

Myofascial Pain Syndrome in Women with Primary Dysmenorrhea: A Case-Control Study

 ,
,  , and
, and 
Abstract
1. Introduction
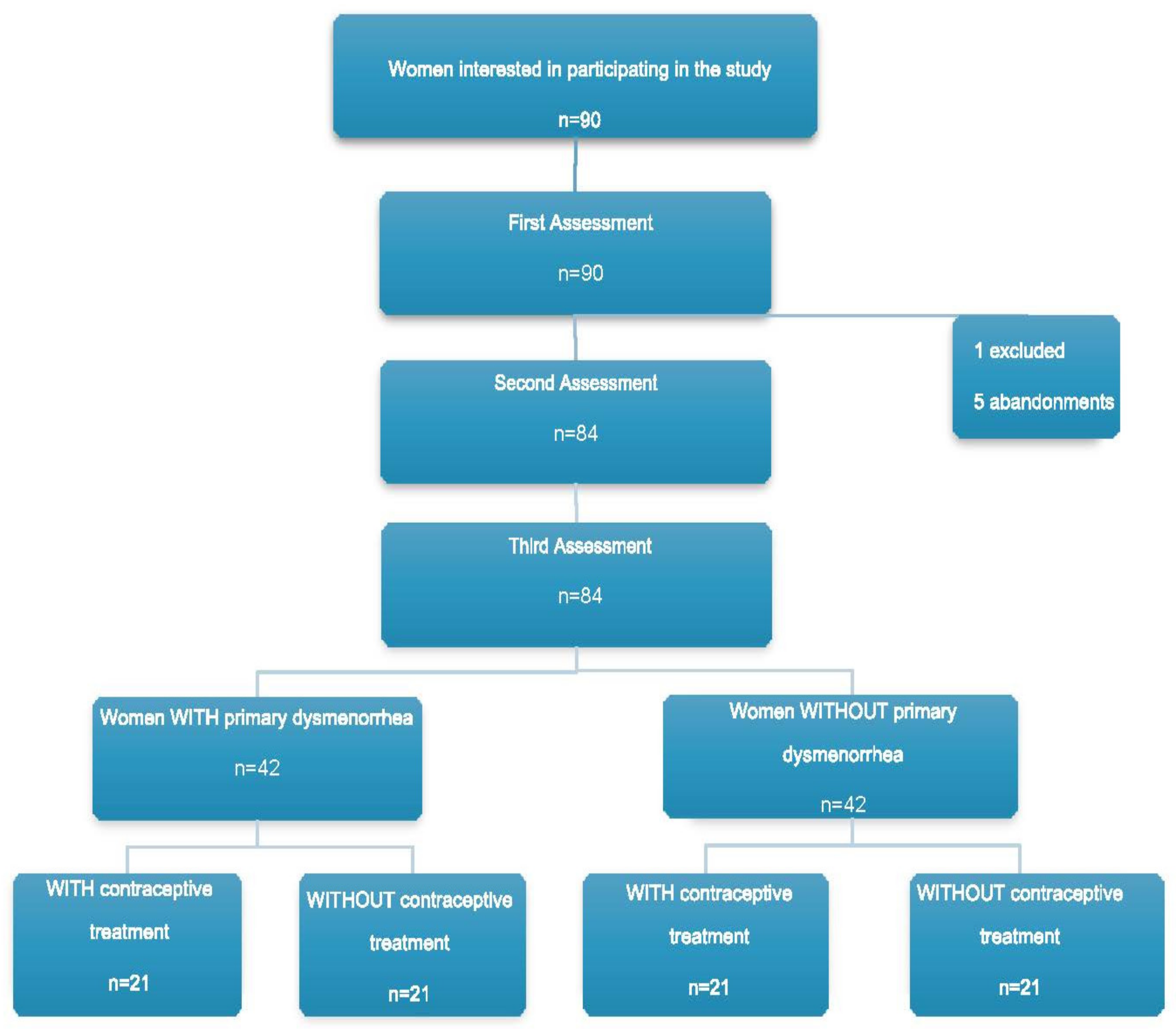
2. Material and Methods
2.1. Procedures, Variables and Assessments
2.2. Sample Size Calculation
2.3. Statistical Analysis
3. Results
3.1. Demographics
3.2. Quality of Life
3.3. Pain
3.3.1. The McGill Pain Questionnaire
3.3.2. Visual Analog Scale
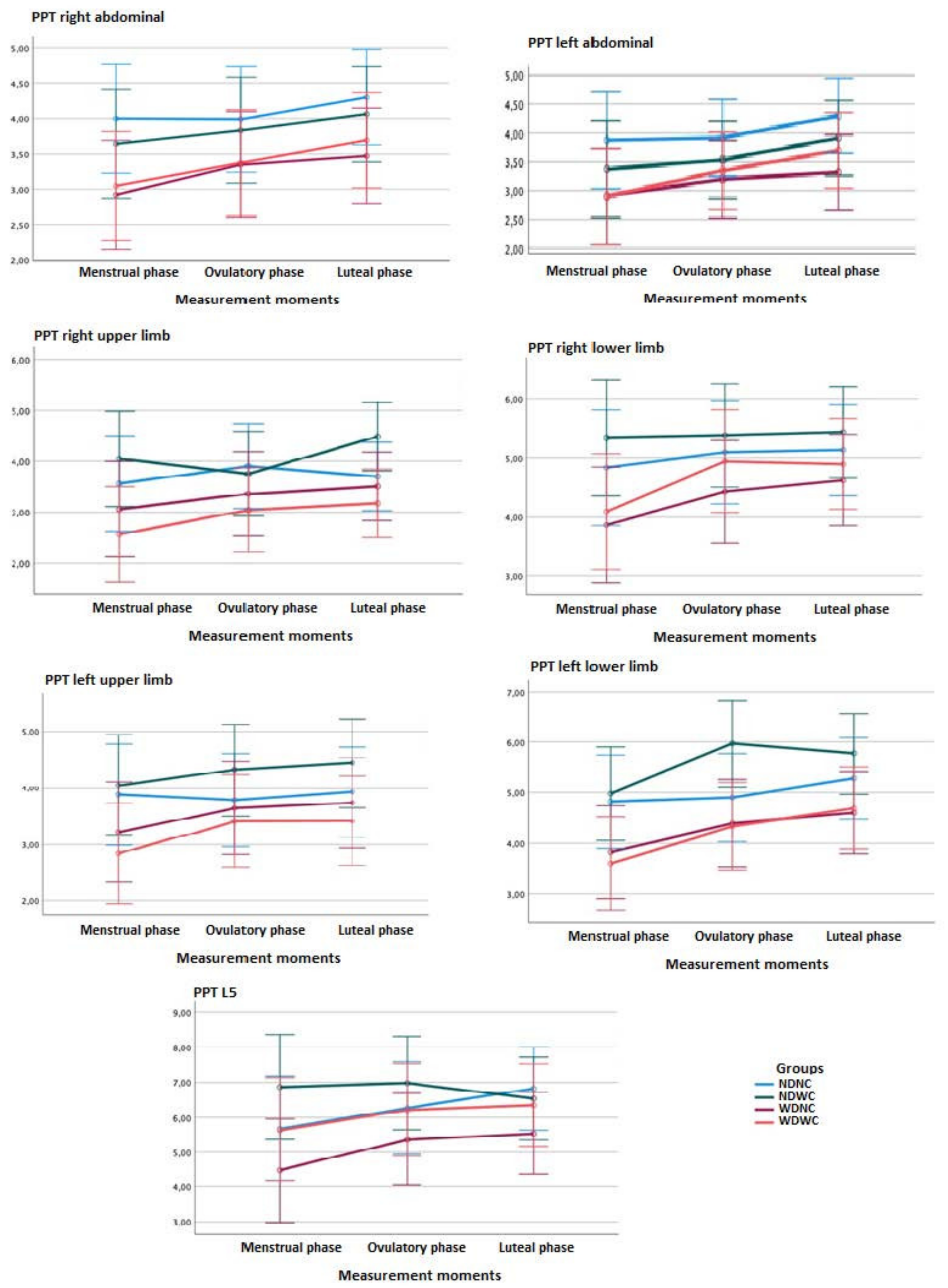
3.4. Mechanosensitivity
3.4.1. Between-Group Comparisons
3.4.2. Within-Group Comparisons
3.5. Presence of MTrPs
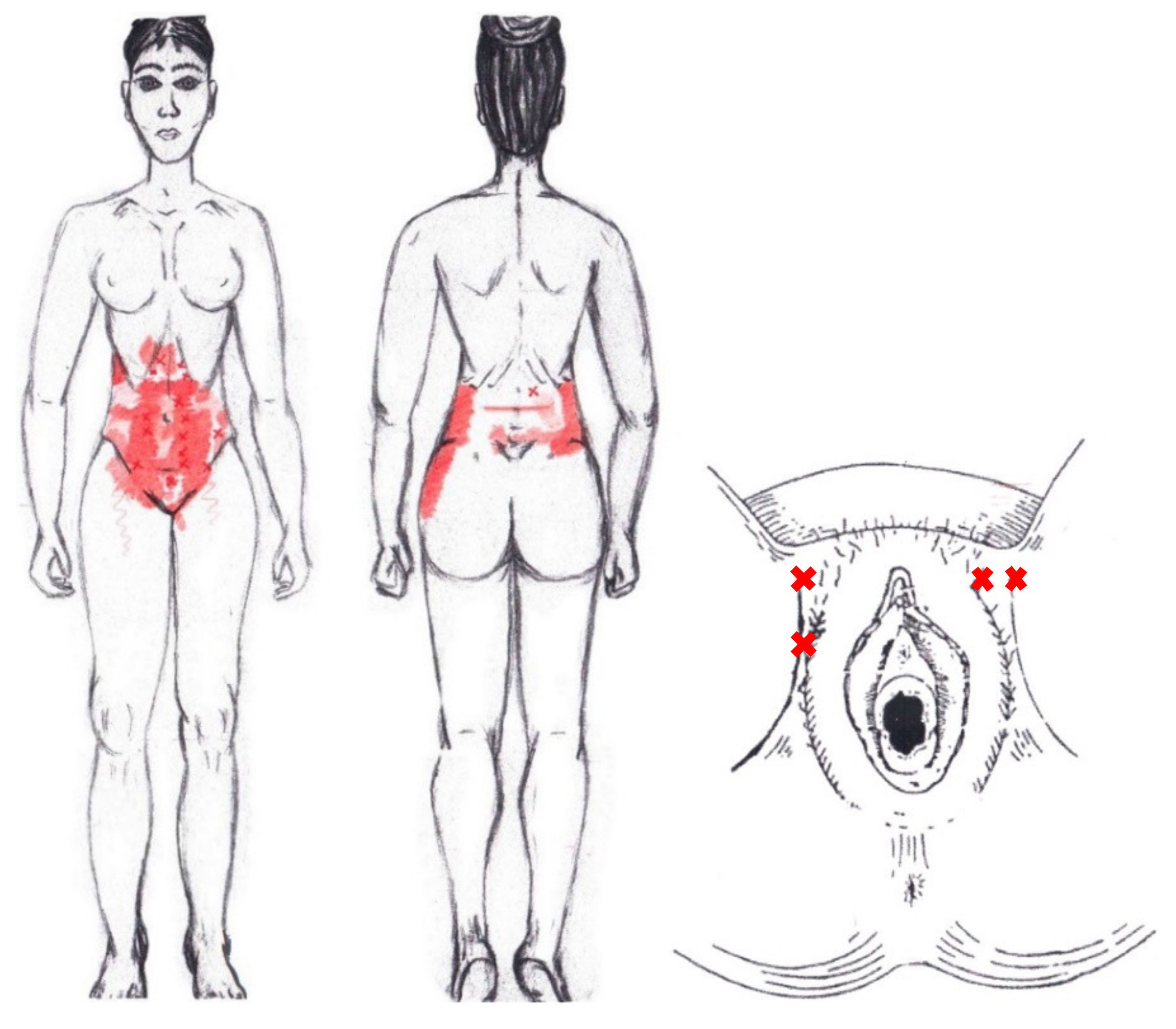
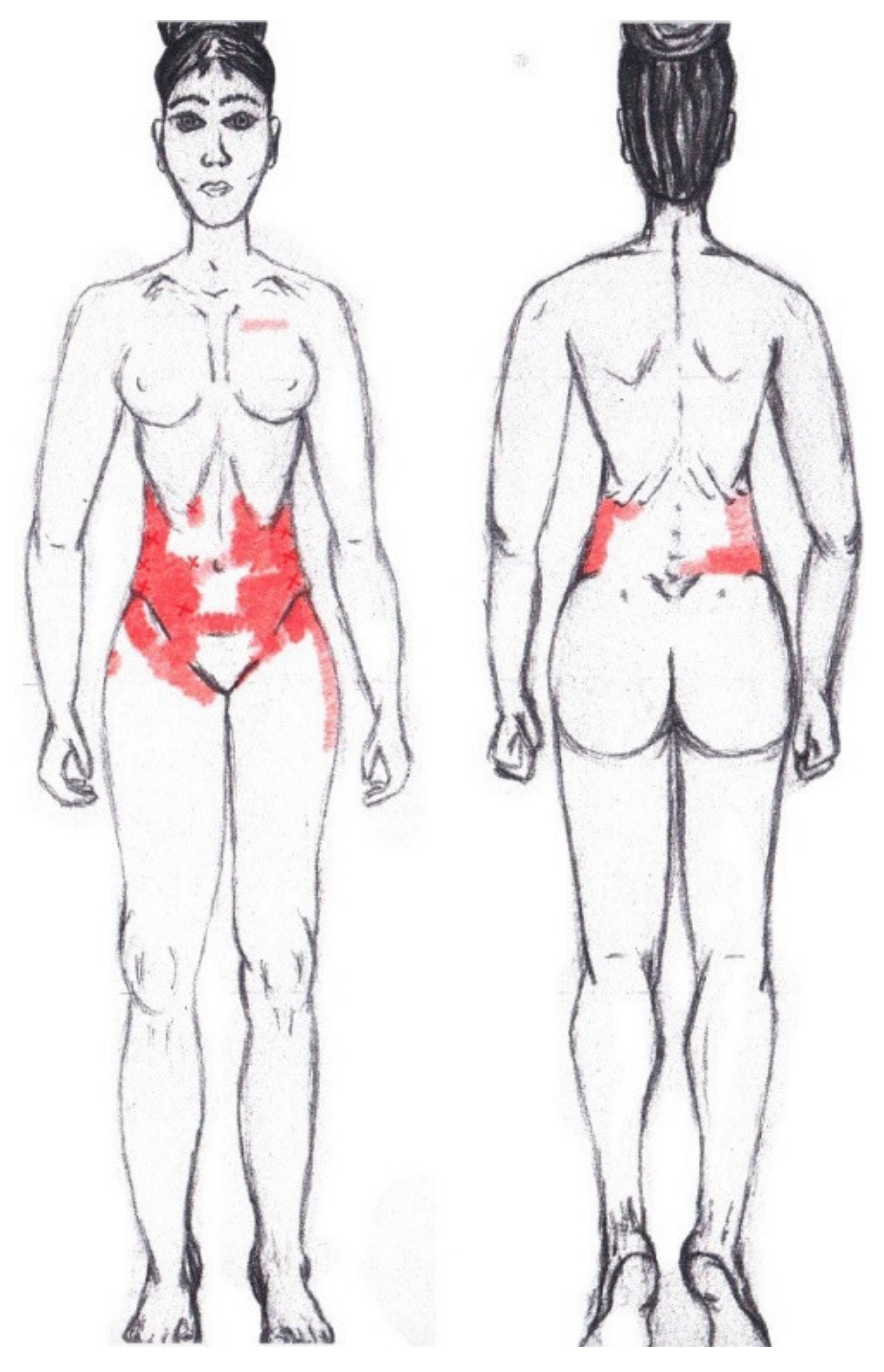
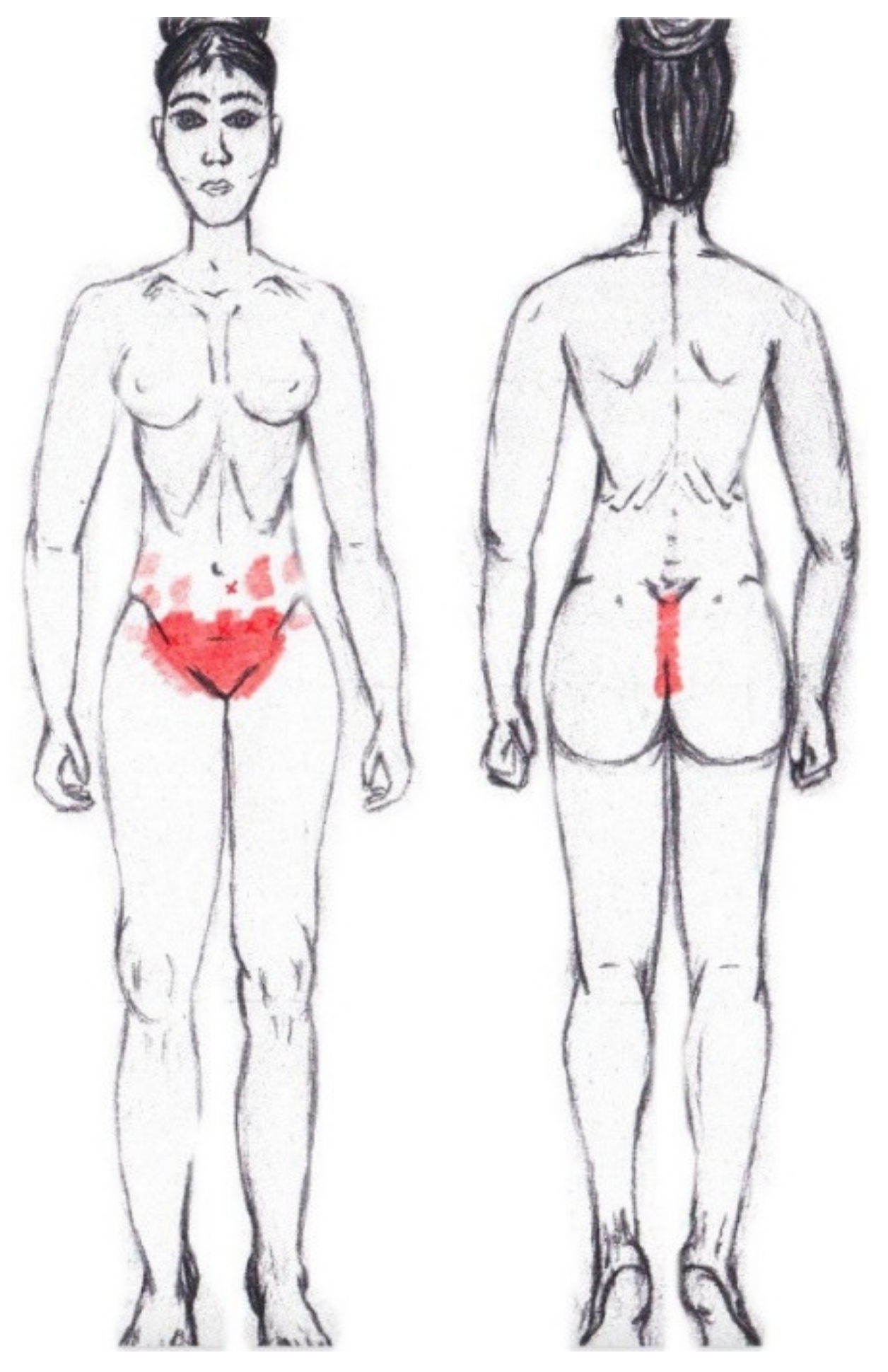
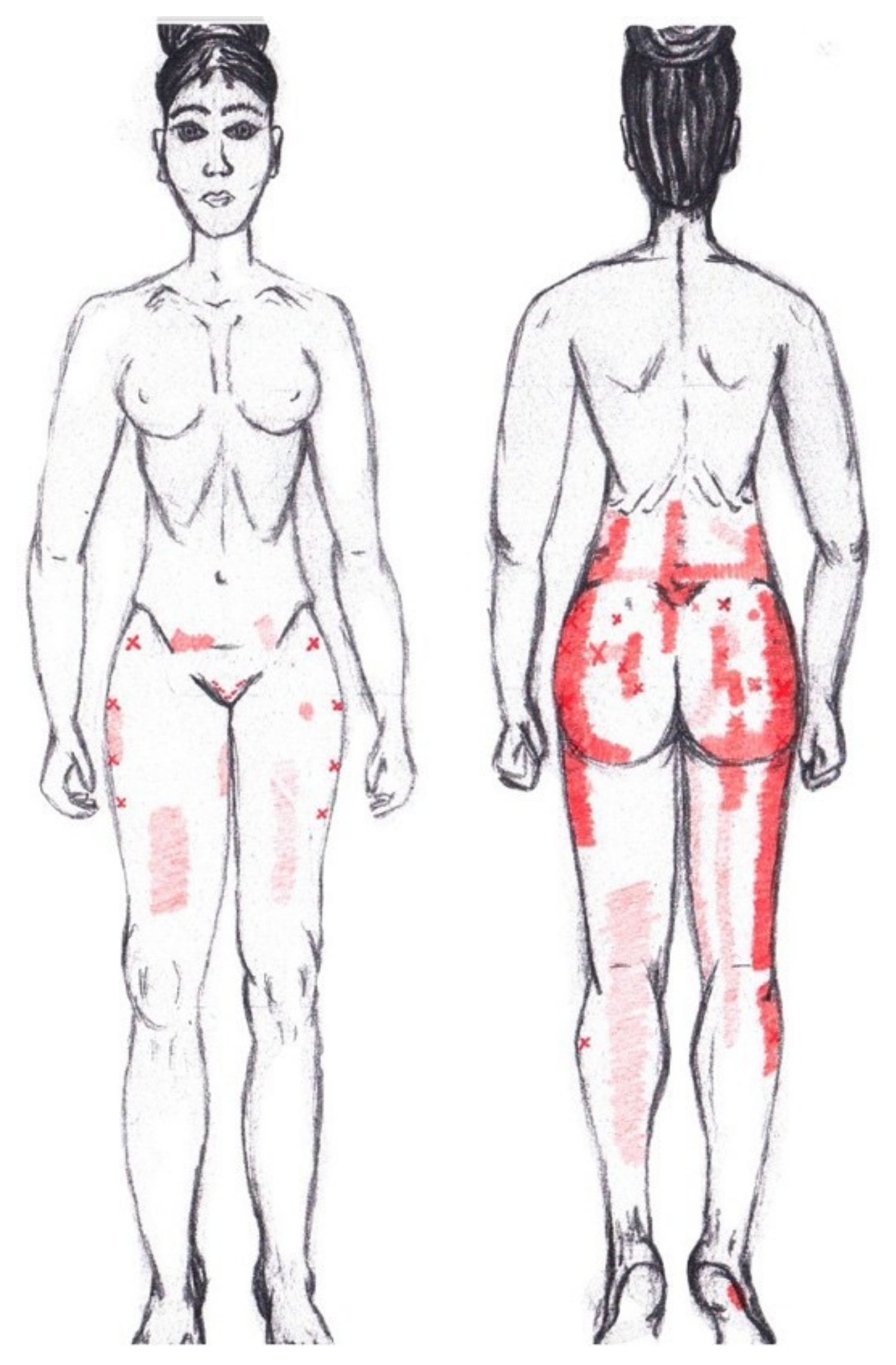
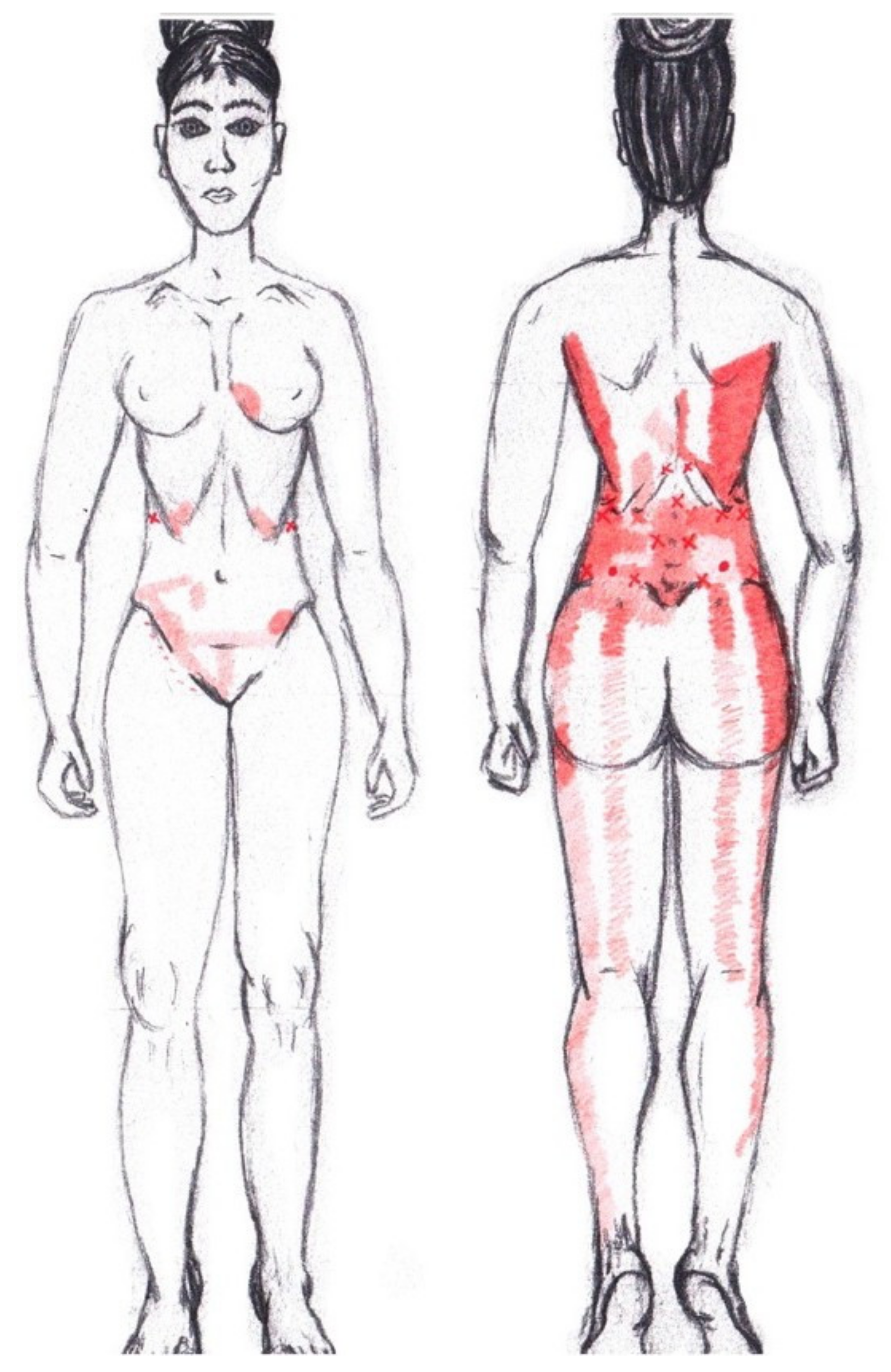
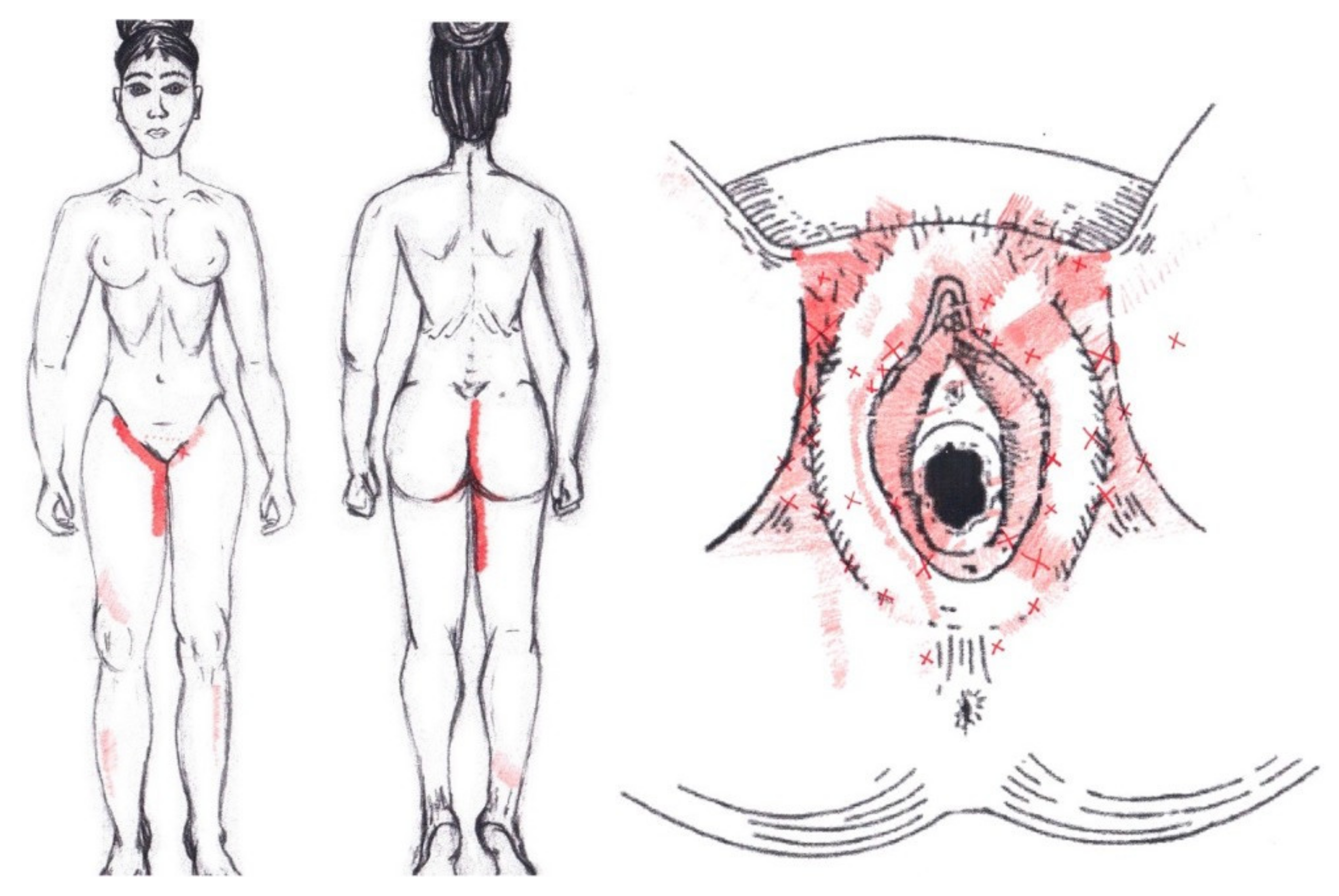
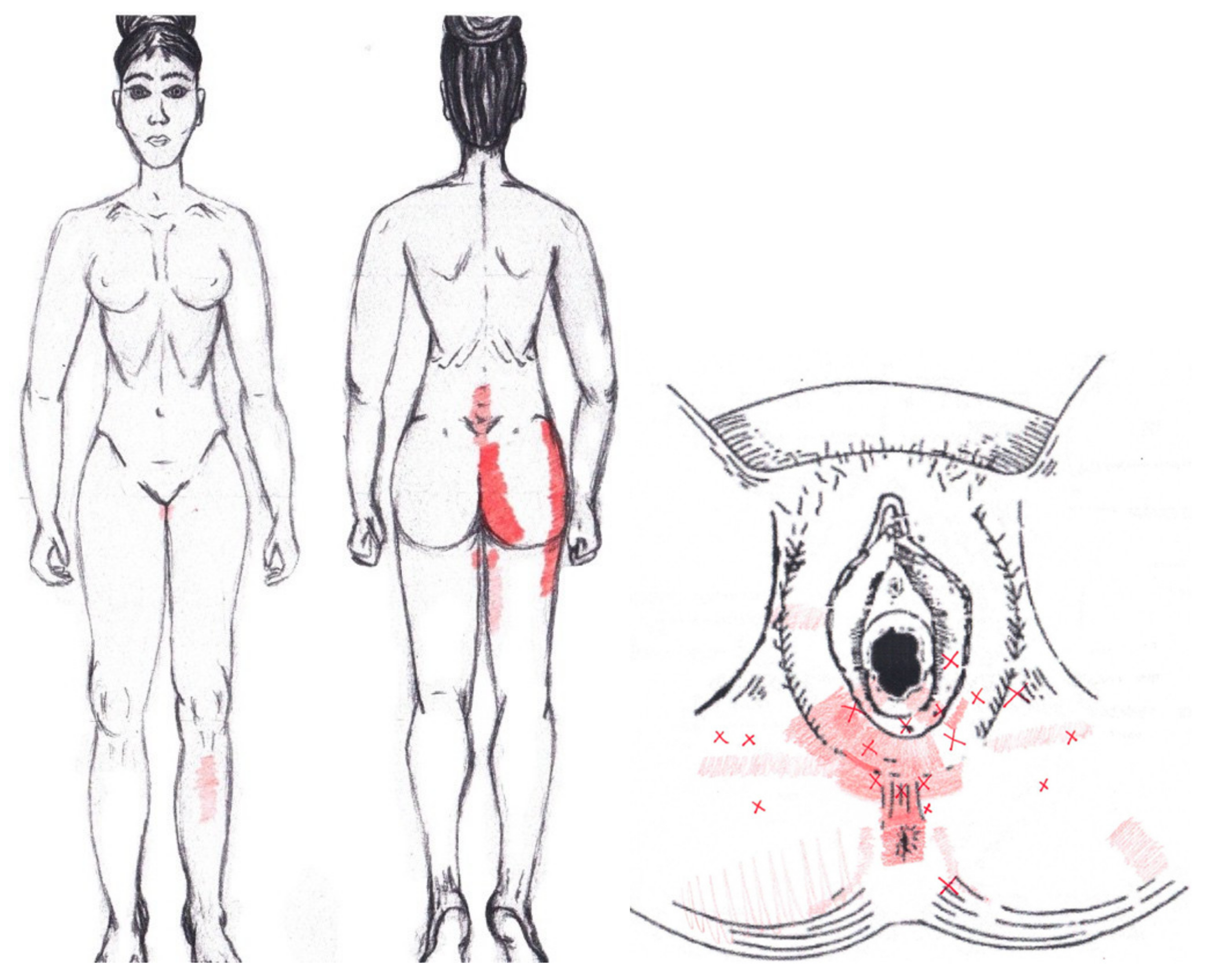
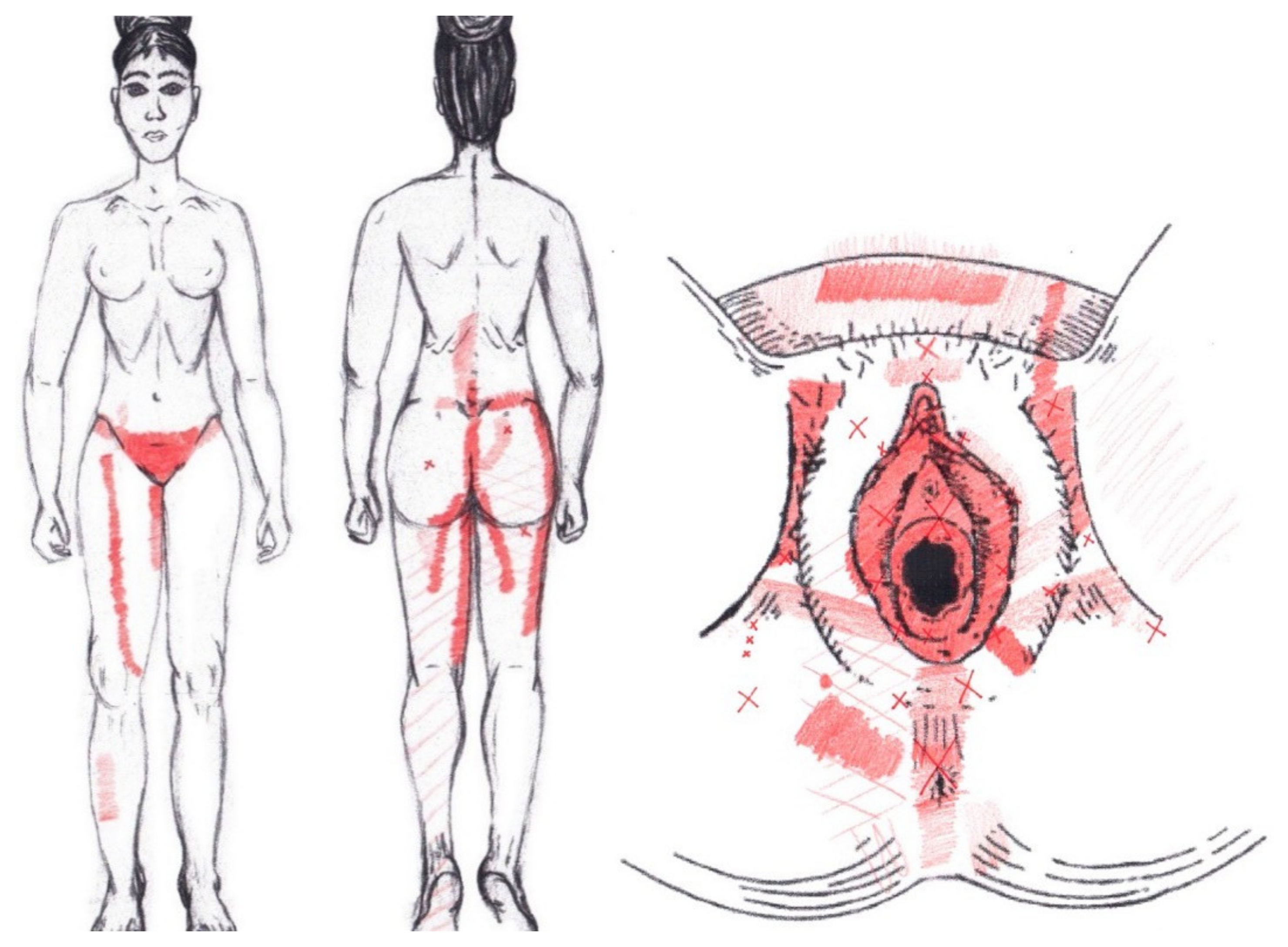
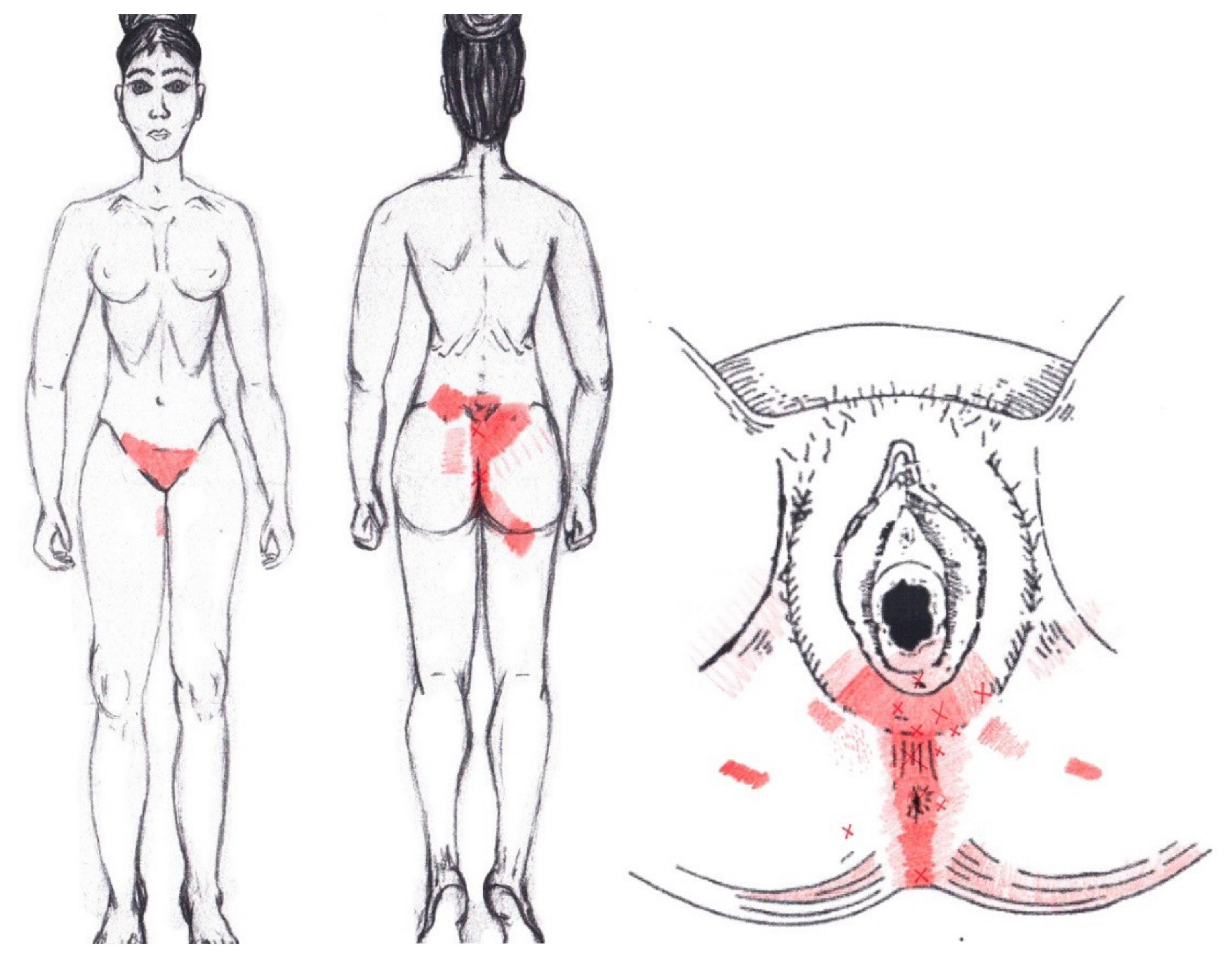
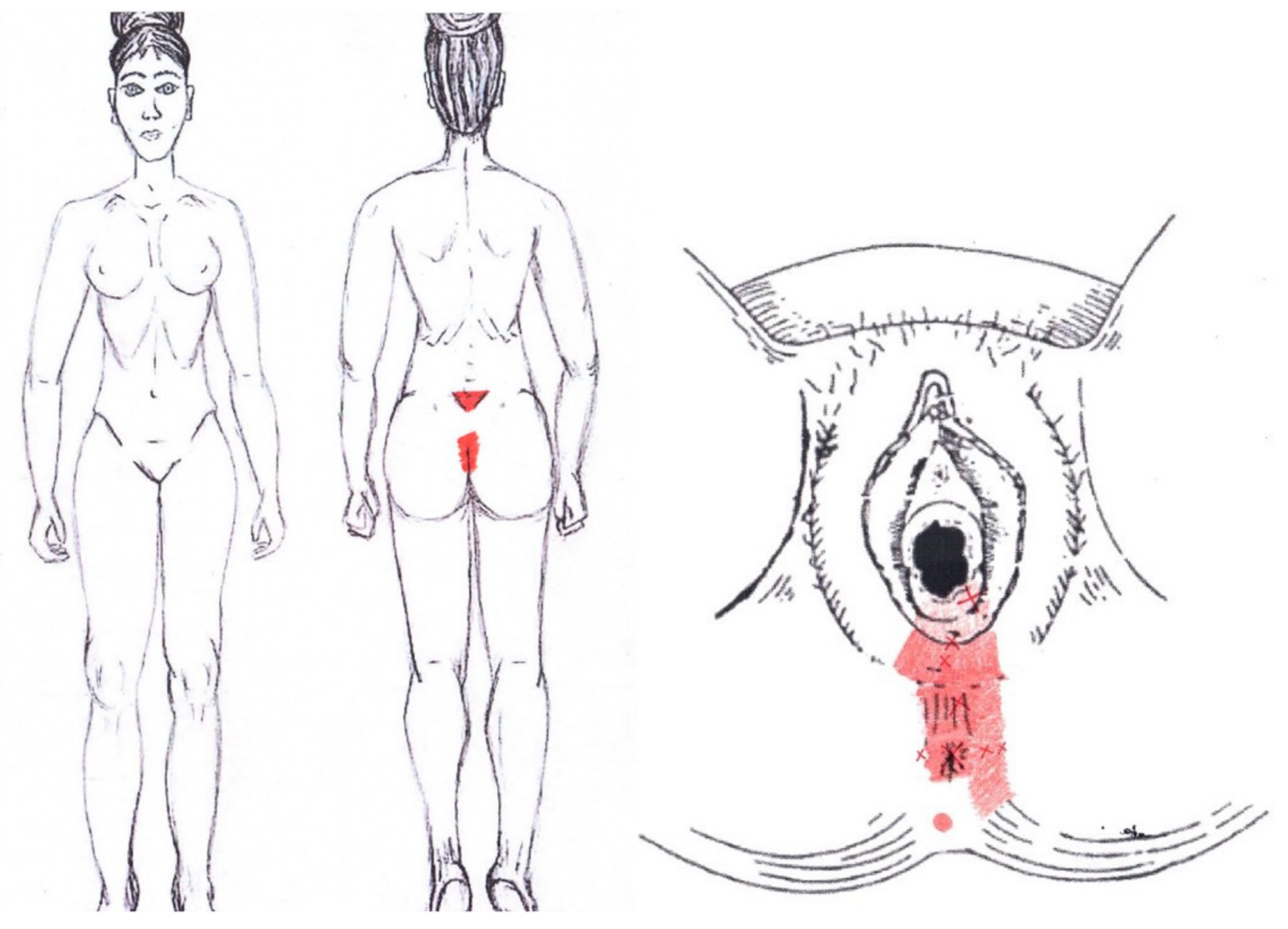
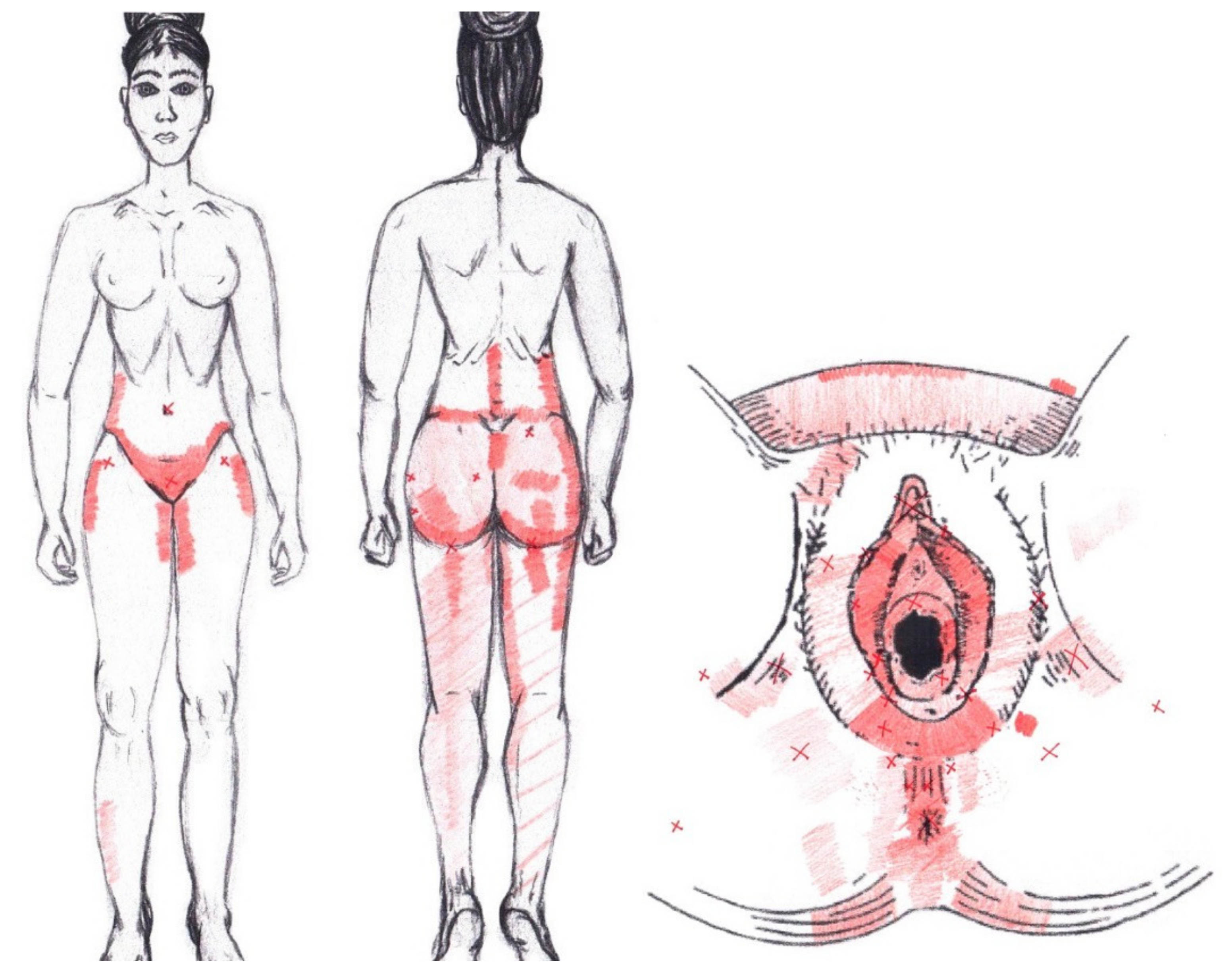
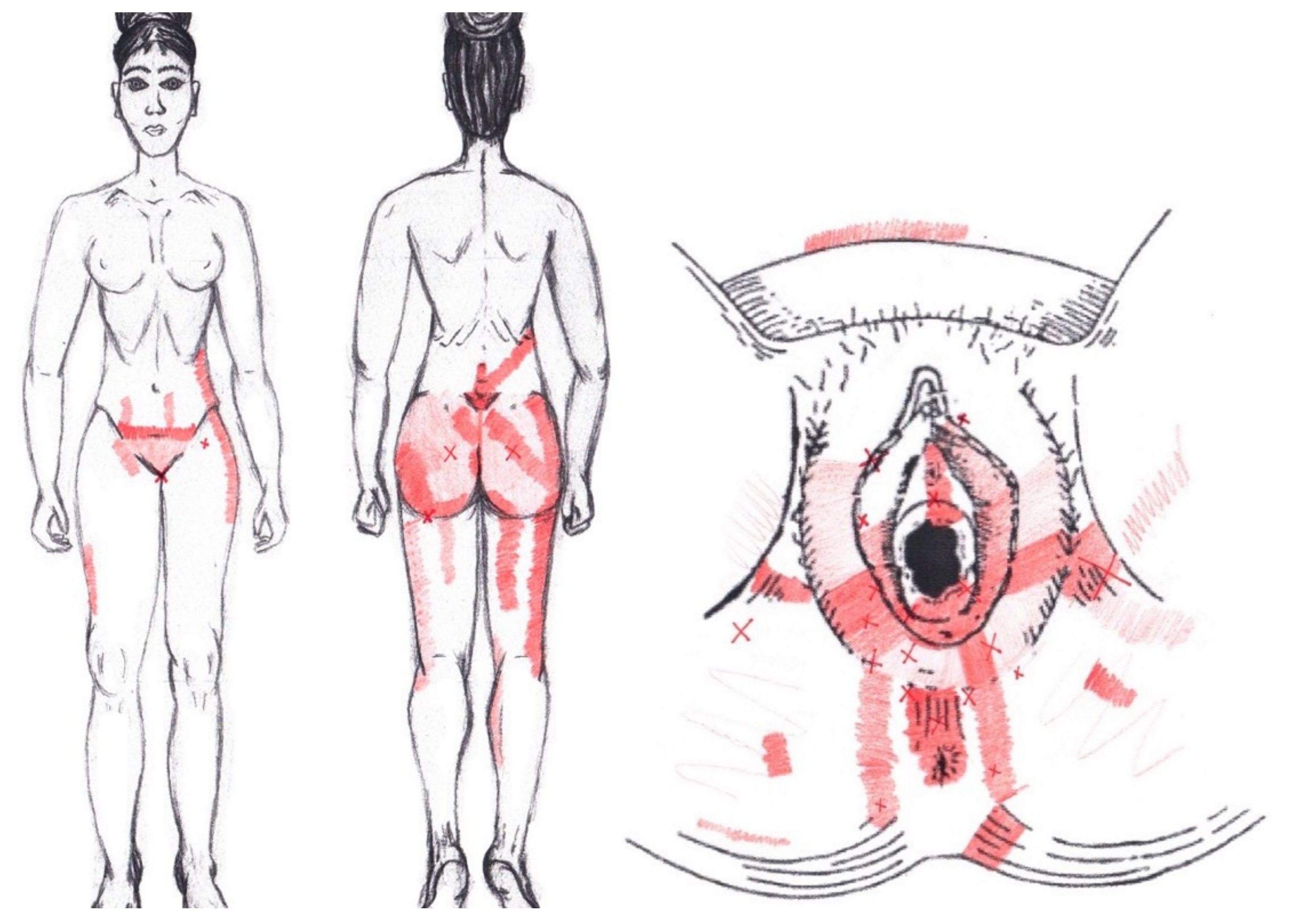
3.6. Referred Pain Areas
Rectus Abdominis Muscle
3.7. External Oblique Muscle
3.8. Internal Oblique Muscle
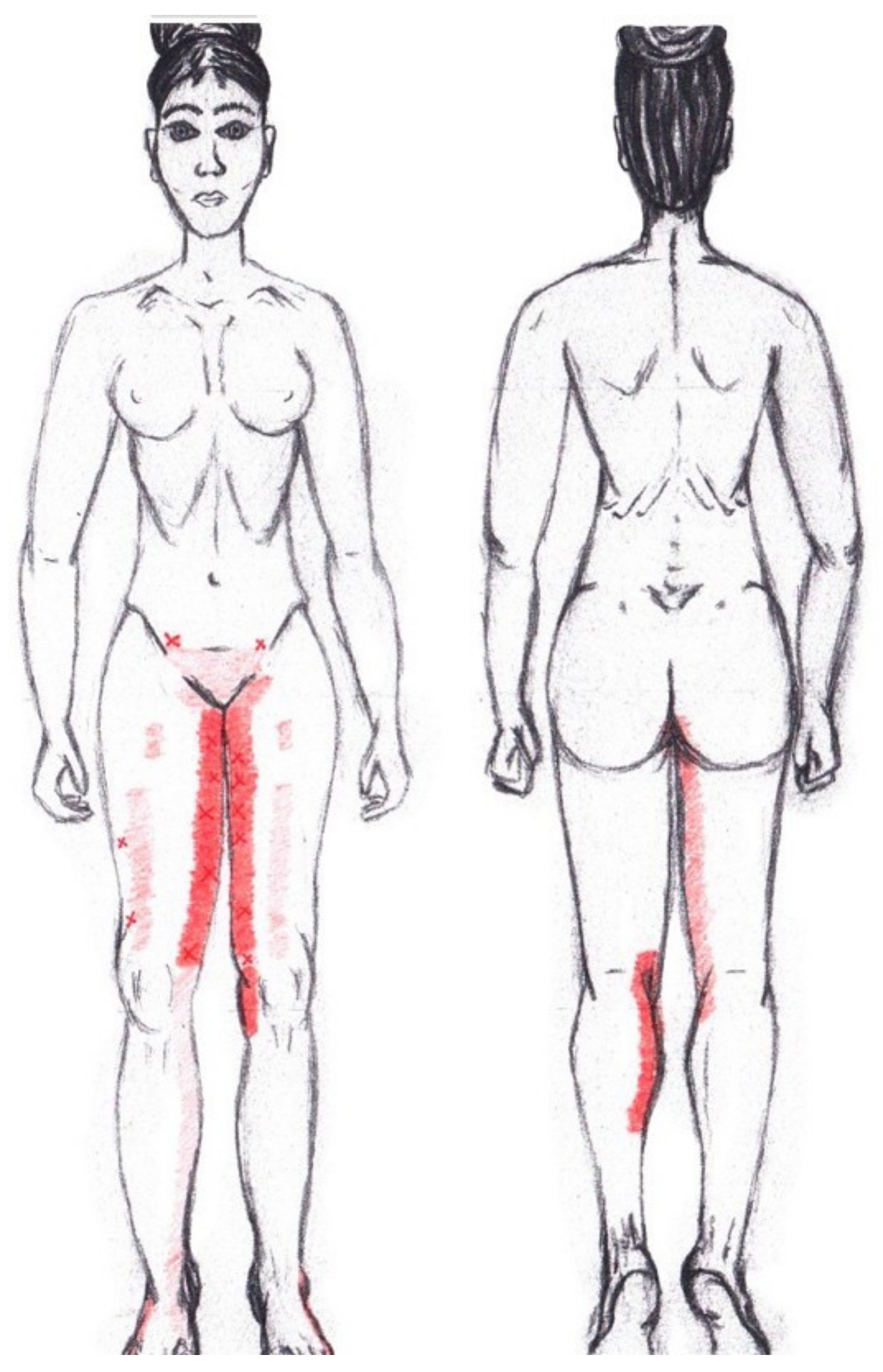
3.9. Adductor Magnus Muscle
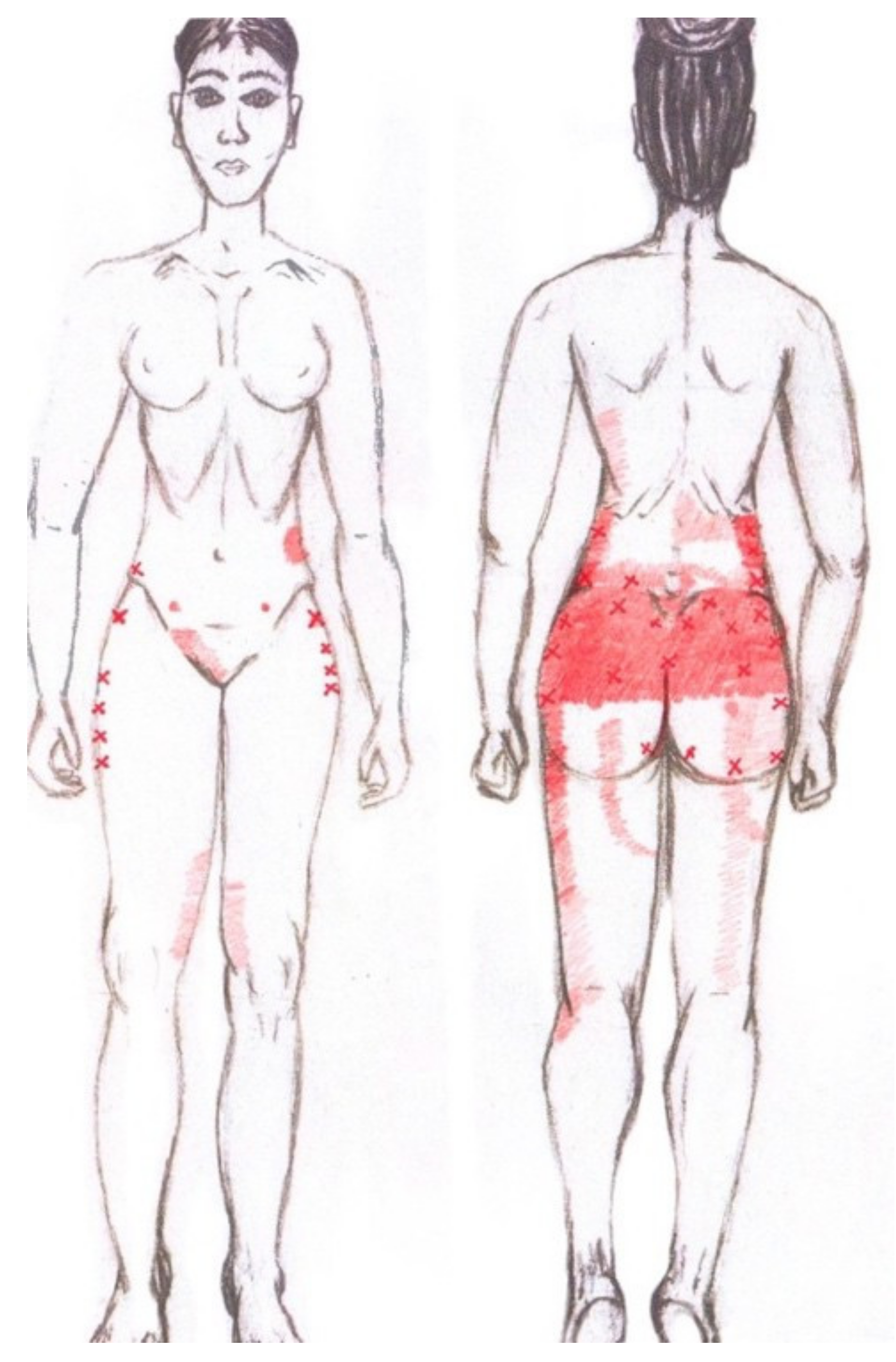
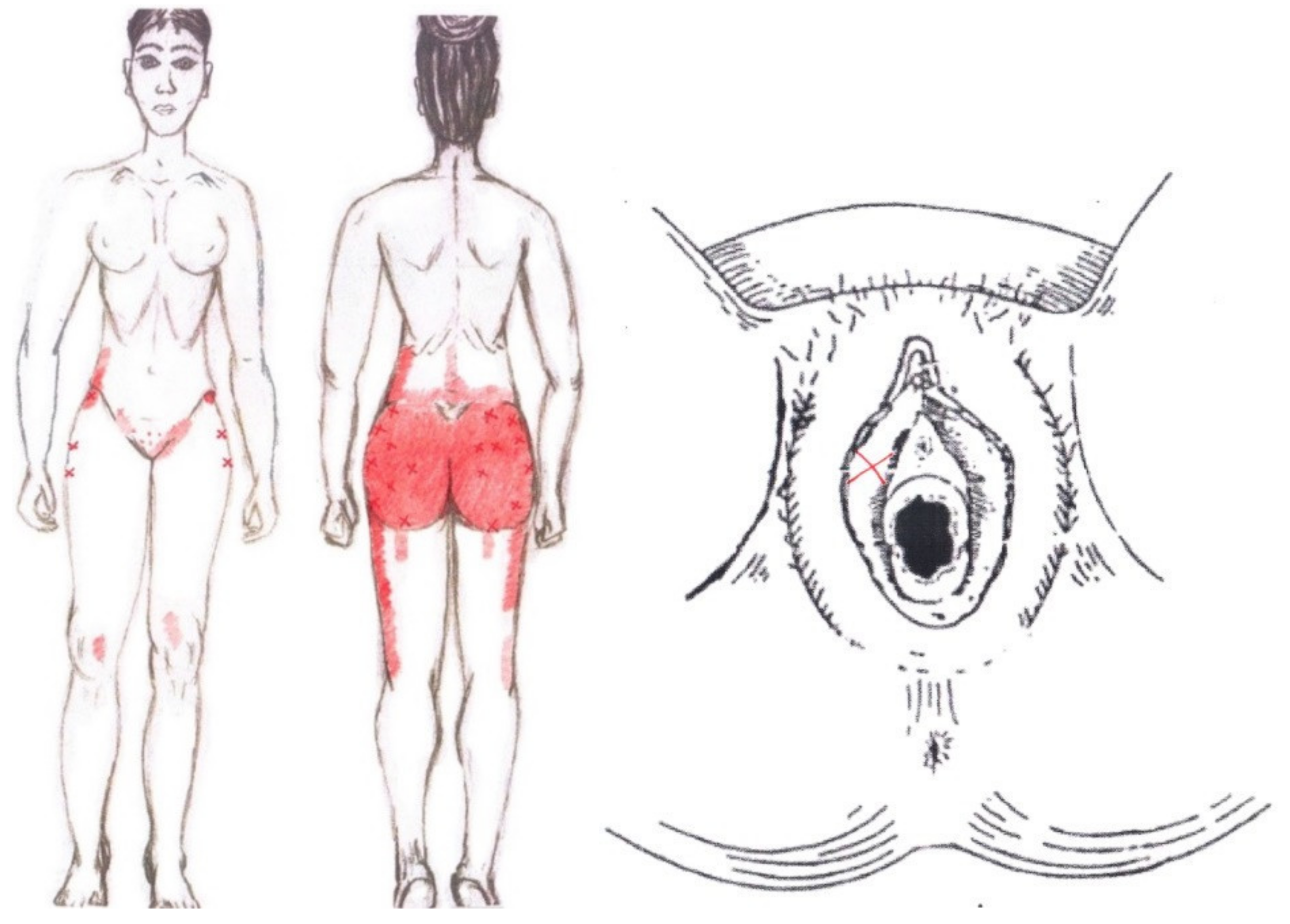
3.10. Gluteus Maximus Muscle
3.11. Gluteus Medius Muscle
3.12. Gluteus Minimus Muscle
3.13. Quadratus Lumborum Muscle
3.14. Ischiocavernosus Muscle
3.15. Bulbospongiosus Muscle
3.16. Transverse Perineal Muscle
3.17. Puborectalis Muscle
3.18. Pubococcygeus Muscle
3.19. Iliococcygeus Muscle
3.20. Coccygeus Muscle
3.21. External Anal Sphincter Muscle
3.22. Obturator Internus Muscle
3.23. Piriformis Muscle
4. Discussion
4.1. Sociodemographic Factors and Clinical Data
4.2. Menstrual Pain and Severity
4.3. Quality of Life
4.4. Pain Mechanosensitivity
4.5. Myofascial Trigger Points in Primary Dysmenorrhea
4.6. Referred Pain Areas
4.7. Hormonal Influence of the Menstrual Cycle on the Perception of Pain
4.8. Peripheral and Central Sensitization, and Their Relationship with Menstruation and Primary Dysmenorrhea
4.9. Future Lines of Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hurtado, B.G.; Chillón-Martínez, R.; Roldán, J.R.; Orta-Perez, M. Dismenorrea primaria y fisioterapia. Fisioterapia 2005, 27, 327–342. [Google Scholar] [CrossRef]
