Spectral CT Hybrid Images in the Diagnostic Evaluation of Hypervascular Abdominal Tumors—Potential Advantages in Clinical Routine

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
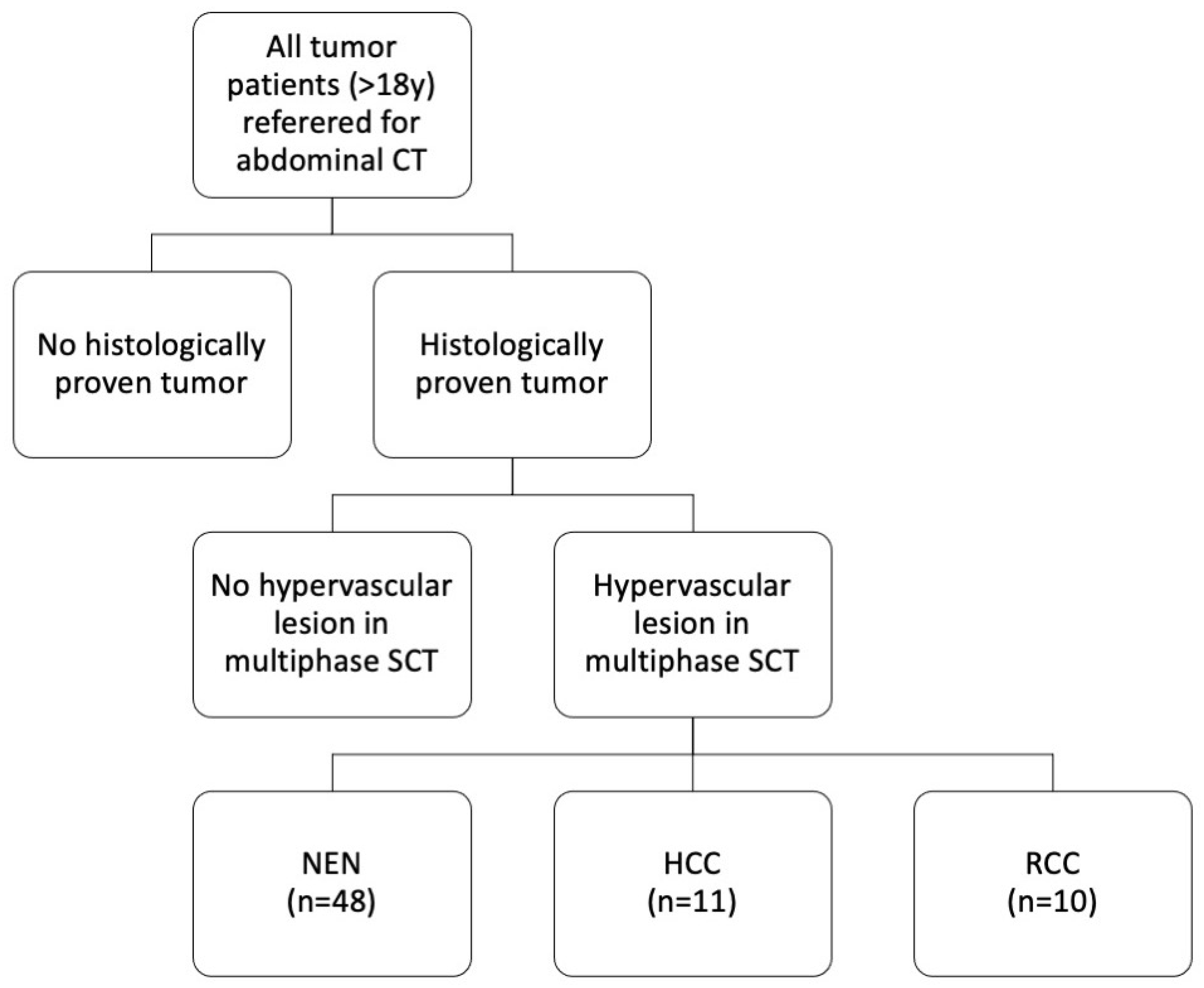
2.1. Patient Population and Study Design
2.2. CT Scanner and Protocol
2.3. Subjective Scoring and Measurements
2.4. Estimated Reading Time
2.5. Statistics
3. Results
3.1. Study Population
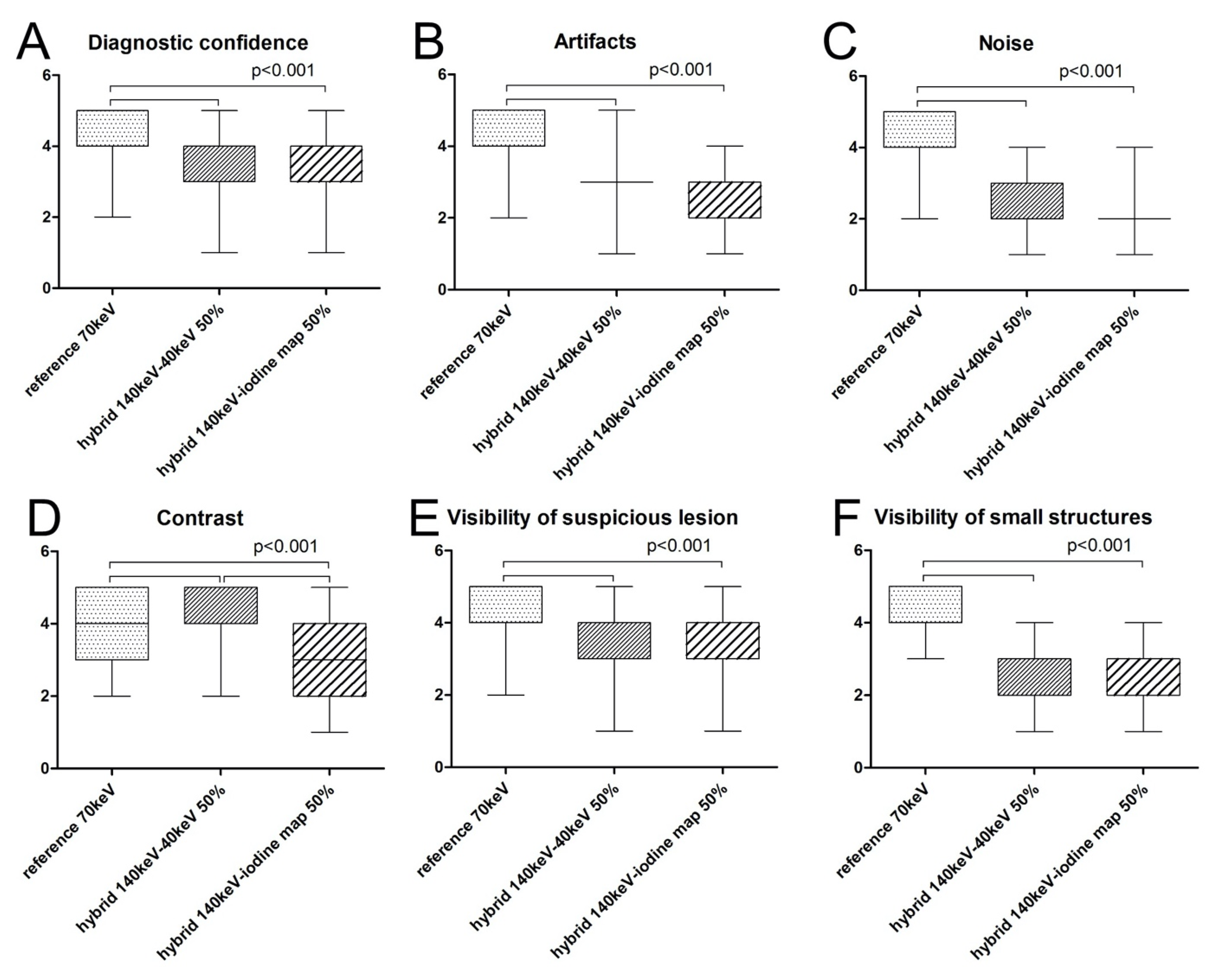
3.2. Subjective Parameters
3.2.1. Diagnostic Confidence
3.2.2. Artifacts
3.2.3. Image Noise
3.2.4. Image Contrast
3.2.5. Visibility of Suspicious Lesions
3.2.6. Visibility of Small Structures
3.3. Estimated Reading Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forner, A.; Vilana, R.; Ayuso, C.; Bianchi, L.; Sole, M.; Ayuso, J.R.; Boix, L.; Sala, M.; Varela, M.; Llovet, J.M.; et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: Prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology 2008, 47, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Sangiovanni, A.; Manini, M.A.; Iavarone, M.; Romeo, R.; Forzenigo, L.V.; Fraquelli, M.; Massironi, S.; Della Corte, C.; Ronchi, G.; Rumi, M.G.; et al. The diagnostic and economic impact of contrast imaging techniques in the diagnosis of small hepatocellular carcinoma in cirrhosis. Gut 2010, 59, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Khalili, K.; Kim, T.K.; Jang, H.J.; Haider, M.A.; Khan, L.; Guindi, M.; Sherman, M. Optimization of imaging diagnosis of 1–2 cm hepatocellular carcinoma: An analysis of diagnostic performance and resource utilization. J. Hepatol. 2011, 54, 723–728. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, C.N.; Darnell, A.; Rengo, M.; Muscogiuri, G.; Bellini, D.; Ayuso, C.; Laghi, A. Dual-energy CT: Oncologic applications. AJR Am. J. Roentgenol. 2012, 199, S98–S105. [Google Scholar] [CrossRef]
- De Cecco, C.N.; Boll, D.T.; Bolus, D.N.; Foley, W.D.; Kaza, R.K.; Morgan, D.E.; Rofsky, N.M.; Sahani, D.V.; Schoepf, U.J.; Shuman, W.P.; et al. White Paper of the Society of Computed Body Tomography and Magnetic Resonance on Dual-Energy CT, Part 4: Abdominal and Pelvic Applications. J. Comput. Assist. Tomogr. 2017, 41, 8–14. [Google Scholar] [CrossRef]
- Fehrenbach, U.; Feldhaus, F.; Kahn, J.; Boning, G.; Maurer, M.H.; Renz, D.; Frost, N.; Streitparth, F. Tumour response in non-small-cell lung cancer patients treated with chemoradiotherapy—Can spectral CT predict recurrence? J. Med. Imaging Radiat. Oncol. 2019, 63, 641–649. [Google Scholar] [CrossRef]
