
Interhemispheric Pediatric Meningioma, YAP1 Fusion-Positive

 , ,
, , 
 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
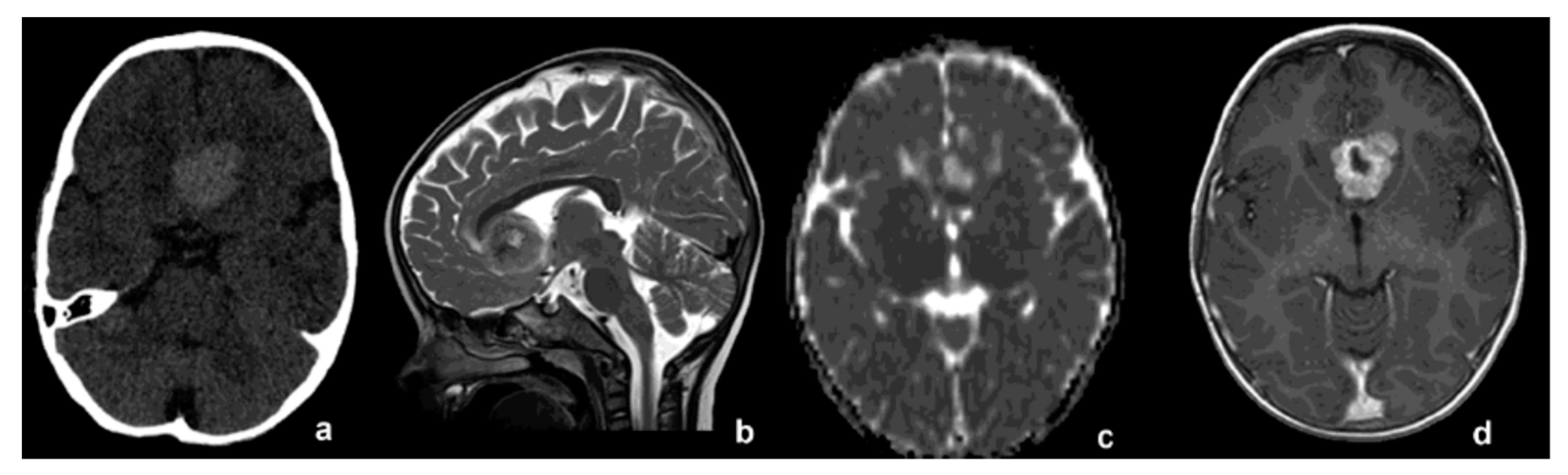
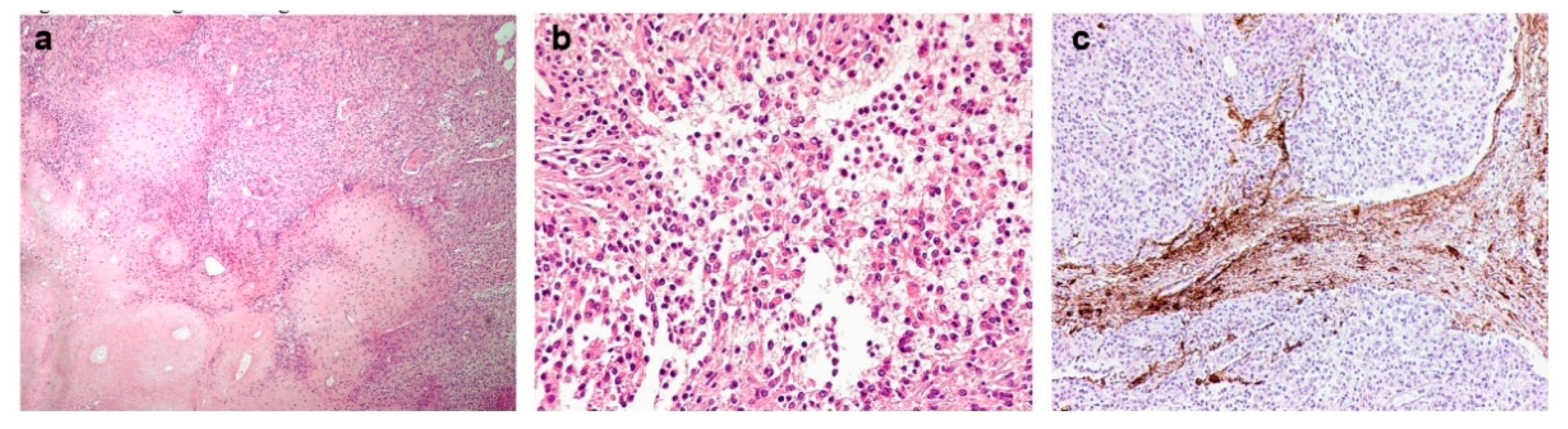
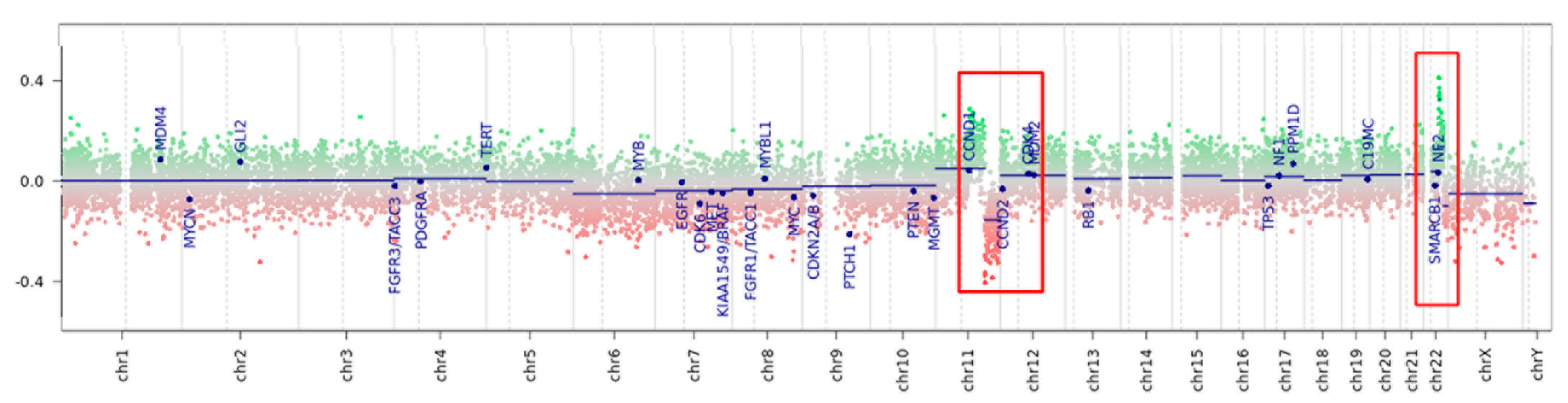
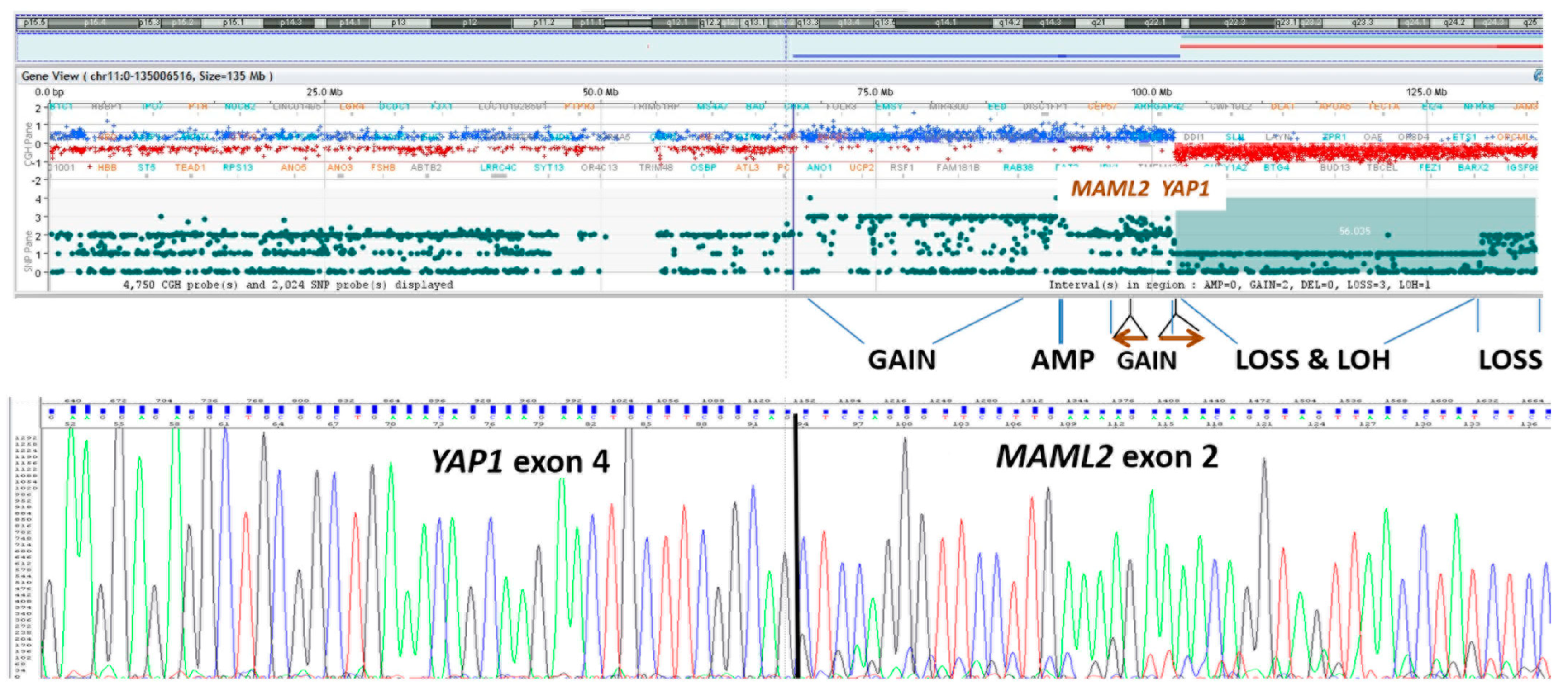
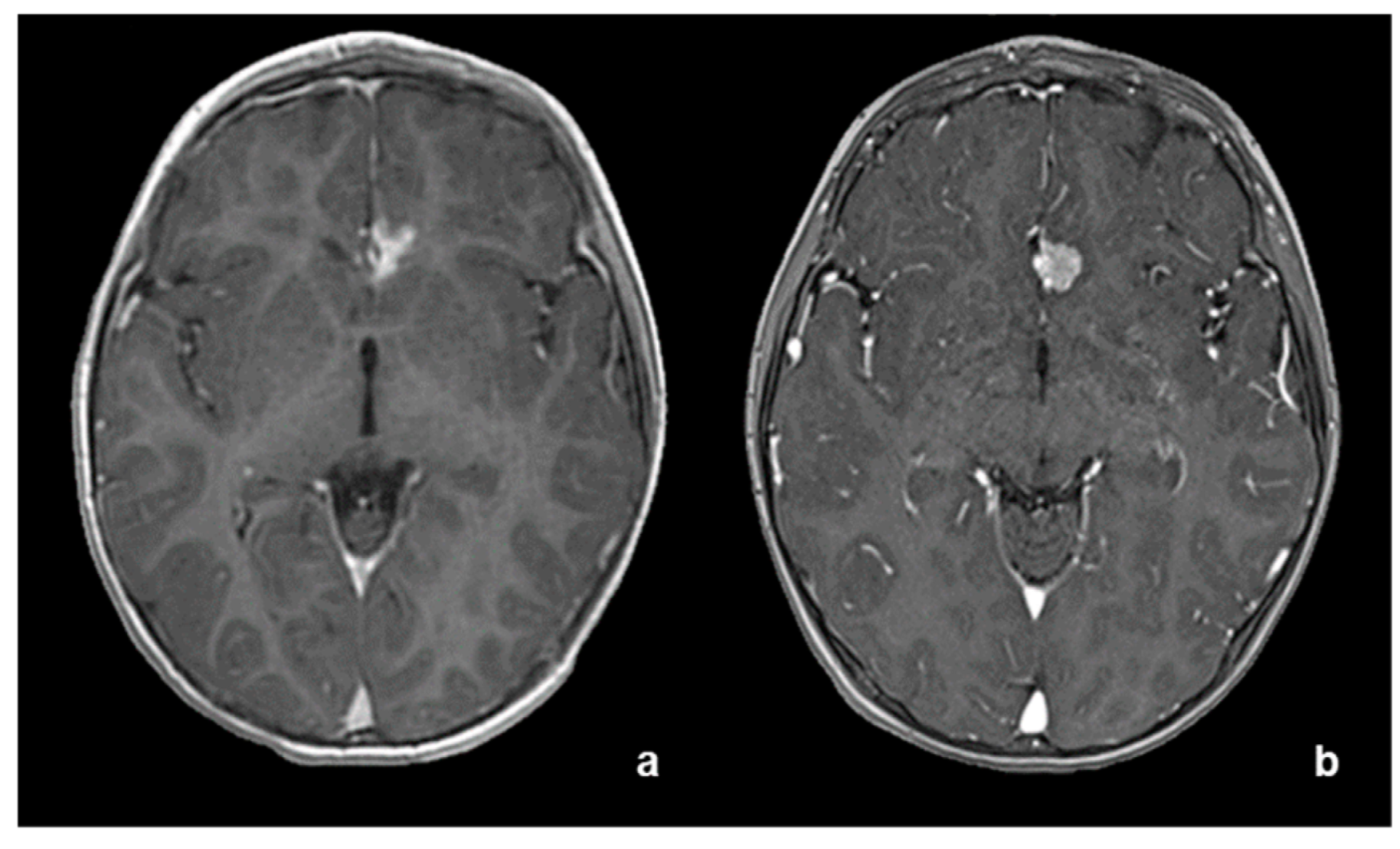
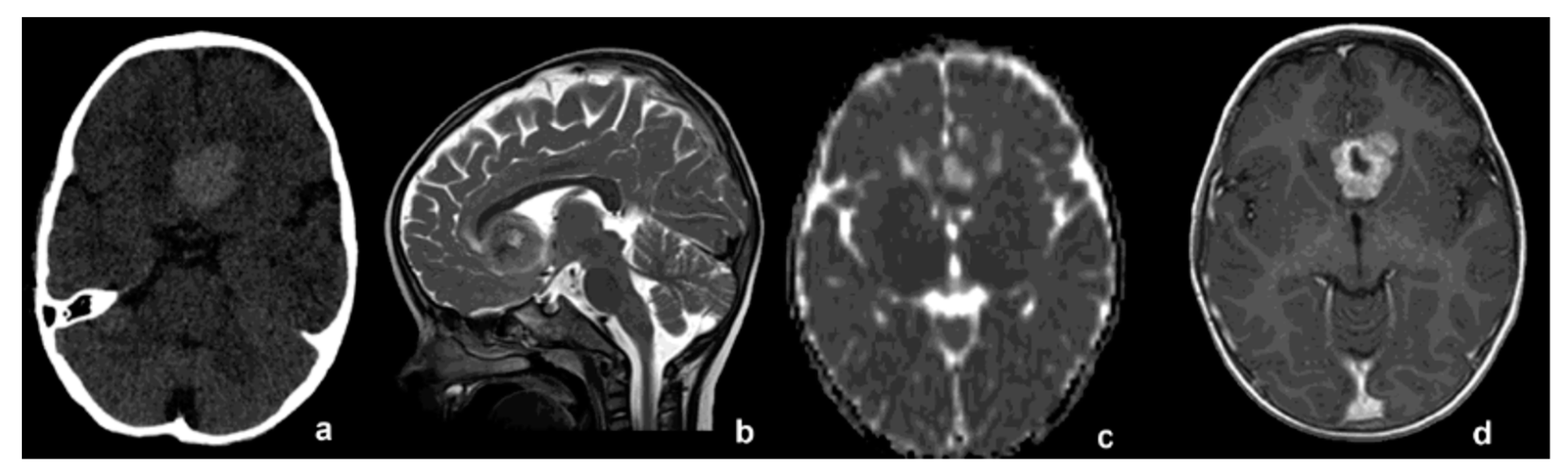
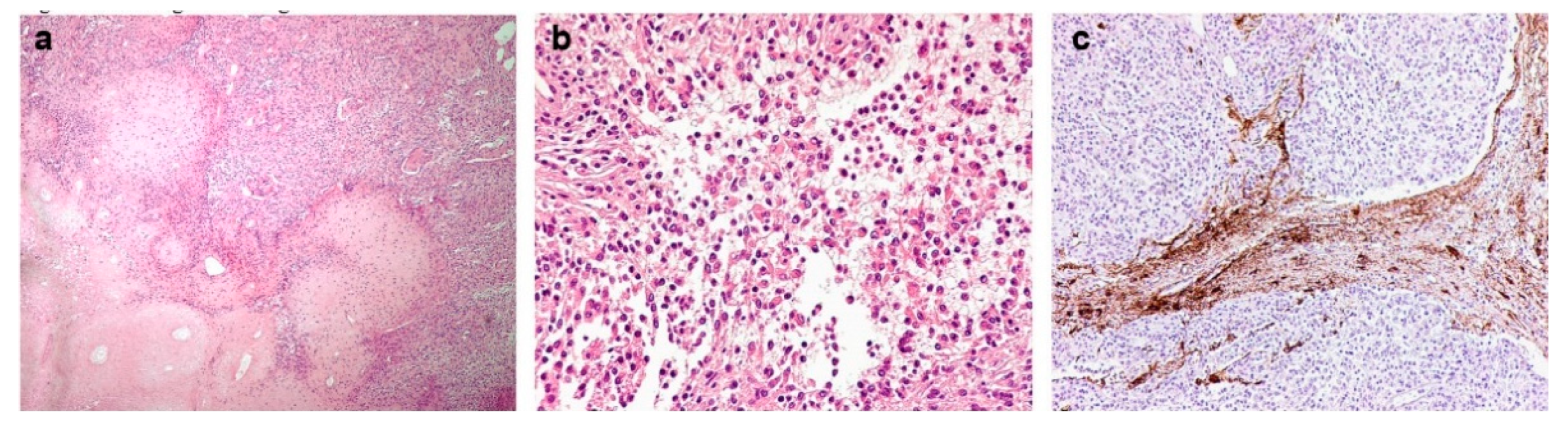
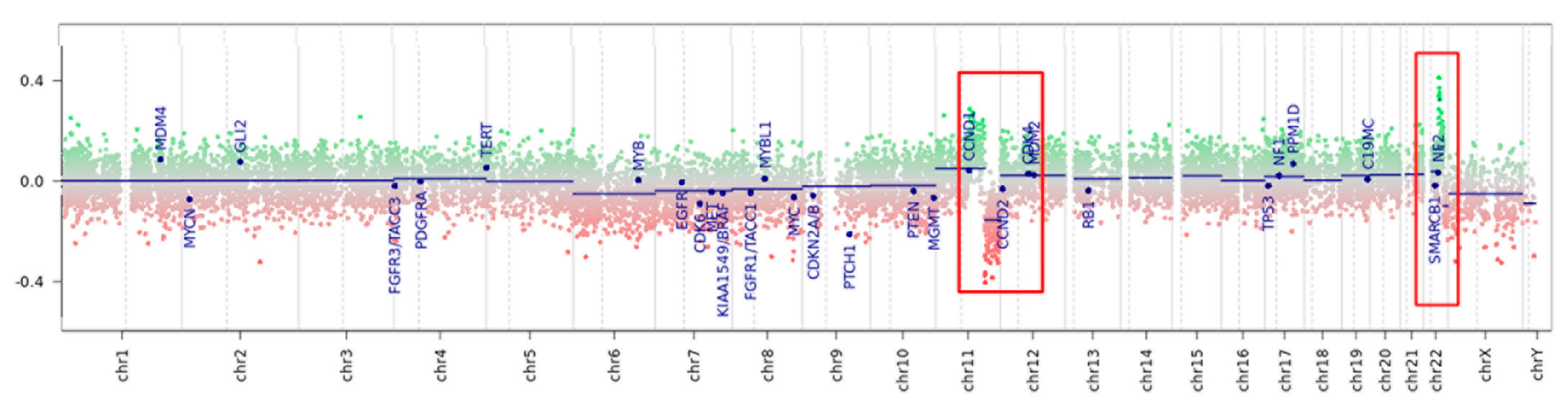
2. Case Report
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Material and Methods:
References
- Szychot, E.; Goodden, J.; Whitfield, G.; Curry, S. Children’s Cancer and Leukaemia Group (CCLG): Review and guidelines for the management of meningioma in children, teenagers and young adults. Br. J. Neurosurg. 