
GestroNet: A Framework of Saliency Estimation and Optimal Deep Learning Features Based Gastrointestinal Diseases Detection and Classification

 ,
,  , ,
, ,
Abstract
1. Introduction
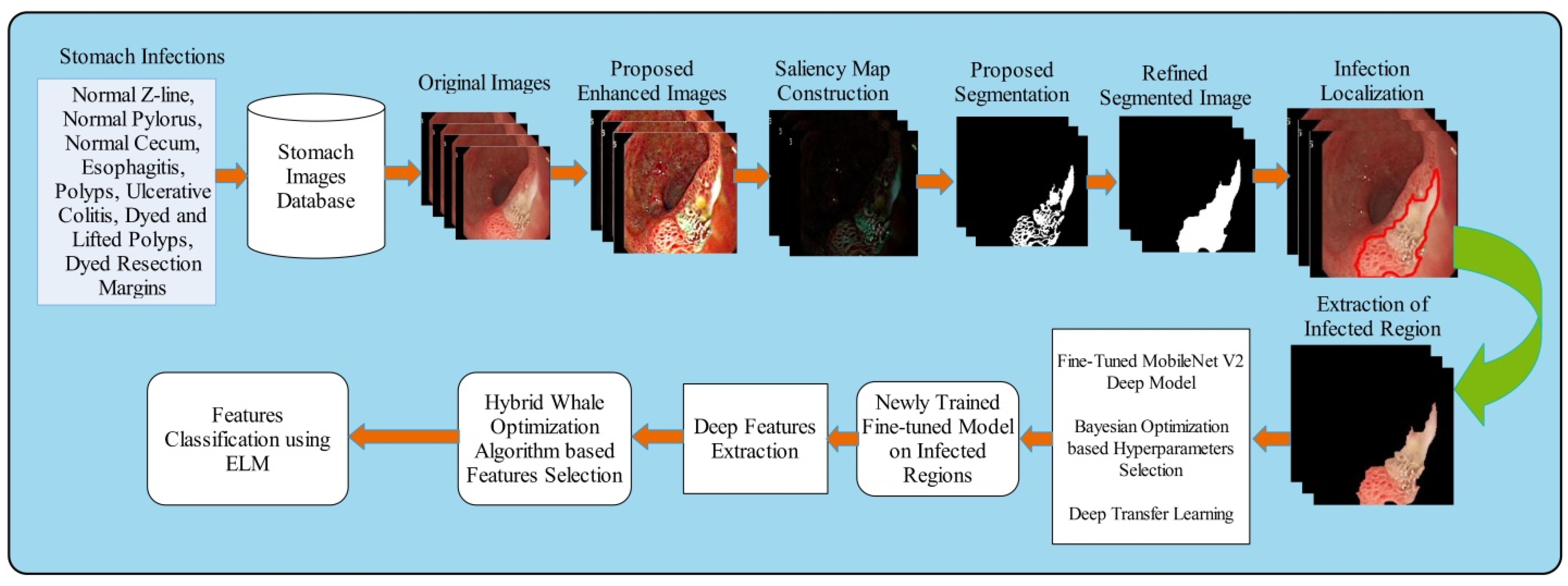
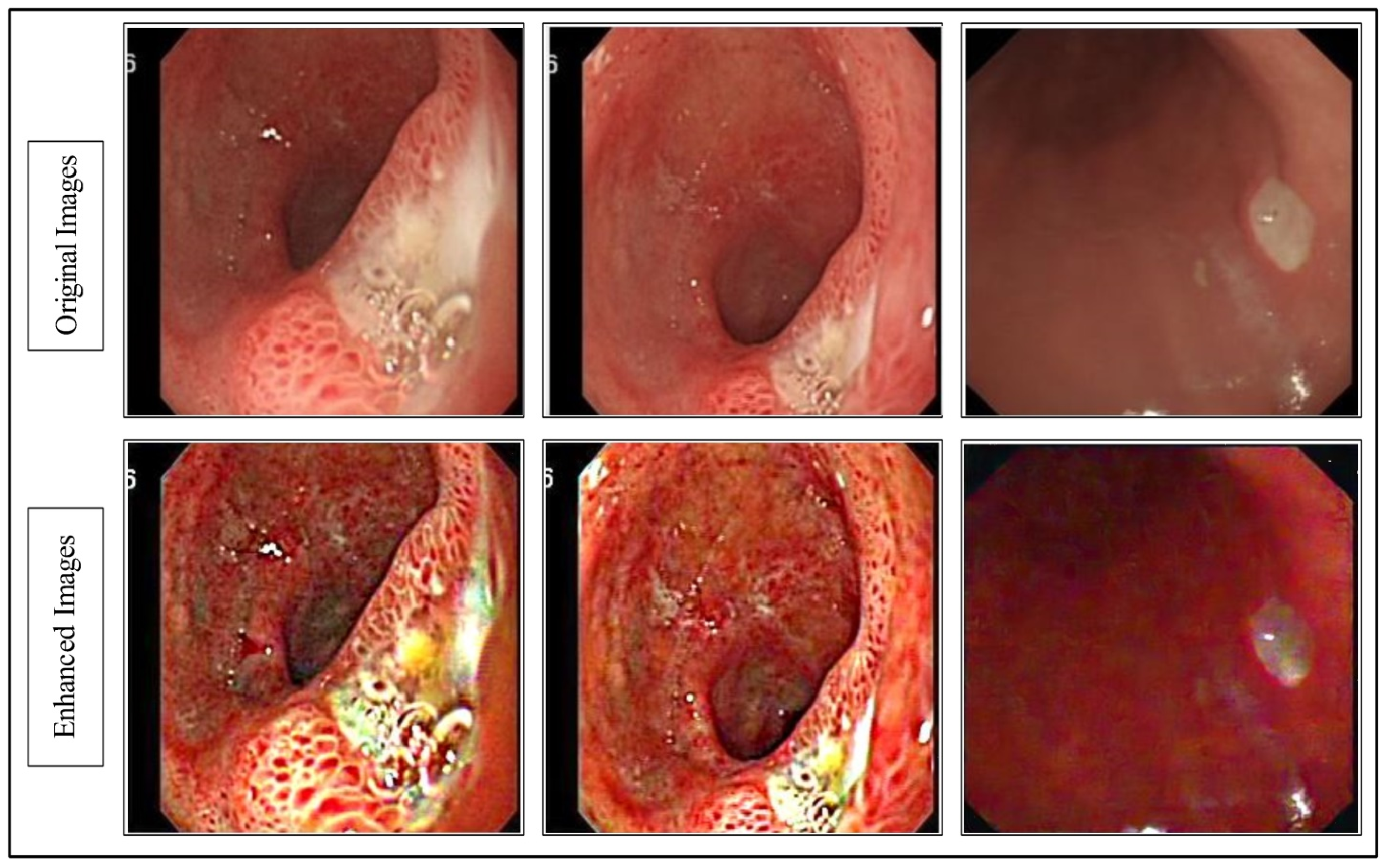
- We proposed a hybrid sequential fusion approach for contrast enhancement. The purpose of this approach is improving the contrast of infected region in the image that further helps in better segmentation.