- Jiang, C.; Yang, P.; Lei, J.; Li, J.; Yan, K.; Li, F.; Yan, R.; Xia, L. The Application of Iodine Quantitative Information Obtained by Dual-Source Dual-Energy Computed Tomography on Chemoradiotherapy Effect Monitoring for Cervical Cancer: A Preliminary Study. J. Comput. Assist. Tomogr. 2017, 41, 737–745. [Google Scholar] [CrossRef]
- McCollough, C.H.; Leng, S.; Yu, L.; Fletcher, J.G. Dual- and Multi-Energy CT: Principles, Technical Approaches, and Clinical Applications. Radiology 2015, 276, 637–653. [Google Scholar] [CrossRef]
- Lam, S.; Gupta, R.; Kelly, H.; Curtin, H.D.; Forghani, R. Multiparametric Evaluation of Head and Neck Squamous Cell Carcinoma Using a Single-Source Dual-Energy CT with Fast kVp Switching: State of the Art. Cancers 2015, 7, 2201–2216. [Google Scholar] [CrossRef] [Green Version]
- Albrecht, M.H.; Vogl, T.J.; Martin, S.S.; Nance, J.W.; Duguay, T.M.; Wichmann, J.L.; De Cecco, C.N.; Varga-Szemes, A.; van Assen, M.; Tesche, C.; et al. Review of Clinical Applications for Virtual Monoenergetic Dual-Energy CT. Radiology 2019, 293, 260–271. [Google Scholar] [CrossRef]
- Kaltenbach, B.; Wichmann, J.L.; Pfeifer, S.; Albrecht, M.H.; Booz, C.; Lenga, L.; Hammerstingl, R.; D’Angelo, T.; Vogl, T.J.; Martin, S.S. Iodine quantification to distinguish hepatic neuroendocrine tumor metastasis from hepatocellular carcinoma at dual-source dual-energy liver CT. Eur. J. Radiol. 2018, 105, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Sofue, K.; Tsurusaki, M.; Mileto, A.; Hyodo, T.; Sasaki, K.; Nishii, T.; Chikugo, T.; Yada, N.; Kudo, M.; Sugimura, K.; et al. Dual-energy computed tomography for non-invasive staging of liver fibrosis: Accuracy of iodine density measurements from contrast-enhanced data. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2018, 48, 1008–1019. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Shi, G.; Qi, X.; Fan, X.; Wang, L. Quantitative analysis of the dual-energy CT virtual spectral curve for focal liver lesions characterization. Eur. J. Radiol. 2014, 83, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.Y.; He, C.D.; Zhou, Y.; Huang, D.; Lin, H.; Wang, Z.; Wang, D.; Wang, J.Q.; Liao, L.P. Application of gemstone spectral imaging for efficacy evaluation in hepatocellular carcinoma after transarterial chemoembolization. World J. Gastroenterol. 2016, 22, 3242–3251. [Google Scholar] [CrossRef] [PubMed]