- Durain, D. Primary Dysmenorrhea: Assessment and Management Update. J. Midwifery Women’s Health 2004, 49, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Latthe, P.; Latthe, M.; Say, L.; Gülmezoglu, A.M.; Khan, K.S. WHO systematic review of prevalence of chronic pelvic pain: A neglected reproductive health morbidity. BMC Public Health 2006, 6, 177. [Google Scholar] [CrossRef]
- Larroy, C.; Crespo, M.; Meseguer, C. Dismenorrea Funcional En La Comunidad Autónoma de Madrid: Estudio de La Prevalencia En Función de La Edad. Rev. Soc. Esp. Dolor 2001, 8, 11–22. [Google Scholar]
- Abarca, L.; Molero, J.M.; Casimiro, C. Dismenorrea. Una revisión multidisciplinaria en el contexto de la medicina basada en la evidencia. FMC 2006, 13, 550–559. [Google Scholar] [CrossRef]
- Chrisler, J.C.; Gorman, J.A. Menstruation. In Encyclopedia of Mental Health, 2nd ed.; Academic Press: Cambridge, MA, USA, 2016; pp. 75–81. [Google Scholar] [CrossRef]
- Terranova, P. Dysmenorrhea. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Coco, A.S. Primary Dysmenorrhea. Am. Fam. Physician 1999, 60, 489. [Google Scholar]
- Guimarães, I.; Póvoa, A.M. Primary Dysmenorrhea: Assessment and Treatment Dismenorreia Primária: Avaliação e Trata-mento. Rev. Bras. Ginecol. Obstet. 2020, 42, 501–507. [Google Scholar] [CrossRef]
- Iacovides, S.; Avidon, I.; Baker, F.C. What we know about primary dysmenorrhea today: A critical review. Hum. Reprod. Update 2015, 21, 762–778. [Google Scholar] [CrossRef]
- Pickles, V.R. Myometrial Responses to the Menstrual Plain Muscle Stimulant. J. Endocrinol. 1959, 19, 150–157. [Google Scholar] [CrossRef]
- Pickles, V.R. A Plain-muscle Stimulant in the Menstruum. Nature 1957, 180, 1198–1199. [Google Scholar] [CrossRef]
- Akman, A.O.; Bozdag, G.; Pehlivantürk-Kizilkan, M.; Akgul, S.; Derman, O.; Kanbur, N. Menstrual Cycle Pain Is Independent of Ovulation in Adolescents with Primary Dysmenorrhea. J. Pediatr. Adolesc. Gynecol. 2021, 34, 635–642. [Google Scholar] [CrossRef]
- Deligeoroglou, E. Dysmenorrhea. Ann. N. Y. Acad. Sci. 2006, 900, 237–244. [Google Scholar] [CrossRef]
- Alfonsín, M.G.; López-Roca, A.; Rodríguez-Pampín, M.; Novo-Domínguez, A. Fisiología femenina II: Ciclo uterino. Ciclo endometrial. Menstruación. Procesos reparativos cervicales. Ciclo endocervical. Ciclo y fisiología de la vagina. Y la vulva. EN: Bajo JM, compilador. In Fundamentos de Obstetricia (SEGO); Grupo ENE Publicidad: Madrid, Spain, 2007; pp. 65–92. [Google Scholar]
- Dawood, M.Y. Dysmenorrhoea and Prostaglandins: Pharmacological and Therapeutic Considerations. Drugs 1981, 22, 42–56. [Google Scholar] [CrossRef]
