
Brain Tumor Detection and Classification on MR Images by a Deep Wavelet Auto-Encoder Model

 , ,
, ,
Abstract
:1. Introduction
2. Related Work
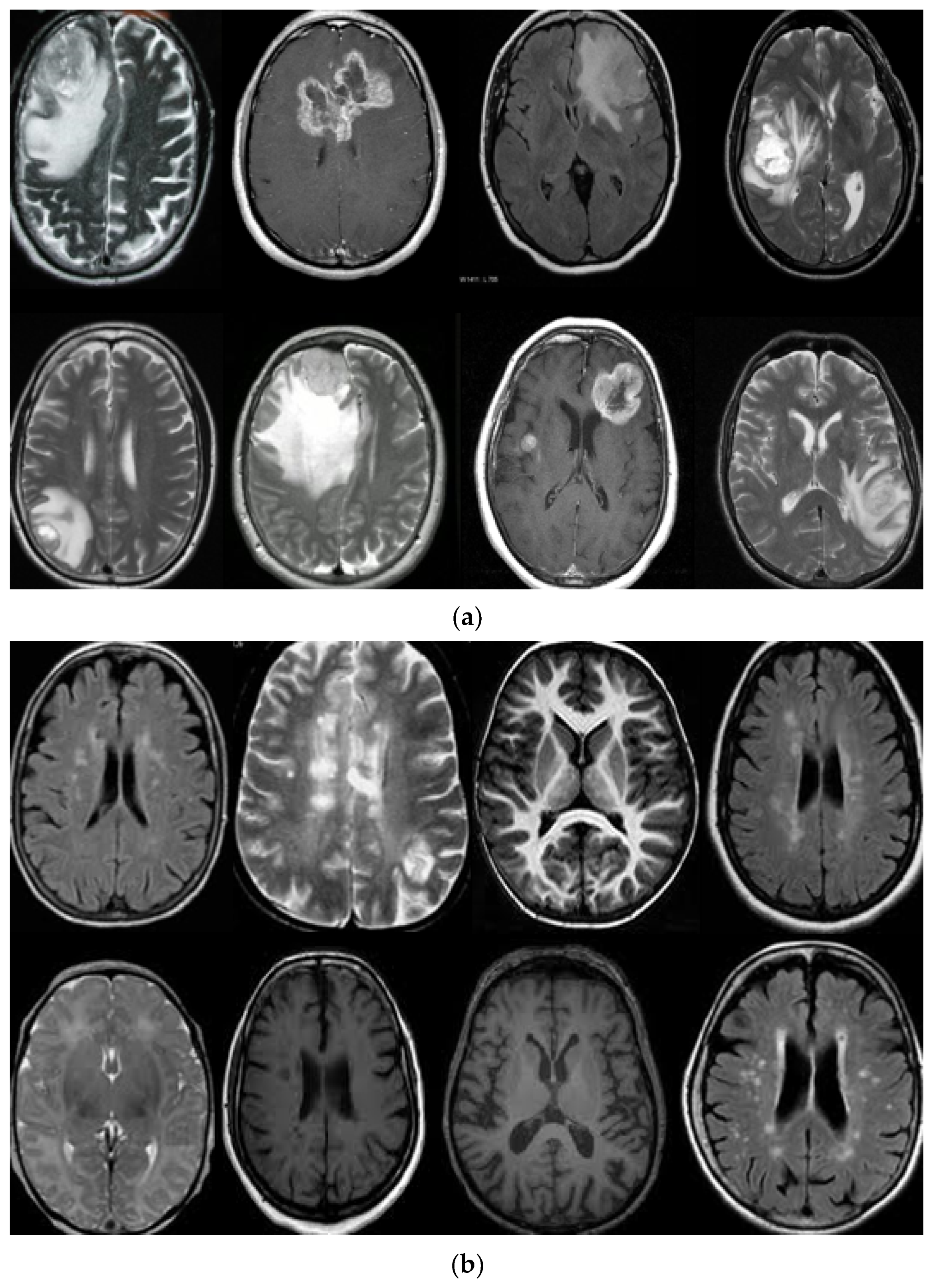
3. Datasets
4. Methodology
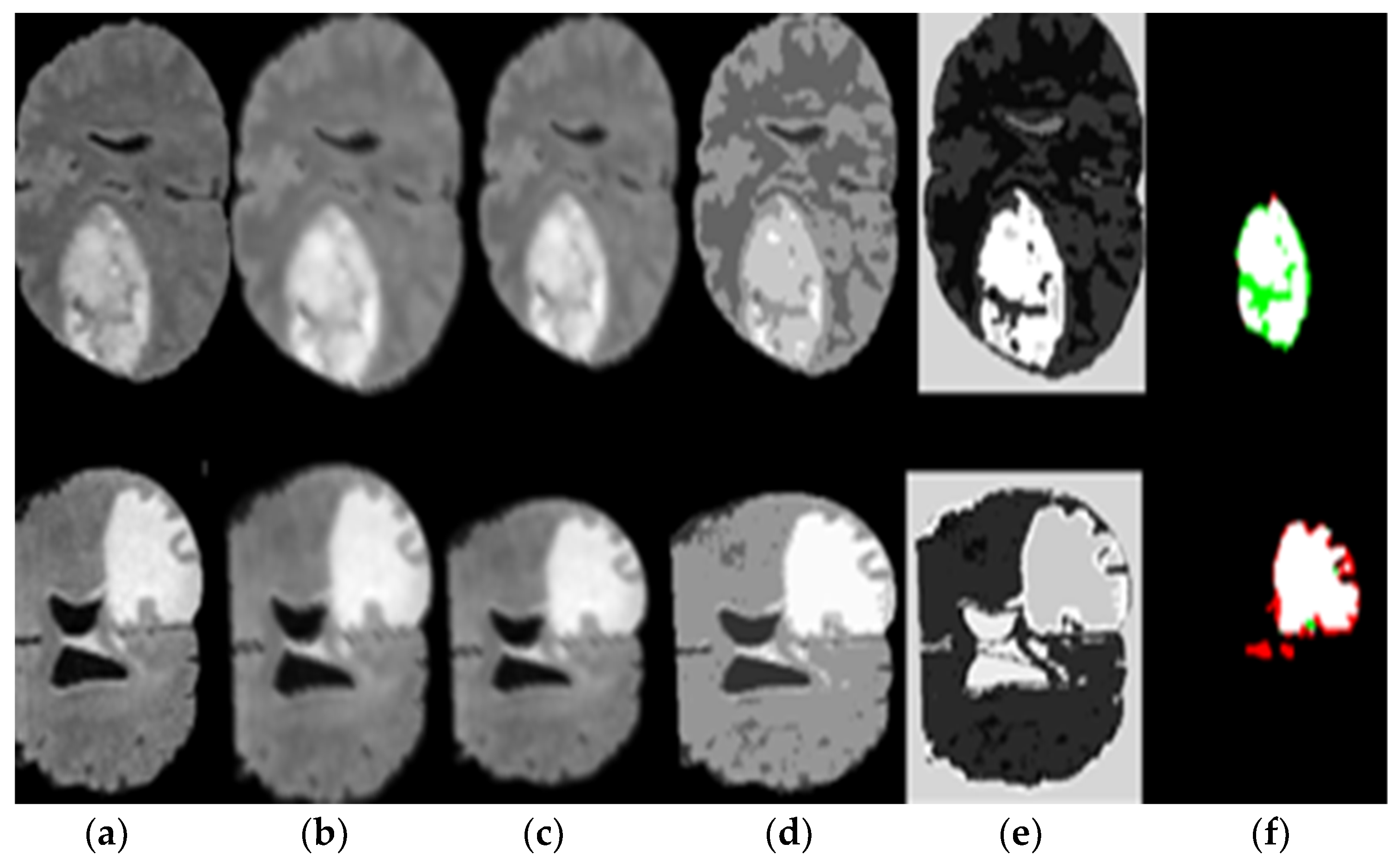
- The pre-processing stage is through an enhancement filter, to improve the image; we introduce a new fusion method. In this step, the input MR brain images were resized by 256 × 256 × 1. Then, we choose a high pass filter to improve the edges of the input MR brain image. The input and output of the MR brain image are fused serially. Finally, a combined, fused MR brain image is smoothed using a 3 × 3 median filter that gives the excellent effect of segmentation results compared with previous models.
- We applied a seed-growing algorithm based on the optimal threshold for good segmentation for a brain tumor.