- Boning, G.; Feldhaus, F.; Adelt, S.; Kahn, J.; Fehrenbach, U.; Streitparth, F. Clinical routine use of virtual monochromatic datasets based on spectral CT in patients with hypervascularized abdominal tumors—evaluation of effectiveness and efficiency. Acta Radiol. 2019, 60, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.R.; Yang, Q.H.; Liu, Q.Y.; Min, J.; Li, H.G.; Liu, Z.F.; Li, J.X. Dual energy computed tomography for detection of metastatic lymph nodes in patients with hepatocellular carcinoma. World J. Gastroenterol. 2019, 25, 1986–1996. [Google Scholar] [CrossRef]
- Marin, D.; Nelson, R.C.; Schindera, S.T.; Richard, S.; Youngblood, R.S.; Yoshizumi, T.T.; Samei, E. Low-tube-voltage, high-tube-current multidetector abdominal CT: Improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm--initial clinical experience. Radiology 2010, 254, 145–153. [Google Scholar] [CrossRef]
- Mileto, A.; Nelson, R.C.; Samei, E.; Choudhury, K.R.; Jaffe, T.A.; Wilson, J.M.; Marin, D. Dual-energy MDCT in hypervascular liver tumors: Effect of body size on selection of the optimal monochromatic energy level. AJR Am. J. Roentgenol. 2014, 203, 1257–1264. [Google Scholar] [CrossRef]
- Marin, D.; Choudhury, K.R.; Gupta, R.T.; Ho, L.M.; Allen, B.C.; Schindera, S.T.; Colsher, J.G.; Samei, E.; Nelson, R.C. Clinical impact of an adaptive statistical iterative reconstruction algorithm for detection of hypervascular liver tumours using a low tube voltage, high tube current MDCT technique. Eur. Radiol. 2013, 23, 3325–3335. [Google Scholar] [CrossRef]
- Boning, G.; Adelt, S.; Feldhaus, F.; Fehrenbach, U.; Kahn, J.; Hamm, B.; Streitparth, F. Spectral CT in clinical routine imaging of neuroendocrine neoplasms. Clin. Radiol. 2021, 76, 348–357. [Google Scholar] [CrossRef]
- Auer, T.A.; Munzfeld, H.; Posch, H.; Stockel, J.; Tietze, A.; Bohner, G.; Boning, G. Evaluation of diagnostic accuracy of intracranial aneurysm detection using medical-grade versus commercial consumer-grade displays and different image reconstructions against the background of process optimization for telemedicine. Acta Radiol. 2020, 61, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Drinkwater, B.L. A comparison of the direction-of-perception technique with the Likert method in the measurement of attitudes. J. Soc. Psychol. 1965, 67, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Boning, G.; Kahn, J.F.; Kaul, D.; Rotzinger, R.; Freyhardt, P.; Pavel, M.; Streitparth, F. CT follow-up in patients with neuroendocrine tumors (NETs): Combined radiation and contrast dose reduction. Acta Radiol. 2018, 59, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Lv, P.; Lin, X.Z.; Chen, K.; Gao, J. Spectral CT in patients with small HCC: Investigation of image quality and diagnostic accuracy. Eur. Radiol. 2012, 22, 2117–2124. [Google Scholar] [CrossRef]