2020, 34, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Toland, A.; McNulty, S.N.; Pekmezci, M.; Evenson, M.; Huntoon, K.; Pierson, C.R.; Boue, D.R.; Perry, A.; Dahiya, S. Pediatric meningioma: A clinicopathologic and molecular study with potential grading implications. Brain Pathol. 2020, 30, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- Battu, S.; Kumar, A.; Pathak, P.; Purkait, S.; Dhawan, L.; Sharma, M.C.; Suri, A.; Singh, M.; Sarkar, C.; Suri, V. Clinicopathological and molecular characteristics of pediatric meningiomas. Neuropathology 2018, 38, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Pathmanaban, O.N.; Sadler, K.V.; Kamaly-Asl, I.D.; King, A.T.; Rutherford, S.A.; Hammerbeck-Ward, C.; McCabe, M.G.; Kilday, J.P.; Beetz, C.; Poplawski, N.K.; et al. Association of Genetic Predisposition with Solitary Schwannoma or Meningioma in Children and Young Adults. JAMA Neurol. 2017, 74, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Sievers, P.; Chiang, J.; Schrimpf, D.; Stichel, D.; Paramasivam, N.; Sill, M.; Gayden, T.; Casalini, B.; Reuss, D.E.; Dalton, J.; et al. YAP1-fusions in pediatric NF2-wildtype meningioma. Acta Neuropathol. 2020, 139, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Schieffer, K.M.; Agarwal, V.; LaHaye, S.; Miller, K.E.; Koboldt, D.C.; Lichtenberg, T.; Leraas, K.; Brennan, P.; Kelly, B.J.; Crist, E.; et al. YAP1-FAM118B Fusion Defines a Rare Subset of Childhood and Young Adulthood Meningiomas. Am. J. Surg. Pathol. 