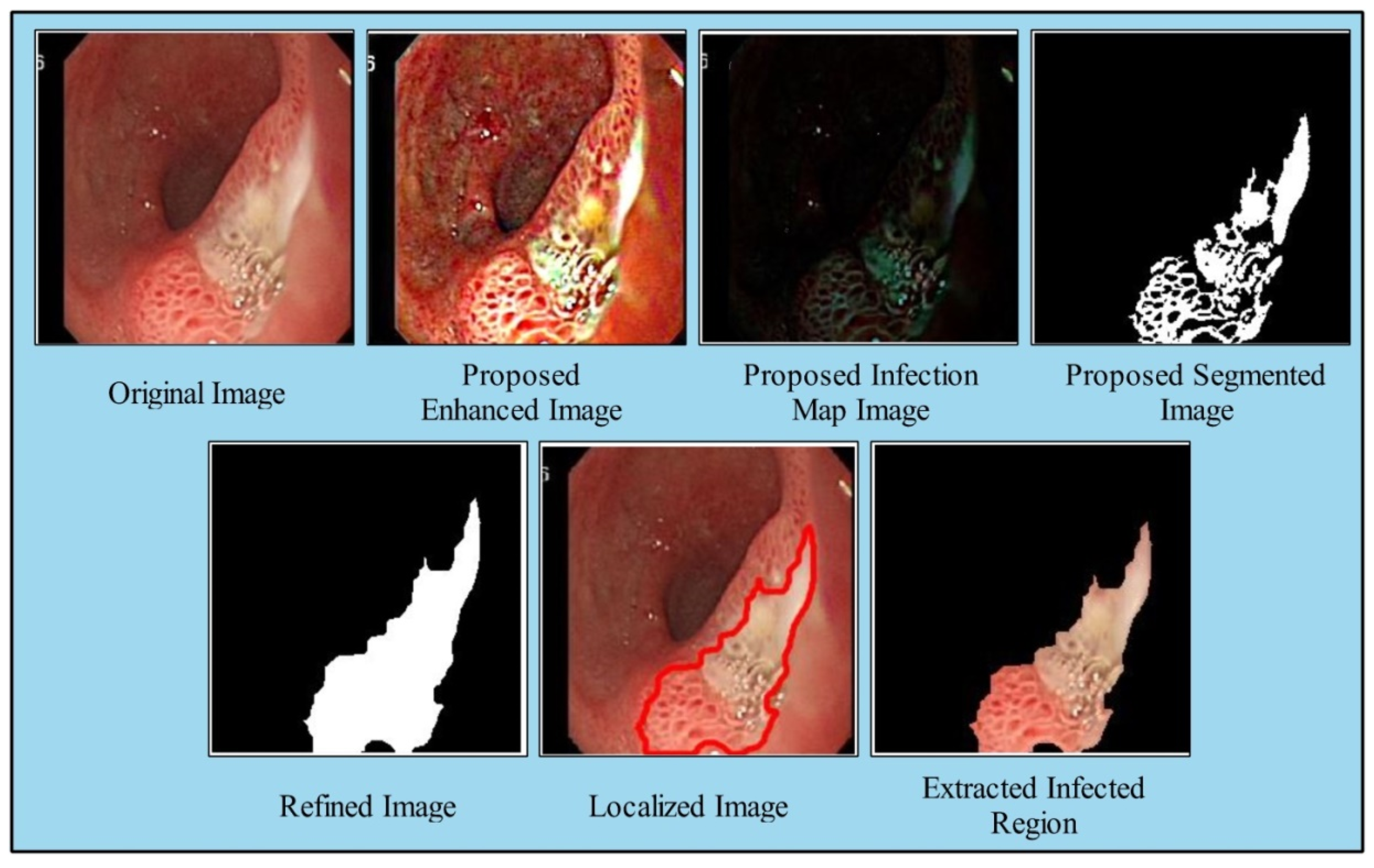
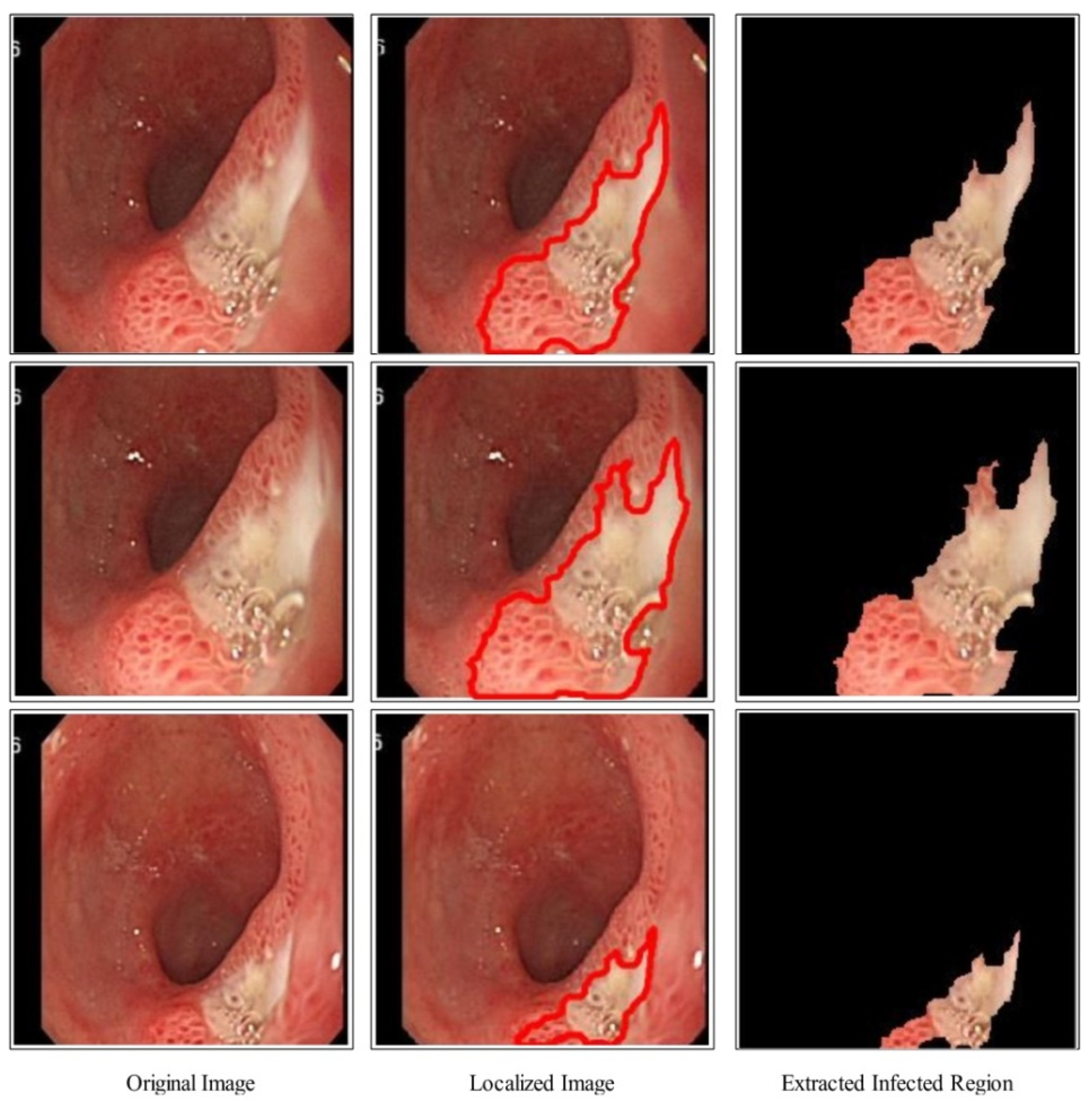
- A deep saliency-based infected region segmentation and localization technique is proposed.
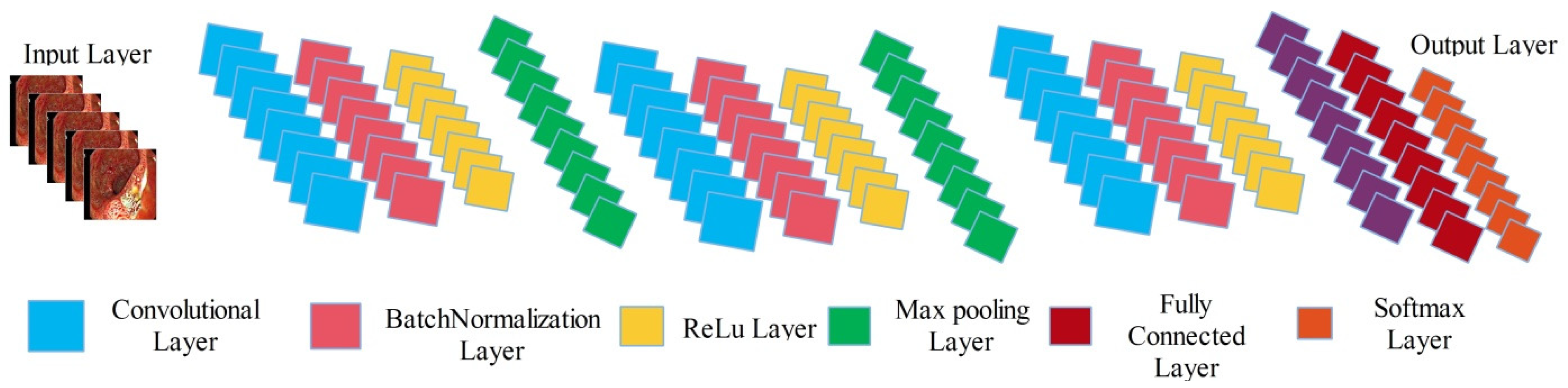
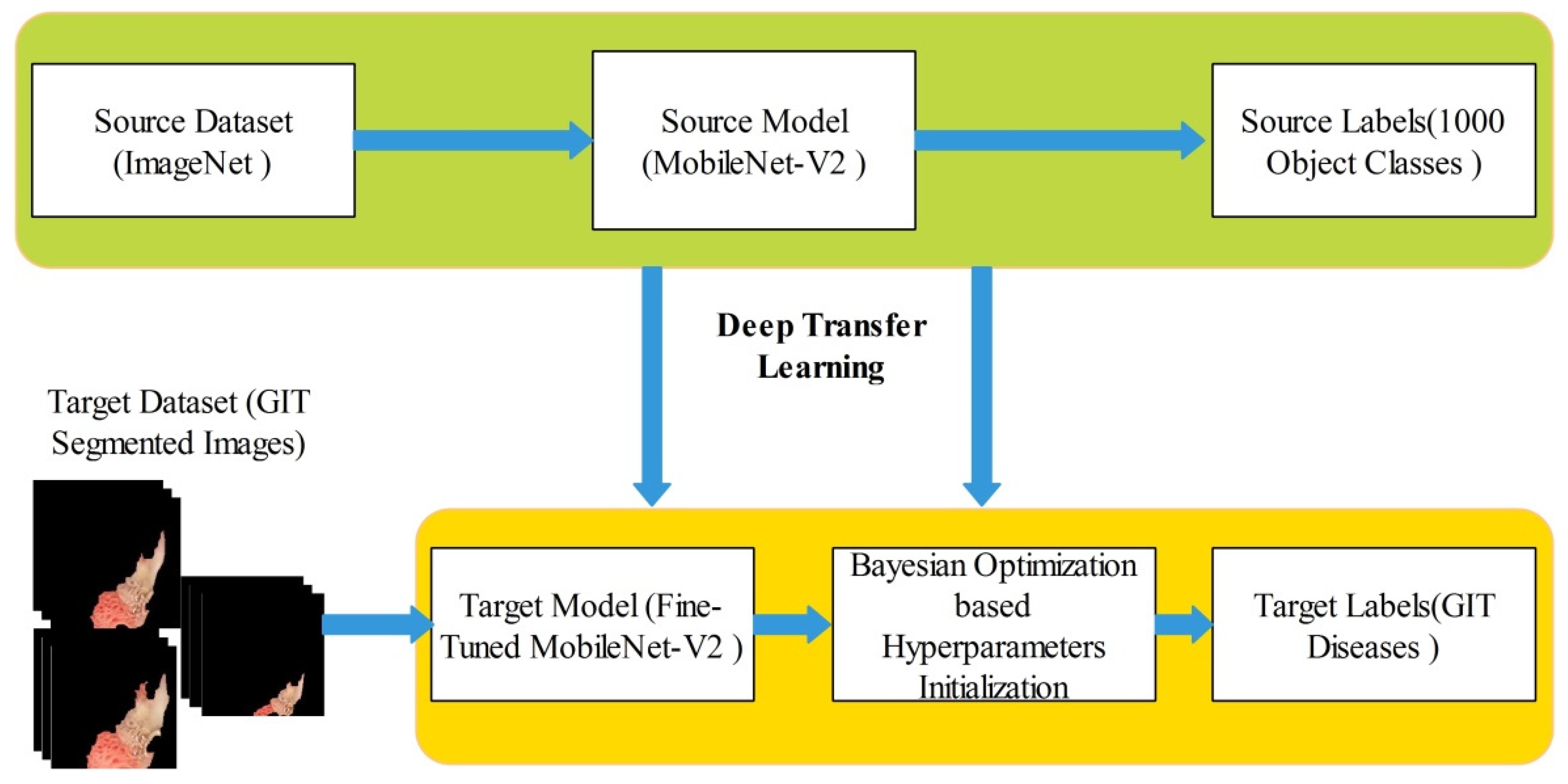
- A fine-tuned MobileNet-V2 model is trained on localized images and hyperparameters are optimized using Bayesian Optimization. Usually, the hyperparameters were initialized in a static way.
- A hybrid whale optimization algorithm is proposed for the selection of best features.
2. Materials and Methods
2.1. Proposed Contrast Enhancement
2.2. Proposed Saliency Map Based Segmentation
2.3. Deep Learning Features
2.4. Bayesian Optimization
2.5. Proposed Feature Selection Algorithm
3. Results
3.1. CUI WCE Dataset Results
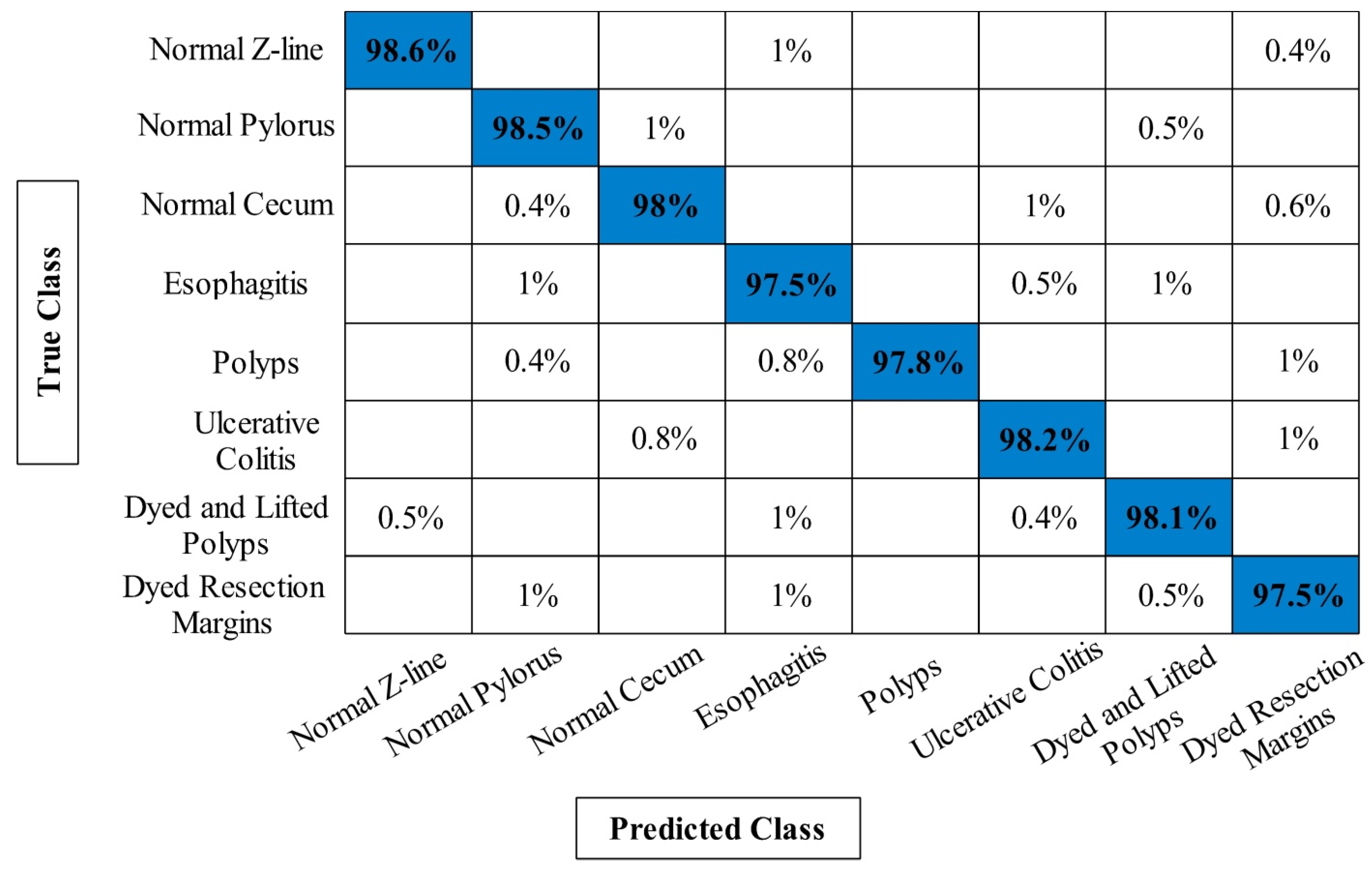
3.2. KVASIR V1 Dataset Results
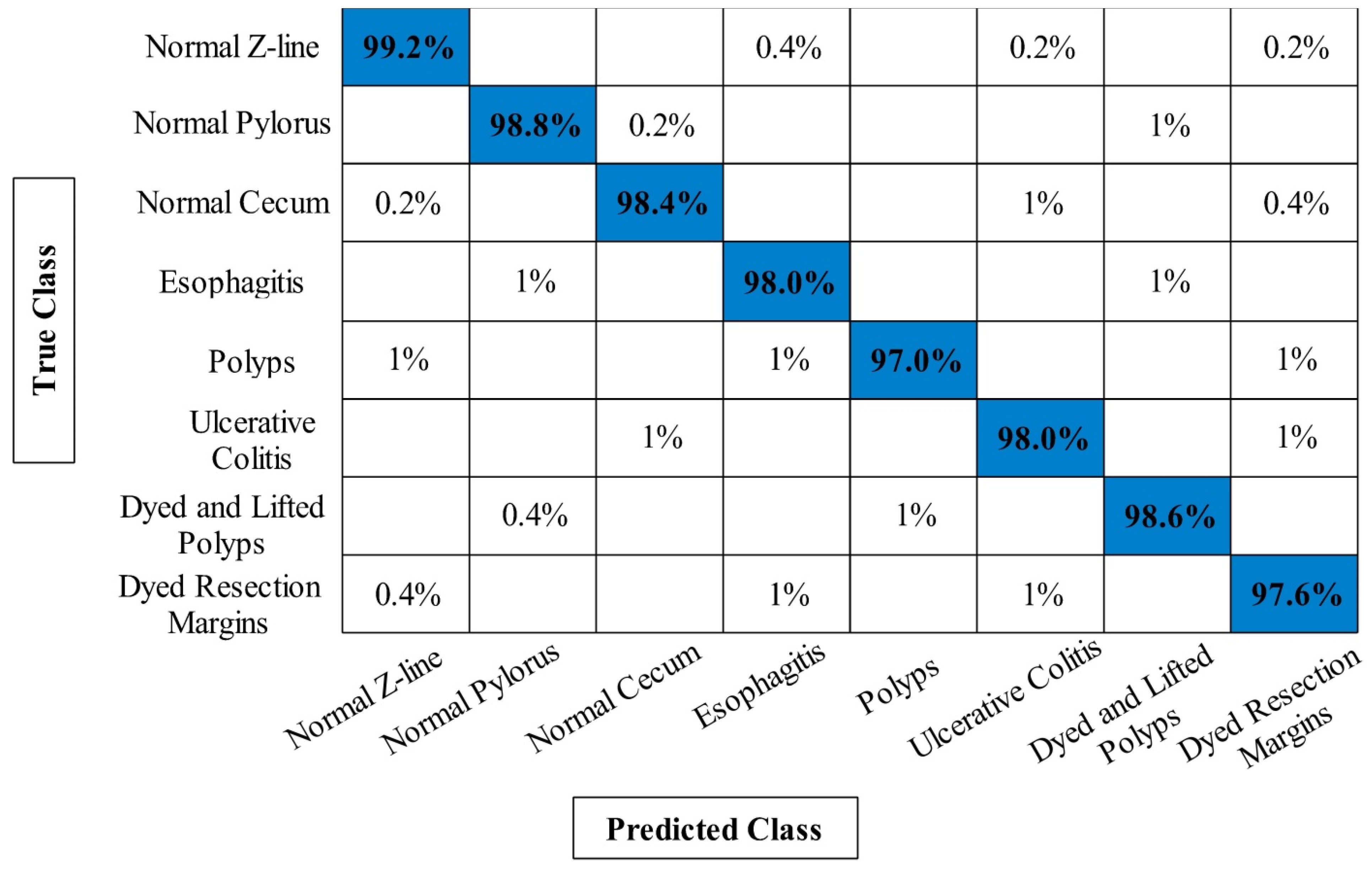
3.3. KVASIR V2 Classification Results
3.4. Discussion and Comparison
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jackson, K.J.; Emmons, K.R.; Nickitas, D.M. Role of Primary Care in Detection of Subsequent Primary Cancers. J. Nurse Pract. 2022, 18, 478–482. [Google Scholar] [CrossRef]
- Bhardwaj, P.; Bhandari, G.; Kumar, Y.; Gupta, S. An Investigational Approach for the Prediction of Gastric Cancer Using Artificial Intelligence Techniques: A Systematic Review. Arch. Comput. Methods Eng. 2022, 29, 4379–4400. [Google Scholar] [CrossRef]
- Ayyaz, M.S.; Lali, M.I.U.; Hussain, M.; Rauf, H.T.; Alouffi, B.; Alyami, H.; Wasti, S. Hybrid deep learning model for endoscopic lesion detection and classification using endoscopy videos. Diagnostics 2021, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Polaka, I.; Bhandari, M.P.; Mezmale, L.; Anarkulova, L.; Veliks, V.; Sivins, A.; Lescinska, A.M.; Tolmanis, I.; Vilkoite, I.; Ivanovs, I. Modular Point-of-Care Breath Analyzer and Shape Taxonomy-Based Machine Learning for Gastric Cancer Detection. Diagnostics 2022, 12, 491. [Google Scholar] [CrossRef] [PubMed]