- Altenbernd, J.; Heusner, T.A.; Ringelstein, A.; Ladd, S.C.; Forsting, M.; Antoch, G. Dual-energy-CT of hypervascular liver lesions in patients with HCC: Investigation of image quality and sensitivity. Eur. Radiol. 2011, 21, 738–743. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, C.N.; Caruso, D.; Schoepf, U.J.; De Santis, D.; Muscogiuri, G.; Albrecht, M.H.; Meinel, F.G.; Wichmann, J.L.; Burchett, P.F.; Varga-Szemes, A.; et al. A noise-optimized virtual monoenergetic reconstruction algorithm improves the diagnostic accuracy of late hepatic arterial phase dual-energy CT for the detection of hypervascular liver lesions. Eur. Radiol. 2018, 28, 3393–3404. [Google Scholar] [CrossRef]
- Glomski, S.A.; Wortman, J.R.; Uyeda, J.W.; Sodickson, A.D. Dual energy CT for evaluation of polycystic kidneys: A multi reader study of interpretation time and diagnostic confidence. Abdom. Radiol. 2018, 43, 3418–3424. [Google Scholar] [CrossRef] [PubMed]
- Husarik, D.B.; Gordic, S.; Desbiolles, L.; Krauss, B.; Leschka, S.; Wildermuth, S.; Alkadhi, H. Advanced virtual monoenergetic computed tomography of hyperattenuating and hypoattenuating liver lesions: Ex-vivo and patient experience in various body sizes. Invest. Radiol. 2015, 50, 695–702. [Google Scholar] [CrossRef] [Green Version]
- Altenbernd, J.; Forsting, M.; Lauenstein, T.; Wetter, A. Improved Image Quality and Detectability of Hypovascular Liver Metastases on DECT with Different Adjusted Window Settings. RoFo Fortschr. Auf Dem Geb. Der Rontgenstrahlen Und Der Nukl. 2017, 189, 228–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobsen, M.C.; Schellingerhout, D.; Wood, C.A.; Tamm, E.P.; Godoy, M.C.; Sun, J.; Cody, D.D. Intermanufacturer Comparison of Dual-Energy CT Iodine Quantification and Monochromatic Attenuation: A Phantom Study. Radiology 2018, 287, 224–234. [Google Scholar] [CrossRef] [Green Version]
- Jacobsen, M.C.; Cressman, E.N.K.; Tamm, E.P.; Baluya, D.L.; Duan, X.; Cody, D.D.; Schellingerhout, D.; Layman, R.R. Dual-Energy CT: Lower Limits of Iodine Detection and Quantification. Radiology 2019, 292, 414–419. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Phase | Arterial (GSI) | Portal Venous | Venous |
|---|---|---|---|
