
IMSI—Guidelines for Sperm Quality Assessment

 , , , ,
, , , , 
Abstract
1. Introduction
2. Magnification and Resolution
- d = optical resolution
- λ = wavelength of the illuminating light used
- η = refractive index of the optical medium between the front lens and cover glass
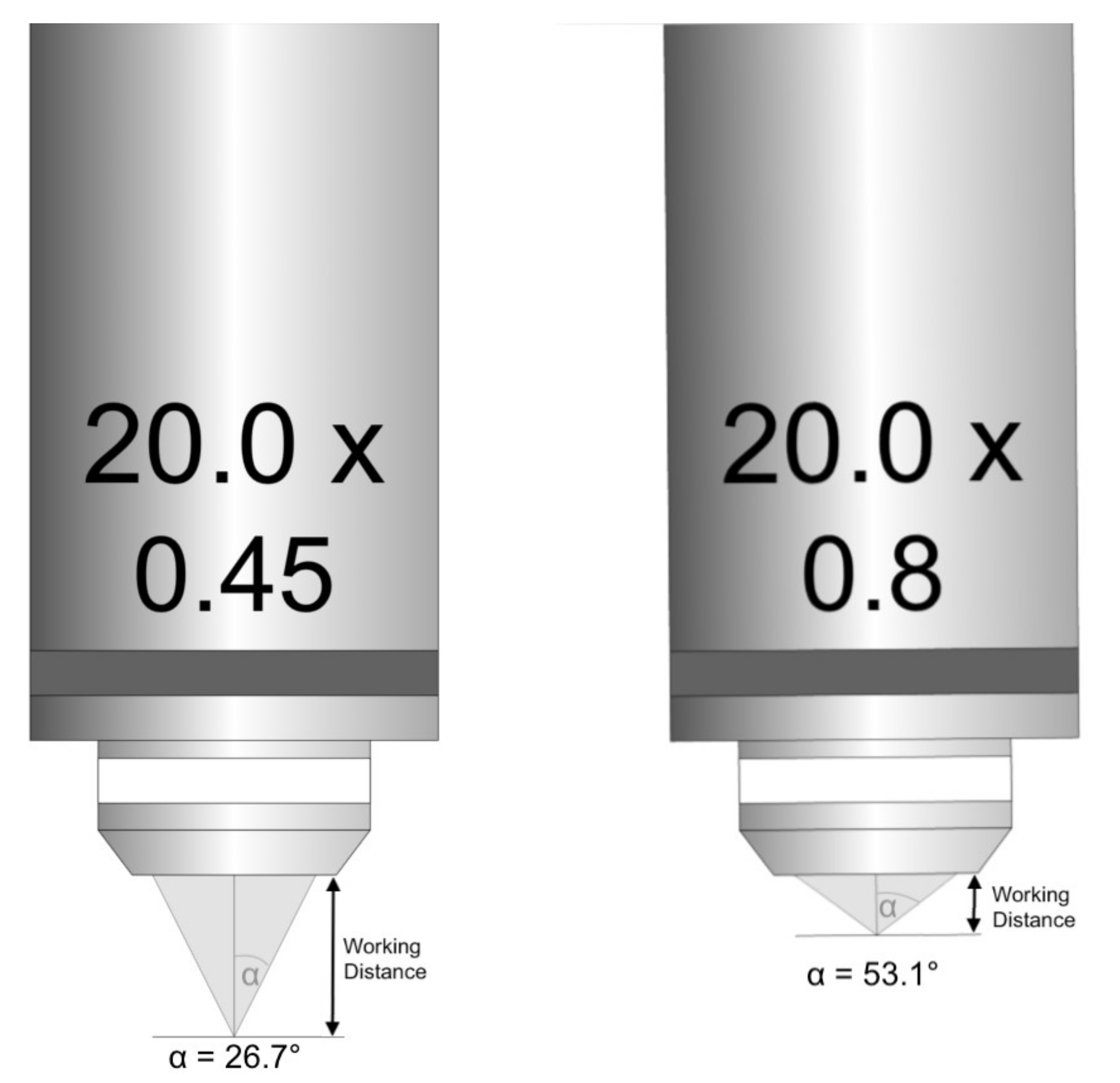
- α = half the opening angle of the objective used.
- NA = numeric aperture
- η = refractive index of the optical medium between the front lens and cover glass
- α = half the opening angle of the objective used.
