
Faster Region-Based Convolutional Neural Network in the Classification of Different Parkinsonism Patterns of the Striatum on Maximum Intensity Projection Images of [18F]FP-CIT Positron Emission Tomography

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
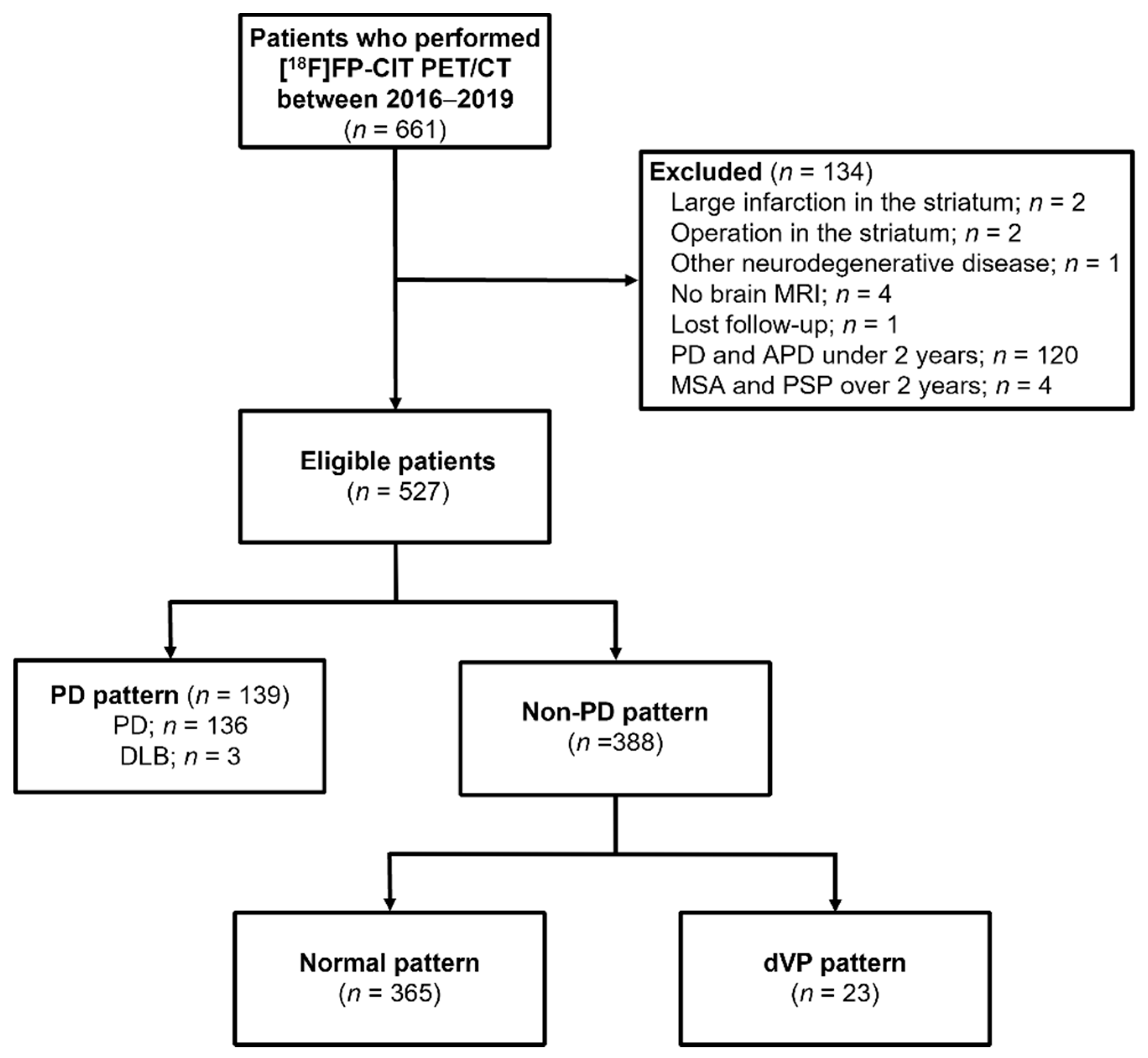
2.1. Subjects
2.2. [18F]FP-CIT Positron Emission Tomography/Computed Tomography Acquisition
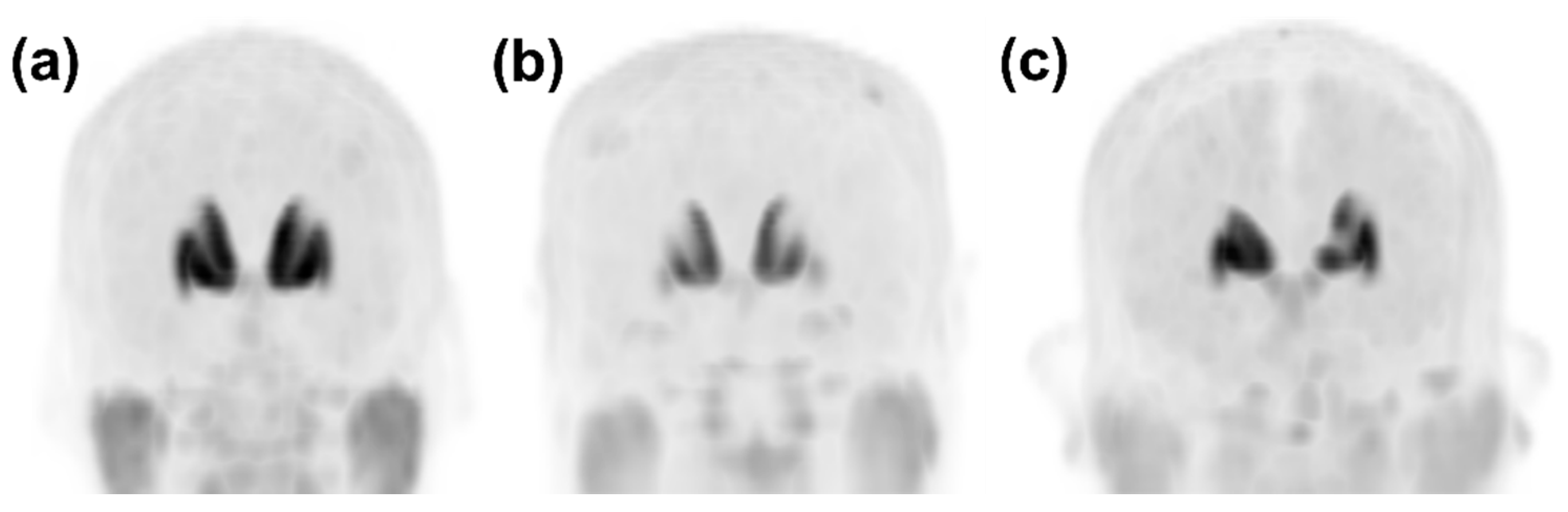
2.3. Image Classification and Data Annotation
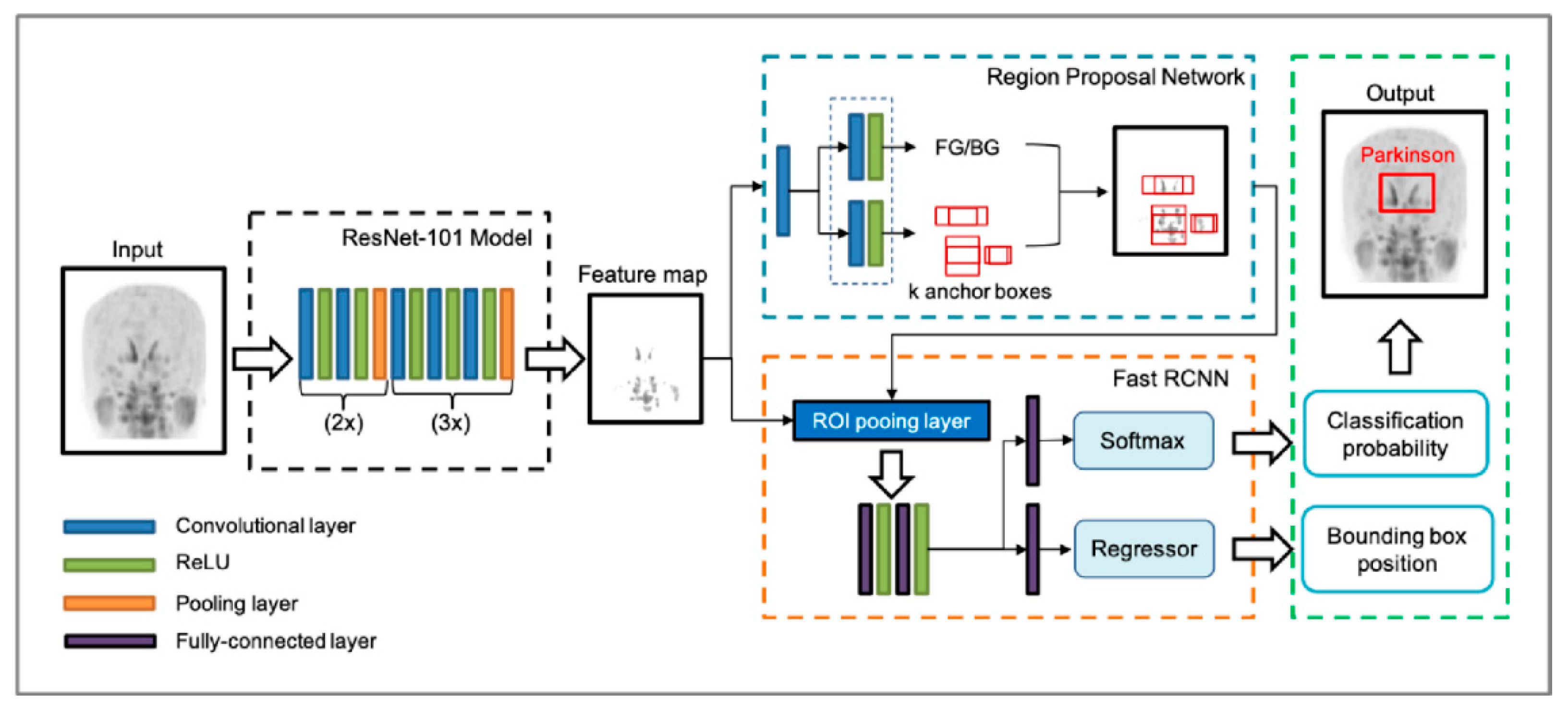
2.4. Faster Region-Based Convolutional Neural Network (Faster R-CNN) Architecture Construction
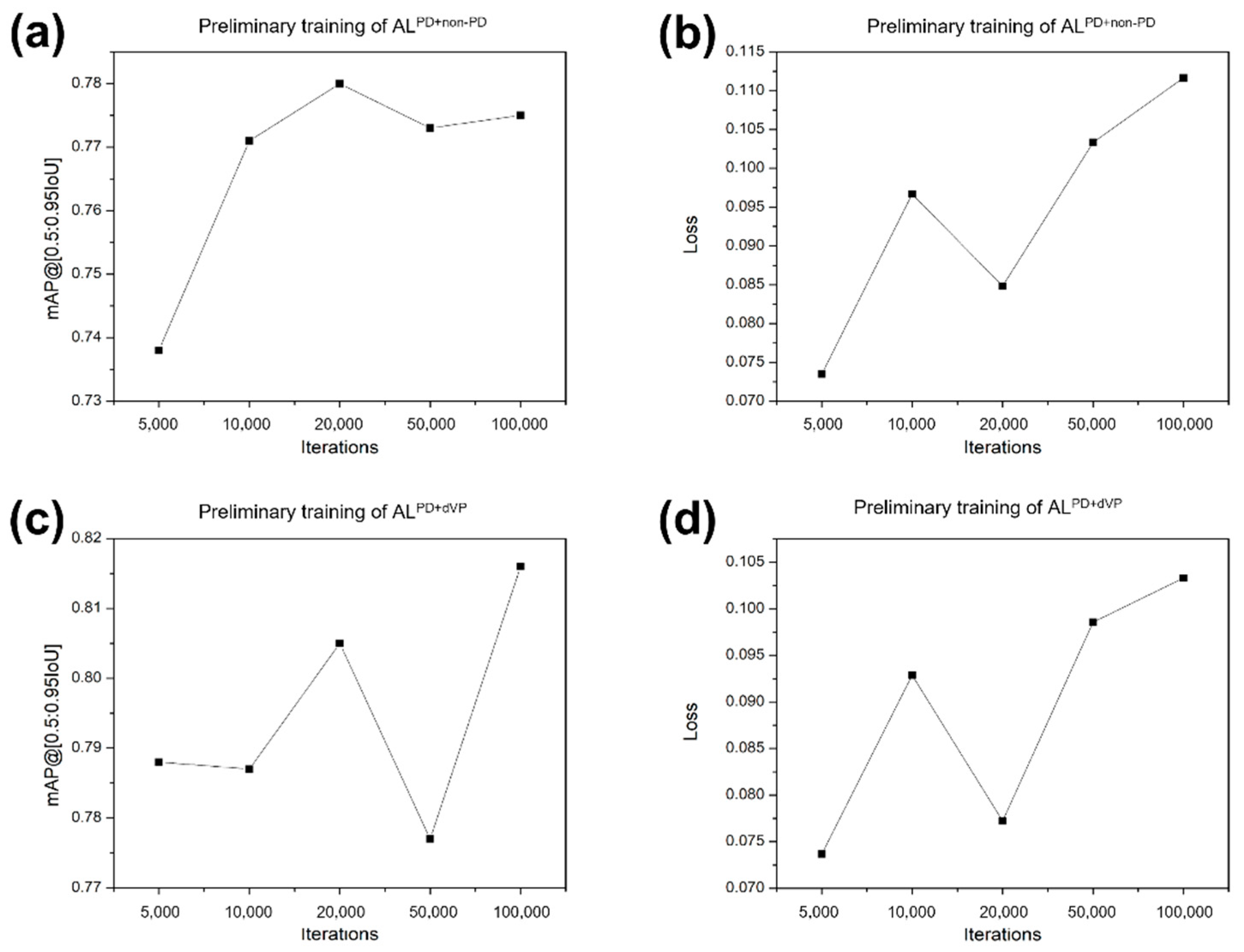
2.5. Training, Validation, and Testing of Faster R-CNN
2.6. Pattern Classification by the NM Physicians
2.7. Statistical Analyses
3. Results
3.1. Patients’ Clinical Characteristics
3.2. Calculated Pattern Score of Each Image Using the Faster R-CNN
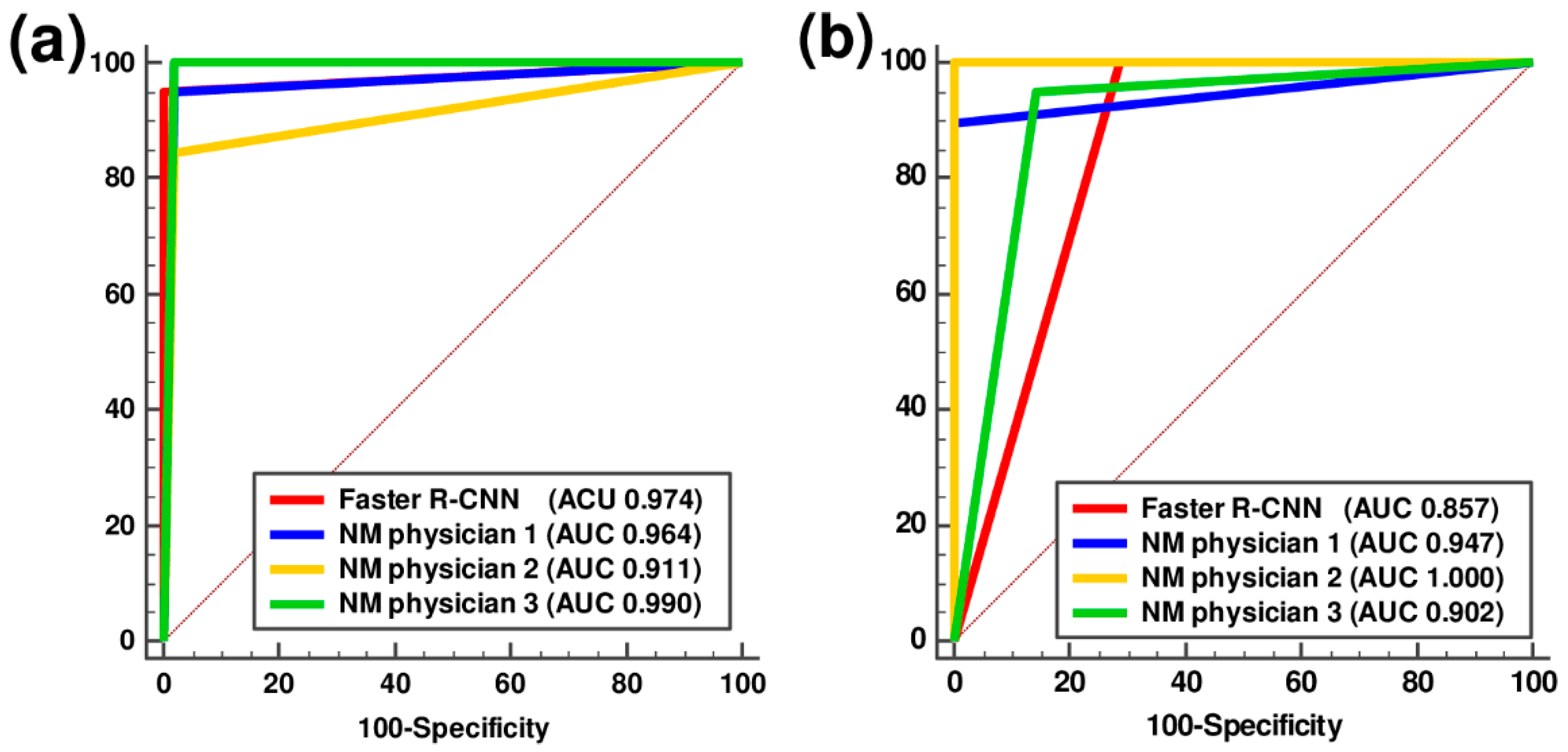
3.3. Performance Comparison between the Faster R-CNN and NM Physicians
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, D.R.; Litvan, I. Parkinsonian syndromes. Continuum 2013, 19, 1189–1212. [Google Scholar] [CrossRef]
- Ogawa, T.; Fujii, S.; Kuya, K.; Kitao, S.-I.; Shinohara, Y.; Ishibashi, M.; Tanabe, Y. Role of Neuroimaging on Differentiation of Parkinson’s Disease and Its Related Diseases. Yonago Acta Med. 2018, 61, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Caslake, R.; Moore, J.N.; Gordon, J.C.; Harris, C.E.; Counsell, C. Changes in diagnosis with follow-up in an incident cohort of patients with parkinsonism. J. Neurol. Neurosurg. Psychiatry 2008, 79, 1202–1207. [Google Scholar] [CrossRef][Green Version]