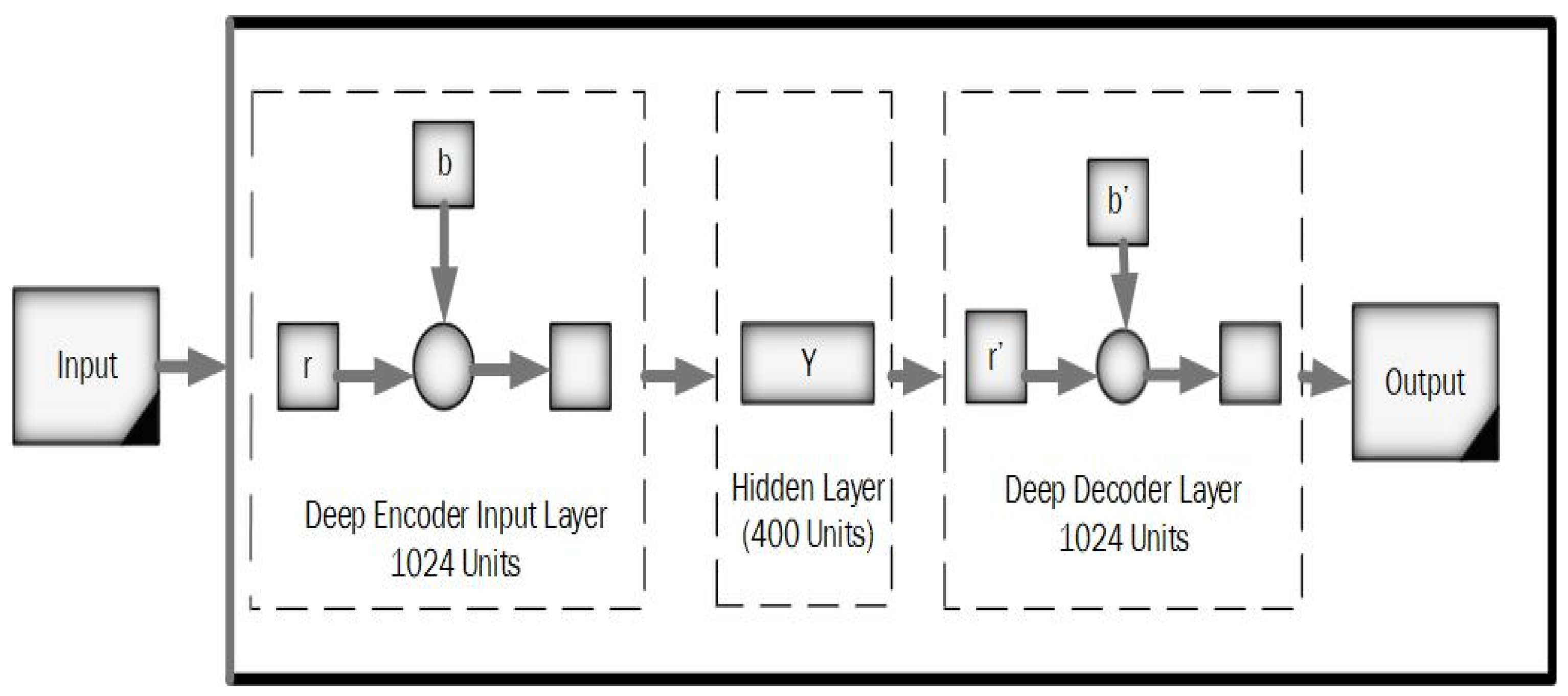
- In classification, we applied a deep wavelet auto-encoder (DWAE) model. In this stage, the segmented MR brain image is resized by 256 × 256 × 1 dimension for faster processing. The objective of this stage is to predict the slices with tumor (abnormal MR brain images and the slices without tumor (normal MR brain images).
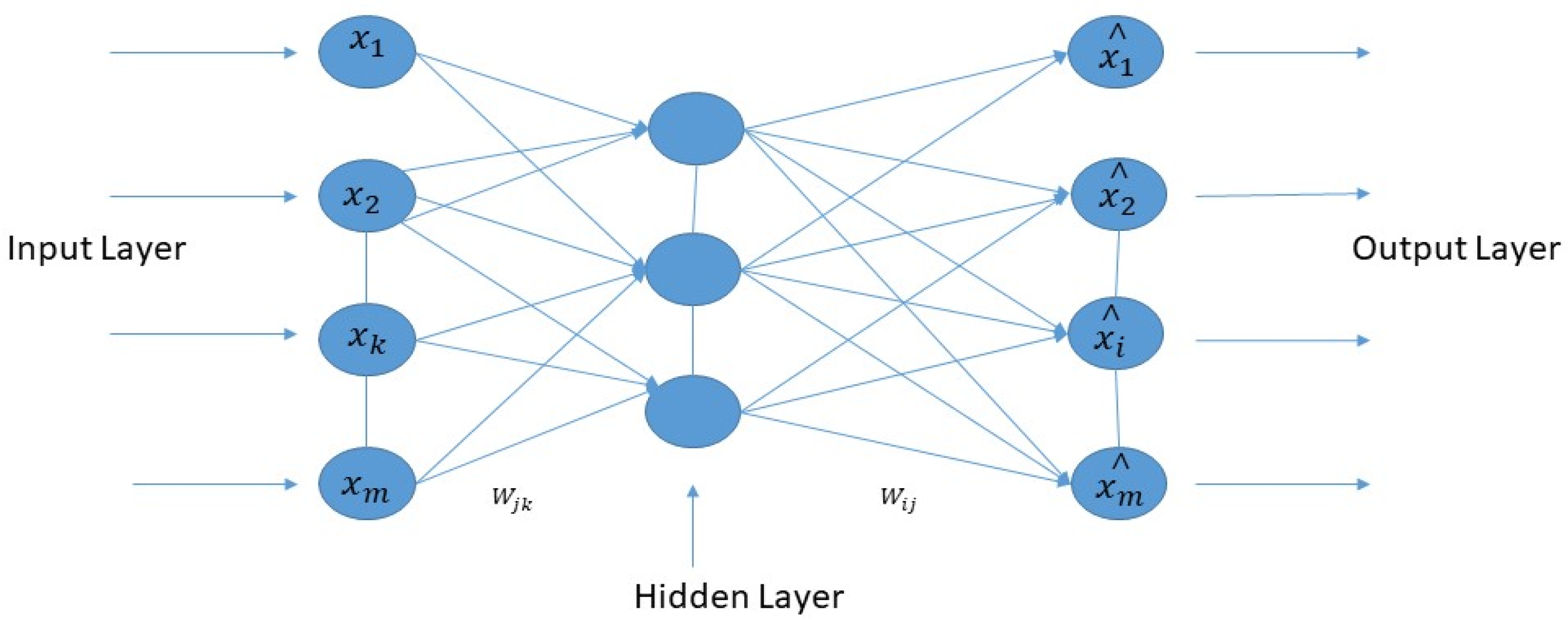
4.1. Deep Wavelet Auto-Encoder
Deep Wavelet Auto-Encoder Model Training
4.2. High Pass Filter
4.3. Segmentation Using a Seeded Region Growing
4.4. Softmax Classifier
5. Experimental Results and Discussion
5.1. The Results of MR Database Processing
5.2. Performances Metrics
5.2.1. Accuracy (ACC)
5.2.2. Sensitivity (SE)
5.2.3. Specificity (SP)
5.2.4. Dice Similarity Coefficient (DSC)
5.2.5. PRECISION (PRE)
5.2.6. JACCARD Similarity Index (JSI)
5.2.7. FALSE Positive Rate (FPR)
5.2.8. FALSE Negative Rate (FNR)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | DSC% |
|---|---|
| CNN [20] | 83.7 |
| CNN-small filter [49] | 88 |
| CRF [55] | 62 |
| HMV [45] | 85 |
| 3D fully connected [21] | 84.7 |
| Integrated hierarchical [56] | 73 |
| Local independent projection [57] | 75 |
| RG + MKM + U-NET [54] | 90 |
| HOG + LBP + deep features [53] | 96.11 |
| Multi-scale 3D with fully connected CRF [21] | 90 |
| Proposed DWAE model | 96.55 |
| Model | FPR | FNR |
|---|---|---|
| DNN [58] | 0.16 | 0.06 |
| DAE-JOA [33] | 0.46 | 0.04 |
| Stacked auto-encoder [32] | 0.07 | 0.1 |
| Alex-Net [52] | 0.07 | 0.128 |
| Google-Net [47] | 0.714 | 0.339 |
| Multimodal [59] | - | 1.74 |
| KNN [48] | 0.62 | 0.54 |
| Proposed DWAE model | 0.0625 | 0.031 |
| Model | JSI% |
|---|---|
| Stacked auto-encoder [32] | 89 |
| DNN [52] | 90.4 |
| Stable algorithm [28] | 92.3 |
| Proposed DWAE model | 93.3 |
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Dahshan, E.-S.A.; Mohsen, H.M.; Revett, K.; Salem, A.-B.M. Computer-aided diagnosis of human brain tumor through MRI: A survey and a new algorithm. Exp. Syst. Appl. 2014, 41, 5526–5545. [Google Scholar] [CrossRef]
- Logeswari, T.; Karnan, M. An improved implementation of brain tumor detection using segmentation based on the hierarchicaself-organizing map. Int. J. Comp. Theory Eng. 2010, 2, 591. [Google Scholar] [CrossRef] [Green Version]
- Tong, J.; Zhao, Y.; Zhang, P.; Chen, L.; Jiang, L. MRI brain tumor segmentation based on texture features and kernel sparse coding. Biomed. Signal Process. Control 2018, 47, 387–392. [Google Scholar] [CrossRef]
- Singh, M.; Verma, A.; Sharma, N. An Optimized Cascaded Stochastic Resonance for the Enhancement of Brain MRI. Innov. Res. Biomed. Eng. J. 2018, 39, 334–342. [Google Scholar] [CrossRef]
- Pham, T.X.; Siarry, P.; Oulhadj, H. Integrating fuzzy entropy clustering with an improved PSO for MRI brain image segmentation. Appl. Soft Comput. 2018, 65, 230–242. [Google Scholar] [CrossRef]