3. What Is Then the Optical Resolution of the Optical Systems Used for In Vitro Fertilization (Micromanipulation for ICSI)?
4. What Is Then the Optical Resolution of the Systems Used for IMSI?
5. What Are the Paremeters of the System Sufficient for ICSI and IMSI?
- ▪
- the blue light filter of 400 nm
- ▪
- condenser with working distance (WD) = 40 mm and NA 0.6
- ▪
- 63× or 100× objective with NA 0.9
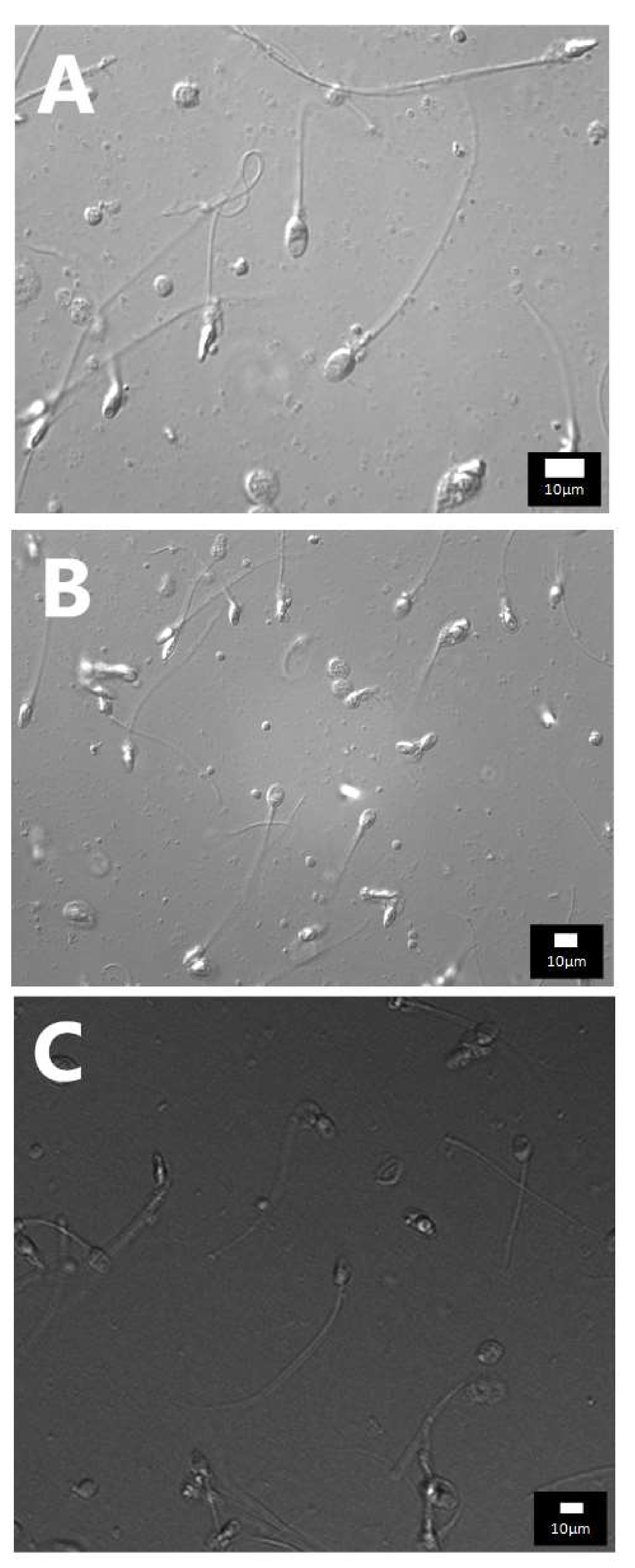
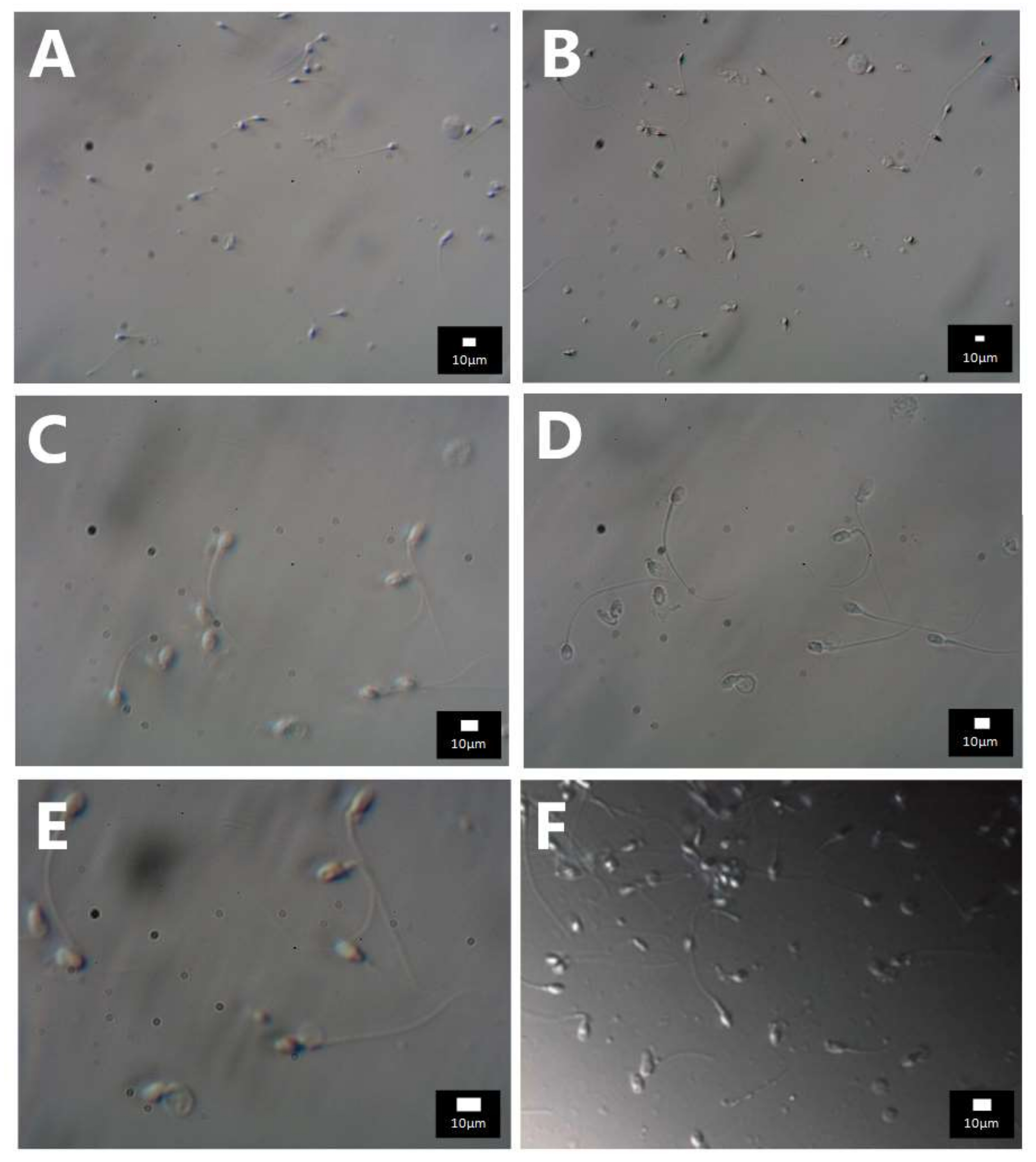
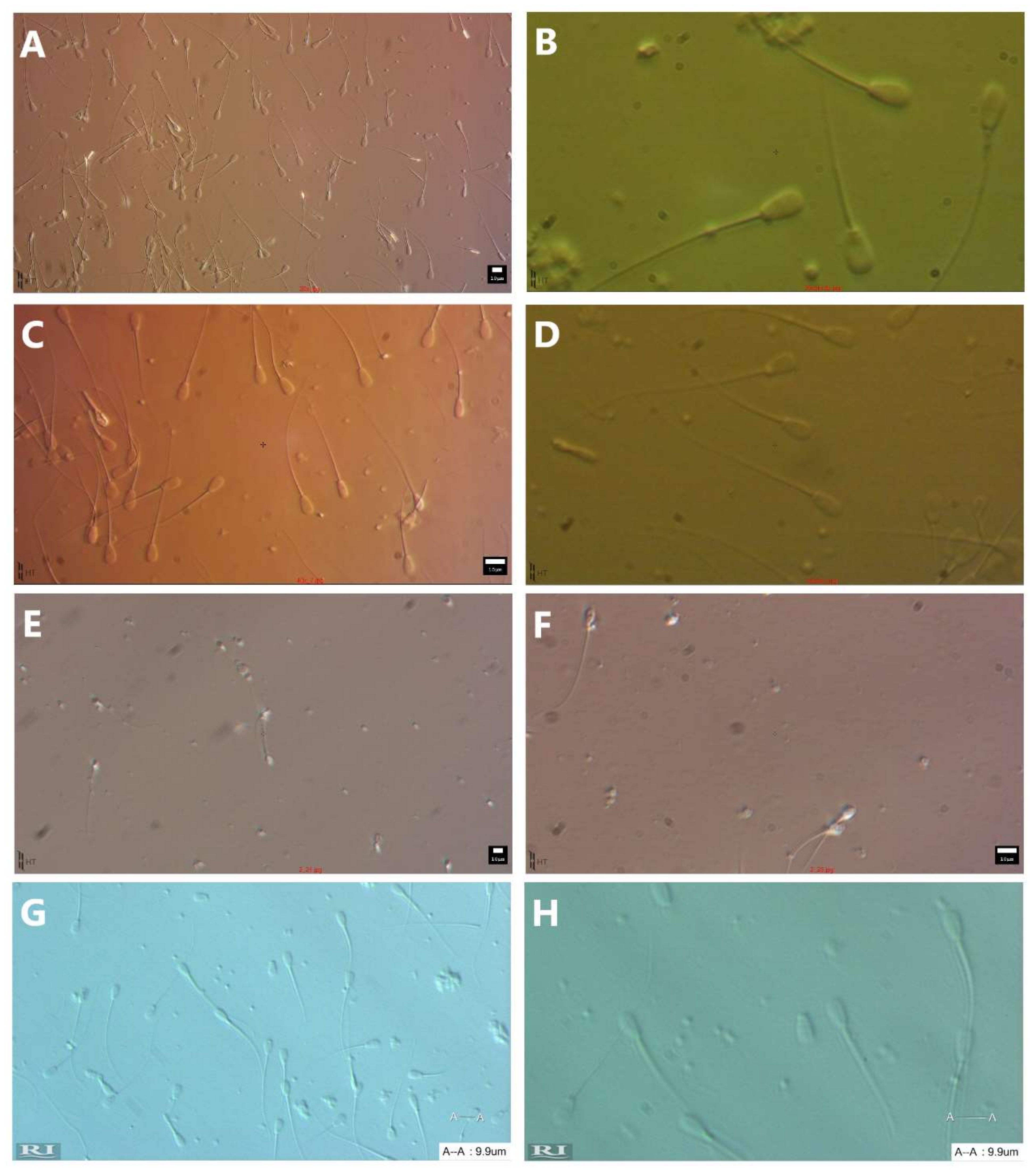
6. Do We Need a Camera for Better Visualization of the Spermatozoa Morphology?
7. Our Experience
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 | 1.22 |
| Wavelength (nm) | 550 | 400 | 550 | 400 | 400 | 700 | 550 | 400 | 550 | 550 | 550 | 550 | 550 | 550 | 550 | 550 |
| nm | 671.00 | 488.00 | 671.00 | 488.00 | 488.00 | 854.00 | 671.00 | 488.00 | 671.00 | 671.00 | 671.00 | 671.00 | 671.00 | 671.00 | 671.00 | 671.00 |
| µm | 0.671 | 0.488 | 0.671 | 0.488 | 0.488 | 0.854 | 0.671 | 0.488 | 0.671 | 0.671 | 0.671 | 0.671 | 0.671 | 0.671 | 0.671 | 0.671 |
| Condenser NA | 0.4 | 0.4 | 0.55 | 0.55 | 0.6 | 0.4 | 0.4 | 1.25 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 |
| Objective NA | 1.35 | 1.35 | 1.35 | 0.7 | 0.6 | 1.35 | 1.3 | 1.5 | 1.35 | 1.35 | 0.6 | 0.55 | 1.35 | 1.35 | 1.35 | 1.35 |
| NA cond. + NA obj. | 1.75 | 1.75 | 1.9 | 1.25 | 1.2 | 1.75 | 1.7 | 2.75 | 1.75 | 1.75 | 1 | 0.95 | 1.75 | 1.75 | 1.75 | 1.75 |
| Resolution (µm) | 0.383429 | 0.27886 | 0.353158 | 0.3904 | 0.40667 | 0.488 | 0.395 | 0.177 | 0.383 | 0.383 | 0.671 | 0.706 | 0.3834 | 0.38343 | 0.38343 | 0.3834 |
| Resolution of good eyesight—81 um | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 81 |
| Magnification required | 211.2519 | 290.471 | 229.3592 | 207.48 | 199.18 | 166 | 205.2 | 456.5 | 211.3 | 211.3 | 120.71535 | 114.7 | 211.25 | 211.252 | 211.252 | 211.25 |
| Objective magnification | 100 | 100 | 100 | 60 | 40 | 100 | 100 | 100 | 100 | 100 | 40 | 40 | 100 | 100 | 100 | 100 |
| Eyepiece magnification | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 |
| Total magnification | 1000 | 1000 | 1000 | 600 | 400 | 1000 | 1000 | 1000 | 1000 | 1000 | 400 | 400 | 1000 | 1000 | 1000 | 1000 |
| Resolution of bad eyesight—250 um | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 | 250 |
