S203–S209. [Google Scholar] [CrossRef] [PubMed]
- Ovadia, C.; Seed, P.T.; Sklavounos, A.; Geenes, V.; Di Ilio, C.; Chambers, J.; Kohari, K.; Bacq, Y.; Bozkurt, N.; Brun-Furrer, R.; et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: Results of aggregate and individual patient data meta-analyses. Lancet 2019, 393, 899–909. [Google Scholar] [CrossRef]
- Wang, J.; Lun, W.; Shi, W. Effects of elevated bile acid levels on fetal myocardium in intrahepatic cholestasis of pregnancy, a retrospective study from a neonatal perspective. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 102013. [Google Scholar] [CrossRef]
- Çelik, S.; Çalışkan, C.S.; Çelik, H.; Güçlü, M.; Başbuğ, A. Predictors of adverse perinatal outcomes in intrahepatic cholestasis of pregnancy. Ginekol. Pol. 2019, 90, 217–222. [Google Scholar] [CrossRef]
- Di Mascio, D.; Quist-Nelson, J.; Riegel, M.; George, B.; Saccone, G.; Brun, R.; Haslinger, C.; Herrera, C.; Kawakita, T.; Lee, R.H.; et al. Perinatal death by bile acid levels in intrahepatic cholestasis of pregnancy: A systematic review. J. Matern. Fetal Neonatal Med. 2021, 34, 3614–3622. [Google Scholar] [CrossRef]
- Rodriguez, M.; Bombin, M.; Ahumada, H.; Bachmann, M.; Egaña-Ugrinovic, G.; Sepúlveda-Martínez, A. Fetal cardiac dysfunction in pregnancies affected by intrahepatic cholestasis of pregnancy: A cohort study. J. Obstet. Gynaecol. Res. 2022, 48, 1658–1667. [Google Scholar] [CrossRef]
- Sarker, M.; Zamudio, A.R.; DeBolt, C.; Ferrara, L. Beyond stillbirth: Association of intrahepatic cholestasis of pregnancy severity and adverse outcomes. Am. J. Obstet. Gynecol. 2022, 227, 517.e1–517.e517. [Google Scholar] [CrossRef]
- Devalla, A.; Srivastava, K. Unfolding newer concepts in placental pathology of obstetric cholestasis-a cause for prematurity. Int. J. Physiol. Pathophysiol. Pharmacol. 2022, 14, 16–23. [Google Scholar] [PubMed]
- Blumenfeld, J.; Koo, K. Navigating Uncertainty: A Case Study of Intrahepatic Cholestasis of Pregnancy. J. Midwifery Womens Health 2022, 67, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Huri, M.; Seravalli, V.; Lippi, C.; Tofani, L.; Galli, A.; Petraglia, F.; Di Tommaso, M. Intrahepatic cholestasis of pregnancy-Time to redefine the reference range of total serum bile acids: A cross-sectional study. BJOG Int. J. Obstet. Gynaecol. 2022, 129, 1887–1896. [Google Scholar] [CrossRef]
- Seyed Khoei, N.; Anton, G.; Peters, A.; Freisling, H.; Wagner, K.-H. The Association between Serum Bilirubin Levels and Colorectal Cancer Risk: Results from the Prospective Cooperative Health Research in the Region of Augsburg (KORA) Study in Germany. Antioxidants 2020, 9, 908. [Google Scholar] [CrossRef]
- Shulpekova, Y.; Shirokova, E.; Zharkova, M.; Tkachenko, P.; Tikhonov, I.; Stepanov, A.; Sinitsyna, A.; Izotov, A.; Butkova, T.; Shulpekova, N.; et al. A Recent Ten-Year Perspective: Bile Acid Metabolism and Signaling. Molecules 2022, 27, 1983. [Google Scholar] [CrossRef]