- El-Dahshan, E.-S.A.; Hosny, T.; Salem, A.-B.M. Hybrid intelligent techniques for MRI brain images classification. Digit. Signal Process. 2010, 20, 433–441. [Google Scholar] [CrossRef]
- Das, S.; Chowdhury, M.; Kundu, M.K. Brain MR image classification using multiscale geometric analysis of ripplet. Prog. Electromagn. Res. 2013, 137, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Cheng, I.; Basu, A. Fluid Vector Flow and Applications in Brain Tumor Segmentation. IEEE Trans. Biomed. Eng. 2009, 56, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Al-Okaili, R.N.; Krejza, J.; Woo, J.H.; Wolf, R.L.; O’Rourke, D.M.; Judy, K.D.; Poptani, H.; Melhem, E.R. Intraaxial brain masses: MR imag-ing-based diagnostic strategy—Initial experience. Radiology 2007, 243, 539–550. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Wu, Y.; Huang, M.; Yang, W.; Chen, W.; Feng, Q. 3D brain tumor segmentation in multimodal MR images based on learning population- and patient-specific feature sets. Comput. Med. Imaging Graph. 2013, 37, 512–521. [Google Scholar] [CrossRef]
- Ortiz, A.; Górriz, J.M.; Ramírez, J.; Salas-Gonzalez, D. Improving MRI segmentation with probabilistic GHSOM and multiobjective optimization. Neurocomputing 2013, 114, 118–131. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Yasmin, M.; Fernandes, S.L. A distinctive approach in brain tumor detection and classification using MRI. Pattern Recognit. Lett. 2020, 139, 118–127. [Google Scholar] [CrossRef]
- Chen, M.; Yan, Q.; Qin, M. A segmentation of brain MRI images utilizing intensity and contextual information by Markov random field. Comput. Assist. Surg. 2017, 22, 200–211. [Google Scholar] [CrossRef]
- Chen, T.; Lin, L.; Zuo, W.; Luo, X.; Zhang, L. Learning a wavelet-like auto-encoder to accelerate deep neural networks. In Proceedings of the AAAI Conference on Artificial Intelligence, New Orleans, LA, USA, 2–7 February 2018; pp. 74–93. [Google Scholar]
- Zhao, X.; Wu, Y.; Song, G.; Li, Z.; Zhang, Y.; Fan, Y. A deep learning model integrating FCNNs and CRFs for brain tumor segmentation. Med. Image Anal. 2018, 43, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Havaei, M.; Dutil, F.; Pal, C.; Larochelle, H.; Jodoin, P.-M. A Convolutional Neural Network Approach to Brain Tumor Segmentation. In BrainLes; Springer: Cham, Switzerland, 2015; pp. 195–208. [Google Scholar]
- Chen, X.; Konukoglu, E. Unsupervised detection of lesions in brain MRI using constrained adversarial auto-encoders. arXiv 2018, arXiv:1806.04972. [Google Scholar]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.-M.; Larochelle, H. Brain tumor segmentation with Deep Neural Networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dvořák, P.; Menze, B. Local Structure Prediction with Convolutional Neural Networks for Multimodal Brain Tumor Segmentation. In International MICCAI Workshop on Medical Computer Vision; Springer: Cham, Switzerland, 2015; pp. 59–71. [Google Scholar]
