
Aerobic Vaginitis Diagnosis Criteria Combining Gram Stain with Clinical Features: An Establishment and Prospective Validation Study

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
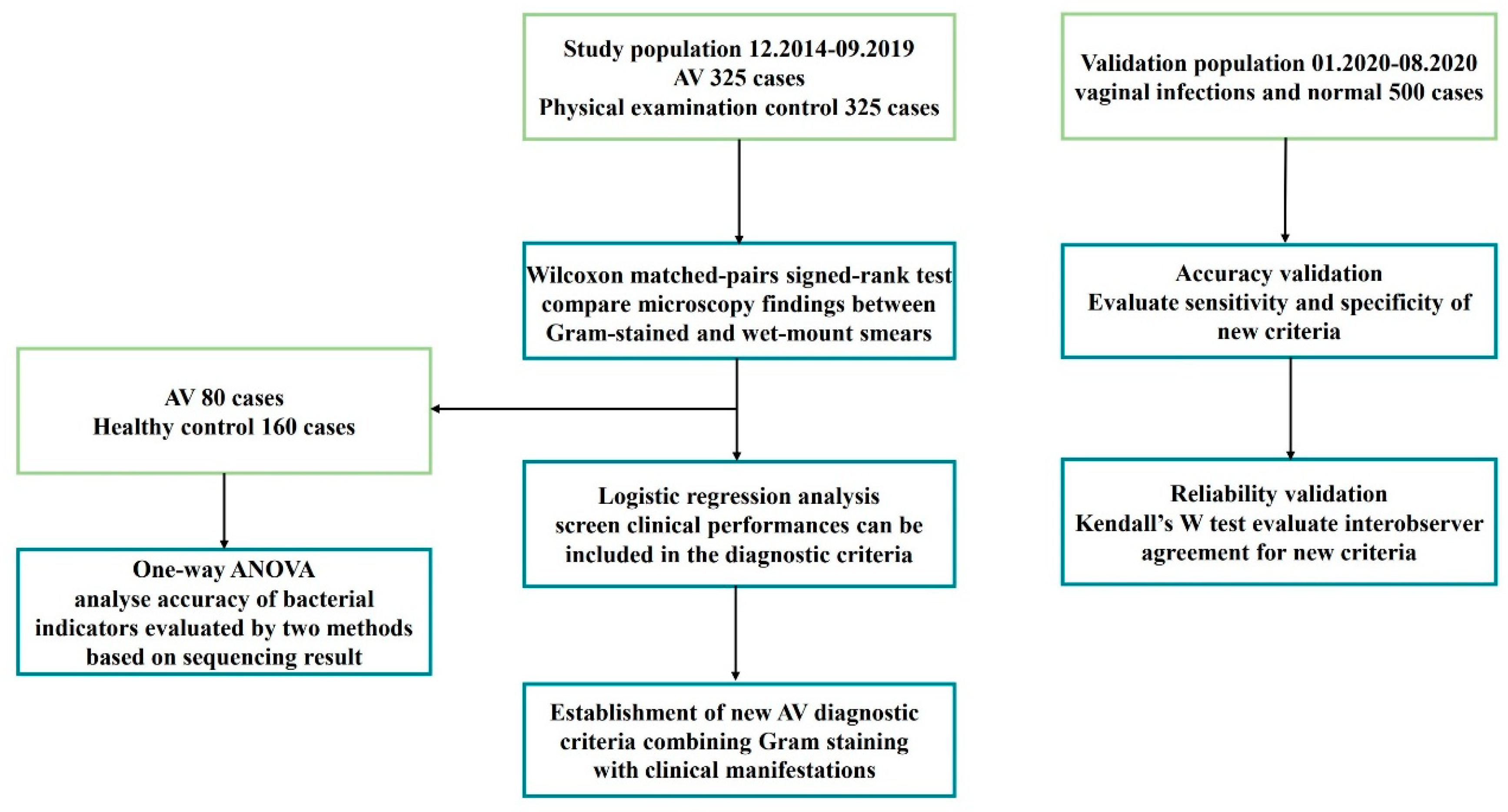
2.1. Study Design and Participants
2.2. Inclusion and Exclusion Criteria
2.3. Clinical History and Sample Collection
2.4. Vaginal Smear Examination
2.5. Diagnostic Criteria
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of the Participants
3.2. Diagnostic Performance of Gram Stain
3.2.1. Comparison of Microscopic Findings from Gram-Stained and Wet-Mount Smears
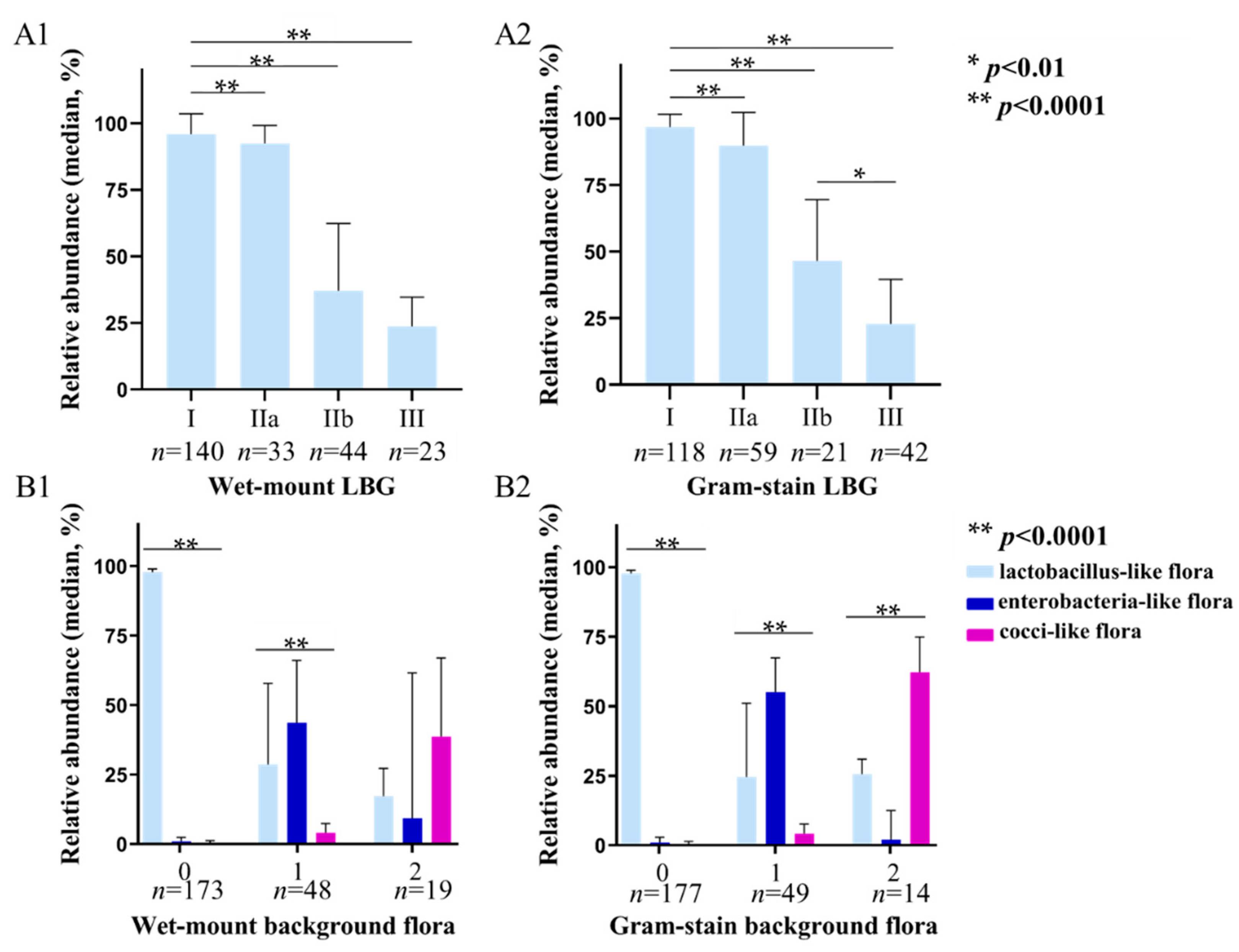
3.2.2. Correlation between Bacterial Indicators Evaluated by Two Methods with 16S rRNA Sequencing
3.3. New AV Diagnostic Criteria
3.3.1. Logistic Analysis for AV Clinical Features
3.3.2. Establishment of New AV Diagnostic Criteria
3.4. Prospective Validation of New AV Diagnostic Criteria
3.4.1. Accuracy of the New AV Diagnostic Criteria
3.4.2. Interobserver Agreement of the New AV Diagnostic Criteria
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donders, G.G.G.; Vereecken, A.; Bosmans, E.; Dekeersmaecker, A.; Salembier, G.; Spitz, B. Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: Aerobic vaginitis. BJOG 2002, 109, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Fan, A.; Yue, Y.; Geng, N.; Zhang, H.; Wang, Y.; Xue, F. Aerobic vaginitis and mixed infections: Comparison of clinical and laboratory findings. Arch. Gynecol. Obstet. 2013, 287, 329–335. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Bellen, G.; Grinceviciene, S.; Ruban, K.; Vieira-Baptista, P. Aerobic vaginitis: No longer a stranger. Res. Microbiol. 2017, 168, 845–858. [Google Scholar] [CrossRef]