| Voltage | Dual-energy spectral mode (80/140 kVp) | Standard monoenergy mode (120 kVp) | |
| Postprocessing datasets | 1st: 70 keV (reference) 2nd: hybrid 140 keV/40 keV (50:50 blending) 3rd: hybrid 140 keV/iodine map (50:50 blending) | Standard polychromatic images | |
| Recon. ASIR-V level | 70% | ||
| Noise index (NI) | 21 | ||
| Pitch | 1.375 | ||
| Collimation | 64 × 0.625 mm | ||
| Rotation time | 0.7 s | ||
| Tube current | average: 260–640 mA | min/max: 100/500 mA | |
| Smart mA | on | ||
| Auto mA | off (not available from vendor) | on | |
| Recon mode | slice (axial) | ||
| Recon slice thickness | 0.625 mm | ||
| Recon section interval | 0.625 mm | ||
| Field of view | DFOV: depending on patient SFOV: 50 cm | ||
| Confidence | Artifacts | Noise | Contrast | Suspicious Lesions | Small Structures | |
|---|---|---|---|---|---|---|
| 1st Set Kendall’s tau-b p-value | 0.833 <0.001 | 0.760 <0.001 | 0.848 <0.001 | 0.812 <0.001 | 0.806 <0.001 | 0.940 <0.001 |
| 2st Set Kendall’s tau-b p-value | 0.862 <0.001 | 0.841 <0.001 | 0.701 <0.001 | 0.972 <0.001 | 0.887 <0.001 | 0.693 <0.001 |
| 3st Set Kendall’s tau-b p-value | 0.909 <0.001 | 0.860 <0.001 | 0.814 <0.001 | 0.914 <0.001 | 0.818 <0.001 | 0.828 <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auer, T.A.; Feldhaus, F.W.; Büttner, L.; Jonczyk, M.; Fehrenbach, U.; Geisel, D.; Böning, G. Spectral CT Hybrid Images in the Diagnostic Evaluation of Hypervascular Abdominal Tumors—Potential Advantages in Clinical Routine. Diagnostics 2021, 11, 1539. https://doi.org/10.3390/diagnostics11091539
Auer TA, Feldhaus FW, Büttner L, Jonczyk M, Fehrenbach U, Geisel D, Böning G. Spectral CT Hybrid Images in the Diagnostic Evaluation of Hypervascular Abdominal Tumors—Potential Advantages in Clinical Routine. Diagnostics. 2021; 11(9):1539. https://doi.org/10.3390/diagnostics11091539
Chicago/Turabian StyleAuer, Timo Alexander, Felix Wilhelm Feldhaus, Laura Büttner, Martin Jonczyk, Uli Fehrenbach, Dominik Geisel, and Georg Böning. 2021. "Spectral CT Hybrid Images in the Diagnostic Evaluation of Hypervascular Abdominal Tumors—Potential Advantages in Clinical Routine" Diagnostics 11, no. 9: 1539. https://doi.org/10.3390/diagnostics11091539
APA StyleAuer, T. A., Feldhaus, F. W., Büttner, L., Jonczyk, M., Fehrenbach, U., Geisel, D., & Böning, G. (2021). Spectral CT Hybrid Images in the Diagnostic Evaluation of Hypervascular Abdominal Tumors—Potential Advantages in Clinical Routine. Diagnostics, 11(9), 1539. https://doi.org/10.3390/diagnostics11091539