- Chen, L.; Bentley, P.; Rueckert, D. Fully automatic acute ischemic lesion segmentation in DWI using convolutional neural networks. NeuroImage Clin. 2017, 15, 633–643. [Google Scholar] [CrossRef]
- Kamnitsas, K.; Ledig, C.; Newcombe, V.; Simpson, J.P.; Kane, A.D.; Menon, D.K.; Rueckert, D.; Glocker, B. Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmentation. Med. Image Anal. 2017, 36, 61–78. [Google Scholar] [CrossRef]
- El-Melegy, M.; El-Magd, K.M.A.; Ali, S.A.; Hussain, K.F.; Mahdy, Y.B. A comparative study of classification methods for automatic multimodal brain tumor segmentation. In Proceedings of the International Conference on Innovative Trends in Computer Engineering (ITCE), Aswan, Egypt, 19–21 February 2018; pp. 36–41. [Google Scholar]
- Lyksborg, M.; Puonti, O.; Agn, M.; Larsen, R. An Ensemble of 2D Convolutional Neural Networks for Tumor Segmentation. In 19th Scandinavian Conference on Image Analysis; Springer: Copenhagen, Denmark, 2015; pp. 201–211. [Google Scholar]
- Rao, V.; Sarabi, M.S.; Jaiswal, A. Brain tumor segmentation with deep learning. In Proceedings of MICCAI Multimodal Brain Tumor Segmentation Challenge (BraTS); Springer: Cham, Switzerland, 2015; Volume 59, p. 56. [Google Scholar]
- Cengil, E.; Çınar, A.; Özbay, E. Image classification with caffe deep learning framework. In Proceedings of the International Conference on Computer Science and Engineering (UBMK), Antalya, Turkey, 5–8 October 2017; pp. 440–444. [Google Scholar]
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N. Brain Tumor Type Classification via Capsule Networks. In Proceedings of the 25th IEEE International Conference on Image Processing (ICIP), Athens, Greece, 7–10 October 2018; pp. 3129–3133. [Google Scholar]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep Learning for Brain MRI Segmentation: State of the Art and Future Directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef] [Green Version]
- Korfiatis, P.; Kline, T.L.; Erickson, B.J. Automated Segmentation of Hyper intense Regions in FLAIR MRI Using Deep Learning. Tomography 2016, 2, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Mallick, P.K.; Ryu, S.H.; Satapathy, S.K.; Mishra, S.; Nguyen, G.N.; Tiwari, P. Brain MRI Image Classification for Cancer Detection Using Deep Wavelet Autoencoder-Based Deep Neural Network. IEEE Access 2019, 7, 46278–46287. [Google Scholar] [CrossRef]
- Nayak, D.R.; Dash, R.; Majhi, B.; Pachori, R.B.; Zhang, Y. A deep stacked random vector functional link network autoencoder for diagnosis of brain abnormalities and breast cancer. Biomed. Signal Process. Control 2020, 58, 101860. [Google Scholar] [CrossRef]
- Mishra, S.K.; Deepthi, V.H. Brain image classification by the combination of different wavelet transforms and support vector machine classification. J. Ambient. Intell. Humaniz. Comput. 2020, 12, 6741–6749. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Gul, N.; Raza, M.; Anjum, M.A.; Nisar, M.W.; Bukhari, S.A.C. Brain Tumor Detection by Using Stacked Autoencoders in Deep Learning. J. Med. Syst. 2020, 44, 32. [Google Scholar] [CrossRef] [PubMed]