- Han, C.; Li, H.; Han, L.; Wang, C.; Yan, Y.; Qi, W.; Fan, A.; Wang, Y.; Xue, F. Aerobic vaginitis in late pregnancy and outcomes of pregnancy. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 233–239. [Google Scholar] [CrossRef]
- Serretiello, E.; Santella, B.; Folliero, V.; Iervolino, D.; Santoro, E.; Manente, R.; Dell’Annunziata, F.; Sperlongano, R.; Crudele, V.; De Filippis, A.; et al. Prevalence and Antibiotic Resistance Profile of Bacterial Pathogens in Aerobic Vaginitis: A Retrospective Study in Italy. Antibiotics 2021, 10, 1133. [Google Scholar] [CrossRef]
- Oerlemans, E.F.M.; Wuyts, S.; Bellen, G.; Wittouck, S.; De Boeck, I.; Ruban, K.; Allonsius, C.N.; van den Broek, M.F.L.; Donders, G.G.G.; Lebeer, S. The Dwindling Microbiota of Aerobic Vaginitis, an Inflammatory State Enriched in Pathobionts with Limited TLR Stimulation. Diagnostics 2020, 10, 879. [Google Scholar] [CrossRef] [PubMed]
- Rumyantseva, T.A.; Bellen, G.; Savochkina, Y.A.; Guschin, A.E.; Donders, G.G.G. Diagnosis of aerobic vaginitis by quantitative real-time PCR. Arch. Gynecol. Obstet. 2016, 294, 109–114. [Google Scholar] [CrossRef]
- Wang, C.; Fan, A.; Li, H.; Yan, Y.; Qi, W.; Wang, Y.; Xue, F. Vaginal bacterial profiles of aerobic vaginitis: A case-control study. Diagn. Microbiol. Infect. Dis. 2020, 96, 114981. [Google Scholar] [CrossRef]