- Sima, R.-M.; Sulea, M.; Radosa, J.C.; Findeklee, S.; Hamoud, B.H.; Popescu, M.; Gorecki, G.P.; Bobircă, A.; Bobirca, F.; Cirstoveanu, C.; et al. The Prevalence, Management and Impact of Dysmenorrhea on Medical Students’ Lives—A Multicenter Study. Healthcare 2022, 10, 157. [Google Scholar] [CrossRef]
- Andersch, B.; Milsom, I. An epidemiologic study of young women with dysmenorrhea. Am. J. Obstet. Gynecol. 1982, 144, 655–660. [Google Scholar] [CrossRef]
- Karout, S.; Soubra, L.; Rahme, D.; Karout, L.; Khojah, H.M.J.; Itani, R. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Women’s Health 2021, 21, 1–14. [Google Scholar] [CrossRef]
- Burnett, M.; Lemyre, M. No. 345-Primary Dysmenorrhea Consensus Guideline. J. Obstet. Gynaecol. Can. 2017, 39, 585–595. [Google Scholar] [CrossRef]
- López-Liria, R.; Torres-Álamo, L.; Vega-Ramírez, F.; García-Luengo, A.; Aguilar-Parra, J.; Trigueros-Ramos, R.; Rocamora-Pérez, P. Efficacy of Physiotherapy Treatment in Primary Dysmenorrhea: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7832. [Google Scholar] [CrossRef]
- Gaubeca-Gilarranz, A.; Fernández-De-Las-Peñas, C.; Medina-Torres, J.R.; Seoane-Ruiz, J.M.; Company-Palonés, A.; A Cleland, J.; Arias-Buría, J.L. Effectiveness of Dry Needling of Rectus Abdominis Trigger Points for the Treatment of Primary Dysmenorrhoea: A Randomised Parallel-Group Trial. Acupunct. Med. J. Br. Med. Acupunct. Soc. 2018, 36, 302–310. [Google Scholar] [CrossRef]
- Huang, Q.-M.; Liu, L. Wet Needling of Myofascial Trigger Points in Abdominal Muscles for Treatment of Primary Dysmenorrhoea. Acupunct. Med. 2014, 32, 346–349. [Google Scholar] [CrossRef]
- Díaz, M.E.; Cabellos, C.F. Relationship between Dysmenorrhoea and Myofascial Pain Syndrome. A Physiotherapist Perspective. Pilot Randomized Trial. Fisioterapia 2020, 43, 5–11. [Google Scholar] [CrossRef]
- Howard, F.M. Chronic Pelvic Pain in Women. Am. J. Manag. Care 2001, 7, 1001–1011. [Google Scholar] [PubMed]
- Merskey, H.; Bogduk, N. Classification of Chronic Pain, IASP Task Force on Taxonomy; International Association for the Study of Pain Press: Seattle, WA, USA, 1994. [Google Scholar]
- Simons, D.G.; Travell, J.G.; Simons, L.S. Myofascial Pain and Dysfunction: The Trigger Point Manual. Volume 1 “Upper Half of Body”, 2nd ed.; Lippincott Williams & Wilkins: Baltimore, PA, USA, 1999. [Google Scholar]
- Cao, Q.-W.; Peng, B.-G.; Wang, L.; Huang, Y.-Q.; Jia, D.-L.; Jiang, H.; Lv, Y.; Liu, X.-G.; Liu, R.-G.; Li, Y.; et al. Expert consensus on the diagnosis and treatment of myofascial pain syndrome. World J. Clin. Cases 2021, 9, 2077–2089. [Google Scholar] [CrossRef] [PubMed]