- Raja, P.S.; Rani, A.V. Brain tumor classification using a hybrid deep autoencoder with Bayesian fuzzy clustering-based segmentation approach. Biocybern. Biomed. Eng. 2020, 40, 440–453. [Google Scholar] [CrossRef]
- Arunkumar, N.; Mohammed, M.A.; Ghani, M.K.A.; Ibrahim, D.A.; Abdulhay, E.; Ramirez-Gonzalez, G.; Albuquerque, V.H.C. K-Means clustering and neural network for object detecting and identifying abnormality of brain tumor. Soft Comput. 2019, 23, 9083–9096. [Google Scholar] [CrossRef]
- Arunkumar, N.; Mohammed, M.; Mostafa, S.A.; Ibrahim, D.A.; Rodrigues, J.J.; De Albuquerque, V.H.C. Fully automatic model-based segmentation and classification approach for MRI brain tumor using artificial neural networks. Concurr. Comput. Pract. Exp. 2020, 32, e4962. [Google Scholar] [CrossRef]
- Odusami, M.; Maskeliūnas, R.; Damaševičius, R.; Krilavičius, T. Analysis of Features of Alzheimer’s Disease: Detection of Early Stage from Functional Brain Changes in Magnetic Resonance Images Using a Finetuned ResNet18 Network. Diagnostics 2021, 11, 1071. [Google Scholar] [CrossRef]
- Huang, Z.; Xu, H.; Su, S.; Wang, T.; Luo, Y.; Zhao, X.; Liu, Y.; Song, G.; Zhao, Y. A computer-aided diagnosis system for brain magnetic resonance imaging images using a novel differential feature neural network. Comput. Biol. Med. 2020, 121, 103818. [Google Scholar] [CrossRef] [PubMed]
- Rundo, L.; Militello, C.; Tangherloni, A.; Russo, G.; Vitabile, S.; Gilardi, M.C.; Mauri, G. NeXt for neuro-radiosurgery: A fully automatic approach for necrosis extraction in brain tumor MRI using an unsupervised machine learning technique. Int. J. Imaging Syst. Technol. 2018, 28, 21–37. [Google Scholar] [CrossRef]
- Mekhmoukh, A.; Mokrani, K. Improved Fuzzy C-Means based Particle Swarm Optimization (PSO) initialization and outlier rejection with level set methods for MR brain image segmentation. Comput. Methods Programs Biomed. 2015, 122, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Rundo, L.; Murao, K.; Noguchi, T.; Shimahara, Y.; Milacski, Z.Á.; Koshino, S.; Sala, E.; Nakayama, H.; Satoh, S. MADGAN: Unsupervised medical anomaly de-tection GAN using multiple adjacent brain MRI slice reconstruction. BMC Bioinform. 2021, 22, 1–20. [Google Scholar] [CrossRef]
- Sahu, Y.K.; Pandey, C.; Biswas, P.; Khan, M.; Rathore, S. Minimum Time Delay and More Efficient Image Filtering Brain Tumour Detection with the help of MATLAB. In Proceedings of the 2020 International Conference on Communication and Signal Processing (ICCSP), Tamilnadu, India, 11–13 November 2020; pp. 1195–1199. [Google Scholar]
- Ramesh, S.; Sasikala, S.; Paramanandham, N. Segmentation and classification of brain tumors using modified median noise filter and deep learning approaches. Multimed. Tools Appl. 2021, 80, 11789–11813. [Google Scholar] [CrossRef]