- Oh, K.Y.; Lee, S.; Lee, M.S.; Lee, M.J.; Shim, E.; Hwang, Y.H.; Ha, J.G.; Yang, Y.S.; Hwang, I.T.; Park, J.S. Composition of Vaginal Microbiota in Pregnant Women with Aerobic Vaginitis. Front. Cell. Infect. Microbiol. 2021, 11, 677648. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Van Calsteren, K.; Bellen, G.; Reybrouck, R.; Van den Bosch, T.; Riphagen, I. Predictive value for preterm birth of abnormal vaginal flora, bacterial vaginosis and aerobic vaginitis during the first trimester of pregnancy. BJOG 2009, 116, 1315–1324. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Wu, W.; Fan, A.; Wang, Y.; Zhang, H.; Chu, Z. Diagnostic and therapeutic advancements for aerobic vaginitis. Arch. Gynecol. Obstet. 2015, 291, 251–257. [Google Scholar] [CrossRef]
- Marconi, C.; Donders, G.G.G.; Martin, L.F.; Ramos, B.R.; Duarte, M.T.; Parada, C.M. Chlamydial infection in a high risk population: Association with vaginal flora patterns. Arch. Gynecol. Obstet. 2012, 285, 1013–1018. [Google Scholar] [CrossRef]
- Vieira-Baptista, P.; Lima-Silva, J.; Pinto, C.; Saldanha, C.; Beires, J.; Martinez-de-Oliveira, J.; Donders, G.G.G. Bacterial vaginosis, aerobic vaginitis, vaginal inflammation and major Pap smear abnormalities. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Sherrard, J.; Wilson, J.; Donders, G.G.G.; Mendling, W.; Jensen, J.S. 2018 European (IUSTI/WHO) International Union Against Sexually Transmitted Infections (IUSTI) World Health Organization (WHO) Guideline on the Management of Vaginal Discharge. 2018. Available online: https://journals.sagepub.com/doi/10.1177/0956462418785451 (accessed on 27 July 2018).