- Gerwin, R.D. Myofascial Trigger Point Pain Syndromes. Semin. Neurol. 2016, 36, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Giamberardino, M.A.; Tana, C.; Costantini, R. Pain thresholds in women with chronic pelvic pain. Curr. Opin. Obstet. Gynecol. 2014, 26, 253–259. [Google Scholar] [CrossRef]
- Rathbone, A.T.; Grosman-Rimon, L.; Kumbhare, D. Interrater Agreement of Manual Palpation for Identification of Myofascial Trigger Points: A Systematic Review and Meta-Analysis. Clin. J. Pain 2017, 33, 715–729. [Google Scholar] [CrossRef]
- Li, L.; Stoop, R.; Clijsen, R.; Hohenauer, E.; Fernández-De-Las-Peñas, C.; Huang, Q.; Barbero, M. Criteria Used for the Diagnosis of Myofascial Trigger Points in Clinical Trials on Physical Therapy: Updated Systematic Review. Clin. J. Pain 2020, 36, 955–967. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Dommerholt, J. International Consensus on Diagnostic Criteria and Clinical Considerations of Myofascial Trigger Points: A Delphi Study. Pain Med. 2018, 19, 142–150. [Google Scholar] [CrossRef]
- Saxena, A.; Chansoria, M.; Tomar, G.; Kumar, A. Myofascial Pain Syndrome: An Overview. J. Pain Palliat. Care Pharmacother. 2015, 29, 16–21. [Google Scholar] [CrossRef]
- Gerwin, R.D. Diagnosis of Myofascial Pain Syndrome. Phys. Med. Rehabil. Clin. N. Am. 2014, 25, 341–355. [Google Scholar] [CrossRef]
- Shah, J.P.; Thaker, N.; Heimur, J.; Aredo, J.V.; Sikdar, S.; Gerber, L. Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective. PM R 2015, 7, 746–761. [Google Scholar] [CrossRef]
- Torres-Chica, B.; Núñez-Samper-Pizarroso, C.; Ortega-Santiago, R.; Cleland, J.A.; Salom-Moreno, J.; Laguarta-Val, S.; Fernández-De-Las-Peñas, C. Trigger Points and Pressure Pain Hypersensitivity in People with Postmeniscectomy Pain. Clin. J. Pain 2015, 31, 265–272. [Google Scholar] [CrossRef]
- Lucas, K.R.; Rich, P.A.; Polus, B.I. Muscle activation patterns in the scapular positioning muscles during loaded scapular plane elevation: The effects of Latent Myofascial Trigger Points. Clin. Biomech. 2010, 25, 765–770. [Google Scholar] [CrossRef]
- Travell, J.; Simons, D. Myofascial Pain and Dysfunction: The Trigger Point Manual, 1st ed.; Lippincott Williams & Wilkins: Baltimore, PA, USA, 1999; Volume 2. [Google Scholar]
- Maddux:Menstruation—Google Académico. Available online: https://scholar.google.com/scholar_lookup?title=Menstruation&author=H.C.Maddux&publication_year=1975 (accessed on 2 March 2022).