- Kleesiek, J.; Biller, A.; Urban, G.; Kothe, U.; Bendszus, M.; Hamprecht, F. Ilastik for multi-modal brain tumor segmentation. In Proceedings MICCAI BraTS (Brain Tumor Segmentation Challenge); Spyridon: Boston, MA, USA, 2014; pp. 12–17. [Google Scholar]
- Reza, S.M.S.; Mays, R.; Iftekharuddin, K.M. Multi-fractal detrended texture feature for brain tumor classification. In Medical Imaging 2015: Computer-Aided Diagnosis; SPIE: Bellingham, WA, USA, 2015; Volume 9414, p. 941410. [Google Scholar]
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-Cramer, J.; Farahani, K.; Kirby, J.; Burren, Y.; Porz, N.; Slotboom, J.; Wiest, R.; et al. The Multimodal Brain Tumor Image Segmentation Benchmark (BRATS). IEEE Trans. Med. Imaging 2014, 34, 1993–2024. [Google Scholar] [CrossRef]
- Badža, M.M.; Barjaktarović, M. Classification of Brain Tumors from MRI Images Using a Convolutional Neural Network. Appl. Sci. 2020, 10, 1999. [Google Scholar] [CrossRef] [Green Version]
- Toğaçar, M.; Ergen, B.; Cömert, Z. BrainMRNet: Brain tumor detection using magnetic resonance images with a novel convolutional neural network model. Med. Hypotheses 2020, 134, 109531. [Google Scholar] [CrossRef] [PubMed]
- Chavan, N.V.; Jadhav, B.; Patil, P. Detection and classification of brain tumors. Int. J. Comp. Appl. 2015, 112, 45–53. [Google Scholar]
- Pereira, S.; Pinto, A.; Alves, V.; Silva, C. Brain Tumor Segmentation Using Convolutional Neural Networks in MRI Images. IEEE Trans. Med. Imaging 2016, 35, 1240–1251. [Google Scholar] [CrossRef]
- Hemanth, D.J.; Anitha, J.; Naaji, A.; Geman, O.; Popescu, D.E.; Son, L.H.; Hoang, L. A Modified Deep Convolutional Neural Network for Abnormal Brain Image Classification. IEEE Access 2018, 7, 4275–4283. [Google Scholar] [CrossRef]
- Ozyurt, F.; Sert, E.; Avcı, D. An expert system for brain tumor detection: Fuzzy C-means with super resolution and convolutional neural network with extreme learning machine. Med. Hypotheses 2020, 134, 109433. [Google Scholar] [CrossRef]
- Chelghoum, R.; Ikhlef, A.; Hameurlaine, A.; Jacquir, S. Transfer learning using convolutional neural network architectures for brain tumor classification from MRI images. In Proceedings of the International Conference on Artificial Intelligence Applications and Innovations, Crete, Greece, 25–27 June 2020; pp. 189–200. [Google Scholar]
- Biratu, E.S.; Schwenker, F.; Debelee, T.G.; Kebede, S.R.; Negera, W.G.; Molla, H.T. Enhanced Region Growing for Brain Tumor MR Image Segmentation. J. Imaging 2021, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Saba, T.; Mohamed, A.S.; El-Affendi, M.; Amin, J.; Sharif, M. Brain tumor detection using a fusion of handcrafted and deep learning features. Cogn. Syst. Res. 2020, 59, 221–230. [Google Scholar] [CrossRef]
- Wu, W.; Chen, A.Y.C.; Zhao, L.; Corso, J.J. Brain tumor detection and segmentation in a CRF (conditional random fields) framework with pixel-pairwise affinity and superpixel-level features. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 241–253. [Google Scholar] [CrossRef]