- Nautiyal, H.; Kazmi, I.; Kaleem, M.; Afzal, M.; Ahmad, M.M.; Zafar, A.; Kaur, R. Mechanism of action of drugs used in gastrointestinal diseases. In How Synthetic Drugs Work; Elsevier: Amsterdam, The Netherlands, 2023; pp. 391–419. [Google Scholar]
- Sinicrope, F.A. Increasing Incidence of Early-Onset Colorectal Cancer. N. Engl. J. Med. 2022, 386, 1547–1558. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, B.; Wang, Y.; Yin, X.; Jiang, Y.; Zhu, X. Identification of gastric cancer with convolutional neural networks: A systematic review. Multimed. Tools Appl. 2022, 81, 11717–11736. [Google Scholar] [CrossRef]
- Deb, A.; Perisetti, A.; Goyal, H.; Aloysius, M.M.; Sachdeva, S.; Dahiya, D.; Sharma, N.; Thosani, N. Gastrointestinal Endoscopy-Associated Infections: Update on an Emerging Issue. Dig. Dis. Sci. 2022, 67, 1718–1732. [Google Scholar] [CrossRef]
- Gholami, E.; Tabbakh, S.R.K. Increasing the accuracy in the diagnosis of stomach cancer based on color and lint features of tongue. Biomed. Signal Process. Control 2021, 69, 102782. [Google Scholar] [CrossRef]
- Alam, M.W.; Vedaei, S.S.; Wahid, K.A. A fluorescence-based wireless capsule endoscopy system for detecting colorectal cancer. Cancers 2020, 12, 890. [Google Scholar] [CrossRef]
- Kim, H.J.; Gong, E.J.; Bang, C.S.; Lee, J.J.; Suk, K.T.; Baik, G.H. Computer-Aided Diagnosis of Gastrointestinal Protruded Lesions Using Wireless Capsule Endoscopy: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis. J. Pers. Med. 2022, 12, 644. [Google Scholar] [CrossRef]
- Amin, M.S.; Shah, J.H.; Yasmin, M.; Ansari, G.J.; Khan, M.A.; Tariq, U.; Kim, Y.J.; Chang, B. A Two Stream Fusion Assisted Deep Learning Framework for Stomach Diseases Classification. CMC-Comput. Mater. Contin. 2022, 73, 4423–4439. [Google Scholar] [CrossRef]
- Iizuka, O.; Kanavati, F.; Kato, K.; Rambeau, M.; Arihiro, K.; Tsuneki, M. Deep learning models for histopathological classification of gastric and colonic epithelial tumours. Sci. Rep. 2020, 10, 1–11. [Google Scholar]