- Smith, D.D.; Kiefer, M.K.; Lee, A.J.; Davis, S.B.; Summerfield, T.L.; Landon, M.B.; Rood, K.M. Effect of Fasting on Total Bile Acid Levels in Pregnancy. Obstet. Gynecol. 2020, 136, 1204–1210. [Google Scholar] [CrossRef]
- Smith, D.D.; Rood, K.M. Intrahepatic Cholestasis of Pregnancy. Clin. Obstet. Gynecol. 2020, 63, 134–151. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.M.; Gowda, M.; Donnelly, J.G. Bile acid ratio in diagnosis of intrahepatic cholestasis of pregnancy. Am. J. Perinatol. 2009, 26, 291–294. [Google Scholar] [CrossRef]
- Adams, A.; Jacobs, K.; Vogel, R.; Lupo, V. Bile acid determination after standardized glucose load in pregnant women. Am. J. Perinatol. Rep. 2015, 5, e168–e171. [Google Scholar]
- Haange, S.-B.; Till, A.; Bergh, P.-O.; Fauler, G.; Gigl, M.; Löfgren-Sandblom, A.; Schaap, F.G.; Clavel, T.; Trautwein, C.; Fenske, W.; et al. Ring Trial on Quantitative Assessment of Bile Acids Reveals a Method- and Analyte-Specific Accuracy and Reproducibility. Metabolites 2022, 12, 583. [Google Scholar] [CrossRef]
- Zhang, B.; Kuipers, F.; de Boer, J.F.; Kuivenhoven, J.A. Modulation of Bile Acid Metabolism to Improve Plasma Lipid and Lipoprotein Profiles. J. Clin. Med. 2022, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.M.; DeMorrow, S. Bile Acid Signaling in Neurodegenerative and Neurological Disorders. Int. J. Mol. Sci. 2020, 21, 5982. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.Y.L.; Ferrell, J.M. Up to date on cholesterol 7 alpha-hydroxylase (CYP7A1) in bile acid synthesis. Liver Res. 2020, 4, 47–63. [Google Scholar] [CrossRef]
- Tagawa, R.; Kobayashi, M.; Sakurai, M.; Yoshida, M.; Kaneko, H.; Mizunoe, Y.; Nozaki, Y.; Okita, N.; Sudo, Y.; Higami, Y. Long-Term Dietary Taurine Lowers Plasma Levels of Cholesterol and Bile Acids. Int. J. Mol. Sci. 2022, 23, 1793. [Google Scholar] [CrossRef] [PubMed]
- Phelps, T.; Snyder, E.; Rodriguez, E.; Child, H.; Harvey, P. The influence of biological sex and sex hormones on bile acid synthesis and cholesterol homeostasis. Biol. Sex Differ. 2019, 10, 52. [Google Scholar] [CrossRef]
- Chiang, J.Y. Bile acid metabolism and signaling. Compr. Physiol. 2013, 3, 1191–1212. [Google Scholar]
- Boyer, J.L.; Soroka, C.J. Bile formation and secretion: An update. J. Hepatol. 2021, 75, 190–201. [Google Scholar] [CrossRef]
- Durník, R.; Šindlerová, L.; Babica, P.; Jurček, O. Bile Acids Transporters of Enterohepatic Circulation for Targeted Drug Delivery. Molecules 2022, 27, 2961. [Google Scholar] [CrossRef]
- Wang, H.H.; Portincasa, P.; Wang, D.Q. Update on the Molecular Mechanisms Underlying the Effect of Cholecystokinin and Cholecystokinin-1 Receptor on the Formation of Cholesterol Gallstones. Curr. Med. Chem. 2019, 26, 3407–3423. [Google Scholar] [CrossRef]
- Poland, J.C.; Flynn, C.R. Bile Acids, Their Receptors, and the Gut Microbiota. Physiology 2021, 36, 235–245. [Google Scholar] [CrossRef]
- Jia, W.; Xie, G.; Jia, W. Bile acid-microbiota crosstalk in gastrointestinal inflammation and carcinogenesis. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 111–128. [Google Scholar] [CrossRef] [PubMed]