| Magnification required | 652.0119 | 896.516 | 707.8987 | 640.369 | 614.754 | 512.3 | 633.4 | 1409 | 652 | 652 | 372.578241 | 353.9 | 652.01 | 652.012 | 652.012 | 652.01 |
| Objective magnification | 100 | 100 | 100 | 60 | 40 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Eyepiece magnification | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 |
| Total magnification | 1000 | 1000 | 1000 | 600 | 400 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 |
References
- Palermo, G.; Joris, H.; Devroey, P.; van Steirteghem, A.C. Pregnancies after intracytoplasmic injection of single spermatozoon into an oocyte. Lancet 1992, 340, 17–18. [Google Scholar] [CrossRef]
- Ferraretti, A.P.; Nygren, K.; Andersen, A.N.; de Mouzon, J.; Kupka, M.; Calhaz-Jorge, C.; Wyns, C.; Gianaroli, L.; Goossens, V.; European IVF-Monitoring Consortium (EIM), for the European Society of Human Reproduction and Embryology (ESHRE). Trends over 15 years in ART in Europe: An analysis of 6 million cycles. Hum. Reprod. Open. 2017, 2017, hox012. [Google Scholar] [CrossRef]
- Alukal, J.P.; Lamb, D.J. Intracytoplasmic sperm injection (ICSI)—What are the risks? Urol. Clin. N. Am. 2008, 35, 277–288. [Google Scholar] [CrossRef]
- Wong, M.Y.W.; Ledger, W.L. Is ICSI Risky? Obstet. Gynecol. Int. Hindawi 2013, 2013, 473289. [Google Scholar] [CrossRef]
- Bartoov, B.; Berkovitz, A.; Eltes, F. Selection of spermatozoa with normal nuclei to improve the pregnancy rate with intracytoplasmic sperm injection. N. Engl. J. Med. 2001, 345, 1067–1068. [Google Scholar] [CrossRef]
- Gatimel, N.; Parinaud, J.; Leandri, R.D. Intracytoplasmic morphologically selected sperm injection (IMSI) does not improve outcome in patients with two successive IVF-ICSI failures. J. Assist. Reprod. Genet. 2016, 33, 349–355. [Google Scholar] [CrossRef]
- Nadalini, M.; Tarozzi, N.; Distratis, V.; Scaravelli, G.; Borini, A. Impact of intracytoplasmic morphologically selected sperm injection on assisted reproduction outcome: A review. Reprod. Biomed. Online 2009, 19 (Suppl. S3), 45–55. [Google Scholar] [CrossRef]