- Son, G.; Eo, T.; An, J.; Oh, D.J.; Shin, Y.; Rha, H.; Kim, Y.J.; Lim, Y.J.; Hwang, D. Small Bowel Detection for Wireless Capsule Endoscopy Using Convolutional Neural Networks with Temporal Filtering. Diagnostics 2022, 12, 1858. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, S.; Prasad, K.; Robels-Kelly, A.; Lu, X. AI-based carcinoma detection and classification using histopathological images: A systematic review. Comput. Biol. Med. 2022, 142, 105209. [Google Scholar] [CrossRef] [PubMed]
- Javed, K.; Khan, S.A.; Saba, T.; Habib, U.; Khan, J.A.; Abbasi, A.A. Human action recognition using fusion of multiview and deep features: An application to video surveillance. Multimed. Tools Appl. 2020, 3, 1–27. [Google Scholar]
- Lahoura, V.; Singh, H.; Aggarwal, A.; Sharma, B.; Mohammed, M.A.; Damaševičius, R.; Kadry, S.; Cengiz, K. Cloud computing-based framework for breast cancer diagnosis using extreme learning machine. Diagnostics 2021, 11, 241. [Google Scholar] [CrossRef]
- Naz, J.; Alhaisoni, M.; Song, O.-Y.; Tariq, U.; Kadry, S. Segmentation and classification of stomach abnormalities using deep learning. CMC-Comput. Mater. Contin. 2021, 69, 607–625. [Google Scholar] [CrossRef]
- Majid, A.; Hussain, N.; Alhaisoni, M.; Zhang, Y.-D.; Kadry, S.; Nam, Y. Multiclass stomach diseases classification using deep learning features optimization. Comput. Mater. Contin. 2021, 69, 1–15. [Google Scholar]
- Sharif, M.; Akram, T.; Yasmin, M.; Nayak, R.S. Stomach deformities recognition using rank-based deep features selection. J. Med. Syst. 2019, 43, 329. [Google Scholar]
- Sarfraz, M.S.; Alhaisoni, M.; Albesher, A.A.; Wang, S.; Ashraf, I. StomachNet: Optimal deep learning features fusion for stomach abnormalities classification. IEEE Access 2020, 8, 197969–197981. [Google Scholar]