- An, C.; Chon, H.; Ku, W.; Eom, S.; Seok, M.; Kim, S.; Lee, J.; Kim, D.; Lee, S.; Koo, H.; et al. Bile Acids: Major Regulator of the Gut Microbiome. Microorganisms 2022, 10, 1792. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Sun, L.; Gonzalez, F.J. Gut microbiota-derived bile acids in intestinal immunity, inflammation, and tumorigenesis. Cell Host Microbe 2022, 30, 289–300. [Google Scholar] [CrossRef]
- Grüner, N.; Mattner, J. Bile Acids and Microbiota: Multifaceted and Versatile Regulators of the Liver–Gut Axis. Int. J. Mol. Sci. 2021, 22, 1397. [Google Scholar] [CrossRef]
- Slijepcevic, D.; van de Graaf, S.F. Bile Acid Uptake Transporters as Targets for Therapy. Dig. Dis. 2017, 35, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Mertens, K.L.; Kalsbeek, A.; Soeters, M.R.; Eggink, H.M. Bile Acid Signaling Pathways from the Enterohepatic Circulation to the Central Nervous System. Front. Neurosci. 2017, 11, 617. [Google Scholar] [CrossRef] [PubMed]
- Shulpekova, Y.; Zharkova, M.; Tkachenko, P.; Tikhonov, I.; Stepanov, A.; Synitsyna, A.; Izotov, A.; Butkova, T.; Shulpekova, N.; Lapina, N.; et al. The Role of Bile Acids in the Human Body and in the Development of Diseases. Molecules 2022, 27, 3401. [Google Scholar] [CrossRef]
- Režen, T.; Rozman, D.; Kovács, T.; Kovács, P.; Sipos, A.; Bai, P.; Mikó, E. The role of bile acids in carcinogenesis. Cell. Mol. Life Sci. 2022, 79, 243. [Google Scholar] [CrossRef]
- di Gregorio, M.C.; Cautela, J.; Galantini, L. Physiology and Physical Chemistry of Bile Acids. Int. J. Mol. Sci. 2021, 22, 1780. [Google Scholar] [CrossRef]
- Caliceti, C.; Punzo, A.; Silla, A.; Simoni, P.; Roda, G.; Hrelia, S. New Insights into Bile Acids Related Signaling Pathways in the Onset of Colorectal Cancer. Nutrients 2022, 14, 2964. [Google Scholar] [CrossRef]
- Ðanić, M.; Stanimirov, B.; Pavlović, N.; Goločorbin-Kon, S.; Al-Salami, H.; Stankov, K.; Mikov, M. Pharmacological Applications of Bile Acids and Their Derivatives in the Treatment of Metabolic Syndrome. Front. Pharmacol. 2018, 9, 1382. [Google Scholar] [CrossRef] [PubMed]
- Trauner, M.; Fuchs, C.D. Novel therapeutic targets for cholestatic and fatty liver disease. Gut 2022, 71, 194–209. [Google Scholar] [CrossRef]
- Zhao, L.; Xuan, Z.; Song, W.; Zhang, S.; Li, Z.; Song, G.; Zhu, X.; Xie, H.; Zheng, S.; Song, P. A novel role for farnesoid X receptor in the bile acid-mediated intestinal glucose homeostasis. J. Cell. Mol. Med. 2020, 24, 12848–12861. [Google Scholar] [CrossRef] [PubMed]
- Massafra, V.; van Mil, S.W.C. Farnesoid X receptor: A "homeostat" for hepatic nutrient metabolism. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 45–59. [Google Scholar] [CrossRef]