- Abreu-Sánchez, A.; Ruiz-Castillo, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Fernández-Martínez, E. Interference and Impact of Dysmenorrhea on the Life of Spanish Nursing Students. Int. J. Environ. Res. Public Health 2020, 17, 6473. [Google Scholar] [CrossRef]
- Aredo, J.V.; Heyrana, K.J.; Karp, B.I.; Shah, J.P.; Stratton, P. Relating Chronic Pelvic Pain and Endometriosis to Signs of Sensitization and Myofascial Pain and Dysfunction. Semin. Reprod. Med. 2017, 35, 088–097. [Google Scholar] [CrossRef]
- Itza, F.; Zarza, D.; Serra, L.; Gómez-Sancha, F.; Salinas, J.; Allona-Almagro, A. Myofascial pain syndrome in the pelvic floor: A common urological condition. Actas Urológicas Españolas 2010, 34, 318–326. [Google Scholar] [CrossRef]
- Montenegro, M.L.; Gomide, L.B.; Mateus-Vasconcelos, E.L.; Rosa-E-Silva, J.C.; Candido-Dos-Reis, F.J.; Nogueira, A.A.; Poli-Neto, O.B. Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 147, 21–24. [Google Scholar] [CrossRef]
- Anderson, R.U.; Sawyer, T.; Wise, D.; Morey, A.; Nathanson, B.H. Painful Myofascial Trigger Points and Pain Sites in Men With Chronic Prostatitis/Chronic Pelvic Pain Syndrome. J. Urol. 2009, 182, 2753–2758. [Google Scholar] [CrossRef]
- Jarrell, J.; Giamberardino, M.A.; Robert, M.; Nasr-Esfahani, M. Bedside Testing for Chronic Pelvic Pain: Discriminating Visceral from Somatic Pain. Pain Res. Treat. 2011, 2011, 692102. [Google Scholar] [CrossRef]
- Oyama, I.A.; Rejba, A.; Lukban, J.C.; Fletcher, E.; Kellogg-Spadt, S.; Holzberg, A.S.; Whitmore, K.E. Modified Thiele massage as therapeutic intervention for female patients with interstitial cystitis and high-tone pelvic floor dysfunction. Urology 2004, 64, 862–865. [Google Scholar] [CrossRef]
- Weiss, J.M. Pelvic Floor Myofascial Trigger Points: Manual Therapy for Interstitial Cystitis and the Urgency-Frequency Syndrome. J. Urol. 2001, 166, 2226–2231. [Google Scholar] [CrossRef] [PubMed]
- Doggweiler-Wiygul, R.; Wiygul, P.J. Interstitial cystitis, pelvic pain, and the relationship to myofascial pain and dysfunction: A report on four patients. World J. Urol. 2002, 20, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Bassaly, R.; Tidwell, N.; Bertolino, S.; Hoyte, L.; Downes, K.; Hart, S. Myofascial pain and pelvic floor dysfunction in patients with interstitial cystitis. Int. Urogynecology J. 2010, 22, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.U.; Wise, D.; Sawyer, T.; Nathanson, B.H.; Smith, J.N. Equal Improvement in Men and Women in the Treatment of Urologic Chronic Pelvic Pain Syndrome Using a Multi-modal Protocol with an Internal Myofascial Trigger Point Wand. Appl. Psychophysiol. Biofeedback 2016, 41, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, M.P.; Anderson, R.U.; Potts, J.; Payne, C.K.; Peters, K.M.; Clemens, J.Q.; Kotarinos, R.; Fraser, L.; Cosby, A.; Fortman, C.; et al. Randomized Multicenter Feasibility Trial of Myofascial Physical Therapy for the Treatment of Urological Chronic Pelvic Pain Syndromes. J. Urol. 2013, 189, S75–S85. [Google Scholar] [CrossRef]
- Tadros, N.N.; Shah, A.B.; Shoskes, D.A. Utility of trigger point injection as an adjunct to physical therapy in men with chronic prostatitis/chronic pelvic pain syndrome. Transl. Androl. Urol. 2017, 6, 534–537. [Google Scholar] [CrossRef]
- Anderson, R.U. Management of chronic prostatitis–chronic pelvic pain syndrome. Urol. Clin. N. Am. 2002, 29, 235–239. [Google Scholar] [CrossRef]
- Anderson, R.U.; Wise, D.; Sawyer, T.; Chan, C. Integration of Myofascial Trigger Point Release and Paradoxical Relaxation Training Treatment of Chronic Pelvic Pain in Men. J. Urol. 2005, 174, 155–160. [Google Scholar] [CrossRef]
- Anderson, R.U.; Wise, D.; Sawyer, T.; Chan, C.A. Sexual Dysfunction in Men with Chronic Prostatitis/Chronic Pelvic Pain Syndrome: Improvement After Trigger Point Release and Paradoxical Relaxation Training. J. Urol. 2006, 176, 1534–1539. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Lee, T.H. Anorectal and Pelvic Pain. Mayo Clin. Proc. 2016, 91, 1471–1486. [Google Scholar] [CrossRef]
- Ashrafi, A.; Arab, A.M.; Abdi, S.; Nourbakhsh, M.R. The association between myofascial trigger points and the incidence of chronic functional constipation. J. Bodyw. Mov. Ther. 2020, 26, 201–206. [Google Scholar] [CrossRef]
- Yacubovich, Y.; Cohen, N.; Tene, L.; Kalichman, L. The prevalence of primary dysmenorrhea among students and its association with musculoskeletal and myofascial pain. J. Bodyw. Mov. Ther. 2019, 23, 785–791. [Google Scholar] [CrossRef]
- Langford, C.F.; Nagy, S.U.; Ghoniem, G. Levator ani trigger point injections: An underutilized treatment for chronic pelvic pain. Neurourol. Urodyn. 2007, 26, 59–62. [Google Scholar] [CrossRef]
- Hong, C.-Z. Lidocaine Injection versus Dry Needling to Myofascial Trigger Point. The Importance of the Local Twitch Response. Am. J. Phys. Med. Rehabil. 1994, 73, 256–263. [Google Scholar] [CrossRef]
- Venancio, R.D.A.; Alencar, F.G.P.; Zamperini, C. Botulinum Toxin, Lidocaine, and Dry-Needling Injections in Patients with Myofascial Pain and Headaches. CRANIO® 2009, 27, 46–53. [Google Scholar] [CrossRef]
- Bhide, A.A.; Puccini, F.; Khullar, V.; Elneil, S.; Digesu, G.A. Botulinum neurotoxin type A injection of the pelvic floor muscle in pain due to spasticity: A review of the current literature. Int. Urogynecology J. 2013, 24, 1429–1434. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Reed, B.G.; Carr, B.R. The Normal Menstrual Cycle and the Control of Ovulation. In Endotext; MDText.com, Inc.: South Dartmouth, MA, USA, 2018. [Google Scholar]
- Macías, A.S.A.; de Miranda, M.L.A.; Díaz, A.Q. La Mujer, El Ciclo Menstrual y La Actividad Física The Woman, the Menstrual Cycle, and the Physical Activity. Rev. Arch. Médico De Camagüey 2017, 21, 294–307. [Google Scholar]
- Úbeda-D’Ocasar, E.; Valera-Calero, J.; Hervás-Pérez, J.; Caballero-Corella, M.; Ojedo-Martín, C.; Gallego-Sendarrubias, G. Pain Intensity and Sensory Perception of Tender Points in Female Patients with Fibromyalgia: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 1461. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 760: Dysmenorrhea and Endometriosis in the Adolescent. Obstet. Gynecol. 2018, 132, e249–e258. [Google Scholar] [CrossRef]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the sf-12 health survey in nine countries: Results from the iqola project. International quality of life assessment. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- Melzack, R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef] [PubMed]
- The Development of a Spanish Questionnaire for Assessing Pain: Preliminary Data Concerning Reliability and Validity—PsycNET. Available online: https://psycnet.apa.org/record/1995-11922-001 (accessed on 6 February 2022).
- Masedo, A.I.; Esteve, R. Some empirical evidence regarding the validity of the Spanish Version of the McGill Pain Questionnaire (MPQ-SV). Pain 2000, 85, 451–456. [Google Scholar] [CrossRef]
- Kahl, C.; Cleland, J.A. Visual analogue scale, numeric pain rating scale and the McGill pain Questionnaire: An overview of psychometric properties. Phys. Ther. Rev. 2005, 10, 123–128. [Google Scholar] [CrossRef]
- Blanca, M.J.; Alarcón, R.; Arnau, J.; Bono, R.; Bendayan, R. Non-Normal Data: Is ANOVA still a Valid Option? Psicothema 2017, 29, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Haverkamp, N.; Beauducel, A. Violation of the Sphericity Assumption and Its Effect on Type-I Error Rates in Repeated Measures ANOVA and Multi-Level Linear Models (MLM). Front. Psychol. 2017, 8, 1841. [Google Scholar] [CrossRef]
- Cohen, J. Eta-Squared and Partial Eta-Squared in Fixed Factor Anova Designs. Educ. Psychol. Meas. 1973, 33, 107–112. [Google Scholar] [CrossRef]
- Kelley, K.; Preacher, K.J. On effect size. Psychol. Methods 2012, 17, 137–152. [Google Scholar] [CrossRef]
- Hazra, A.; Gogtay, N. Biostatistics series module 4: Comparing groups—Categorical variables. Indian J. Dermatol. 2016, 61, 385–392. [Google Scholar] [CrossRef]
- Maity, S.; Wray, J.; Coffin, T.; Nath, R.; Nauhria, S.; Sah, R.; Waechter, R.; Ramdass, P.; Nauhria, S. Academic and Social Impact of Menstrual Disturbances in Female Medical Students: A Systematic Review and Meta-Analysis. Front. Med. 2022, 9, 821908. [Google Scholar] [CrossRef]
- Çinar, G.N.; Akbayrak, T.; Gürşen, C.; Baran, E.; Üzelpasacı, E.; Nakip, G.; Bozdağ, G.; Beksaç, M.S.; Özgül, S. Factors Related to Primary Dysmenorrhea in Turkish Women: A Multiple Multinomial Logistic Regression Analysis. Reprod. Sci. 2020, 28, 381–392. [Google Scholar] [CrossRef]
- Latthe, P.; Mignini, L.; Gray, R.; Hills, R.; Khan, K. Factors predisposing women to chronic pelvic pain: Systematic review. BMJ 2006, 332, 749–755. [Google Scholar] [CrossRef]
- Hu, Z.; Tang, L.; Chen, L.; Kaminga, A.C.; Xu, H. Prevalence and Risk Factors Associated with Primary Dysmenorrhea among Chinese Female University Students: A Cross-sectional Study. J. Pediatr. Adolesc. Gynecol. 2020, 33, 15–22. [Google Scholar] [CrossRef]
- Gudipally, P.R.; Sharma, G.K. Premenstrual Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Bouchoucha, M.; Devroede, G.; Rompteaux, P.; Mary, F.; Bejou, B.; Benamouzig, R. Clinical, Physiological, and Psychological Correlates of the Improvement of Defecation during Menses in Women with Functional Gastrointestinal Disorders. Visc. Med. 2020, 36, 487–493. [Google Scholar] [CrossRef]
- Armour, M.; Ee, C.C.; Naidoo, D.; Ayati, Z.; Chalmers, K.J.; A Steel, K.; de Manincor, M.; Delshad, E. Exercise for dysmenorrhoea. Cochrane Database Syst. Rev. 2019, 2019, CD004142. [Google Scholar] [CrossRef]
- French, L. Dysmenorrhea. Am. Fam. Physician 2005, 71, 285–292. [Google Scholar] [CrossRef]
- Dawood, M.Y. Ibuprofen and Dysmenorrhea. Am. J. Med. 1984, 77, 87–94. [Google Scholar] [CrossRef]
- Lefebvre, G.; Pinsonneault, O.; Antao, V.; Black, A.; Burnett, M.; Feldman, K.; Lea, R.; Robert, M. Sogc Primary Dysmenorrhea Consensus Guideline. J. Obstet. Gynaecol. Can. 2005, 27, 1117–1130. [Google Scholar] [CrossRef]
- Sachedina, A.; Todd, N. Dysmenorrhea, Endometriosis and Chronic Pelvic Pain in Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2020, 12, 7–17. [Google Scholar] [CrossRef]
- Wildemeersch, D.; Jandi, S.; Pett, A.; Hasskamp, T. Management of primary dysmenorrhea in young women with frameless LNG-IUS. Open Access J. Contracept. 2014, 5, 23–28. [Google Scholar] [CrossRef]
- Lindh, I.; Milsom, I. The influence of intrauterine contraception on the prevalence and severity of dysmenorrhea: A longitudinal population study. Hum. Reprod. 2013, 28, 1953–1960. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.C.; Klipping, C.; Nguyen, A.M.; Frenkl, T.L.; Cruz, S.M.; Wang, Y.; Korver, T. A phase 2b multicenter, randomized, double-blind, placebo-controlled clinical trial to evaluate the efficacy and safety of vaginal rings containing nomegestrol acetate or etonogestrel and 17β-estradiol in the treatment of women with primary dysmenorrhea. Contraception 2019, 99, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.R.; Prabhakar, B.; Wairkar, S. Non-oral routes, novel formulations and devices of contraceptives: An update. J. Control. Release 2022, 345, 798–810. [Google Scholar] [CrossRef]
- dos Santos, L.B.; Ferreira, C.W.S.; Gonçalves, C.G.; Xavier, M.A.D.O.; Dantas, J.H.; Barbosa, I.R.; da Câmara, S.M.A.; Dantas, D. Association among dysmenorrhea and activity limitation and participation restrictions in adult women: A cross-sectional study, Brazil -2017. Arch. Public Health 2021, 79, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fraser, I.S.; Critchley, H.; Munro, M.; Broder, M. Can we achieve international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding? Hum. Reprod. 2007, 22, 635–643. [Google Scholar] [CrossRef]
- Bajaj, P.; Bajaj, P.; Madsen, H.; Arendt-Nielsen, L. A Comparison of Modality-Specific Somatosensory Changes During Menstruation in Dysmenorrheic and Nondysmenorrheic Women. Clin. J. Pain 2002, 18, 180–190. [Google Scholar] [CrossRef]
- Vatine, J.-J.; Shapira, S.C.; Magora, F.; Adler, D.; Magora, A. Electronic pressure algometry of deep pain in healthy volunteers. Arch. Phys. Med. Rehabil. 1993, 74, 526–530. [Google Scholar] [CrossRef]
- Amodei, N.; Nelson-Gray, R.O. Reactions of dysmenorrheic and nondysmenorrheic women to experimentally induced pain throughout the menstrual cycle. J. Behav. Med. 1989, 12, 373–385. [Google Scholar] [CrossRef]
- Tassorelli, C.; Sandrini, G.; Proietti Cecchini, A.; Nappi, R.E.; Sances, G.; Martignoni, E. Changes in Nociceptive Flexion Reflex Threshold Across the Menstrual Cycle in Healthy Women. Psychosom. Med. 2002, 64, 621–626. [Google Scholar] [CrossRef]
- Fischer, A.A. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain 1987, 30, 115–126. [Google Scholar] [CrossRef]
- Kosek, E.; Ekholm, J.; Hansson, P. Pressure Pain Thresholds in Different Tissues in One Body Region. The Influence of Skin Sensitivity in Pressure Algometry. Scand. J. Rehabil. Med. 1999, 31, 89–93. [Google Scholar] [CrossRef]
- Isselée, H.; Laat, A.; Bogaerts, K.; Lysens, R. Long-term fluctuations of pressure pain thresholds in healthy men, normally menstruating women and oral contraceptive users. Eur. J. Pain 2001, 5, 27–37. [Google Scholar] [CrossRef]
- Chesterton, L.S.; Sim, J.; Wright, C.C.; Foster, N.E. Interrater Reliability of Algometry in Measuring Pressure Pain Thresholds in Healthy Humans, Using Multiple Raters. Clin. J. Pain 2007, 23, 760–766. [Google Scholar] [CrossRef]
- Isselée, H.; Laat, A.; Lesaffre, E.; Lysens, R. Short-term reproducibility of pressure pain thresholds in masseter and temporalis muscles of symptom-free subjects. Eur. J. Oral Sci. 1997, 105, 583–587. [Google Scholar] [CrossRef]