- Donders, G.G.G.; Donders, F.; Bellen, G. Screening for abnormal vaginal microflora by self-assessed vaginal pH does not enable detection of sexually transmitted infections in Ugandan women. Diagn. Microbiol. Infect. Dis. 2016, 85, 227–230. [Google Scholar] [CrossRef]
- Larsson, P.G.; Platz-Christensen, J.J. Enumeration of clue cells in rehydrated air-dried vaginal wet smears for the diagnosis of bacterial vaginosis. Obstet. Gynecol. 1990, 76, 727–730. [Google Scholar] [CrossRef]
- Lynch, T.; Peirano, G.; Lloyd, T.; Read, R.; Carter, J.; Chu, A.; Shaman, J.A.; Jarvis, J.P.; Diamond, E.; Ijaz, U.Z.; et al. Molecular Diagnosis of Vaginitis: Comparing Quantitative PCR and Microbiome Profiling Approaches to Current Microscopy Scoring. J. Clin. Microbiol. 2019, 5, e00300-19. [Google Scholar] [CrossRef]
- Tomusiak, A.; Heczko, P.; Janeczko, J.; Adamski, P.; Pilarczyk-Zurek, M.; Strus, M. Bacterial infections of the lower genital tract in fertile and infertile women from the southeastern Poland. Ginekol. Pol. 2013, 84, 352–358. [Google Scholar]
- Blancarte-Lagunas, M.I.; Castro-Escarpulli, G.; Navarro-Ocaña, A.; Ibáñez-Cervantes, G.; Marquez-Valdelamar, L.M.; Hernández-Carrillo, J.M.; Salazar-Salinas, J.; Mendoza-Vásquez, O.F.; Damazo-Hernández, G.; Sosa-Hernández, O.; et al. Commensal and virulent Escherichia coli strains of vaginal origin are reservoirs of resistance cassettes in class 1 integrons. J Infect. Dev. Ctries 2020, 14, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.L.; Fu, L.Y.; Xiong, Z.A.; Qin, Q.; Yu, T.H.; Wu, Y.T. Diagnosis and microecological characteristics of aerobic vaginitis in outpatients based on preformed enzymes. Taiwan. J. Obstet. Gynecol. 2016, 55, 40–44. [Google Scholar] [CrossRef]
- Tempera, G.; Bonfiglio, G.; Cammarata, E.; Corsello, S.; Cianci, A. Microbiological/clinical characteristics and validation of topical therapy with kanamycin in aerobic vaginitis: A pilot study. Int. J. Antimicrob. Agents 2004, 24, 85–88. [Google Scholar] [CrossRef]
- Boccella, M.; Santella, B.; Pagliano, P.; De Filippis, A.; Casolaro, V.; Galdiero, M.; Borrelli, A.; Capunzo, M.; Boccia, G.; Franci, G. Enterococcus Prevalence and Antimicrobial Resistance of Species: A Retrospective Cohort Study in Italy. Antibiotics 2021, 12, 1552. [Google Scholar] [CrossRef]
- Workowski, K.A.; Bolan, G.A. Centers for Disease Control and Prevention, Sexually transmitted diseases treatment guidelines. MMWR Recomm. Rep. 2015, 64, 1–137. [Google Scholar] [CrossRef]
- Søgaard, M.; Nørgaard, M.; Schønheyder, H.J. First notification of positive blood cultures and the high accuracy of the gram stain report. J. Clin. Microbiol. 2007, 45, 1113–1117. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, L.; Zhao, M.; Wang, Y.; Bai, H.; Wang, Y. Deep Neural Networks Offer Morphologic Classification and Diagnosis of Bacterial Vaginosis. J. Clin. Microbiol. 2020, 59. [Google Scholar] [CrossRef]
- Berek, J.S. Berek, & Novak’s Gynecology, 15th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; p. 262. [Google Scholar]
- Holt, G.J.; Krieg, N.R.; Sneath, H.P.; Staley, J.T.; Williams, S.T. Bergey’s Manual of Determinative Bacteriology, 9th ed.; Williams & Wilkins: Philadelphia, PA, USA, 1994. [Google Scholar]
- Sonthalia, S.; Aggarwal, P.; Das, S.; Sharma, P.; Sharma, R.; Singh, S. Aerobic vaginitis—An underdiagnosed cause of vaginal discharge—Narrative review. Int. J. STD AIDS 2020, 1018–1027. [Google Scholar] [CrossRef]
- Redelinghuys, M.J.; Ehlers, M.M.; Dreyer, A.W.; Kock, M.M. Normal flora and bacterial vaginosis in pregnancy: An overview. Crit. Rev. Microbiol. 2016, 42, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G.; Gonzaga, A.; Marconi, C.; Donders, F.; Michiels, T.; Eggermont, N. Increased vaginal pH in Ugandan women: What does it indicate? Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1297–1303. [Google Scholar] [CrossRef][Green Version]
- Clinical & Laboratory Standards Institute (CLSI). Abbreviated Identification of Bacteria and Yeast; Approved Guideline—Second Edition. 24 November 2008. Available online: https://www.clsi.org/standards/products/microbiology/documents/m35/ (accessed on 24 November 2008).