- Ba, W.; Wang, S.; Shang, M.; Zhang, Z.; Wu, H.; Yu, C.; Xing, R.; Wang, W.; Wang, L.; Liu, C. Assessment of deep learning assistance for the pathological diagnosis of gastric cancer. Mod. Pathol. 2022, 35, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Majid, A.; Yasmin, M.; Rehman, A.; Yousafzai, A.; Tariq, U. Classification of stomach infections: A paradigm of convolutional neural network along with classical features fusion and selection. Microsc. Res. Technol. 2020, 83, 562–576. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.; Sharif, M.; Javed, K.; Akram, T. Classification of gastrointestinal diseases of stomach from WCE using improved saliency-based method and discriminant features selection. Multimed. Tools Appl. 2019, 78, 27743–27770. [Google Scholar]
- Hmoud Al-Adhaileh, M.; Mohammed Senan, E.; Alsaade, W.; Aldhyani, T.H.; Alsharif, N.; Abdullah Alqarni, A.; Uddin, M.I.; Alzahrani, M.Y.; Alzain, E.D.; Jadhav, M.E. Deep Learning Algorithms for Detection and Classification of Gastrointestinal Diseases. Complexity 2021, 2021, 6170416. [Google Scholar] [CrossRef]
- Park, D.; Park, H.; Han, D.K.; Ko, H. Single image dehazing with image entropy and information fidelity. In Proceedings of the 2014 IEEE International Conference on Image Processing (ICIP), Paris, France, 27–30 October 2014; pp. 4037–4041. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.-C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE conference on computer vision and pattern recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 4510–4520. [Google Scholar]
- Wu, J.; Chen, X.-Y.; Zhang, H.; Xiong, L.-D.; Lei, H.; Deng, S.-H. Hyperparameter optimization for machine learning models based on Bayesian optimization. J. Electron. Sci. Technol. 2019, 17, 26–40. [Google Scholar]
- Mirjalili, S.; Lewis, A. The whale optimization algorithm. Adv. Eng. Softw. 2016, 95, 51–67. [Google Scholar] [CrossRef]
- Heidari, A.A.; Mirjalili, S.; Faris, H.; Aljarah, I.; Mafarja, M.; Chen, H. Harris hawks optimization: Algorithm and applications. Future Gener. Comput. Syst. 2019, 97, 849–872. [Google Scholar] [CrossRef]