- Delaroche, L.; Yazbeck, C.; Gout, C.; Kahn, V.; Oger, P.; Rougier, N. Intracytoplasmic morphologically selected sperm injection (IMSI) after repeated IVF or ICSI failures: A prospective comparative study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 167, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Setti, A.S.; Figueira, R.C.S.; Braga, D.P.A.F.; Iaconelli, A.; Borges, E. Gender incidence of intracytoplasmic morphologically selected sperm injection-derived embryos: A prospective randomized study. Reprod. Biomed. Online 2012, 24, 420–423. [Google Scholar] [CrossRef][Green Version]
- Leandri, R.D.; Gachet, A.; Pfeffer, J.; Celebi, C.; Rives, N.; Carre-Pigeon, F.; Kulski, O.; Mitchell, J.; Parinaud, J. Is intracytoplasmic morphologically selected sperm injection (IMSI) beneficial in the first ART cycle? A multicentric randomized controlled trial. Andrology 2013, 1, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Bartoov, B.; Berkovitz, A.; Eltes, F.; Kogosovsky, A.; Yagoda, A.; Lederman, H.; Artzi, S.; Gross, M.; Barak, Y. Pregnancy rates are higher with intracytoplasmic morphologically selected sperm injection than with conventional intracytoplasmic injection. Fertil. Steril. 2003, 80, 1413–1419. [Google Scholar] [CrossRef]
- Wilding, M.; Coppola, G.; di Matteo, L.; Palagiano, A.; Fusco, E.; Dale, B. Intracytoplasmic injection of morphologically selected spermatozoa (IMSI) improves outcome after assisted reproduction by deselecting physiologically poor quality spermatozoa. J. Assist. Reprod. Genet. 2011, 28, 253–262. [Google Scholar] [CrossRef]
- Berkovitz, A.; Eltes, F.; Lederman, H.; Peer, S.; Ellenbogen, A.; Feldberg, B.; Bartoov, B. How to improve IVF-ICSI outcome by sperm selection. Reprod. Biomed. Online 2006, 12, 634–638. [Google Scholar] [CrossRef]
- Vanderzwalmen, P.; Hiemer, A.; Rubner, P.; Bach, M.; Neyer, A.; Stecher, A.; Uher, P.; Zintz, M.; Lejeune, B.; Vanderzwalmen, S.; et al. Blastocyst development after sperm selection at high magnification is associated with size and number of nuclear vacuoles. Reprod. Biomed. Online 2008, 17, 617–627. [Google Scholar] [CrossRef]
- El Khattabi, L.; Dupont, C.; Sermondade, N.; Hugues, J.-N.; Poncelet, C.; Porcher, R.; Cedrin-Durnerin, I.; Lévy, R.; Sifer, C. Is intracytoplasmic morphologically selected sperm injection effective in patients with infertility related to teratozoospermia or repeated implantation failure? Fertil. Steril. 2013, 100, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Luna, D.; Hilario, R.; Dueñas-Chacón, J.; Romero, R.; Zavala, P.; Villegas, L.; García-Ferreyra, J. The IMSI Procedure Improves Laboratory and Clinical Outcomes Without Compromising the Aneuploidy Rate When Compared to the Classical ICSI Procedure. Clin. Med. Insights Reprod. Health 2015, 9, 29–37. [Google Scholar] [CrossRef]