- Stofan, M.; Guo, G.L. Bile Acids and FXR: Novel Targets for Liver Diseases. Front. Med. 2020, 7, 544. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lou, G.; Meng, Z.; Huang, W. TGR5: A novel target for weight maintenance and glucose metabolism. Exp. Diabetes Res. 2011, 2011, 853501. [Google Scholar] [CrossRef]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Sáez, M.A.; Álvarez-Mon, M.A.; Torres-Carranza, D.; Álvarez-Mon, M.; Bujan, J.; García-Honduvilla, N.; Bravo, C.; et al. The Pivotal Role of the Placenta in Normal and Pathological Pregnancies: A Focus on Preeclampsia, Fetal Growth Restriction, and Maternal Chronic Venous Disease. Cells 2022, 11, 568. [Google Scholar] [CrossRef]
- Wojczakowski, W.; Kimber-Trojnar, Ż.; Dziwisz, F.; Słodzińska, M.; Słodziński, H.; Leszczyńska-Gorzelak, B. Preeclampsia and Cardiovascular Risk for Offspring. J. Clin. Med. 2021, 10, 3154. [Google Scholar] [CrossRef]
- Yañez, M.J.; Leiva, A. Human Placental Intracellular Cholesterol Transport: A Focus on Lysosomal and Mitochondrial Dysfunction and Oxidative Stress. Antioxidants 2022, 11, 500. [Google Scholar] [CrossRef]
- Nikolov, A.; Popovski, N. Role of Gelatinases MMP-2 and MMP-9 in Healthy and Complicated Pregnancy and Their Future Potential as Preeclampsia Biomarkers. Diagnostics 2021, 11, 480. [Google Scholar] [CrossRef]
- Wang, P.; Song, Y.; Zhong, H.; Lin, S.; Zhang, X.; Li, J.; Che, L.; Feng, B.; Lin, Y.; Xu, S.; et al. Transcriptome Profiling of Placenta through Pregnancy Reveals Dysregulation of Bile Acids Transport and Detoxification Function. Int. J. Mol. Sci. 2019, 20, 4099. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, M.; Trottier, J.; Weisnagel, S.J.; Gagnon, C.; Carreau, A.M.; Barbier, O.; Morisset, A.S. Bile acids during pregnancy: Trimester variations and associations with glucose homeostasis. Health Sci. Rep. 2021, 4, e243. [Google Scholar] [CrossRef] [PubMed]
- Ronin-Walknowska, E. Cholestaza ciężarnych-choroba niedoceniona. Przegląd piśmiennictwa. Perinatol. Neonatol. Ginekol. 2010, 3, 165–174. [Google Scholar]
- Fan, H.M.; Mitchell, A.L.; Williamson, C. ENDOCRINOLOGY in PREGNANCY: Metabolic impact of bile acids in gestation. Eur. J. Endocrinol. 2021, 184, R69–R83. [Google Scholar] [CrossRef] [PubMed]
- Pataia, V.; Dixon, P.H.; Williamson, C. Pregnancy and bile acid disorders. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 313, G1–G6. [Google Scholar] [CrossRef]
- Ontsouka, E.; Epstein, A.; Kallol, S.; Zaugg, J.; Baumann, M.; Schneider, H.; Albrecht, C. Placental Expression of Bile Acid Transporters in Intrahepatic Cholestasis of Pregnancy. Int. J. Mol. Sci. 2021, 22, 10434. [Google Scholar] [CrossRef]
- McIlvride, S.; Dixon, P.H.; Williamson, C. Bile acids and gestation. Mol. Aspects Med. 2017, 56, 90–100. [Google Scholar] [CrossRef]
- Kroll, T.; Prescher, M.; Smits, S.H.J.; Schmitt, L. Structure and Function of Hepatobiliary ATP Binding Cassette Transporters. Chem. Rev. 2021, 121, 5240–5288. [Google Scholar] [CrossRef]
- Heikkinen, J.; Mäentausta, O.; Ylöstalo, P.; Jänne, O. Changes in serum bile acid concentrations during normal pregnancy, in patients with intrahepatic cholestasis of pregnancy and in pregnant women with itching. Br. J. Obstet. Gynaecol. 1981, 88, 240–245. [Google Scholar] [CrossRef]
