
High Sensitivity C Reactive Protein in Patients with Rheumatoid Arthritis Treated with Antibodies against IL-6 or Jak Inhibitors: A Clinical and Ultrasonographic Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Measurement of Clinical Disease Activity and Assessment of Blood Biomarkers
2.3. Imaging Biomarkers: Ultrasound Score
2.4. Statistical Analysis
3. Results
3.1. Demographic, Clinical, and Therapeutic Characteristics
3.2. Correlation between hsCRP and Disease Activity
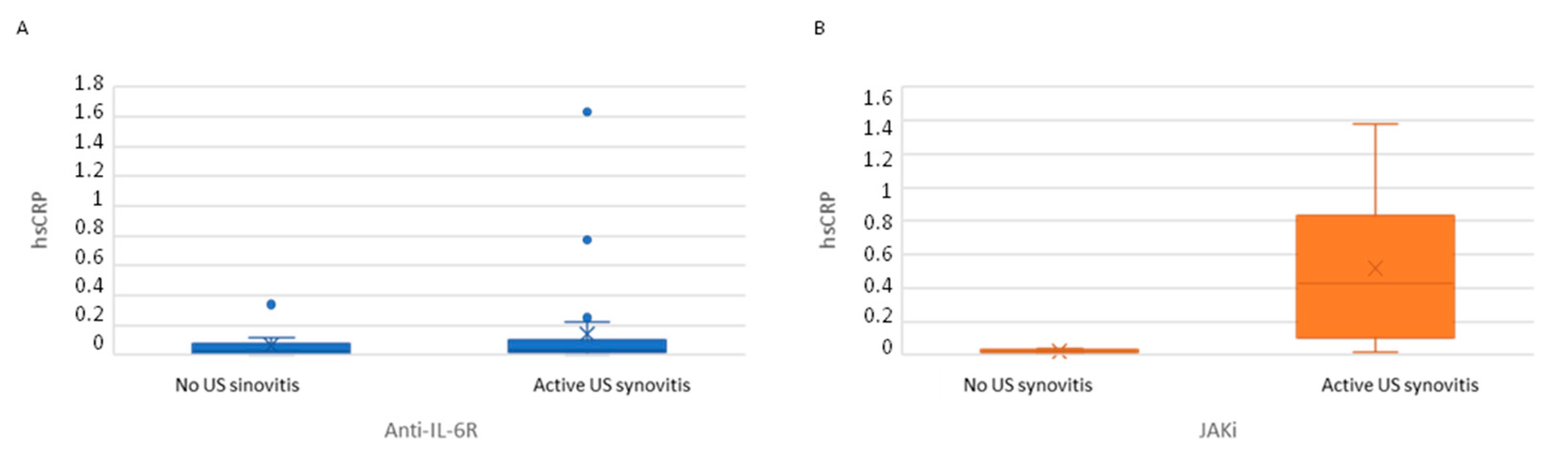
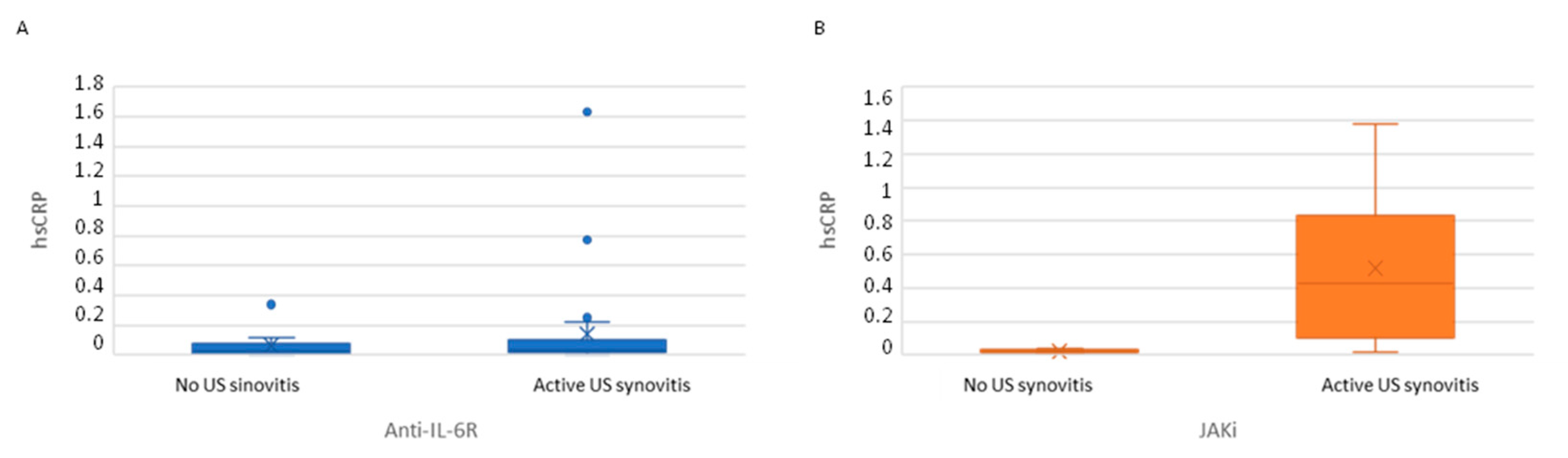
3.3. hsCRP Serum Levels in Patients with and without Ultrasound Synovitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- England, B.R.; Tiong, B.K.; Bergman, M.J.; Curtis, J.R.; Kazi, S.; Mikuls, T.R.; O’Dell, J.R.; Ranganath, V.K.; Limanni, A.; Suter, L.G.; et al. 2019 Update of the American College of Rheumatology Recommended Rheumatoid Arthritis Disease Activity Measures. Arthritis Care Res. 2019, 71, 1540–1555. [Google Scholar] [CrossRef]
- Pope, J.E.; Choy, E.H. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. Semin. Arthritis Rheum. 2021, 51, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Brahe, C.H.; Østergaard, M.; Lund Hetland, M.; Hambardzumyan, K.; Saevarsdottir, S.; Wang, X.; Flake Ii, D.D.; Sasso, E.H.; Huizinga, T.W. Predicting risk for radiographic damage in rheumatoid arthritis: Comparative analysis of the multi-biomarker disease activity score and conventional measures of disease activity in multiple studies. Curr. Med. Res. Opin. 2019, 35, 1483–1493. [Google Scholar] [CrossRef] [Green Version]
- Jansen, L.M.; van der Horst-Bruinsma, I.E.; van Schaardenburg, D.; Bezemer, P.D.; Dijkmans, B.A.C. Predictors of radiographic joint damage in patients with early rheumatoid arthritis. Ann. Rheum. Dis. 2001, 60, 924–927. [Google Scholar] [CrossRef] [Green Version]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, S685–S699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smolen, J.S.; Aletaha, D. Interleukin-6 receptor inhibition with tocilizumab and attainment of disease remission in rheumatoid arthritis: The role of acute-phase reactants. Arthritis Rheum. 2011, 63, 43–52. [Google Scholar] [CrossRef]
- Asai, S.; Takahashi, N.; Kobayakawa, T.; Kaneko, A.; Watanabe, T.; Kato, T.; Nishiume, T.; Ishikawa, H.; Yoshioka, Y.; Kanayama, Y.; et al. Comparison of the effects of baricitinib and tocilizumab on disease activity in patients with rheumatoid arthritis: A propensity score matching analysis. Clin. Rheumatol. 2021, 40, 3143–3151. [Google Scholar] [CrossRef]