- Klement, A.H.; Koren-Morag, N.; Itsykson, P.; Berkovitz, A. Intracytoplasmic morphologically selected sperm injection versus intracytoplasmic sperm injection: A step toward a clinical algorithm. Fertil. Steril. 2013, 99, 1290–1293. [Google Scholar] [CrossRef] [PubMed]
- Setti, A.S.; Figueira, R.C.S.; Braga, D.P.A.F.; Aoki, T.; Iaconelli, A.; Borges, E. Intracytoplasmic morphologically selected sperm injection is beneficial in cases of advanced maternal age: A prospective randomized study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 171, 286–290. [Google Scholar] [CrossRef]
- Hazout, A.; Dumont-Hassan, M.; Junca, A.-M.; Cohen Bacrie, P.; Tesarik, J. High-magnification ICSI overcomes paternal effect resistant to conventional ICSI. Reprod. Biomed. Online 2006, 12, 19–25. [Google Scholar] [CrossRef]
- Antinori, M.; Licata, E.; Dani, G.; Cerusico, F.; Versaci, C.; d’Angelo, D.; Antinori, S. Intracytoplasmic morphologically selected sperm injection: A prospective randomized trial. Reprod. Biomed. Online 2008, 16, 835–841. [Google Scholar] [CrossRef]
- Knez, K.; Tomazevic, T.; Zorn, B.; Vrtacnik-Bokal, E.; Virant-Klun, I. Intracytoplasmic morphologically selected sperm injection improves development and quality of preimplantation embryos in teratozoospermia patients. Reprod. Biomed. Online 2012, 25, 168–179. [Google Scholar] [CrossRef]
- Berkovitz, A.; Eltes, F.; Ellenbogen, A.; Peer, S.; Feldberg, D.; Bartoov, B. Does the presence of nuclear vacuoles in human sperm selected for ICSI affect pregnancy outcome? Hum. Reprod. 2006, 21, 1787–1790. [Google Scholar] [CrossRef]
- Pastuszek, E.; Kiewisz, J.; Kulwikowska, P.; Liss, J.; Lukaszuk, M.; Bruszczynska, A.; Jakiel, G.; Lukaszuk, K. An investigation of the potential effect of sperm nuclear vacuoles in human spermatozoa on DNA fragmentation using a neutral and alkaline Comet assay. Andrology 2017, 5, 392–398. [Google Scholar] [CrossRef]