- Rizzo, G.; Copetti, M.; Arcuti, S.; Martino, D.; Fontana, A.; Logroscino, G. Accuracy of clinical diagnosis of Parkinson disease: A systematic review and meta-analysis. Neurology 2016, 86, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Saeed, U.; Compagnone, J.; Aviv, R.I.; Strafella, A.P.; Black, S.E.; Lang, A.E.; Masellis, M. Imaging biomarkers in Parkinson’s disease and Parkinsonian syndromes: Current and emerging concepts. Transl. Neurodegener. 2017, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Harvey, H.B.; Watson, L.C.; Subramaniam, R.M.; Burns, J.; Bykowski, J.; Chakraborty, S.; Ledbetter, L.N.; Lee, R.K.; Pannell, J.S.; Pollock, J.M.; et al. ACR Appropriateness Criteria® Movement Disorders and Neurodegenerative Diseases. J. Am. Coll. Radiol. 2020, 17, S175–S187. [Google Scholar] [CrossRef]
- Darcourt, J.; Booij, J.; Tatsch, K.; Varrone, A.; Vander Borght, T.; Kapucu, O.L.; Någren, K.; Nobili, F.; Walker, Z.; Van Laere, K. EANM procedure guidelines for brain neurotransmission SPECT using (123)I-labelled dopamine transporter ligands, version 2. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Djang, D.S.; Janssen, M.J.; Bohnen, N.; Booij, J.; Henderson, T.A.; Herholz, K.; Minoshima, S.; Rowe, C.C.; Sabri, O.; Seibyl, J.; et al. SNM practice guideline for dopamine transporter imaging with 123I-ioflupane SPECT 1.0. J. Nucl. Med. 2012, 53, 154–163. [Google Scholar] [CrossRef]
- Oh, M.; Kim, J.S.; Kim, J.Y.; Shin, K.H.; Park, S.H.; Kim, H.O.; Moon, D.H.; Oh, S.J.; Chung, S.J.; Lee, C.S. Subregional patterns of preferential striatal dopamine transporter loss differ in Parkinson disease, progressive supranuclear palsy, and multiple-system atrophy. J. Nucl. Med. 2012, 53, 399–406. [Google Scholar] [CrossRef]