- Joshua, F.; Edmonds, J.; Lassere, M. Power Doppler Ultrasound in Musculoskeletal Disease: A Systematic Review. Semin. Arthritis Rheum. 2006, 36, 99–108. [Google Scholar] [CrossRef]
- Brown, A.K.; Quinn, M.A.; Karim, Z.; Conaghan, P.; Peterfy, C.G.; Hensor, E.; Wakefield, R.J.; O’Connor, P.J.; Emery, P. Presence of significant synovitis in rheumatoid arthritis patients with disease-modifying antirheumatic drug–induced clinical remission: Evidence from an imaging study may explain structural progression. Arthritis Rheum. 2006, 54, 3761–3773. [Google Scholar] [CrossRef]
- Scirè, C.A.; Montecucco, C.; Codullo, V.; Epis, O.; Todoerti, M.; Caporali, R.F. Ultrasonographic evaluation of joint involvement in early rheumatoid arthritis in clinical remission: Power Doppler signal predicts short-term relapse. Rheumatology 2009, 48, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., III; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Backhaus, M.; Burmester, G.-R.; Gerber, T.; Grassi, W.; Machold, K.; Swen, W.A.; Wakefield, R.J.; Manger, B.; Working Group for Musculoskeletal Ultrasound in the EULAR Standing Committee on International Clinical Studies including Therapeutic Trials. Guidelines for musculoskeletal ultrasound in rheumatology. Ann. Rheum. Dis. 2001, 60, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, R.J.; Balint, P.V.; Szkudlarek, M.; Filippucci, E.; Backhaus, M.; D’Agostino, M.A.; Sanchez, E.N.; Iagnocco, A.; Schmidt, W.A.; Bruyn, G.A.; et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J. Rheumatol. 2006, 33, 440. [Google Scholar]
- Szkudlarek, M.; Court-Payen, M.; Jacobsen, S.; Klarlund, M.; Thomsen, H.S.; Østergaard, M. Interobserver agreement in ultrasonography of the finger and toe joints in rheumatoid arthritis. Arthritis Rheum. 2003, 48, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, J.; Ruíz-Esquide, V.; Pomés, I.; Celis, R.; Cuervo, A.; Hernández, M.V.; Pomés, J.; Pablos, J.L.; Sanmartí, R.; Cañete, J.D. Patients with rheumatoid arthritis in clinical remission and ultrasound-defined active synovitis exhibit higher disease activity and increased serum levels of angiogenic biomarkers. Arthritis Res. Ther. 2014, 16, R5. [Google Scholar] [CrossRef] [Green Version]