- Bauer, S.; Fejes, T.; Slotboom, J.; Wiest, R.; Nolte, L.-P.; Reyes, M. Segmentation of brain tumor images based on integrated hierarchical classification and regularization. In Proceedings of the MICCAI BraTS Workshop; Miccai Society: Nice, France, 2012; p. 11. [Google Scholar]
- Huang, M.; Yang, W.; Wu, Y.; Jiang, J.; Chen, W.; Feng, Q. Brain tumor segmentation based on local independent projection-based classification. Trans. Biomed. Eng. J. 2014, 61, 2633–2645. [Google Scholar] [CrossRef] [PubMed]
- Amin, J.; Sharif, M.; Yasmin, M.; Fernandes, S.L. Big data analysis for brain tumor detection: Deep convolutional neural networks. Future Gener. Comput. Syst. 2018, 87, 290–297. [Google Scholar] [CrossRef]
- Khan, M.A.; Ashraf, I.; Alhaisoni, M.; Damaševičius, R.; Scherer, R.; Rehman, A.; Bukhari, S.A.C. Multimodal Brain Tumor Classification Using Deep Learning and Robust Feature Selection: A Machine Learning Application for Radiologists. Diagnostics 2020, 10, 565. [Google Scholar] [CrossRef] [PubMed]





| Model | Accuracy % | Sensitivity % | Specificity % | Precision % |
|---|---|---|---|---|
| DWA-DNN [29] | 93.14 | 92.16 | 94.26 | 93.15 |
| DAE-JOA [33] | 98.5 | 95.4 | - | 95.6 |
| CNN [46] | 96.5 | - | 95 | 94.81 |
| Google-Net [47] | 89.66 | 84.85 | 96 | 96.55 |
| Vgg16 [47] | 84.48 | 81.25 | 88.48 | 89.66 |
| KNN [48] | 78 | 46 | 50 | 52 |
| DNN [49] | 93 | 75 | 80 | 72 |
| M-CNN [50] | 96.4 | 95 | 93 | 95.7 |
| CNN-SVM [51] | 95.62 | - | 95 | 92.12 |
| Alex-Net [52] | 87.66 | 84.38 | 92.31 | 93.1 |
| HOG + LBP + Deep features [53] | 98.71 | 98.46 | 96.72 | - |
| RG + MKM + U-NET [54] | 98.72 | 90.7 | 99.7 | - |
| Proposed DWAE Model | 99.3 | 95.6 | 96.9 | 97.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abd El Kader, I.; Xu, G.; Shuai, Z.; Saminu, S.; Javaid, I.; Ahmad, I.S.; Kamhi, S. Brain Tumor Detection and Classification on MR Images by a Deep Wavelet Auto-Encoder Model. Diagnostics 2021, 11, 1589. https://doi.org/10.3390/diagnostics11091589
Abd El Kader I, Xu G, Shuai Z, Saminu S, Javaid I, Ahmad IS, Kamhi S. Brain Tumor Detection and Classification on MR Images by a Deep Wavelet Auto-Encoder Model. Diagnostics. 2021; 11(9):1589. https://doi.org/10.3390/diagnostics11091589
Chicago/Turabian StyleAbd El Kader, Isselmou, Guizhi Xu, Zhang Shuai, Sani Saminu, Imran Javaid, Isah Salim Ahmad, and Souha Kamhi. 2021. "Brain Tumor Detection and Classification on MR Images by a Deep Wavelet Auto-Encoder Model" Diagnostics 11, no. 9: 1589. https://doi.org/10.3390/diagnostics11091589
APA StyleAbd El Kader, I., Xu, G., Shuai, Z., Saminu, S., Javaid, I., Ahmad, I. S., & Kamhi, S. (2021). Brain Tumor Detection and Classification on MR Images by a Deep Wavelet Auto-Encoder Model. Diagnostics, 11(9), 1589. https://doi.org/10.3390/diagnostics11091589