- Kahraman, D.; Eggers, C.; Schicha, H.; Timmermann, L.; Schmidt, M. Visual assessment of dopaminergic degeneration pattern in 123I-FP-CIT SPECT differentiates patients with atypical parkinsonian syndromes and idiopathic Parkinson’s disease. J. Neurol. 2012, 259, 251–260. [Google Scholar] [CrossRef]
- Mazurowski, M.A.; Buda, M.; Saha, A.; Bashir, M.R. Deep learning in radiology: An overview of the concepts and a survey of the state of the art with focus on MRI. J. Magn. Reson. Imaging 2019, 49, 939–954. [Google Scholar] [CrossRef]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards Real-Time Object Detection with Region Proposal Networks. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 1137–1149. [Google Scholar] [CrossRef]
- Ruhan, S.; Owens, W.; Wiegand, R.; Studin, M.; Capoferri, D.; Barooha, K.; Greaux, A.; Rattray, R.; Hutton, A.; Cintineo, J.; et al. Intervertebral disc detection in X-ray images using faster R-CNN. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2017, 2017, 564–567. [Google Scholar] [CrossRef]
- Lu, Y.; Yu, Q.; Gao, Y.; Zhou, Y.; Liu, G.; Dong, Q.; Ma, J.; Ding, L.; Yao, H.; Zhang, Z.; et al. Identification of Metastatic Lymph Nodes in MR Imaging with Faster Region-Based Convolutional Neural Networks. Cancer Res. 2018, 78, 5135–5143. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.M.; Tremoleda, J.L.; Bayomy, T.B.; Gsell, W. Molecular SPECT Imaging: An Overview. Int. J. Mol. Imaging 2011, 2011, 796025. [Google Scholar] [CrossRef] [PubMed]