- Oliveira, J.B.A.; Cavagna, M.; Petersen, C.G.; Mauri, A.L.; Massaro, F.C.; Silva, L.F.I.; Baruffi, R.L.R.; Franco, J.G., Jr. Pregnancy outcomes in women with repeated implantation failures after intracytoplasmic morphologically selected sperm injection (IMSI). Reprod. Biol. Endocrinol. 2011, 9, 99. [Google Scholar] [CrossRef] [PubMed]
- Knez, K.; Zorn, B.; Tomazevic, T.; Vrtacnik-Bokal, E.; Virant-Klun, I. The IMSI procedure improves poor embryo development in the same infertile couples with poor semen quality: A comparative prospective randomized study. Reprod. Biol. Endocrinol. 2011, 9, 123. [Google Scholar] [CrossRef]
- Setti, A.S.; de Cássia Figueira, R.S.; Braga, D.P.A.F.; Iaconelli, A.; Borges, E. Intracytoplasmic morphologically selected sperm injection benefits for patients with oligoasthenozoospermia according to the 2010 World Health Organization reference values. Fertil. Steril. 2011, 95, 2711–2714. [Google Scholar] [CrossRef]
- Balaban, B.; Yakin, K.; Alatas, C.; Oktem, O.; Isiklar, A.; Urman, B. Clinical outcome of intracytoplasmic injection of spermatozoa morphologically selected under high magnification: A prospective randomized study. Reprod. Biomed. Online 2011, 22, 472–476. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Marci, R.; Murisier, F.; Lo Monte, G.; Soave, I.; Chanson, A.; Urner, F.; Germond, M. Clinical outcome after IMSI procedure in an unselected infertile population: A pilot study. Reprod. Health 2013, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- De Cássia Figueira, R.S.; Braga, D.P.A.F.; Setti, A.S.; Iaconelli, A.; Borges, E. Morphological nuclear integrity of sperm cells is associated with preimplantation genetic aneuploidy screening cycle outcomes. Fertil. Steril. 2011, 95, 990–993. [Google Scholar] [CrossRef] [PubMed]
- De Vos, A.; van de Velde, H.; Bocken, G.; Eylenbosch, G.; Franceus, N.; Meersdom, G.; Tistaert, S.; Vankelecom, A.; Tournaye, H.; Verheyen, G. Does intracytoplasmic morphologically selected sperm injection improve embryo development? A randomized sibling-oocyte study. Hum. Reprod. 2013, 28, 617–626. [Google Scholar] [CrossRef]
- Orief, Y.; Elabd, M.; Said, T.; Ahmed, N. Comparative study between intracytoplasmic morphologically selected sperm injection versus intracytoplasmic sperm injection in patients with severe male factor infertility and repeated intra cytoplasmic sperm injection failure. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016, 5, 1102–1107. [Google Scholar] [CrossRef]