- Mason, M.J.; Winter, A.J. How to diagnose and treat aerobic and desquamative inflammatory vaginitis. Sex. Transm. Infect. 2017, 93, 8–10. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Vereecken, A.; Salembier, G.; Van Bulck, B.; Spitz, B. Assessment of vaginal lactobacillary flora in wet mount and fresh or delayed gram’s stain. Infect. Dis. Obstet. Gynecol. 1996, 4, 2–6. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Vereecken, A.; Dekeersmaecker, A.; Van Bulck, B.; Spitz, B. Wet mount microscopy reflects functional vaginal lactobacillary flora better than Gram stain. J. Clin. Pathol. 2000, 53, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G. Wet smear compared with Gram stain diagnosis in asymptomatic pregnant women. Obstet. Gynecol. 2001, 97, 482. [Google Scholar] [PubMed]
- Kim, H.; Kim, T.; Kang, J.; Kim, Y.; Kim, H. Is Lactobacillus Gram-Positive? A Case Study of lactobacillus iners. Microorganisms 2020, 7, 969. [Google Scholar] [CrossRef] [PubMed]
- Ozyurt, E.; Toykuliyeva, M.; Danilyans, I.; Morton, O.; Baktir, G. Efficacy of 7-day treatment with metronidazole + miconazole (Neo-Penotran)—A triple-active pessary for the treatment of single and mixed vaginal infections. Int. J. Gynaecol. Obstet. 2001, 74, 35–43. [Google Scholar] [CrossRef]
- Smith, K.; Kirby, J. Image analysis and artificial intelligence in infectious disease diagnostics. Clin. Microbiol. Infect. 2020, 26, 1318–1323. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| AV Related Microscopic Findings | Wet-Mount Smear (400×) n (%) | Gram-Stained Smear (400×) n (%) | Z *,# | p *,# | Wet-Mount Smear(400×) n (%) | Gram-Stained Smear (1000×) n (%) | Z **,# | p **,# |
|---|---|---|---|---|---|---|---|---|
| Leukocyte counts | 11.8 (3.20, 26.95) | 12.0 (2.83, 28.97) | −1.43 | 0.15 | ||||
| Toxic leukocyte/ Leukocyte ratio | 0.00% (0.00%, 33.83%) | - | - | - | ||||
| PBC ratio | 0.00% (0.00%, 0.00%) | 0.00% (0.00%, 0.00%) | −0.15 | 0.88 | ||||
| LBG score | −2.23 | 0.03 | −1.60 | 0.11 | ||||
| 0 (I, IIa) | 282 (43.38) | 293 (45.08) | 282 (43.38) | 288 (44.31) | ||||
| 1 (IIb) | 145 (22.31) | 58 (8.92) | 145 (22.31) | 83 (12.77) | ||||
| 2 (III) | 223 (34.31) | 299 (46.00) | 223 (34.31) | 279 (42.92) | ||||
| Background flora score | −2.05 | 0.04 | −1.19 | 0.23 | ||||
| 0 (No other bacteria) | 316 (48.62) | 326 (50.15) | 316 (48.62) | 327 (50.31) | ||||
| 1 (Small coliform bacilli) | 254 (39.08) | 278 (42.77) | 254 (39.08) | 262 (40.31) | ||||
| 2 (Cocci or chains) | 80 (12.31) | 46 (7.08) | 80 (12.31) | 61 (9.38) |
| Clinical Manifestations | Univariate Logistic Regression Analysis | Multivariate Logistic Regression Analysis | ||
|---|---|---|---|---|
| p | OR (95% CI) | p | OR (95% CI) | |
| Vulvovaginal itching | ||||
| no | ||||
| yes | <0.0001 | 4.651 (3.040−7.143) | 0.066 | 2.091 (0.952−4.593) |
| Vaginal dyspareunia | ||||
| no | ||||
| yes | 0.001 | 11.905 (4.219−33.333) | 0.153 | 3.388 (0.635−18.072) |
| Increased vaginal discharge | ||||
| no | ||||