2021, 45, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Capper, D.; Jones, D.T.W.; Sill, M.; Hovestadt, V.; Schrimpf, D.; Sturm, D.; Koelsche, C.; Sahm, F.; Chavez, L.; Reuss, D.E.; et al. DNA methylation-based classification of central nervous system tumours. Nature 2018, 555, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Zanconato, F.; Cordenonsi, M.; Piccolo, S. YAP/TAZ at the Roots of Cancer. Cancer Cell 2016, 29, 783–803. [Google Scholar] [CrossRef] [PubMed]
- Szulzewsky, F.; Holland, E.C.; Vasioukhin, V. YAP1 and its fusion proteins in cancer initiation, progression and therapeutic resistance. Dev. Biol. 2021, 475, 205–221. [Google Scholar] [CrossRef] [PubMed]
- Ohba, S.; Abe, M.; Hasegawa, M.; Hirose, Y. Intraparenchymal Meningioma: Clinical, Radiologic, and Histologic Review. World Neurosurg. 2016, 92, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Liang, H.; Wang, J.; Wen, S.; Wang, Y.; Wang, Y.; Ma, Z. Giant Intraparenchymal Meningioma in a Female Child: Case Report and Literature Review. Cancer Manag. Res. 2021, 13, 1989–1997. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age (Years) | Sex | Tumor Location | MNG WHO Grade | Genetic Alteration |
|---|---|---|---|---|---|
| Present case | |||||
| 1 | 2 | M | Frontal interhemispheric space | II | YAP1-MAML2 |
| Sievers et al. [5] | |||||
| 2 | 4 | F | Lateral ventricles, third ventricle | II | YAP1:MAML2 |
| 3 | 3 | M | Temporal | I | YAP1:PYGO1 |
| 4 | 1 | M | Third ventricle, lateral ventricle | NA | YAP1:MAML2 |
| 5 | 2 | M | Skull base | NA | YAP1:MAML2 |
| 6 | 8 | F | Skull base | I | YAP1:LMO1 |