- Lunzer, M.; Barnes, P.; Byth, K.; O’Halloran, M. Serum bile acid concentrations during pregnancy and their relationship to obstetric cholestasis. Gastroenterology 1986, 91, 825–829. [Google Scholar] [CrossRef]
- He, Y.; Zhang, X.; Shao, Y.; Xu, B.; Cui, Y.; Chen, X.; Chen, H.; Luo, C.; Ding, M. Recognition of asymptomatic hypercholanemia of pregnancy: Different clinical features, fetal outcomes and bile acids metabolism from intrahepatic cholestasis of pregnancy. Biochim. Biophys. Acta Mol. Basis Dis. 2022, 1868, 166269. [Google Scholar] [CrossRef] [PubMed]
- Pascual, M.J.; Serrano, M.A.; El-Mir, M.Y.; Macias, R.I.; Jiménez, F.; Marin, J.J. Relationship between asymptomatic hypercholanaemia of pregnancy and progesterone metabolism. Clin. Sci. 2002, 102, 587–593. [Google Scholar] [CrossRef]
- Walker, K.F.; Chappell, L.C.; Hague, W.M.; Middleton, P.; Thornton, J.G. Pharmacological interventions for treating intrahepatic cholestasis of pregnancy. Cochrane Database Syst. Rev. 2020, 7, CD000493. [Google Scholar] [PubMed]
- Bicocca, M.J.; Sperling, J.D.; Chauhan, S.P. Intrahepatic cholestasis of pregnancy: Review of six national and regional guidelines. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 231, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Geenes, V.; Chappell, L.C.; Seed, P.T.; Steer, P.J.; Knight, M.; Williamson, C. Association of severe intrahepatic cholestasis of pregnancy with adverse pregnancy outcomes: A prospective population-based case-control study. Hepatology 2014, 59, 1482–1491. [Google Scholar] [CrossRef]
- Wood, A.M.; Livingston, E.G.; Hughes, B.L.; Kuller, J.A. Intrahepatic cholestasis of pregnancy: A review of diagnosis and management. Obstet. Gynecol. Surv. 2018, 73, 103–109. [Google Scholar] [CrossRef]
- Jurate, K.; Rimantas, Z.; Jolanta, S.; Vladas, G.; Limas, K. Sensitivity and specificity of biochemical tests for diagnosis of intrahepatic cholestasis of pregnancy. Ann. Hepatol. 2017, 16, 569–573. [Google Scholar] [CrossRef]
- Girling, J.; Knight, C.L.; Chappell, L. Royal College of Obstetricians and Gynaecologists. Intrahepatic cholestasis of pregnancy: Green-top Guideline No. 43 June 2022. BJOG Int. J. Obstet. Gynaecol. 2022. [Google Scholar] [CrossRef]
- Society for Maternal-Fetal Medicine (SMFM); Lee, R.H.; Greenberg, M.; Metz, T.D.; Pettker, C.M. Society for Maternal-Fetal Medicine Consult Series #53: Intrahepatic cholestasis of pregnancy: Replaces Consult #13, April 2011. Am. J. Obstet. Gynecol. 2021, 224, B2–B9. [Google Scholar]
- South Australian Perinatal Practice Guideline. Intrahepatic Cholestasis of Pregnancy. Available online: https://www.sahealth.sa.gov.au/wps/wcm/connect/f91fbf004ee530b2a5ebadd150ce4f37/Intrahepatic+cholestasis+of+pregnancy_PPG_v4_0.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-f91fbf004ee530b2a5ebadd150ce4f37-ocQJ9qe (accessed on 4 November 2022).