- Smolen, J.S.; Aletaha, D.; Gruben, D.; Zwillich, S.H.; Krishnaswami, S.; Mebus, C. Brief Report: Remission Rates With Tofacitinib Treatment in Rheumatoid Arthritis: A Comparison of Various Remission Criteria. Arthritis Rheumatol. 2017, 69, 728–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dejaco, C.; Duftner, C.; Wipfler-Freißmuth, E.; Weiss, H.; Graninger, W.B.; Schirmer, M. Ultrasound-Defined Remission and Active Disease in Rheumatoid Arthritis: Association with Clinical and Serologic Parameters. Semin. Arthritis Rheum. 2012, 41, 761–767. [Google Scholar] [CrossRef]
- Hammer, H.B.; Ødegård, S.; Syversen, S.W.; Landewé, R.; van der Heijde, D.; Uhlig, T.; Mowinckel, P.; Kvien, T.K. Calprotectin (a major S100 leucocyte protein) predicts 10-year radiographic progression in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2008, 69, 150–154. [Google Scholar] [CrossRef]
- Kim, S.K.; Jung, U.H.; Kim, J.W.; Choe, J.Y. The beneficial effect of baricitinib on ultrasound-detected synovial inflammation and bone damage in rheumatoid arthritis: Preliminarily data from single center-based observational study for 24 weeks. Medicine 2021, 100, e26739. [Google Scholar] [CrossRef]
- Nishimoto, N.; Yoshizaki, K.; Maeda, K.; Kuritani, T.; Deguchi, H.; Sato, B.; Imai, N.; Suemura, M.; Kakehi, T.; Takagi, N.; et al. Toxicity, pharmacokinetics, and dose-finding study of repetitive treatment with the humanized anti-interleukin 6 receptor antibody MRA in rheumatoid arthritis. Phase I/II clinical study. J. Rheumatol. 2003, 30, 1426–1435. [Google Scholar] [PubMed]
- Choy, E.H.S.; Isenberg, D.; Garrood, T.; Farrow, S.; Ioannou, Y.; Bird, H.; Cheung, N.; Williams, B.; Hazleman, B.; Price, R.; et al. Therapeutic benefit of blocking interleukin-6 activity with an anti-interleukin-6 receptor monoclonal antibody in rheumatoid arthritis: A randomized, double-blind, placebo-controlled, dose-escalation trial. Arthritis Care Res. 2002, 46, 3143–3150. [Google Scholar] [CrossRef]
- Schoels, M.; Alasti, F.; Smolen, J.S.; Aletaha, D. Evaluation of newly proposed remission cut-points for disease activity score in 28 joints (DAS28) in rheumatoid arthritis patients upon IL-6 pathway inhibition. Arthritis Res. Ther. 2017, 19, 155. [Google Scholar] [CrossRef] [Green Version]