| 7 | 17 | M | Cavernous sinus | I | YAP1:MAML2 |
| 8 | 7 | F | Parietal | NA | YAP1:MAML2 |
| 9 | 7 | F | Frontal | I | YAP1:MAML2 |
| Schieffer et al. [6] | |||||
| 10 | 0, 57 | F | Temporal | II | YAP1:FAM118B |
| 11 | 20 | M | Rolandic sulcus | II | YAP1:FAM118B |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esposito, S.; Marucci, G.; Antonelli, M.; Miele, E.; Modena, P.; Giagnacovo, M.; Massimino, M.; Biassoni, V.; Taddei, M.; Schiariti, M.P.; et al. Interhemispheric Pediatric Meningioma, YAP1 Fusion-Positive. Diagnostics 2022, 12, 2367. https://doi.org/10.3390/diagnostics12102367
Esposito S, Marucci G, Antonelli M, Miele E, Modena P, Giagnacovo M, Massimino M, Biassoni V, Taddei M, Schiariti MP, et al. Interhemispheric Pediatric Meningioma, YAP1 Fusion-Positive. Diagnostics. 2022; 12(10):2367. https://doi.org/10.3390/diagnostics12102367
Chicago/Turabian StyleEsposito, Silvia, Gianluca Marucci, Manila Antonelli, Evelina Miele, Piergiorgio Modena, Marzia Giagnacovo, Maura Massimino, Veronica Biassoni, Matilde Taddei, Marco Paolo Schiariti, and et al. 2022. "Interhemispheric Pediatric Meningioma, YAP1 Fusion-Positive" Diagnostics 12, no. 10: 2367. https://doi.org/10.3390/diagnostics12102367
APA StyleEsposito, S., Marucci, G., Antonelli, M., Miele, E., Modena, P., Giagnacovo, M., Massimino, M., Biassoni, V., Taddei, M., Schiariti, M. P., Doniselli, F. M., Moscatelli, M., Chiapparini, L., & Pollo, B. (2022). Interhemispheric Pediatric Meningioma, YAP1 Fusion-Positive. Diagnostics, 12(10), 2367. https://doi.org/10.3390/diagnostics12102367