- Gilman, S.; Wenning, G.K.; Low, P.A.; Brooks, D.J.; Mathias, C.J.; Trojanowski, J.Q.; Wood, N.W.; Colosimo, C.; Dürr, A.; Fowler, C.J.; et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology 2008, 71, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Höglinger, G.U.; Respondek, G.; Stamelou, M.; Kurz, C.; Josephs, K.A.; Lang, A.E.; Mollenhauer, B.; Müller, U.; Nilsson, C.; Whitwell, J.L.; et al. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov. Disord. 2017, 32, 853–864. [Google Scholar] [CrossRef]
- Greenland, J.C.; Baker, R.A. The Differential Diagnosis of Parkinson’s Diseas. In Parkinson’s Disease: Pathogenesis and Clinical Aspects; Stoker, T.B., Greenland, J.C., Eds.; Codon Publications: Brisbane, Australia, 2018. [Google Scholar]
- Jin, S.; Oh, M.; Oh, S.J.; Oh, J.S.; Lee, S.J.; Chung, S.J.; Lee, C.S.; Kim, J.S. Differential Diagnosis of Parkinsonism Using Dual-Phase F-18 FP-CIT PET Imaging. Nucl. Med. Mol. Imaging 2013, 47, 44–51. [Google Scholar] [CrossRef]
- Dutta, A.; Zisserman, A. The VIA Annotation Software for Images, Audio and Video. In Proceedings of the 27th ACM International Conference on Multimedia, Nice, France, 21–25 October 2019; pp. 2276–2279. [Google Scholar]
- Huertas-Fernández, I.; García-Gómez, F.J.; García-Solís, D.; Benítez-Rivero, S.; Marín-Oyaga, V.A.; Jesús, S.; Cáceres-Redondo, M.T.; Lojo, J.A.; Martín-Rodríguez, J.F.; Carrillo, F.; et al. Machine learning models for the differential diagnosis of vascular parkinsonism and Parkinson’s disease using [(123)I]FP-CIT SPECT. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 112–119. [Google Scholar] [CrossRef]