- Shafran, I.H.; Alasti, F.; Smolen, J.S.; Aletaha, D. Implication of baseline levels and early changes of C-reactive protein for subsequent clinical outcomes of patients with rheumatoid arthritis treated with tocilizumab. Ann. Rheum. Dis. 2020, 79, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Inciarte-Mundo, J.; Ruiz-Esquide, V.; Hernández, M.V.; Cañete, J.D.; Cabrera-Villalba, S.R.; Ramirez, J.; Yagüe, J.; Sanmarti, R. Calprotectin more accurately discriminates the disease status of rheumatoid arthritis patients receiving tocilizumab than acute phase reactants. Rheumatology 2015, 54, 2239–2243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, M.; Serada, S.; Suzuki, K.; Nishikawa, A.; Ogata, A.; Nanki, T.; Hattori, K.; Kohsaka, H.; Miyasaka, N.; Takeuchi, T.; et al. Brief Report: Leucine-Rich α2-Glycoprotein as a Potential Biomarker for Joint Inflammation During Anti-Interleukin-6 Biologic Therapy in Rheumatoid Arthritis. Arthritis Rheumatol. 2015, 67, 2056–2060. [Google Scholar] [CrossRef]
- Murdaca, G.; Spanò, F.; Contatore, M.; Guastalla, A.; Magnani, O.; Puppo, F. Pharmacogenetics of etanercept: Role of TNF-α gene polymorphisms in improving its efficacy. Expert Opin. Drug Metab. Toxicol. 2014, 10, 1703–1710. [Google Scholar] [CrossRef] [PubMed]
- Maldonado-Montoro, M.; Cañadas-Garre, M.; González-Utrilla, A.; Plaza-Plaza, J.C.; Calleja-Hernández, M.Ÿ. Genetic and clinical biomarkers of tocilizumab response in patients with rheumatoid arthritis. Pharmacol. Res. 2016, 111, 264–271. [Google Scholar] [CrossRef]

{kind=link}
| Anti-IL-6R (n = 42) | JAKi (n = 21) | p-Value | |
|---|---|---|---|
| DEMOGRAPHIC VARIABLES | |||
| Age | 59.9 (34.0–79.4) | 52.4 (26.4–84.7) | 0.145 |
| Female, n (%) | 39 (92.9) | 19 (90.5) | 1 |
| CCP, n (%) | 34 (91.9) | 19 (95.0) | 1 |
| FR, n (%) | 31 (83.8) | 17 (85.0) | 1 |
| Erosive disease, n (%) | 34 (81.0) | 13 (61.9) | 0.102 |
| Disease duration (years) | 15.7 (3.47–37.5) | 12.09 (0.2–34.3) | 0.040 |
| Previous biologic treatments | 1 (0–4) | 1 (0–7) | 0.89 |
| Patients with previous biologic treatment, n (%) | 25 (58.5) | 11 (52.4) | 0.65 |
| CONCOMITANT TREATMENT | |||
| Treatment duration (months) | 43.8 (7.9–139.9) | 9.9 (2.9–77.7) | <0.001 |
| prednisone, n (%) | 17 (40.5) | 12 (57.1) | 0.211 |
| Prednisone equivalent dose (mg/day) | 2.5 (1.25–10) | 5 (1.25–10) | 0.586 |
| NSAID treatment, n (%) | 13 (31.0) | 2 (9.5) | 0.60 |
| CsDMARD treatment, n (%) | 18 (42.9) | 11 (52.4) | 0.475 |
| Anti-IL-6R (n = 42) | JAKi (n = 21) | p-Value | |
|---|---|---|---|
| 28TJC | 2 (0–20) | 3 (0.25) | 0.591 |
| 28SJC | 1 (0–7) | 1 (0–9) | 0.580 |
| PGA | 4 (0–8.5) | 4 (0–7.5) | 0.321 |
| PhGA | 3 (0–7) | 3 (0–7) | 0.111 |