- Escobar, J.; Sanchez, K.; Hinojosa, C.; Arguello, H.; Castillo, S. Accurate deep learning-based gastrointestinal disease classification via transfer learning strategy. In Proceedings of the 2021 XXIII Symposium on Image, Signal Processing and Artificial Vision (STSIVA), Popayan, Colombia, 15–17 September 2021; pp. 1–5. [Google Scholar]
- Wang, W.; Yang, X.; Li, X.; Tang, J. Convolutional-capsule network for gastrointestinal endoscopy image classification. Int. J. Intell. Syst. 2022, 37, 5796–5815. [Google Scholar] [CrossRef]
- Liaqat, A.; Shah, J.H.; Sharif, M.; Yasmin, M.; Fernandes, S.L. Automated ulcer and bleeding classification from WCE images using multiple features fusion and selection. J. Mech. Med. Biol. 2018, 18, 1850038. [Google Scholar] [CrossRef]
- Calvo, B.; Santafé Rodrigo, G. scmamp: Statistical comparison of multiple algorithms in multiple problems. R J. 2016, 8, 1–11. [Google Scholar] [CrossRef]
- Demšar, J. Statistical comparisons of classifiers over multiple data sets. J. Mach. Learn. Res. 2006, 7, 1–30. [Google Scholar]
- Muhammad, K.; Wang, S.-H.; Alsubai, S.; Binbusayyis, A.; Alqahtani, A.; Majumdar, A.; Thinnukool, O. Gastrointestinal diseases recognition: A framework of deep neural network and improved moth-crow optimization with dcca fusion. Hum.-Cent. Comput. Inf. Sci. 2022, 12, 25. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classifier | Org-MobV2 | Enh-MobV2 | Seg-MobV2 | Proposed | Accuracy (%) | Time (s) |
|---|---|---|---|---|---|---|
| √ | 95.24 | 116.5424 | ||||
| ELM | √ | 96.94 | 110.2010 | |||
| √ | 97.39 | 103.1152 | ||||
| √ | 99.61 | 69.5442 | ||||
| √ | 90.56 | 131.5032 | ||||
| Fine Tree | √ | 91.04 | 122.5629 | |||
| √ | 92.39 | 116.0424 | ||||
| √ | 94.84 | 74.5006 | ||||
| √ | 92.10 | 147.0302 | ||||
| Q-SVM | √ | 94.56 | 141.5624 | |||
| √ | 94.90 | 136.9206 | ||||
| √ | 96.36 | 89.1432 | ||||
| √ | 91.04 | 134.1142 | ||||
| W-KNN | √ | 92.50 | 129.5260 | |||