- Nussbaum, E.L.; Downes, L. Reliability of Clinical Pressure-Pain Algometric Measurements Obtained on Consecutive Days. Phys. Ther. 1998, 78, 160–169. [Google Scholar] [CrossRef]
- As-Sanie, S.; Harris, R.E.; Harte, S.E.; Tu, F.F.; Neshewat, G.; Clauw, D.J. Increased Pressure Pain Sensitivity in Women With Chronic Pelvic Pain. Obstet. Gynecol. 2013, 122, 1047–1055. [Google Scholar] [CrossRef]
- Fenton, B.W.; Palmieri, P.A.; Durner, C.; Fanning, J. Quantification of Abdominal Wall Pain Using Pain Pressure Threshold Algometry in Patients with Chronic Pelvic Pain. Clin. J. Pain 2009, 25, 500–505. [Google Scholar] [CrossRef]
- Giamberardino, M.A.; Berkley, K.J.; Iezzi, S.; de Bigontina, P.; Vecchiet, L. Pain threshold variations in somatic wall tissues as a function of menstrual cycle, segmental site and tissue depth in non-dysmenorrheic women, dysmenorrheic women and men. Pain 1997, 71, 187–197. [Google Scholar] [CrossRef]
- Granot, M.; Yarnitsky, D.; Itskovitz-Eldor, J.; Granovsky, Y.; Peer, E.; Zimmer, E.Z. Pain perception in women with dysmenorrhea. Obstet. Gynecol. 2001, 98, 407–411. [Google Scholar] [CrossRef]
- Costantini, R.; Affaitati, G.; Fiordaliso, M.; Giamberardino, M.A. Viscero-visceral hyperalgesia in dysmenorrhoea plus previous urinary calculosis: Role of myofascial trigger points and their injection treatment in the referred area. Eur. J. Pain 2020, 24, 933–944. [Google Scholar] [CrossRef]
- Isselée, H.; de Laat, A.; de Mot, B.; Lysens, R. Pressure-pain threshold variation in temporomandibular disorder myalgia over the course of the menstrual cycle. J. Orofac. Pain 2002, 16, 105–117. [Google Scholar] [PubMed]
- Sherman, J.J.; LeResche, L. Does experimental pain response vary across the menstrual cycle? A methodological review. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 291, R245–R256. [Google Scholar] [CrossRef] [PubMed]
- Payne, L.A.; Seidman, L.C.; Sim, M.-S.; Rapkin, A.J.; Naliboff, B.D.; Zeltzer, L.K. Experimental evaluation of central pain processes in young women with primary dysmenorrhea. Pain 2019, 160, 1421–1430. [Google Scholar] [CrossRef] [PubMed]
- Stratton, P.; Khachikyan, I.; Sinaii, N.; Ortiz, R.; Shah, J. Association of Chronic Pelvic Pain and Endometriosis With Signs of Sensitization and Myofascial Pain. Obstet. Gynecol. 2015, 125, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Pastore, E.A.; Katzman, W.B. Recognizing Myofascial Pelvic Pain in the Female Patient with Chronic Pelvic Pain. J. Obstet. Gynecol. Neonatal Nurs. 2012, 41, 680–691. [Google Scholar] [CrossRef]
- Bedaiwy, M.; Patterson, B.; Mahajan, S. Prevalence of myofascial chronic pelvic pain and the effectiveness of pelvic floor physical therapy. J. Reprod. Med. 2013, 58, 504–510. [Google Scholar]
- Montenegro, M.L.L.S.; Braz, C.A.; Rosa-E-Silva, J.C.; Candido-Dos-Reis, F.J.; Nogueira, A.A.; Poli-Neto, O.B. Anaesthetic injection versus ischemic compression for the pain relief of abdominal wall trigger points in women with chronic pelvic pain. BMC Anesthesiol. 2015, 15, 1–8. [Google Scholar] [CrossRef]
- Sedighimehr, N.; Manshadi, F.D.; Shokouhi, N.; Baghban, A.A. Pelvic musculoskeletal dysfunctions in women with and without chronic pelvic pain. J. Bodyw. Mov. Ther. 2018, 22, 92–96. [Google Scholar] [CrossRef]
- Howard, F. Pelvic Pain: Diagnosis and Management; Lippincott Williams & Wilkins: Baltimore, PA, USA, 2000. [Google Scholar]
- Tu, F.; Kane, J.; Hellman, K. Noninvasive experimental bladder pain assessment in painful bladder syndrome. BJOG Int. J. Obstet. Gynaecol. 2016, 124, 283–291. [Google Scholar] [CrossRef]
- Hetrick, D.C.; Ciol, M.; Rothman, I.; Turner, J.A.; Frest, M.; Berger, R.E. Musculoskeletal Dysfunction in Men with Chronic Pelvic Pain Syndrome Type III: A Case-control Study. J. Urol. 2003, 170, 828–831. [Google Scholar] [CrossRef]
- Montenegro, M.L.L.D.S.; Mateus-Vasconcelos, E.C.L.; Silva, J.C.R.E.; Nogueira, A.A.; Dos Reis, F.J.C.; Neto, O.B.P. Importance of Pelvic Muscle Tenderness Evaluation in Women with Chronic Pelvic Pain. Pain Med. 2010, 11, 224–228. [Google Scholar] [CrossRef]
- Fernández-Carnero, J.; Fernández-De-Las-Peñas, C.; de la Llave-Rincón, A.I.; Ge, H.-Y.; Arendt-Nielsen, L. Prevalence of and Referred Pain from Myofascial Trigger Points in the Forearm Muscles in Patients with Lateral Epicondylalgia. Clin. J. Pain 2007, 23, 353–360. [Google Scholar] [CrossRef]
- Ríos-León, M.; Ortega-Santiago, R.; Madeleine, P.; Fernández-De-Las-Peñas, C.; Plaza-Manzano, G. Topographical Pressure Pain Sensitivity Maps of the Feet Reveal Bilateral Pain Sensitivity in Patients with Unilateral Plantar Heel Pain. J. Orthop. Sports Phys. Ther. 2019, 49, 640–646. [Google Scholar] [CrossRef]
- Iglesias-González, J.J.; Muñoz-García, M.T.; Rodrigues-De-Souza, D.P.; Alburquerque-Sendín, F.; Fernández-De-Las-Peñas, C. Myofascial Trigger Points, Pain, Disability, and Sleep Quality in Patients with Chronic Nonspecific Low Back Pain. Pain Med. 2013, 14, 1964–1970. [Google Scholar] [CrossRef]
- Muñoz-Muñoz, S.; Muñoz-García, M.T.; Alburquerque-Sendín, F.; Arroyo-Morales, M.; Fernández-De-Las-Peñas, C. Myofascial Trigger Points, Pain, Disability, and Sleep Quality in Individuals with Mechanical Neck Pain. J. Manip. Physiol. Ther. 2012, 35, 608–613. [Google Scholar] [CrossRef]
- Shah, J.P.; Phillips, T.M.; Danoff, J.V.; Gerber, L. An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. J. Appl. Physiol. 2005, 99, 1977–1984. [Google Scholar] [CrossRef]
- Shah, J.P.; Danoff, J.V.; Desai, M.J.; Parikh, S.; Nakamura, L.Y.; Phillips, T.M.; Gerber, L. Biochemicals Associated with Pain and Inflammation are Elevated in Sites Near to and Remote From Active Myofascial Trigger Points. Arch. Phys. Med. Rehabil. 2008, 89, 16–23. [Google Scholar] [CrossRef]
- Ge, H.-Y.; Monterde, S.; Graven-Nielsen, T.; Arendt-Nielsen, L. Latent Myofascial Trigger Points Are Associated with an Increased Intramuscular Electromyographic Activity During Synergistic Muscle Activation. J. Pain 2014, 15, 181–187. [Google Scholar] [CrossRef]
- Quesada, S.A.; Arias-Buría, J.L.; Courtney, C.A.; Arendt-Nielsen, L.; Fernández-De-Las-Peñas, C. Exploration of Quantitative Sensory Testing in Latent Trigger Points and Referred Pain Areas. Clin. J. Pain 2018, 34, 409–414. [Google Scholar] [CrossRef]
- Kimura, Y.; Ge, H.-Y.; Zhang, Y.; Kimura, M.; Sumikura, H.; Arendt-Nielsen, L. Evaluation of sympathetic vasoconstrictor response following nociceptive stimulation of latent myofascial trigger points in humans. Acta Physiol. 2009, 196, 411–417. [Google Scholar] [CrossRef]
- Ibarra, J.M.; Ge, H.-Y.; Wang, C.; Vizcaino, V.M.; Graven-Nielsen, T.; Arendt-Nielsen, L. Latent Myofascial Trigger Points are Associated with an Increased Antagonistic Muscle Activity During Agonist Muscle Contraction. J. Pain 2011, 12, 1282–1288. [Google Scholar] [CrossRef] [PubMed]
- Itza, F.; Zarza, D.; Salinas, J.; Teba, F.; Ximenez, C. Turn-amplitude analysis as a diagnostic test for myofascial syndrome in patients with chronic pelvic pain. Pain Res. Manag. 2015, 20, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, D.R.; Berkoff, G.M. Myofascial Trigger Points Show Spontaneous Needle EMG Activity. Spine 1993, 18, 1803–1807. [Google Scholar] [CrossRef] [PubMed]
- Simons, D.G.; Hong, C.-Z.; Simons, L.S. Endplate Potentials Are Common to Midfiber Myofacial Trigger Points. Am. J. Phys. Med. Rehabilitation 2002, 81, 212–222. [Google Scholar] [CrossRef]
- Partanen, J.V.; Ojala, T.A.; Arokoski, J.P. Myofascial syndrome and pain: A neurophysiological approach. Pathophysiology 2010, 17, 19–28. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Madsen, H.; Jarrell, J.; Gregersen, H.; Drewes, A.M. Pain evoked by distension of the uterine cervix in women with dysmenorrhea: Evidence for central sensitization. Acta Obstet. Et Gynecol. Scand. 2014, 93, 741–748. [Google Scholar] [CrossRef]
- Iacovides, S.; Avidon, I.; Baker, F. Does pain vary across the menstrual cycle? A review. Eur. J. Pain 2015, 19, 1389–1405. [Google Scholar] [CrossRef]
- LeResche, L.; Mancl, L.; Sherman, J.J.; Gandara, B.; Dworkin, S.F. Changes in temporomandibular pain and other symptoms across the menstrual cycle. Pain 2003, 106, 253–261. [Google Scholar] [CrossRef]
- Bartley, E.J.; Rhudy, J.L. Comparing Pain Sensitivity and the Nociceptive Flexion Reflex Threshold Across the Mid-follicular and Late-luteal Menstrual Phases in Healthy Women. Clin. J. Pain 2013, 29, 154–161. [Google Scholar] [CrossRef]
- Schmalenberger, K.M.; Tauseef, H.A.; Barone, J.C.; Owens, S.A.; Lieberman, L.; Jarczok, M.N.; Girdler, S.S.; Kiesner, J.; Ditzen, B.; Eisenlohr-Moul, T.A. How to Study the Menstrual Cycle: Practical Tools and Recommendations. Psychoneuroendocrinology 2021, 123, 104895. [Google Scholar] [CrossRef]
- MacLean, J.A.; Hayashi, K. Progesterone Actions and Resistance in Gynecological Disorders. Cells 2022, 11, 647. [Google Scholar] [CrossRef]
- Hassan, S.; Muere, A.; Einstein, G. Ovarian hormones and chronic pain: A comprehensive review. Pain 2014, 155, 2448–2460. [Google Scholar] [CrossRef]
- Rezaii, T.; Hirschberg, A.L.; Carlström, K.; Ernberg, M. The Influence of Menstrual Phases on Pain Modulation in Healthy Women. J. Pain 2012, 13, 646–655. [Google Scholar] [CrossRef]
- Christin-Maitre, S. Human Menstrual Cycle. In Encyclopedia of Endocrine Diseases; Academic Press: Cambridge, MA, USA, 2018; pp. 399–403. [Google Scholar] [CrossRef]
- Greenwald, J.D.; Shafritz, K.M. An Integrative Neuroscience Framework for the Treatment of Chronic Pain: From Cellular Alterations to Behavior. Front. Integr. Neurosci. 2018, 12, 18. [Google Scholar] [CrossRef]
- Wang, C.; Ge, H.-Y.; Ibarra, J.M.; Yue, S.-W.; Madeleine, P.; Arendt-Nielsen, L. Spatial Pain Propagation Over Time Following Painful Glutamate Activation of Latent Myofascial Trigger Points in Humans. J. Pain 2012, 13, 537–545. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Dommerholt, J. Myofascial Trigger Points: Peripheral or Central Phenomenon? Curr. Rheumatol. Rep. 2014, 16, 1–6. [Google Scholar] [CrossRef]
- Ge, H.-Y.; Fernández-De-Las-Peñas, C.; Yue, S.-W. Myofascial trigger points: Spontaneous electrical activity and its consequences for pain induction and propagation. Chin. Med. 2011, 6, 13. [Google Scholar] [CrossRef]
- Ge, H.-Y.; Nie, H.; Madeleine, P.; Danneskiold-Samsøe, B.; Graven-Nielsen, T.; Arendt-Nielsen, L. Contribution of the local and referred pain from active myofascial trigger points in fibromyalgia syndrome. Pain 2009, 147, 233–240. [Google Scholar] [CrossRef]
- McPartland, J.M.; Simons, D.G. Myofascial Trigger Points: Translating Molecular Theory into Manual Therapy. J. Man. Manip. Ther. 2006, 14, 232–239. [Google Scholar] [CrossRef]
- Bartley, E.J.; Fillingim, R.B. Sex differences in pain: A brief review of clinical and experimental findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Pieretti, S.; Di Giannuario, A.; Di Giovannandrea, R.; Marzoli, F.; Piccaro, G.; Minosi, P.; Aloisi, A.M. Gender differences in pain and its relief. Ann. Dell’istituto Super. Di Sanita 2016, 52, 184–189. [Google Scholar] [CrossRef]
- Schwartz, E.S.; Gebhart, G.F. Visceral Pain. Curr. Top Behav. Neurosci. 2014, 20, 171–197. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.M. Basic neuroanatomy for understanding pelvic pain. J. Am. Assoc. Gynecol. Laparosc. 1999, 6, 15–29. [Google Scholar] [CrossRef]
- Sánchez-García, O.; López-Juárez, R.; Corona-Quintanilla, D.L.; Ruiz, C.; Martínez-Gómez, M.; Cuevas-Romero, E.; Castelán, F. Estrogens influence differentially on the pelvic floor muscles activation at somatovisceral reflexes involved in micturition of rabbits. Menopause 2021, 28, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, S.A.; Weiss, J.M. Screening for Musculoskeletal Causes of Pelvic Pain. Clin. Obstet. Gynecol. 2003, 46, 773–782. [Google Scholar] [CrossRef]
- Tu, C.-H.; Niddam, D.M.; Chao, H.-T.; Liu, R.-S.; Hwang, R.-J.; Yeh, T.-C.; Hsieh, J.-C. Abnormal cerebral metabolism during menstrual pain in primary dysmenorrhea. NeuroImage 2009, 47, 28–35. [Google Scholar] [CrossRef]
- Vincent, K.; Warnaby, C.; Stagg, C.; Moore, J.; Kennedy, S.; Tracey, I. Dysmenorrhoea is associated with central changes in otherwise healthy women. Pain 2011, 152, 1966–1975. [Google Scholar] [CrossRef]
- Iacovides, S.; Baker, F.C.; Avidon, I.; Bentley, A. Women with Dysmenorrhea Are Hypersensitive to Experimental Deep Muscle Pain Across the Menstrual Cycle. J. Pain 2013, 14, 1066–1076. [Google Scholar] [CrossRef]
- Oladosu, F.A.; Hellman, K.M.; Ham, P.J.; Kochlefl, L.E.; Datta, A.; Garrison, E.F.; Steiner, N.D.; Roth, G.E.; Tu, F.F. Persistent autonomic dysfunction and bladder sensitivity in primary dysmenorrhea. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | NDNC | NDWC | WDNC | WDWC | p-Value * F (η2) | |
|---|---|---|---|---|---|---|
| Mean ± SD (99% CI, n = 84) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | ||
| Age (years) | 31.20 ± 7.65 (28.99–33.40) | 35.47 ± 9.36 (29.65–41.29) | 30.57 ± 5.57 (27.11–34.03) | 30.71 ± 7.65 (25.96–35.46) | 28.04 ± 5.97 (28.99–33.40) | p = 0.013 F = 3.792 η2 = 0.124 |
| Weight (kg) | 58.22 ± 6.50 (56.35–60.09) | 61.08 ± 8.42 (55.84–66.31) | 57.23 ± 4.04 (54.72–59.75) | 56.80 ± 5.68 (53.27–60.34) | 57.76 ± 6.60 (53.65–61.86) | p = 0.129 F = 1.944 η2 = 0.068 |
| Height (m) | 1.64 ± 0.04 (1.63–1.65) | 1.64 ± 0.04 (1.61–1.67) | 1.65 ± 0.03 (1.63–1.67) | 1.63 ± 0.03 (1.60–1.65) | 1.65 ± 0.05 (1.61–1.68) | p= 0.334 F = 1.151 η2 = 0.041 |