- Mauri, A.L.; Petersen, C.G.; Oliveira, J.B.A.; Massaro, F.C.; Baruffi, R.L.R.; Franco, J.G. Comparison of day 2 embryo quality after conventional ICSI versus intracytoplasmic morphologically selected sperm injection (IMSI) using sibling oocytes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 150, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Boediono, A.; Handayani, N.; Sari, H.N.; Yusup, N.; Indrasari, W.; Polim, A.A.; Sini, I. Morphokinetics of embryos after IMSI versus ICSI in couples with sub-optimal sperm quality: A time-lapse study. Andrologia 2021, 53, e14002. [Google Scholar] [CrossRef]
- Mangoli, E.; Khalili, M.A.; Talebi, A.R.; Kalantar, S.M.; Montazeri, F.; Agharahimi, A.; Woodward, B.J. Association between early embryo morphokinetics plus transcript levels of sperm apoptotic genes and clinical outcomes in IMSI and ICSI cycles of male factor patients; Springer. J. Assist. Reprod. Genet. 2020, 37, 2555–2567. [Google Scholar] [CrossRef]
- Asali, A.; Miller, N.; Pasternak, Y.; Freger, V.; Belenky, M.; Berkovitz, A. The possibility of integrating motile sperm organelle morphology examination (MSOME) with intracytoplasmic morphologically-selected sperm injection (IMSI) when treating couples with unexplained infertility; Public Library of Science. PLoS ONE 2020, 15, e0232156. [Google Scholar] [CrossRef]
- Teixeira, D.M.; Hadyme Miyague, A.; Barbosa, M.A.P.; Navarro, P.A.; Raine-Fenning, N.; Nastri, C.O.; Martins, W.P. Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction. Cochrane Database Syst. Rev. 2020, 2, CD010167. [Google Scholar] [CrossRef] [PubMed]
- Schachter-Safrai, N.; Karavani, G.; Reuveni-Salzman, A.; Gil, M.; Ben-Meir, A. Which semen analysis correlates with favorable Intracytoplasmic morphologically selected sperm injection (IMSI) outcomes? Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 234, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Duran-Retamal, M.; Morris, G.; Achilli, C.; Gaunt, M.; Theodorou, E.; Saab, W.; Serhal, P.; Seshadri, S. Live birth and miscarriage rate following intracytoplasmic morphologically selected sperm injection vs intracytoplasmic sperm injection: An updated systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2020, 99, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Diaspro, A.; Usai, C. Optical Microscopy. Wiley Encyclopedia of Biomedical Engineering; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Weisenburger, S.; Sandoghdar, V. Light microscopy: An ongoing contemporary revolution. Contemp. Phys. 2015, 56, 123–143. [Google Scholar] [CrossRef]