| √ | 94.14 | 121.1124 | ||||
| √ | 94.80 | 80.5142 | ||||
| √ | 92.52 | 119.4504 | ||||
| Bi-Layer NN | √ | 94.06 | 113.1492 | |||
| √ | 95.84 | 106.5824 | ||||
| √ | 98.16 | 71.0062 | ||||
| XGBOOST | √ | 92.26 | 126.0047 | |||
| √ | 92.95 | 110.8072 | ||||
| √ | 93.60 | 106.4921 | ||||
| √ | 94.00 | 70.6075 |
| Classifier | Org-MobV2 | Enh-MobV2 | Seg-MobV2 | Proposed | Accuracy (%) | Time (s) |
|---|---|---|---|---|---|---|
| √ | 95.24 | 92.1124 | ||||
| ELM | √ | 95.80 | 90.3645 | |||
| √ | 96.14 | 84.1046 | ||||
| √ | 98.20 | 52.5046 | ||||
| √ | 93.04 | 98.2446 | ||||
| Fine Tree | √ | 93.64 | 95.3604 | |||
| √ | 94.03 | 87.2942 | ||||
| √ | 96.46 | 63.1142 | ||||
| √ | 91.62 | 97.3046 | ||||
| Q-SVM | √ | 92.14 | 94.2946 | |||
| √ | 93.42 | 87.5042 | ||||
| √ | 95.14 | 71.0246 | ||||
| √ | 90.54 | 99.6214 | ||||
| W-KNN | √ | 91.32 | 97.5429 | |||
| √ | 91.98 | 90.1120 | ||||
| √ | 93.02 | 61.1129 | ||||
| √ | 94.34 | 94.1126 | ||||
| Bi-Layer NN | √ | 94.96 | 91.6624 | |||
| √ | 95.70 | 86.2404 | ||||
| √ | 97.10 | 55.5246 | ||||
| XGBOOST | √ | 93.58 | 104.5093 | |||
| √ | 94.02 | 101.9226 | ||||
| √ | 95.16 | 93.5521 | ||||
| √ | 95.90 | 69.4050 |
| Classifier | Org-MobV2 | Enh-MobV2 | Seg-MobV2 | Proposed | Accuracy (%) | Time (s) |
|---|---|---|---|---|---|---|
| √ | 94.20 | 191.5246 | ||||
| ELM | √ | 95.18 | 186.5509 | |||
| √ | 96.76 | 173.1142 | ||||
| √ | 98.02 | 102.5026 | ||||
| √ | 92.14 | 205.0426 | ||||
| Fine Tree | √ | 93.24 | 201.0020 | |||
| √ | 93.60 | 191.5462 | ||||
| √ | 95.46 | 120.2500 | ||||
| √ | 92.92 | 226.2042 | ||||
| Q-SVM | √ | 93.60 | 216.1120 | |||
| √ | 94.10 | 204.0526 | ||||
| √ | 96.40 | 140.0329 | ||||
| √ | 92.62 | 207.1246 | ||||
| W-KNN | √ | 92.94 | 203.0204 | |||
| √ | 93.56 | 195.5509 | ||||
| √ | 95.84 | 120.5426 | ||||
| √ | 93.04 | 195.0694 | ||||
| Bi-Layer NN | √ | 94.16 | 191.1124 | |||
| √ | 94.86 | 185.0329 | ||||
| √ | 96.94 | 110.0046 | ||||
| XGBOOST | √ | 93.00 | 220.0945 | |||
| √ | 93.84 | 211.2572 | ||||