| VAS pain | 3 (0–8) | 4 (0–7.5) | 0.433 |
| DAS28 | 2.349 (0.970–5.06) | 3.439 (1.502–7.294) | 0.002 |
| CDAI | 8.5 (0–31) | 13 (0–41) | 0.240 |
| SDAI | 8.9 (0.40–31.40) | 13.40 (0.40–42.91) | 0.231 |
| HAQ | 0.88 (0.0–2.88) | 0.75 (0.0–2.275) | 0.421 |
| Rapid3 | 8.6 (0–25.50) | 9.0 (1–18) | 0.560 |
| LABORATORY TESTS | |||
| hsCRP mg/dL | 0.04 (0.0–1.63) | 0.16 (0.01–1.38) | 0.007 |
| ESR | 5 (2–14) | 16 (6–140) | <0.001 |
| Hemoglobin g/L | 143 (100–168) | 125 (100–148) | <0.001 |
| ULTRASOUND INDICES | |||
| SH score | 4 (0–18) | 4 (0–28) | 0.352 |
| PD score | 3.5 (0–18) | 3 (0–27) | 0.825 |
| Global score | 8 (0–35) | 7 (0–55) | 0.534 |
| Anti-IL-6R (n = 42) | JAKi (n = 21) | Total (n = 63) | ||||
|---|---|---|---|---|---|---|
| Rho | p-Value | Rho | p-Value | Rho | p-Value | |
| 28TJC28 | −0.087 | 0.587 | 0.094 | 0.0684 | −0.038 | 0.768 |
| 28SJC | −0.25 | 0.876 | 0.045 | 0.06 | 0.203 | 0.113 |
| PGA | −0.191 | 0.876 | −0.019 | 0.933 | −0.070 | 0.590 |
| PhGA | −0.171 | 0.298 | 0.376 | 0.093 | 0.117 | 0.369 |
| Pain | −0.056 | 0.730 | 0.069 | 0.767 | 0.003 | 0.981 |
| CDAI | −0.142 | 0.374 | 0.247 | 0.280 | 0.054 | 0.679 |
| SDAI | −1.36 | 0.395 | 0.247 | 0.280 | 0.066 | 0.609 |
| DAS28 | −0.141 | 0.379 | 0.330 | 0.144 | 0.148 | 0.252 |
| HAQ | 0.12 | 0.938 | 0.270 | 0.236 | 0.065 | 0.613 |
| Rapid3 | −0.258 | 0.103 | −0.005 | 0.984 | −0.133 | 0.304 |
| HS score | 0.156 | 0.324 | 0.402 | 0.071 | 0.296 * | 0.019 |
| PD score | 0.077 | 0.627 | 0.544 * | 0.011 | 0.275 * | 0.029 |
| HD + PD score | 0.138 | 0.385 | 0.533 * | 0.013 | 0.296 * | 0.018 |
| Anti-IL-6R (n = 42) | JAKi (n = 21) | |||||
|---|---|---|---|---|---|---|
| No Active US Synovitis (n = 12) | Active US Synovitis (n = 30) | p-Value | No Active US Synovitis (n = 5) | Active US Synovitis (n = 16) | p-Value | |
| 28TJC | 0.5 (0–15) | 2 (0–20) | 0.153 | 3 (0–9) | 1.5 (0–25) | 0.398 |
| 28SJC | 0 (0–1) | 1 (0–7) | <0.001 | 0 (0–1) | 2 (0–9) | 0.075 |
| PGA | 3 (0–8.5) | 4 (0–6) | 0.773 | 2.5 (2–7) | 4.75 (0–7.5) | 0.398 |
| PhGA | 1 (0–4) | 3 (0–7) | 0.017 | 1 (0–3) | 4 (0–7) | 0.011 |
| DAS28 | 2.074 (0.97–4.827) | 2.537 (0.970–5.064) | 0.146 | 3.216 (1.534–4.787) | 3.780 (1.502–7.293) | 0.313 |
| CDAI | 6.5 (0–25) | 10 (0–31) | 0.052 | 6 (3–20) | 14 (0–41) | 0.313 |
| SDAI | 6.9 (0.4–25.4) | 10.40 (0.40–31.40) | 0.052 | 6.4 (3.4–20.4) | 14.475 (0.40–42.91) | 0.313 |
| hsPCR mg/dL | 0.03 (0–0.34) | 0.04 (0–1.63) | 0.417 | 0.02 (0.01–0.04) | 0.42 (0.02–1.38) | 0.001 |