- Quilliam, T.A. The electromagnetic spectrum, the eye, and vision. Med Boil. Illustration 1971, 21, 223–228. [Google Scholar]
- Hoffman, R.; Gross, L. The modulation contrast microscope. Nat. Cell Biol. 1975, 254, 586–588. [Google Scholar] [CrossRef]
- Hoffman, R. The modulation contrast microscope: Principles and performance. J. Microsc. 1977, 110, 205–222. [Google Scholar] [CrossRef]
- Lang, W. Nomarski differential interference-contrast microscopy. ZEISS Inf. 1968, 70, 114–120. [Google Scholar]
- Shribak, M. Differential Interference Contrast Microscopy (DIC). Biomed. Opt. Phase Microscopy Nanoscopy 2013, 19–42. [Google Scholar] [CrossRef]
- Montag, M. A Practical Guide to Selecting Gametes and Embryos.; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Deering, M.F. The Limits of Human Vision. 2nd International Immersive Projection Technology Workshop. 1998. Available online: http://michaelfrankdeering.org/Projects/EyeModel/limits.pdf (accessed on 27 November 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lukaszuk, K.; Jakiel, G.; Wocławek Potocka, I.; Kiewisz, J.; Olszewska, J.; Sieg, W.; Podolak, A.; Pastuszek, E.; Wdowiak, A. IMSI—Guidelines for Sperm Quality Assessment. Diagnostics 2022, 12, 192. https://doi.org/10.3390/diagnostics12010192
Lukaszuk K, Jakiel G, Wocławek Potocka I, Kiewisz J, Olszewska J, Sieg W, Podolak A, Pastuszek E, Wdowiak A. IMSI—Guidelines for Sperm Quality Assessment. Diagnostics. 2022; 12(1):192. https://doi.org/10.3390/diagnostics12010192
Chicago/Turabian StyleLukaszuk, Krzysztof, Grzegorz Jakiel, Izabela Wocławek Potocka, Jolanta Kiewisz, Jolanta Olszewska, Wlodzimierz Sieg, Amira Podolak, Ewa Pastuszek, and Artur Wdowiak. 2022. "IMSI—Guidelines for Sperm Quality Assessment" Diagnostics 12, no. 1: 192. https://doi.org/10.3390/diagnostics12010192
APA StyleLukaszuk, K., Jakiel, G., Wocławek Potocka, I., Kiewisz, J., Olszewska, J., Sieg, W., Podolak, A., Pastuszek, E., & Wdowiak, A. (2022). IMSI—Guidelines for Sperm Quality Assessment. Diagnostics, 12(1), 192. https://doi.org/10.3390/diagnostics12010192