| √ | 94.10 | 182.9443 | ||||
| √ | 94.90 | 136.0790 |
| Method | Accuracy (%) | ||
|---|---|---|---|
| CUI WCE Dataset | Kvasir V1 Dataset | Kvasir V2 Dataset | |
| VGG16 Model embedded in Figure 1 instead of MobileNetV2 | 95.80 | 94.28 | 95.11 |
| VGG19 Model embedded in Figure 1 instead of MobileNetV2 | 96.24 | 95.02 | 95.76 |
| AlexNet Model embedded in Figure 1 instead of MobileNetV2 | 95.16 | 94.66 | 94.90 |
| ResNet50 Model embedded in Figure 1 instead of MobileNetV2 | 97.88 | 95.89 | 96.16 |
| Khan et al. [36], 2022 | 99.42 | 97.85 | 97.85 |
| Proposed Framework | 99.61 | 98.20 | 98.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, M.A.; Sahar, N.; Khan, W.Z.; Alhaisoni, M.; Tariq, U.; Zayyan, M.H.; Kim, Y.J.; Chang, B. GestroNet: A Framework of Saliency Estimation and Optimal Deep Learning Features Based Gastrointestinal Diseases Detection and Classification. Diagnostics 2022, 12, 2718. https://doi.org/10.3390/diagnostics12112718
Khan MA, Sahar N, Khan WZ, Alhaisoni M, Tariq U, Zayyan MH, Kim YJ, Chang B. GestroNet: A Framework of Saliency Estimation and Optimal Deep Learning Features Based Gastrointestinal Diseases Detection and Classification. Diagnostics. 2022; 12(11):2718. https://doi.org/10.3390/diagnostics12112718
Chicago/Turabian StyleKhan, Muhammad Attique, Naveera Sahar, Wazir Zada Khan, Majed Alhaisoni, Usman Tariq, Muhammad H. Zayyan, Ye Jin Kim, and Byoungchol Chang. 2022. "GestroNet: A Framework of Saliency Estimation and Optimal Deep Learning Features Based Gastrointestinal Diseases Detection and Classification" Diagnostics 12, no. 11: 2718. https://doi.org/10.3390/diagnostics12112718
APA StyleKhan, M. A., Sahar, N., Khan, W. Z., Alhaisoni, M., Tariq, U., Zayyan, M. H., Kim, Y. J., & Chang, B. (2022). GestroNet: A Framework of Saliency Estimation and Optimal Deep Learning Features Based Gastrointestinal Diseases Detection and Classification. Diagnostics, 12(11), 2718. https://doi.org/10.3390/diagnostics12112718