| BMI (Kg/m2) | 21.51 ± 2.25 (20.87–22.16) | 22.61 ± 3.26 20.59–24.64) | 20.93 ± 1.79 (19.82–22.05) | 21.31 ± 1.28 (20.52–22.11) | 21.20 ± 1.96 (19.98–22.42) | p= 0.070 F = 2.441 η2 = 0.084 |
| Total (n = 84) | NDNC (n = 21) | NDWC (n = 21) | WDNC (n = 21) | WDWC (n = 21) | p-Value * χ2 | ||
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Contraceptive treatment | YES | 42 (50) | 0 (0) | 21 (100) | 0 (0) | 21 (100) | p < 0.001 χ2 = 80.188 |
| NO | 42 (50) | 21 (100) | 0 (0) | 21 (100) | 0 (0) | ||
| Type of contraceptive treatment | NO TRT | 42 (50) | 21 (100) | 0 (0) | 21 (100) | 0 (0) | p < 0.001 χ2 = 83.765 |
| RING | 11 (13.10) | 0 (0) | 7 (33.33) | 0 (0) | 4 (19.05) | ||
| IUD | 6 (7.14) | 0 (0) | 2 (9.52) | 0 (0) | 4 (19.05) | ||
| COCs | 25 (29.76) | 0 (0) | 12 (57.14) | 0 (0) | 13 (61.90) | ||
| Low back pain | YES | 42 (50) | 9 (42.86) | 9 (42.86) | 16 (76.19) | 8 (9.52) | p = 0.05 χ2 = 7.81 |
| NO | 42 (50) | 12 (57.14) | 12 (57.14) | 5 (23.81) | 13 (61.90) | ||
| Pelvic pain | YES | 24 (28.57) | 5 (23.81) | 6 (7.14) | 8 (9.52) | 5 (23.81) | p = 0.706 χ2 = 1.400 |
| NO | 60 (71.43) | 16 (76.19) | 15 (71.43) | 13 (61.90) | 16 (76.19) | ||
| GI symptoms during menstruation | YES | 53 (63.10) | 15 (71.43) | 7 (33.33) | 17 (20.24) | 14 (66.67) | p < 0.01 * χ2 = 11.606 |
| NO | 31 (36.90) | 6 (7.14) | 14 (66.67) | 4 (19.05) | 7 (33.33) | ||
| Common GI symptoms | YES | 13 (15.48) | 4 (19.05) | 5 (23.81) | 1 (4.76) | 3 (14.28) | p = 0.364 χ2 = 3.185 |
| NO | 71 (84.52) | 17 (20.24) | 16 (76.19) | 20 (95.24) | 18 (85.71) | ||
| Dyspareunia | YES | 25 (29.76) | 6 (7.14) | 7 (33.33) | 6 (7.14) | 6 (7.14) | p = 0.982 χ2 = 0.171 |
| NO | 59 (70.24) | 15 (71.43) | 14 (66.67) | 15 (71.43) | 15 (71.43) | ||
| Menstrual pain | YES | 58 (69.05) | 9 (42.86) | 7 (33.33) | 21 (100) | 21 (100) | p < 0.001 * χ2 = 34.659 |
| NO | 26 (30.95) | 12 (57.14) | 14 (66.67) | 0 (0) | 0 (0) | ||
| Menstrual Pain Treatment | Heat | 2 (2.38) | 0 (0) | 1 (4.76) | 1 (4.76) | 0 (0) | p < 0.144 χ2 = 17.147 |
| Medication | 26 (30.95) | 7 (33.33) | 3 (14.28) | 8 (9.52) | 8 (9.52) | ||
| Heat and medication | 24 (28.57) | 2 (9.52) | 1 (4.76) | 10 (47.62) | 11 (52.38) | ||
| Kinesiotape | 2 (2.38) | 0 (0) | 1 (4.76) | 0 (0) | 1 (4.76) | ||
| Total | NDNC | NDWC | WDNC | WDWC | p-Value * F (η2) | Post-Hoc P (d Cohen) a-NDNC vs. NDWC b-NDNC vs. WDNC c-NDNC vs. WDWC d-NDWC vs. WDNC e-NDWC vs. WDWC f-WDNC vs. WDWC | |
|---|---|---|---|---|---|---|---|
| Mean ± SD (99% CI, n = 84) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | |||
| Physical Health | 18.07 ± 1.81 (17.54–18.59) | 18.09 ± 2.02 (16.83–19.35) | 18.95 ± 1.20 (18.20–19.69) | 16.85 ± 2.15 (15.52–18.19) | 18.38 ± 1.02 (17.74–19.01) | p = 0.001 * F = 5.860 η2 = 0.180 | a-p = 0.606 d = 0.517 b-p = 0.113 d = 0.594 c-p = 1.000 d = 0.181 d-p = 0.001 d = 1.206 e-p = 1.000 d = 0.511 f-p = 0.025 d = 0.909 |
| Physical Health (%) | 86.36 ± 12.98 (82.63–90.10) | 86.52 ± 14.43 (77.55–95.48) | 92.61 ± 8.58 (87.28–97.95) | 77.71 ± 15.46 (68.11–87.31) | 88.61 ± 7.28 (84.09–93.14) | p = 0.001 * F = 5.805 η2 = 0.179 | a-p = 0.619 d = 0.513 b-p = 0.117 d = 0.589 c-p = 1.000 d = 0.182 d-p = 0.001 d = 1.191 e-p = 1.000 d = 0.502 f-p = 0.025 d = 0.902 |
| Mental Health | 20.90 ± 3.13 (20.00–21.80) | 20.04 ± 3.98 (17.57–22.51) | 22.61 ± 2.13 (21.29–23.94) | 20.38 ± 2.97 (18.53–22.22) | 20.57 ± 2.71 (18.88–22.25) | p = 0.31 F = 3.105 η2 = 0.104 | a-p = 0.044 d = 0.805 b-p = 1.000 d = 0.096 c-p = 1.000 d = 0.155 d-p = 0.113 d = 0.862 e-p = 0.187 d = 0.836 f-p = 1.000 d = 0.066 |
| Mental Health (%) | 71.00 ± 14.90 (66.71–75.28) | 66.90 ± 18.88 (55.18–78.62) | 79.19 ± 10.12 (72.90–85.47) | 68.42 ± 14.04 (59.70–77.15) | 69.47 ± 12.94 (61.43–77.51) | p = 0.029 F = 3.153 η2 = 0.106 | a-p = 0.041 d = 0.811 b-p = 1.000 d = 0.091 c-p = 1.000 d = 0.158 d-p = 0.104 d = 0.880 e-p = 0.187 d = 0.836 f-p = 1.000 d = 0.077 |
| Total | 38.97 ± 3.92 (37.84–40.10) | 38.14 ± 4.74 (35.19–41.08) | 41.57 ± 2.80 (39.83–43.31) | 37.23 ± 3.92 (34.80–39.67) | 38.95 ± 2.65 (37.30–40.60) | p = 0.002 * F = 5.54 η2 = 0.172 | a-p = 0.018 d = 0.881 b-p = 1.000 d = 0.209 c-p = 1.000 d = 0.210 d-p = 0.001 d = 1.274 e-p = 0.132 d = 0.961 f-p = 0.782 d = 0.514 |
| Total (%) | 77.05 ± 11.15 (73.84–80.26) | 74.71 ± 13.57 (66.28–83.14) | 84.38 ± 7.93 (79.45–89.30) | 72.19 ± 11.14 (65.27–79.10) | 76.95 ± 7.63 (72.21–81.69) | p = 0.002 * F = 5.396 η2 = 0.168 | a-p = 0.020 d = 0.870 b-p = 1.000 d = 0.202 c-p = 1.000 d = 0.203 d-p = 0.002 d = 1.260 e-p = 0.137 d = 0.954 f-p = 0.843 d = 0.498 |
| Total | NDNC | NDWC | WDNC | WDWC | p-Value * F (η2) | Post-Hoc P (d Cohen) a-NDNC vs. NDWC b-NDNC vs. WDNC c-NDNC vs. WDWC d-NDWC vs. WDNC e-NDWC vs. WDWC f-WDNC vs. WDWC | |
|---|---|---|---|---|---|---|---|
| Mean ± SD (99% CI, n = 84) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | Mean ± SD (99% CI, n = 21) | |||
| PRI-S | 14.92 ± 10.34 (11.95–17.90) | 11.61 ± 8.89 (6.08–17.13) | 5.61 ± 6.93 (1.31–9.92) | 22.52 ± 9.02 (16.92–28.12) | 19.95 ± 6.77 (15.74–24.15) | p = 0.000 * F = 19.879 η2 = 0.427 | a-p = 0.102 d = 0.752 b-p = 0.000 d = 1.218 c-p = 0.007 d = 1.055 d-p = 0.000 d = 2.102 e-p = 0.000 d = 2.093 f-p = 1.000 d = 0.326 |
| PRI-A | 1.17 ± 1.48 (0.75–1.60) | 0.76 ± 0.83 (0.24–1.27) | 0.19 ± 0.40 (−0.05–0.44) | 2.14 ± 1.87 (0.97–3.30) | 1.61 ± 1.53 (0.66–2.57) | p = 0.000 * F = 9.462 η2 = 0.262 | a-p = 0.944 d = 0.874 b-p = 0.005 d = 0.953 c-p = 0.212 d = 0.690 d-p = 0.000 d = 1.442 e-p = 0.004 d = 1.269 f-p = 1.000 d = 0.310 |
| PRI-E | 1.85 ± 1.28 (1.48–2.22) | 1.61 ± 0.97 (1.01–2.22) | 0.61 ± 0.86 (0.08–1.15) | 2.95 ± 1.07 (2.28–3.61) | 2.23 ± 0.94 (1.65–2.82) | p = 0.000 * F = 22.007 η2 = 0.452 | a-p = 0.007 d = 1.090 b-p = 0.000 d = 1.312 c-p = 0.246 d = 0.649 d-p = 0.000 d = 2.410 e-p = 0.000 d = 1.798 f-p = 0.114 d = 0.714 |
| PRI-Total | 17.96 ± 12.34 (14.41–21.51) | 14.09 ± 10.46 (7.59–20.59) | 6.33 ± 7.85 (1.45–11.21) | 27.47 ± 9.97 (21.28–33.66) | 23.95 ± 8.43 (18.71–29.18) | p = 0.000 * F = 22.649 η2 = 0.459 | a-p = 0.048 d = 0.839 b-p = 0.000 d = 1.309 c- p = 0.005 d = 1.037 d-p = 0.000 d = 2.356 e-p = 0.000 d = 2.163 f-p = 1.000 d = 0.381 |
| Nº of words | 8.38 ± 4.61 (7.05–9.70) | 7.19 ± 4.26 (4.54–9.83) | 4.38 ± 4.34 (1.68–7.07) | 11.09 ± 3.46 (8.94–13.24) | 10.85 ± 2.63 (9.22–12.49) | p = 0.000 * F = 15.478 η2 = 0.367 | a-p = 0.103 d = 0.653 b-p = 0.007 d = 1.004 c-p = 0.013 d = 1.033 d-p = 0.000 d = 1.709 e-p = 0.000 d = 1.803 f-p = 1.000 d = 0.078 |
| PPI | 1.63 ± 1.01 (1.33–1.92) | 1.19 ± 0.51 (0.87–1.50) | 0.90 ± 0.62 (0.51–1.29) | 2.66 ± 1.15 (1.94–3.38) | 1.76 ± 0.62 (1.37–2.14) | p = 0.000 * F = 21.343 η2 = 0.445 | a-p = 1.000 d = 0.510 b-p = 0.000 d = 1.652 c-p = 0.112 d = 1.004 d-p = 0.000 d = 1.905 e-p = 0.003 d = 1.387 f-p = 0.002 d = 0.974 |
| Muscles | Presence of MTrPs | Total (n = 84) | NDNC (n = 21) | NDWC (n = 21) | WDNC (n = 21) | WDWC (n = 21) | p-Value * χ2 |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Rectus abdominis | Does not have | 7 (8.33) | 4 (19.04) | 3 (14.28) | 0 | 0 | p < 0.001 * χ2 = 25.510 |
| Active | 28 (33.33) | 2 (9.52) | 2 (9.52) | 11 (52.38) | 13 (61.90) | ||
| Latent | 49 (58.33) | 15 (71.42) | 16 (76.19) | 10 (47.61) | 8 (38.09) | ||
| External oblique | Does not have | 13 (15.47) | 6 (28.57) | 4 (19.04) | 2 (9.52) | 1 (4.76) | p = 0.082 χ2 = 11.230 |
| Active | 10 (11.90) | 3 (14.28) | 0 | 5 (23.80) | 2 (9.52) | ||
| Latent | 61 (72.61) | 12 (57.14) | 17 (80.95) | 14 (66.66) | 18 (85.71) | ||
| Internal oblique | Does not have | 34 (40.47) | 13 (61.90) | 11 (52.38) | 3 (14.28) | 7 (33.33) | p = 0.015 χ2 = 15.827 |
| Active | 23 (27.38) | 1 (4.76) | 4 (19.04) | 10 (47.61) | 8 (38.09) | ||
| Latent | 27 (32.14) | 7 (33.33) | 6 (28.57) | 8 (38.09) | 6 (28.57) | ||
| Adductor magnus | Does not have | 6 (7.14) | 3 (14.28) | 0 | 1 (4.76) | 2 (9.52) | p = 0.132 χ2 = 9.820 |
| Active | 4 (4.76) | 0 | 0 | 3 (14.28) | 1 (4.76) | ||
| Latent | 74 (88.09) | 18 (85.71) | 21 (100) | 17 (80.95) | 18 (85.71) | ||
| Gluteus maximus | Does not have | 17 (20.23) | 5 (23.80) | 9 (42.85) | 2 (9.52) | 1 (4.76) | p < 0.01 * χ2 = 19.280 |
| Active | 7 (8.33) | 0 | 1 (4.76) | 1 (4.76) | 5 (23.80) | ||
| Latent | 60 (71.42) | 16 (76.19) | 11 (52.38) | 18 (85.71) | 15 (71.42) | ||
| Gluteus medius | Does not have | 9 (10.71) | 4 (19.04) | 3 (14.28) | 0 | 2 (9.52) | p = 0.042 χ2 = 13.053 |
| Active | 8 (9.52) | 0 | 0 | 5 (23.80) | 3 (14.28) | ||
| Latent | 67 (79.76) | 17 (80.95) | 18 (85.71) | 16 (76.19) | 16 (76.19) | ||
| Gluteus minimus | Does not have | 13 (15.47) | 5 (23.80) | 5 (23.80) | 2 (9.52) | 1 (4.76) | p = 0.219 χ2 = 8.269 |
| Active | 5 (5.95) | 1 (4.76) | 0 | 3 (14.28) | 1 (4.76) | ||
| Latent | 66 (78.57) | 15 (71.42) | 16 (76.19) | 16 (76.19) | 19 (90.47) | ||
| Quadratus lumborum | Does not have | 4 (4.76) | 3 (14.28) | 0 | 1 (4.76) | 0 | p = 0.067 χ2 = 11.762 |
| Active | 24 (28.57) | 3 (14.28) | 4 (19.04) | 9 (42.85) | 8 (38.09) | ||
| Latent | 56 (66.66) | 15 (71.42) | 17 (80.95) | 11 (52.38) | 13 (61.90) | ||
| Piriformis | Does not have | 4 (4.76) | 1 (4.76) | 1 (4.76) | 0 | 2 (9.52) | p = 0.082 χ2 = 11.209 |
| Active | 28 (33.33) | 4 (19.04) | 4 (19.04) | 12 (57.14) | 8 (38.09) | ||
| Latent | 52 (61.90) | 16 (76.19) | 16 (76.19) | 9 (42.85) | 11 (52.38) | ||
| Muscles | Presence of MTrPs | Total(n = 84) | NDNC(n = 21) | NDWC(n = 21) | WDNC(n = 21) | WDWC(n = 21) | p-Value * χ2 |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Ischiocavernosus | Does not have | 27 (32.14) | 10 (47.61) | 12 (57.14) | 2 (9.52) | 3 (14.28) | p < 0.01 * χ2 = 20.680 |
| Active | 7 (8.33) | 0 | 0 | 3 (14.28) | 4 (19.04) | ||
| Latent | 50 (59.52) | 11 (52.38) | 9 (42.85) | 16 (76.19) | 14 (66.66) | ||
| Bulbospongiosus | Does not have | 39 (46.42) | 13 (61.90) | 13 (61.90) | 8 (38.09) | 5 (23.80) | p = 0.125 χ2 = 9.990 |
| Active | 4 (4.76) | 0 | 1 (4.76) | 1 (4.76) | 2 (9.52) | ||
| Latent | 41 (48.80) | 8 (38.09) | 7 (33.33) | 12 (57.14) | 14 (66.66) | ||
| Transverse perineal | Does not have | 37 (44.04) | 12 (57.14) | 12 (57.14) | 7 (33.33) | 6 (28.57) | p = 0.043 χ2 = 12.972 |
| Active | 5 (5.95) | 0 | 0 | 1 (4.76) | 4 (19.04) | ||
| Latent | 42 (50) | 9 (42.85) | 9 (42.85) | 13 (61.90) | 11 (52.38) | ||
| Puborectalis | Does not have | 12 (14.28) | 6 (28.57) | 4 (19.04) | 1 (4.76) | 1 (4.76) | p = 0.268 χ2 = 7.610 |
| Active | 28 (33.33) | 5 (23.80) | 6 (28.57) | 9 (42.85) | 8 (38.09) | ||
| Latent | 44 (52.38) | 10 (47.61) | 11 (52.38) | 11 (52.38) | 12 (57.14) | ||
| Pubococcygeus | Does not have | 6 (7.14) | 5 (23.80) | 0 | 0 | 1 (4.76) | p = 0.001 * χ2 = 22.140 |
| Active | 41 (48.80) | 7 (33.33) | 6 (28.57) | 14 (66.66) | 14 (66.66) | ||
| Latent | 37 (44.04) | 9 (42.85) | 15 (71.42) | 7 (33.33) | 6 (28.57) | ||
| Iliococcygeus | Does not have | 1 (1.19) | 1 (4.76) | 0 | 0 | 0 | p = 0.035 χ2 = 13.539 |
| Active | 58 (69.04) | 12 (57.14) | 11 (52.38) | 20 (95.23) | 15 (71.42) | ||
| Latent | 25 (29.76) | 8 (38.09) | 10 (47.61) | 1 (4.76) | 6 (28.57) | ||
| Obturator internus | Does not have | 0 | 0 | 0 | 0 | 0 | p = 0.110 χ2 = 6.024 |
| Active | 35 (41.66) | 6 (28.57) | 6 (28.57) | 11 (52.38) | 12 (57.14) | ||
| Latent | 49 (58.33) | 15 (71.42) | 15 (71.42) | 10 (47.61) | 9 (42.85) | ||
| Coccygeus | Does not have | 32 (38.09) | 9 (42.85) | 8 (38.09) | 8 (38.09) | 7 (33.33) | p = 0.274 χ2 = 7.532 |
| Active | 13 (15.47) | 3 (14.28) | 0 | 4 (19.04) | 6 (28.57) | ||
| Latent | 39 (46.42) | 9 (42.85) | 13 (61.90) | 9 (42.85) | 8 (38.09) | ||
| Anal sphincter | Does not have | 58 (69.04) | 12 (57.14) | 16 (76.19) | 15 (71.42) | 15 (71.42) | p = 0.774 χ2 = 3.268 |
| Active | 5 (5.95) | 1 (4.76) | 1 (4.76) | 2 (9.52) | 1 (4.76) | ||
| Latent | 21 (25) | 8 (38.09) | 4 (19.04) | 4 (19.04) | 5 (23.80) |
| Muscles | Presence of MTrPs | Total (n = 84) | NDNC (n = 21) | NDWC (n = 21) | WDNC (n = 21) | WDWC (n = 21) | p-Value * χ2 |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Rectus abdominis | Does not have | 13 (15.47) | 6 (28.57) | 3 (14.28) | 1 (4.76) | 3 (14.28) | p = 0.073 χ2 = 11.554 |
| Active | 3 (3.57) | 3 (14.28) | 0 | 4 (19.04) | 6 (28.57) | ||
| Latent | 58 (69.04) | 12 (57.14) | 18 (85.71) | 16 (76.19) | 12 (57.14) | ||
| External oblique | Does not have | 20 (23.80) | 7 (33.33) | 5 (23.80) | 3 (14.28) | 5 (23.80) | p = 0.216 χ2 = 8.310 |
| Active | 2 (2.38) | 0 | 0 | 0 | 2 (9.52) | ||
| Latent | 62 (73.80) | 14 (66.66) | 16 (76.19) | 18 (85.71) | 14 (66.66) | ||
| Internal oblique | Does not have | 55 (65.47) | 17(80.95) | 18 (85.71) | 10 (47.61) | 10 (47.61) | p = 0.021 χ2 = 14.959 |
| Active | 10 (11.90) | 0 | 2 (9.52) | 3 (14.28) | 5 (23.80) | ||
| Latent | 19 (22.61) | 4 (19.04) | 1 (4.76) | 8 (38.09) | 6 (28.57) | ||
| Adductor magnus | Does not have | 14 (16.66) | 5 (23.80) | 5 (23.80) | 0 | 4 (19.04) | p = 0.177 χ2 = 8.944 |
| Active | 1 (1.19) | 0 | 0 | 0 | 1 (4.76) | ||
| Latent | 69 (82.14) | 16 (76.19) | 16 (76.19) | 21 (100) | 16 (76.19) | ||
| Gluteus maximus | Does not have | 19 (22.61) | 6 (28.57) | 7 (33.33) | 3 (14.28) | 3 (14.28) | p = 0.683 χ2 = 3.951 |
| Active | 5 (5.95) | 1 (4.76) | 1 (4.76) | 2 (9.52) | 1 (4.76) | ||
| Latent | 60 (71.42) | 14 (66.66) | 13 (61.90) | 16 (76.19) | 17(80.95) | ||
| Gluteus medius | Does not have | 20 (23.80) | 4 (19.04) | 9 (42.85) | 3 (14.28) | 4 (19.04) | p = 0.379 χ2 = 6.407 |
| Active | 5 (5.95) | 1 (4.76) | 1 (4.76) | 1 (4.76) | 2 (9.52) | ||
| Latent | 59 (70.23) | 16 (76.19) | 11 (52.38) | 17 (80.95) | 15 (71.42) | ||
| Gluteus minimus | Does not have | 16 (19.04) | 5 (23.80) | 6 (28.57) | 2 (9.52) | 3 (14.28) | p = 0.500 χ2 = 4.875 |
| Active | 4 (4.76) | 1 (4.76) | 0 | 1 (4.76) | 2 (9.52) | ||