- Leszczyńska-Gorzelak, B.; Oleszczuk, J.; Maciniak, B.; Poręba, R.; Oszukowski, P.; Wielgoś, M.; Czajkowski, K.; Zespoł Ekspertów Polskiego Towarzystwa Ginekologicznego. Clinical practice guidelines of the Team of Experts of the Polish Gynecological Society: Management of the intrahepatic cholestasis of pregnancy. Ginekol. Pol. 2012, 83, 713–717. [Google Scholar]
- Lu, L.; Chinese Society of Hepatology and Chinese Medical Association. Guidelines for the Management of Cholestatic Liver Diseases (2021). J. Clin. Transl. Hepatol. 2022, 10, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Laatikainen, T.; Karjalainen, O. Excertion of progesterone metabolites in urine and bile of pregnant women with intrahepatic cholestasis. J. Steroid Biochem. 1973, 4, 641–648. [Google Scholar] [CrossRef]
- Macias, R.I.; Pascual, M.J.; Bravo, A.; Alcalde, M.P.; Larena, M.G.; St-Pierre, M.V.; Serrano, M.A.; Marin, J.J. Effect of maternal cholestasis on bile acid transfer across the rat placenta-maternal liver tandem. Hepatology 2000, 31, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Serrano, M.A.; Brites, D.; Larena, M.G.; Monte, M.J.; Bravo, M.P.; Oliveira, N.; Marin, J.J. Beneficial effect of ursodeoxycholic acid on alterations induced by cholestasis of pregnancy in bile acid transport across the human placenta. J. Hepatol. 1998, 28, 829–839. [Google Scholar] [CrossRef]
- Howard, P.J.; Murphy, G.M. Bile acid stress in the mother and baby unit. Eur. J. Gastroenterol. Hepatol. 2003, 15, 317–321. [Google Scholar] [CrossRef]
- Borges Manna, L.; Papacleovoulou, G.; Flaviani, F.; Pataia, V.; Qadri, A.; Abu-Hayyeh, S.; McIlvride, S.; Jansen, E.; Dixon, P.; Chambers, J.; et al. Ursodeoxycholic acid improves feto-placental and offspring metabolic outcomes in hypercholanemic pregnancy. Sci. Rep. 2020, 10, 10361. [Google Scholar] [CrossRef]
- Martinefski, M.R.; Cocucci, S.E.; Di Carlo, M.B.; Vega, H.R.; Lucangioli, S.E.; Perazzi, B.E.; Tripodi, V.P. Fetal coenzyme Q10 deficiency in intrahepatic cholestasis of pregnancy. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 368–374. [Google Scholar] [CrossRef]
- Heikkinen, J. Serum bile acids in the early diagnosis of intrahepatic cholestasis of pregnancy. Obstet. Gynecol. 1983, 61, 581–587. [Google Scholar]
- UpToDate. Intrahepatic Cholestasis of Pregnancy. Available online: https://www.uptodate.com/contents/intrahepatic-cholestasis-of-pregnancy?search=cholestasis%20in%20pregnancy&source=search_result&selectedTitle=1~64&usage_type=default&display_rank=1#H21 (accessed on 4 November 2022).
- Williamson, C.; Geenes, V. Intrahepatic cholestasis of pregnancy. Obstet. Gynecol. 2014, 124, 120–133. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Guidelines | Bile Acids | Reference |
|---|---|---|
| RCOG | >19 μmol/L | [98] |
| SMFM | >10 μmol/L | [99] |
| SAPPG | >19 μmol/L | [100] |
| PGS | >10 μmol/L | [101] |
| ChSH and ChMA | >10 μmol/L | [102] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Majsterek, M.; Wierzchowska-Opoka, M.; Makosz, I.; Kreczyńska, L.; Kimber-Trojnar, Ż.; Leszczyńska-Gorzelak, B. Bile Acids in Intrahepatic Cholestasis of Pregnancy. Diagnostics 2022, 12, 2746. https://doi.org/10.3390/diagnostics12112746
Majsterek M, Wierzchowska-Opoka M, Makosz I, Kreczyńska L, Kimber-Trojnar Ż, Leszczyńska-Gorzelak B. Bile Acids in Intrahepatic Cholestasis of Pregnancy. Diagnostics. 2022; 12(11):2746. https://doi.org/10.3390/diagnostics12112746
Chicago/Turabian StyleMajsterek, Maciej, Magdalena Wierzchowska-Opoka, Inga Makosz, Lena Kreczyńska, Żaneta Kimber-Trojnar, and Bożena Leszczyńska-Gorzelak. 2022. "Bile Acids in Intrahepatic Cholestasis of Pregnancy" Diagnostics 12, no. 11: 2746. https://doi.org/10.3390/diagnostics12112746
APA StyleMajsterek, M., Wierzchowska-Opoka, M., Makosz, I., Kreczyńska, L., Kimber-Trojnar, Ż., & Leszczyńska-Gorzelak, B. (2022). Bile Acids in Intrahepatic Cholestasis of Pregnancy. Diagnostics, 12(11), 2746. https://doi.org/10.3390/diagnostics12112746