- Kim, D.H.; Wit, H.; Thurston, M. Artificial intelligence in the diagnosis of Parkinson’s disease from ioflupane-123 single-photon emission computed tomography dopamine transporter scans using transfer learning. Nucl. Med. Commun. 2018, 39, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Shiiba, T.; Arimura, Y.; Nagano, M.; Takahashi, T.; Takaki, A. Improvement of classification performance of Parkinson’s disease using shape features for machine learning on dopamine transporter single photon emission computed tomography. PLoS ONE 2020, 15, e0228289. [Google Scholar] [CrossRef] [PubMed]
- Augimeri, A.; Cherubini, A.; Cascini, G.L.; Galea, D.; Caligiuri, M.E.; Barbagallo, G.; Arabia, G.; Quattrone, A. CADA-computer-aided DaTSCAN analysis. EJNMMI Phys. 2016, 3, 4. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Ha, S.; Im, H.J.; Paek, S.H.; Lee, D.S. Refining diagnosis of Parkinson’s disease with deep learning-based interpretation of dopamine transporter imaging. NeuroImage Clin. 2017, 16, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Tondeur, M.C.; Hambye, A.S.; Dethy, S.; Ham, H.R. Interobserver reproducibility of the interpretation of I-123 FP-CIT single-photon emission computed tomography. Nucl. Med. Commun. 2010, 31, 717–725. [Google Scholar] [CrossRef]
- Papathanasiou, N.; Rondogianni, P.; Chroni, P.; Themistocleous, M.; Boviatsis, E.; Pedeli, X.; Sakas, D.; Datseris, I. Interobserver variability, and visual and quantitative parameters of (123)I-FP-CIT SPECT (DaTSCAN) studies. Ann. Nucl. Med. 2012, 26, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Acton, P.D.; Newberg, A.; Plössl, K.; Mozley, P.D. Comparison