| Latent | 64 (76.19) | 15 (71.42) | 15 (71.42) | 18 (85.71) | 16 (76.19) | ||
| Quadratus lumborum | Does not have | 10 (11.90) | 4 (19.04) | 2 (9.52) | 3 (14.28) | 1 (4.76) | p = 0.082 χ2 = 11.209 |
| Active | 15 (17.85) | 4 (19.04) | 1 (4.76) | 2 (9.52) | 8 (38.09) | ||
| Latent | 59 (70.23) | 13 (61.90) | 18 (85.71) | 16 (76.19) | 12 (57.14) | ||
| Piriformis | Does not have | 17 (20.23) | 5 (23.80) | 3 (14.28) | 7 (33.33) | 2 (9.52) | p = 0.358 χ2 = 6.616 |
| Active | 21 (25) | 3 (14.28) | 5 (23.80) | 6 (28.57) | 7 (33.33) | ||
| Latent | 46 (54.76) | 13 (61.90) | 13 (61.90) | 8 (38.09) | 12 (57.14) |
| Muscles | Presence of MTrPs | Total (n = 84) | NDNC (n = 21) | NDWC (n = 21) | WDNC (n = 21) | WDWC (n = 21) | p-Value * χ2 |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Ischiocavernosus | Does not have | 39 (46.42) | 14 (66.66) | 14 (66.66) | 7 (3333) | 4 (19.04) | p < 0.01 * χ2 = 16.969 |
| Active | 4 (4.76) | 1 (4.76) | 1 (4.76) | 0 | 2 (9.52) | ||
| Latent | 41 (48.80) | 6 (28.57) | 6 (28.57) | 14 (66.66) | 15 (71.42) | ||
| Bulbospongiosus | Does not have | 56 (66.66) | 17 (80.95) | 17 (80.95) | 13 (61.90) | 9 (42.85) | p = 0.052 χ2 = 12.476 |
| Active | 1 (1.19) | 0 | 0 | 1 (4.76) | 0 | ||
| Latent | 27 (32.14) | 4 (19.04) | 4 (19.04) | 7 (33.33) | 12 (57.14) | ||
| Transverse perineal | Does not have | 52 (61.90) | 13 (61.90) | 16 (76.19) | 11 (52.38) | 12 (57.14) | p = 0.600 χ2 = 4.573 |
| Active | 5 (5.95) | 2 (9.52) | 0 | 1 (4.76) | 2 (9.52) | ||
| Latent | 27 (32.14) | 6 (28.57) | 5 (23.80) | 9 (42.85) | 7 (33.33) | ||
| Puborectalis | Does not have | 18 (21.42) | 4 (19.04) | 10 (47.61) | 1 (4.76) | 3 (14.28) | p = 0.030 χ2 = 14.000 |
| Active | 22 (26.19) | 6 (28.57) | 2 (9.52) | 8 (38.09) | 6 (28.57) | ||
| Latent | 44 (52.38) | 11 (52.38) | 9 (42.85) | 12 (57.14) | 12 (57.14) | ||
| Pubococcygeus | Does not have | 21 (25) | 6 (28.57) | 8 (38.09) | 6 (28.57) | 1 (4.76) | p = 0.116 χ2 = 10.210 |
| Active | 35 (41.66) | 6 (28.57) | 6 (28.57) | 10 (47.61) | 13 (61.90) | ||
| Latent | 28 (33.33) | 9 (42.85) | 7 (33.33) | 5 (23.80) | 7 (33.33) | ||
| Iliococcygeus | Does not have | 15 (17.85) | 6 (28.57) | 8 (38.09) | 1 (4.76) | 0 | p < 0.001 * χ2 = 25.286 |
| Active | 51 (60.71) | 7 (33.33) | 8 (38.09) | 18 (85.71) | 18 (85.71) | ||
| Latent | 18 (21.42) | 8 (38.09) | 5 (23.80) | 2 (9.52) | 3 (14.28) | ||
| Obturator internus | Does not have | 6 (7.14) | 2 (9.52) | 4 (19.04) | 0 | 0 | p = 0.049 χ2 = 12.659 |
| Active | 28 (33.33) | 4 (19.04) | 5 (23.80) | 8 (38.09) | 11 (52.38) | ||
| Latent | 50 (59.52) | 15 (71.42) | 12 (57.14) | 13 (61.90) | 10 (11.90) | ||
| Coccygeus | Does not have | 39 (46.42) | 12 (57.14) | 10 (47.61) | 12 (57.14) | 5 (23.80) | p = 0.55 χ2 = 12.314 |
| Active | 7 (8.33) | 0 | 1 (4.76) | 1 (4.76) | 5 (23.80) | ||
| Latent | 38 (45.23) | 9 (42.85) | 10 (47.61) | 8 (38.09) | 11 (52.38) | ||
| Anal sphincter | Does not have | 69 (82.14) | 17 (80.95) | 21 (100) | 17 (80.95) | 14 (66.66) | p < 0.01 * χ2 = 18.435 |
| Active | 5 (5.95) | 3 (14.28) | 0 | 2 (9.52) | 0 | ||
| Latent | 10 (11.90) | 1 (4.76) | 0 | 2 (9.52) | 7 (33.33) |
| Self-Reported Pain Site | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Muscles | Flank n (%) | Iliac Fossa n (%) | Hypogastrium n (%) | Mesogastrium n (%) | Epigastrium n (%) | Anterior Part Lower Limb n (%) | Posterior Part Lower Limb n (%) | Pubis n (%) | Groin n (%) | Gluteus n (%) | Lumbar n (%) | Coccyx n (%) | Sacrum n (%) | Internal Part Lower Limb n (%) | Vulva n (%) | Vagina n (%) | Urethra n (%) | Anus n (%) | Rectum n (%) |
| Rectus Abdominis | 54 (64.29) | 34 (40.48) | 68 (80.95) | 61 (72.62) | 24 (28.57) | 1 (1.19) | 0 (0) | 10 (11.90) | 7 (8.33) | 1 (1.19) | 4 (4.76) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| External Oblique | 56 (66.67) | 60 (71.43) | 7 (8.33) | 4 (4.76) | 0 (0) | 4 (4.76) | 1 (1.19) | 3 (3.57) | 4 (4.76) | 0 (0) | 4 (4.76) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Internal Oblique | 1 (1.19) | 12 (14.29) | 24 (28.57) | 0 (0) | 0 (0) | 10 (11.90) | 0 (0) | 10 (11.90) | 14 (16.67) | 0 (0) | 0 (0) | 1 (1.19) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Adductor Magnus | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 7 (8.33) | 3 (3.57) | 2 (2.38) | 2 (2.38) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 75 (89.29) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Gluteus Maximus | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 5 (5.95) | 1 (1.19) | 0 (0) | 0 (0) | 64 (76.19) | 12 (14.29) | 3 (3.57) | 4 (4.76) | 9 (10.71) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Gluteus Medius | 1 (1.19) | 1 (1.19) | 1 (1.19) | 0 (0) | 0 (0) | 4 (4.76) | 9 (10.71) | 1 (1.19) | 3 (3.57) | 74 (88.10) | 5 (5.95) | 3 (3.57) | 4 (4.76) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Gluteus Minimus | 0 (0) | 1 (1.19) | 1 (1.19) | 0 (0) | 0 (0) | 9 (10.71) | 15 (17.86) | 1 (1.19) | 2 (2.38) | 70 (83.33) | 5 (5.95) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Quadratus Lumborum | 3 (3.57) | 3 (3.57) | 5 (5.95) | 1 (1.19) | 1 (1.19) | 1 (1.19) | 2 (2.38) | 2 (2.38) | 2 (2.38) | 20 (23.81) | 75 (89.29) | 1 (1.19) | 8 (9.52) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Piriformis | 1 (1.19) | 7 (8.33) | 11 (13.10) | 1 (1.19) | 0 (0) | 6 (7.14) | 10 (11.90) | 10 (11.90) | 17 (20.24) | 48 (57.14) | 6 (7.14) | 11 (13.10) | 9 (10.71) | 2 (2.38) | 16 (19.05) | 3 (3.57) | 2 (2.38) | 8 (9.52) | 0 (0) |
| Self-Reported Pain Site | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Muscles n (%) | Flank n (%) | Iliac Fossa n (%) | Hypogastrium n (%) | Mesogastrium n (%) | Epigastrium n (%) | Anterior Part Lower Limb n (%) | Pubis n (%) | Groin n (%) | Vulva n (%) | Sacrum n (%) | Lumbar n (%) | Internal Part Lower Limb n (%) | Coccyx n (%) | Posterior Part Lower Limb n (%) | Gluteus n (%) | Vagina n (%) | Urethra n (%) | Anus n (%) | Rectum n (%) |
| Rectus Abdominis | 15 (17.86) | 25 (29.76) | 56 (66.67) | 50 (59.52) | 14 (16.67) | 1 (1.19) | 1 (1.19) | 4 (4.76) | 1 (1.19) | 1 (1.19) | 5 (5.95) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| External Oblique | 43 (51.19) | 56 (66.67) | 5 (5.95) | 2 (2.38) | 2 (2.38) | 5 (5.95) | 0 (0) | 1 (1.19) | 0 (0) | 1 (1.19) | 2 (2.38) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Internal Oblique | 0 (0) | 10 (11.90) | 11 (13.10) | 0 (0) | 0 (0) | 4 (4.76) | 6 (7.14) | 4 (4.76) | 0 (0) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Adductor Magnus | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 8 (9.52) | 0 (0) | 2 (2.38) | 0 (0) | 0 (0) | 0 (0) | 65 (77.38) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Gluteus Maximus | 2 (2.38) | 2 (2.38) | 1 (1.19) | 0 (0) | 0 (0) | 9 (10.71) | 1 (1.19) | 1 (1.19) | 0 (0) | 3 (3.57) | 17 (20.24) | 1 (1.19) | 1 (1.19) | 3 (3.57) | 64 (76.19) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Gluteus Medius | 1 (1.19) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 6 (7.14) | 1 (1.19) | 1 (1.19) | 0 (0) | 1 (1.19) | 6 (7.14) | 0 (0) | 0 (0) | 7 (8.33) | 61 (71.62) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Gluteus Minimus | 0 (0) | 1 (1.19) | 2 (2.38) | 0 (0) | 0 (0) | 8 (9.52) | 0 (0) | 0 (0) | 0 (0) | 2 (2.38) | 9 (10.71) | 1 (1.19) | 1 (1.19) | 7 (8.33) | 62 (73.81) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Quadratus Lumborum | 1 (1.19) | 4 (4.76) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.19) | 2 (2.38) | 0 (0) | 4 (4.76) | 72 (85.71) | 0 (0) | 0 (0) | 3 (3.57) | 18 (21.43) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Piriformis | 1 (1.19) | 8 (9.52) | 7 (8.33) | 1 (1.19) | 0 (0) | 3 (3.57) | 9 (10.71) | 11 (13.10) | 17 (20.24) | 2 (2.38) | 4 (4.76) | 2 (2.38) | 4 (4.76) | 6 (7.14) | 47 (55.95) | 4 (4.76) | 0 (0) | 10 (11.90) | 3 (3.57) |
| Self-Reported Pain Site | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Muscles n (%) | Flank n (%) | Iliac Fossa n (%) | Hypogastrium n (%) | Mesogastrium n (%) | Epigastrium n (%) | Anterior Part Lower Limb n (%) | Posterior Part Lower Limb n (%) | Pubis n (%) | Groin n (%) | Gluteus n (%) | Lumbar n (%) | Coccyx n (%) | Sacrum n (%) | Internal Part Lower Limb n (%) | Vulva n (%) | Vagina n (%) | Urethra n (%) | Anus n (%) | Rectum n (%) |
| Ischiocavernosus | 0 (0) | 0 (0) | 2 (2.38) | 0 (0) | 0 (0) | 1 (1.19) | 1 (1.19) | 1 (1.19) | 14 (16.67) | 3 (3.57) | 1 (1.19) | 2 (2.38) | 0 (0) | 4 (4.76) | 55 (65.48) | 3 (3.57) | 4 (4.76) | 0 (0) | 0 (0) |
| Bulbospongiosus | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 41 (48.81) | 11 (13.10) | 6 (7.14) | 0 (0) | 0 (0) |
| Transverse Perineal | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.19) | 1 (1.19) | 0 (0) | 1 (1.19) | 21 (25.00) | 0 (0) | 2 (2.38) | 0 (0) | 2 (2.38) | 29 (34.52) | 1 (1.19) | 0 (0) | 9 (10.71) | 0 (0) |
| Puborectalis | 0 (0) | 1 (1.19) | 5 (5.95) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 9 (10.71) | 11 (13.10) | 13 (15.48) | 0 (0) | 6 (7.14) | 2 (2.38) | 5 (5.95) | 41 (48.81) | 28 (33.33) | 7 (8.33) | 19 (22.62) | 6 (7.14) |
| Pubococcygeus | 0 (0) | 13 (15.48) | 23 (27.38) | 0 (0) | 0 (0) | 5 (5.95) | 9 (10.71) | 14 (16.67) | 18 (21.43) | 14 (16.67) | 4 (4.76) | 5 (5.95) | 2 (2.38) | 6 (7.14) | 31 (36.90) | 14 (16.67) | 4 (4.76) | 6 (7.14) | 0 (0) |
| Iliococcygeus | 2 (2.38) | 18 (21.43) | 46 (54.76) | 2 (2.38) | 0 (0) | 4 (4.76) | 4 (4.76) | 37 (44.05) | 23 (27.38) | 10 (11.90) | 3 (3.57) | 4 (4.76) | 2 (2.38) | 3 (3.57) | 37 (44.05) | 12 (14.29) | 9 (10.71) | 5 (5.95) | 1 (1.19) |
| Coccygeus | 0 (0) | 2 (2.38) | 3 (3.57) | 0 (0) | 0 (0) | 0 (0) | 2 (2.38) | 1 (1.19) | 3 (3.57) | 20 (23.81) | 2 (2.38) | 21 (25.00) | 5 (5.95) | 1 (1.19) | 13 (15.48) | 2 (2.38) | 0 (0) | 20 (23.81) | 6 (7.14) |
| External Anal Sphincter | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 4 (4.76) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 7 (8.33) | 0 (0) | 0 (0) | 26 (30.95) | 0 (0) |
| Obturator Internus | 0 (0) | 7 (8.33) | 17 (20.24) | 0 (0) | 0 (0) | 9 (10.71) | 33 (39.29) | 19 (22.62) | 19 (22.62) | 42 (50.00) | 9 (10.71) | 8 (9.52) | 8 (9.52) | 13 (15.48) | 35 (41.67) | 10 (11.90) | 6 (7.14) | 25 (29.76) | 7 (8.33) |
| Self-Reported Pain Site | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Muscles n (%) | Flank n (%) | Iliac Fossa n (%) | Hypogastrium n (%) | Mesogastrium n (%) | Epigastrium n (%) | Anterior Part Lower Limb n (%) | Pubis n (%) | Groin n (%) | Vulva n (%) | Sacrum n (%) | Lumbar n (%) | Internal Part Lower Limb n (%) | Coccyx n (%) | Posterior Part Lower Limb n (%) | Gluteus n (%) | Vagina n (%) | Urethra n (%) | Anus n (%) | Rectum n (%) |
| Ischiocavernosus | 0 (0) | 0 (0) | 2 (2.38) | 0 (0) | 0 (0) | 2 (2.38) | 0 (0) | 11 (13.10) | 48 (57.14) | 0 (0) | 0 (0) | 2 (2.38) | 0 (0) | 0 (0) | 3 (3.57) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) |
| Bulbospongiosus | 0 (0) | 1 (1.19) | 1 (1.19) | 0 (0) | 0 (0) | 2 (2.38) | 0 (0) | 2 (2.38) | 24 (28.57) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 8 (9.52) | 3 (3.57) | 0 (0) | 0 (0) |
| Transverse Perineal | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 2 (2.38) | 18 (21.43) | 1 (1.19) | 1 (1.19) | 0 (0) | 0 (0) | 0 (0) | 16 (19.04) | 2 (2.38) | 1 (1.19) | 7 (8.33) | 0 (0) |
| Puborectalis | 0 (0) | 0 (0) | 5 (5.95) | 1 (1.19) | 0 (0) | 2 (2.38) | 1 (1.19) | 6 (7.14) | 50 (59.52) | 2 (2.38) | 2 (2.38) | 0 (0) | 2 (2.38) | 1 (1.19) | 11 (13.10) | 22 (26.19) | 4 (4.76) | 20 (23.81) | 4 (4.76) |
| Pubococcygeus | 1 (1.19) | 2 (2.38) | 22 (26.19) | 0 (0) | 0 (0) | 4 (4.76) | 18 (21.43) | 16 (19.05) | 23 (27.38) | 1 (1.19) | 2 (2.38) | 6 (7.14) | 3 (3.57) | 5 (5.95) | 10 (11.90) | 11 (13.10) | 6 (7.14) | 6 (7.14) | 0 (0) |
| Iliococcygeus | 0 (0) | 15 (17.86) | 42 (50.00) | 1 (1.19) | 0 (0) | 6 (7.14) | 22 (26.19) | 15 (17.86) | 30 (35.71) | 2 (2.38) | 5 (5.95) | 4 (4.76) | 1 (1.19) | 3 (3.57) | 5 (5.95) | 9 (10.71) | 5 (5.95) | 2 (2.38) | 0 (0) |
| Coccygeus | 1 (1.19) | 2 (2.38) | 3 (3.57) | 0 (0) | 0 (0) | 3 (3.57) | 3 (3.57) | 3 (3.57) | 9 (10.71) | 4 (4.76) | 0 (0) | 1 (1.19) | 12 (14.29) | 0 (0) | 13 (15.48) | 1 (1.19) | 0 (0) | 19 (22.62) | 5 (5.95) |
| External Anal Sphincter | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 3 (3.57) | 2 (2.38) | 0 (0) | 0 (0) | 1 (1.19) | 0 (0) | 4 (4.76) | 0 (0) | 0 (0) | 18 (21.43) | 0 (0) |
| Obturator Internus | 2 (2.38) | 10 (11.90) | 17 (20.24) | 1 (1.19) | 0 (0) | 6 (7.14) | 11 (13.10) | 14 (16.67) | 33 (39.29) | 3 (3.57) | 4 (4.76) | 8 (9.52) | 4 (4.76) | 23 (27.38) | 38 (45.24) | 12 (14.29) | 4 (4.76) | 23 (27.38) | 5 (5.95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano-Imedio, A.; Calvo-Lobo, C.; Casañas-Martin, C.; Garrido-Marin, A.; Pecos-Martin, D. Myofascial Pain Syndrome in Women with Primary Dysmenorrhea: A Case-Control Study. Diagnostics 2022, 12, 2723. https://doi.org/10.3390/diagnostics12112723
Serrano-Imedio A, Calvo-Lobo C, Casañas-Martin C, Garrido-Marin A, Pecos-Martin D. Myofascial Pain Syndrome in Women with Primary Dysmenorrhea: A Case-Control Study. Diagnostics. 2022; 12(11):2723. https://doi.org/10.3390/diagnostics12112723
Chicago/Turabian StyleSerrano-Imedio, Ana, Cesar Calvo-Lobo, Coraima Casañas-Martin, Alejandro Garrido-Marin, and Daniel Pecos-Martin. 2022. "Myofascial Pain Syndrome in Women with Primary Dysmenorrhea: A Case-Control Study" Diagnostics 12, no. 11: 2723. https://doi.org/10.3390/diagnostics12112723
APA StyleSerrano-Imedio, A., Calvo-Lobo, C., Casañas-Martin, C., Garrido-Marin, A., & Pecos-Martin, D. (2022). Myofascial Pain Syndrome in Women with Primary Dysmenorrhea: A Case-Control Study. Diagnostics, 12(11), 2723. https://doi.org/10.3390/diagnostics12112723