| yes | <0.0001 | 5.348 (3.817−7.519) | 0.064 | 1.878 (0.964−3.662) |
| Yellow discharge | ||||
| no | ||||
| yes | <0.0001 | 26.316 (11.364−62.500) | <0.0001 | 10.189 (2.907−35.714) |
| Vaginal hyperemia | ||||
| no | ||||
| yes | <0.0001 | 16.129 (9.901−26.316) | <0.0001 | 5.092 (2.269−11.427) |
| pH value | ||||
| ≤4.5 | ||||
| >4.5 | <0.0001 | 14.925 (10.204−22.222) | <0.0001 | 6.542 (3.421−12.509) |
| Score | LBG (1000×) | No. of Leukocytes (400×) | Background Flora (1000×) | Proportion of PBC (400×) | Clinical Manifestation |
|---|---|---|---|---|---|
| 0 | I, IIa | ≤10/hpf | No other bacteria | <1% | pH ≤ 4.5 and no abnormal signs # |
| 1 | IIb | >10/hpf and ≤10/epithelial cells | Small coliform bacilli | ≥1% and ≤10% | pH > 4.5 or at least one of abnormal signs # |
| 2 | III | >10/epithelial cells | Cocci or chains | >10% | pH > 4.5 and at least one of abnormal signs # |
| New Criteria AV | Wet-Mount Simple AV | Total | Sensitivity (%) | Specificity (%) | Youden Index | Wet-Mount Simple and Mixed AV | Total | Sensitivity (%) | Specificity (%) | Youden Index | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | |||||||||
| Yes | 46 | 12 | 58 | 86.79 | 95.97 | 0.828 | 93 | 20 | 113 | 82.30 | 94.83 | 0.771 |
| No | 7 | 286 | 293 | 20 | 367 | 387 | ||||||
| Total | 53 | 298 | 351 | 113 | 387 | 500 | ||||||
| Indicators | New Diagnostic Criteria KW Value | Wet-Mount Diagnostic Criteria KW Value |
|---|---|---|
| LBG | 0.876 | 0.828 |
| Background flora | 0.713 | 0.603 |
| No. of leukocytes | 0.778 | 0.771 |
| PBC proportion | 0.544 | 0.544 |
| AV score | 0.899 | 0.811 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, M.; Wang, C.; Li, H.; Yan, Y.; Ma, X.; Li, H.; Li, X.; Wang, H.; Zhang, Y.; Qi, W.; et al. Aerobic Vaginitis Diagnosis Criteria Combining Gram Stain with Clinical Features: An Establishment and Prospective Validation Study. Diagnostics 2022, 12, 185. https://doi.org/10.3390/diagnostics12010185
Dong M, Wang C, Li H, Yan Y, Ma X, Li H, Li X, Wang H, Zhang Y, Qi W, et al. Aerobic Vaginitis Diagnosis Criteria Combining Gram Stain with Clinical Features: An Establishment and Prospective Validation Study. Diagnostics. 2022; 12(1):185. https://doi.org/10.3390/diagnostics12010185
Chicago/Turabian StyleDong, Mengting, Chen Wang, Huiyang Li, Ye Yan, Xiaotong Ma, Huanrong Li, Xingshuo Li, Huihui Wang, Yixuan Zhang, Wenhui Qi, and et al. 2022. "Aerobic Vaginitis Diagnosis Criteria Combining Gram Stain with Clinical Features: An Establishment and Prospective Validation Study" Diagnostics 12, no. 1: 185. https://doi.org/10.3390/diagnostics12010185
APA StyleDong, M., Wang, C., Li, H., Yan, Y., Ma, X., Li, H., Li, X., Wang, H., Zhang, Y., Qi, W., Meng, K., Tian, W., Wang, Y., Fan, A., Han, C., Donders, G. G. G., & Xue, F. (2022). Aerobic Vaginitis Diagnosis Criteria Combining Gram Stain with Clinical Features: An Establishment and Prospective Validation Study. Diagnostics, 12(1), 185. https://doi.org/10.3390/diagnostics12010185