of region-of-interest analysis and human observers in the diagnosis of Parkinson’s disease using [99mTc]TRODAT-1 and SPECT. Phys. Med. Biol. 2006, 51, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Illan, I.A.; Gorrz, J.M.; Ramirez, J.; Segovia, F.; Jimenez-Hoyuela, J.M.; Ortega Lozano, S.J. Automatic assistance to Parkinson’s disease diagnosis in DaTSCAN SPECT imaging. Med. Phys. 2012, 39, 5971–5980. [Google Scholar] [CrossRef]
- Brahim, A.; Ramírez, J.; Górriz, J.M.; Khedher, L.; Salas-Gonzalez, D. Comparison between Different Intensity Normalization Methods in 123I-Ioflupane Imaging for the Automatic Detection of Parkinsonism. PLoS ONE 2015, 10, e0130274. [Google Scholar] [CrossRef]
- Chakraborty, S.; Aich, S.; Kim, H. Detection of parkinson’s disease from 3T T1 weighted MRI scans using 3D convolutional neural network. Diagnostics 2020, 10, 402. [Google Scholar] [CrossRef]
- Chakraborty, S.; Aich, S.; Kim, H. 3D textural, morphological and statistical analysis of voxel of interests in 3T MRI scans for the detection of Parkinson’s disease using artificial neural networks. Healthcare 2020, 8, 34. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean Average Precision | Loss of Function | |||||||
|---|---|---|---|---|---|---|---|---|
| ALPD+non-PD | ALPD+dVP | ALPD+non-PD | ALPD+dVP | |||||
| Train | Validation | Train | Validation | Train | Validation | Train | Validation | |
| Model 1 | 0.762 | 0.768 | 0.794 | 0.794 | 0.108 | 0.096 | 0.09 | 0.088 |
| Model 2 | 0.743 | 0.755 | 0.724 | 0.754 | 0.101 | 0.088 | 0.124 | 0.116 |