| ESR | 5 (3–14) | 5.50 (2–14) | 0.923 | 14 (6–15) | 20.50 (7–140) | 0.062 |
| ULTRASOUND INDICES | ||||||
| SH score | 0 (0–2) | 6 (2–18) | <0.001 | 2 (0–3) | 6.5 (2–28) | 0.002 |
| PD score | 0 (0–1) | 4 (1–18) | <0.001 | 0 (0–0) | 5 (1–27) | <0.001 |
| Global score | 0 (0–2) | 10 (3–35) | <0.001 | 2 (0–3) | 12.5 (4–55) | <0.001 |
| Anti-IL-6R (n = 42) | JAKi (n = 21) | |||||
|---|---|---|---|---|---|---|
| CDAI ≤ 10 n = 25 | CDAI > 10 n = 17 | p Value | CDAI ≤ 10 n = 8 | CDAI > 10 n = 13 | p Value | |
| hs-PCRP mg/dL | 0.035 (0.0–0.77) | 0.04 (0.0–1.63) | 0.38 | 0.09 (0.01–1.08) | 0.34 (0.02–1.38) | 0.57 |
| Hs-CRP ≥ 0.1 mg/dL | 4 (16) | 4 (23) | 0.51 | 4 (50) | 8 (61.5) | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frade-Sosa, B.; Ponce, A.; Ruiz-Esquide, V.; García-Yébenes, M.J.; Morlá, R.; Sapena, N.; Ramirez, J.; Azuaga, A.B.; Sarmiento, J.C.; Cañete, J.D.; et al. High Sensitivity C Reactive Protein in Patients with Rheumatoid Arthritis Treated with Antibodies against IL-6 or Jak Inhibitors: A Clinical and Ultrasonographic Study. Diagnostics 2022, 12, 182. https://doi.org/10.3390/diagnostics12010182
Frade-Sosa B, Ponce A, Ruiz-Esquide V, García-Yébenes MJ, Morlá R, Sapena N, Ramirez J, Azuaga AB, Sarmiento JC, Cañete JD, et al. High Sensitivity C Reactive Protein in Patients with Rheumatoid Arthritis Treated with Antibodies against IL-6 or Jak Inhibitors: A Clinical and Ultrasonographic Study. Diagnostics. 2022; 12(1):182. https://doi.org/10.3390/diagnostics12010182
Chicago/Turabian StyleFrade-Sosa, Beatriz, Andrés Ponce, Virginia Ruiz-Esquide, Maria Jesús García-Yébenes, Rosa Morlá, Nuria Sapena, Julio Ramirez, Ana Belen Azuaga, Juan Camilo Sarmiento, Juan D. Cañete, and et al. 2022. "High Sensitivity C Reactive Protein in Patients with Rheumatoid Arthritis Treated with Antibodies against IL-6 or Jak Inhibitors: A Clinical and Ultrasonographic Study" Diagnostics 12, no. 1: 182. https://doi.org/10.3390/diagnostics12010182
APA StyleFrade-Sosa, B., Ponce, A., Ruiz-Esquide, V., García-Yébenes, M. J., Morlá, R., Sapena, N., Ramirez, J., Azuaga, A. B., Sarmiento, J. C., Cañete, J. D., Gomez-Puerta, J. A., & Sanmarti, R. (2022). High Sensitivity C Reactive Protein in Patients with Rheumatoid Arthritis Treated with Antibodies against IL-6 or Jak Inhibitors: A Clinical and Ultrasonographic Study. Diagnostics, 12(1), 182. https://doi.org/10.3390/diagnostics12010182