| Model 3 | 0.769 | 0.765 | 0.782 | 0.789 | 0.094 | 0.089 | 0.081 | 0.082 |
| Model 4 | 0.761 | 0.784 | 0.790 | 0.799 | 0.107 | 0.095 | 0.103 | 0.102 |
| Mean | 0.759 | 0.768 | 0.772 | 0.784 | 0.103 | 0.092 | 0.100 | 0.097 |
| SD | 0.011 | 0.012 | 0.032 | 0.020 | 0.006 | 0.004 | 0.019 | 0.015 |
| p-value | NS | NS | p < 0.05 | NS | ||||
| PD Pattern (n = 139) | Non-PD Pattern (n = 388) | p-Value | |
|---|---|---|---|
| Age of onset (years) | 65.4 ± 9.1 | 69.1 ± 11.6 | <0.001 |
| Sex, male/female (n) | 55/84 | 133/255 | 0.264 |
| Follow-up duration (months) | 56.3 ± 38.0 | 12.9 ± 10.5 | <0.001 |
| Modified Hoehn and Yahr stage | 2.2 ± 0.9 | NA |
| Reader | Sens (%) | Spec (%) | PPV (%) | NPV (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|
| PD vs. non-PD | Faster R-CNN | 94.7 | 100.0 | 100.0 | 98.1 | 98.6 |
| NM Physician 1 | 94.7 | 98.1 | 94.7 | 98.1 | 97.2 | |
| NM Physician 2 | 84.2 | 98.1 | 94.1 | 94.4 | 94.4 | |
| NM Physician 3 | 100.0 | 98.1 | 95.0 | 100.0 | 98.6 | |
| PD vs. dVP | Faster R-CNN | 100.0 | 71.4 | 90.5 | 100.0 | 92.3 |
| NM Physician 1 | 89.5 | 100.0 | 100.0 | 77.8 | 92.3 | |
| NM Physician 2 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | |
| NM Physician 3 | 94.7 | 85.7 | 94.7 | 85.7 | 92.3 |
| Difference between Areas | SE | 95% CI | Z Statistics | p-Value * | ||
|---|---|---|---|---|---|---|
| PD vs. non-PD | NM Physician 1 | 0.0096 | 0.0394 | −0.0677 to 0.0869 | 0.244 | 0.807 |
| NM Physician 2 | 0.0622 | 0.0535 | −0.0426 to 0.1670 | 1.163 | 0.245 | |
| NM Physician 3 | 0.0167 | 0.0280 | −0.0382 to 0.0716 | 0.596 | 0.551 | |
| PD vs. dVP | NM Physician 1 | 0.0902 | 0.0991 | −0.1040 to 0.2840 | 0.911 | 0.362 |
| NM Physician 2 | 0.1430 | 0.0922 | −0.0379 to 0.3240 | 1.549 | 0.121 | |
| NM Physician 3 | 0.0451 | 0.1330 | −0.2160 to 0.3060 | 0.339 | 0.735 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, B.W.; Kang, S.; Kim, H.W.; Kwon, O.D.; Vu, H.D.; Youn, S.W. Faster Region-Based Convolutional Neural Network in the Classification of Different Parkinsonism Patterns of the Striatum on Maximum Intensity Projection Images of [18F]FP-CIT Positron Emission Tomography. Diagnostics 2021, 11, 1557. https://doi.org/10.3390/diagnostics11091557
Choi BW, Kang S, Kim HW, Kwon OD, Vu HD, Youn SW. Faster Region-Based Convolutional Neural Network in the Classification of Different Parkinsonism Patterns of the Striatum on Maximum Intensity Projection Images of [18F]FP-CIT Positron Emission Tomography. Diagnostics. 2021; 11(9):1557. https://doi.org/10.3390/diagnostics11091557
Chicago/Turabian StyleChoi, Byung Wook, Sungmin Kang, Hae Won Kim, Oh Dae Kwon, Huy Duc Vu, and Sung Won Youn. 2021. "Faster Region-Based Convolutional Neural Network in the Classification of Different Parkinsonism Patterns of the Striatum on Maximum Intensity Projection Images of [18F]FP-CIT Positron Emission Tomography" Diagnostics 11, no. 9: 1557. https://doi.org/10.3390/diagnostics11091557
APA StyleChoi, B. W., Kang, S., Kim, H. W., Kwon, O. D., Vu, H. D., & Youn, S. W. (2021). Faster Region-Based Convolutional Neural Network in the Classification of Different Parkinsonism Patterns of the Striatum on Maximum Intensity Projection Images of [18F]FP-CIT Positron Emission Tomography. Diagnostics, 11(9), 1557. https://doi.org/10.3390/diagnostics11091557