
MRI of the Entire Spinal Cord—Worth the While or Waste of Time? A Retrospective Study of 74 Patients with Multiple Sclerosis

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MRI Protocol
2.3. MRI Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Demographics and Clinical Findings
3.2. Brain MRI
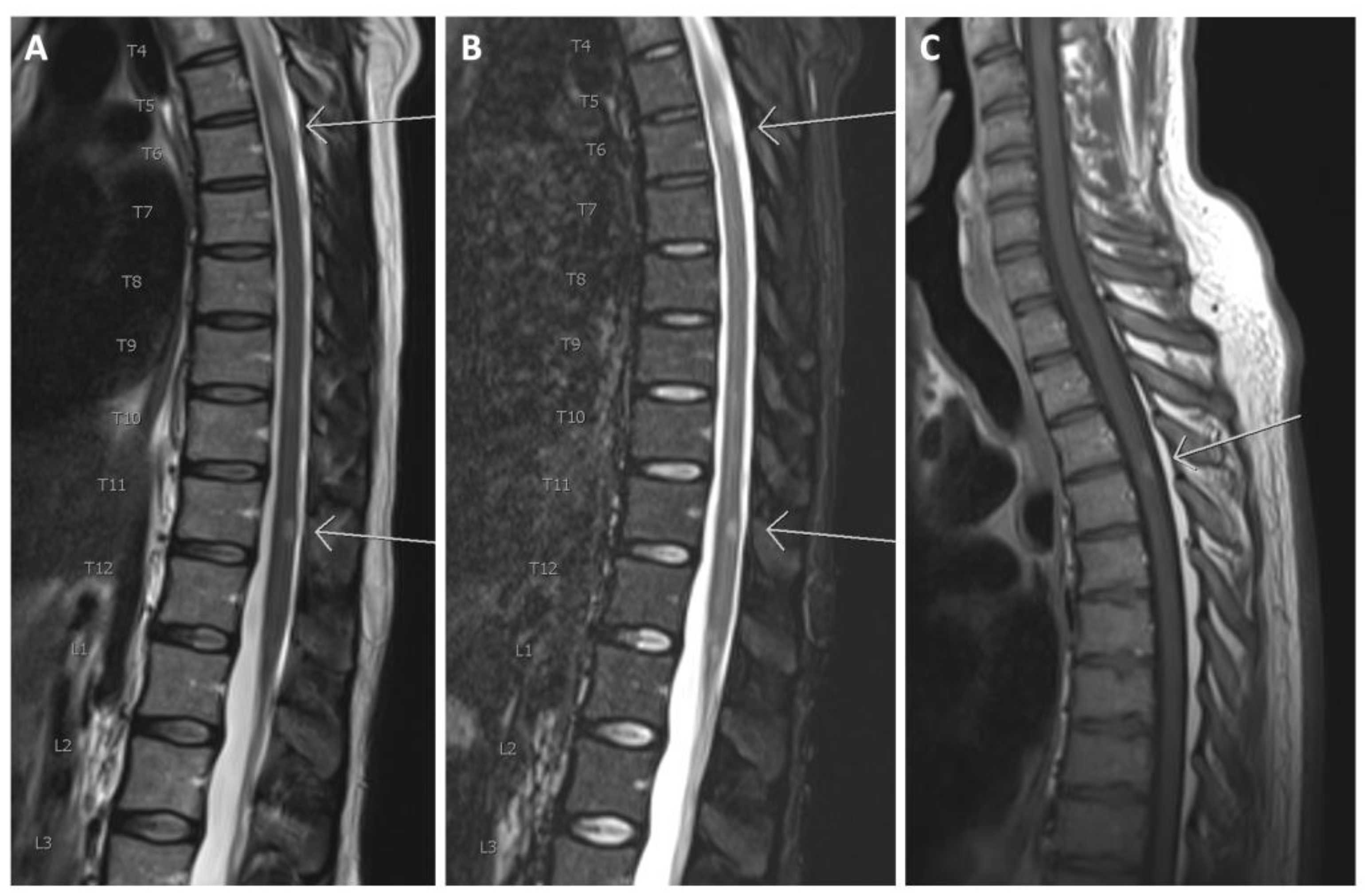
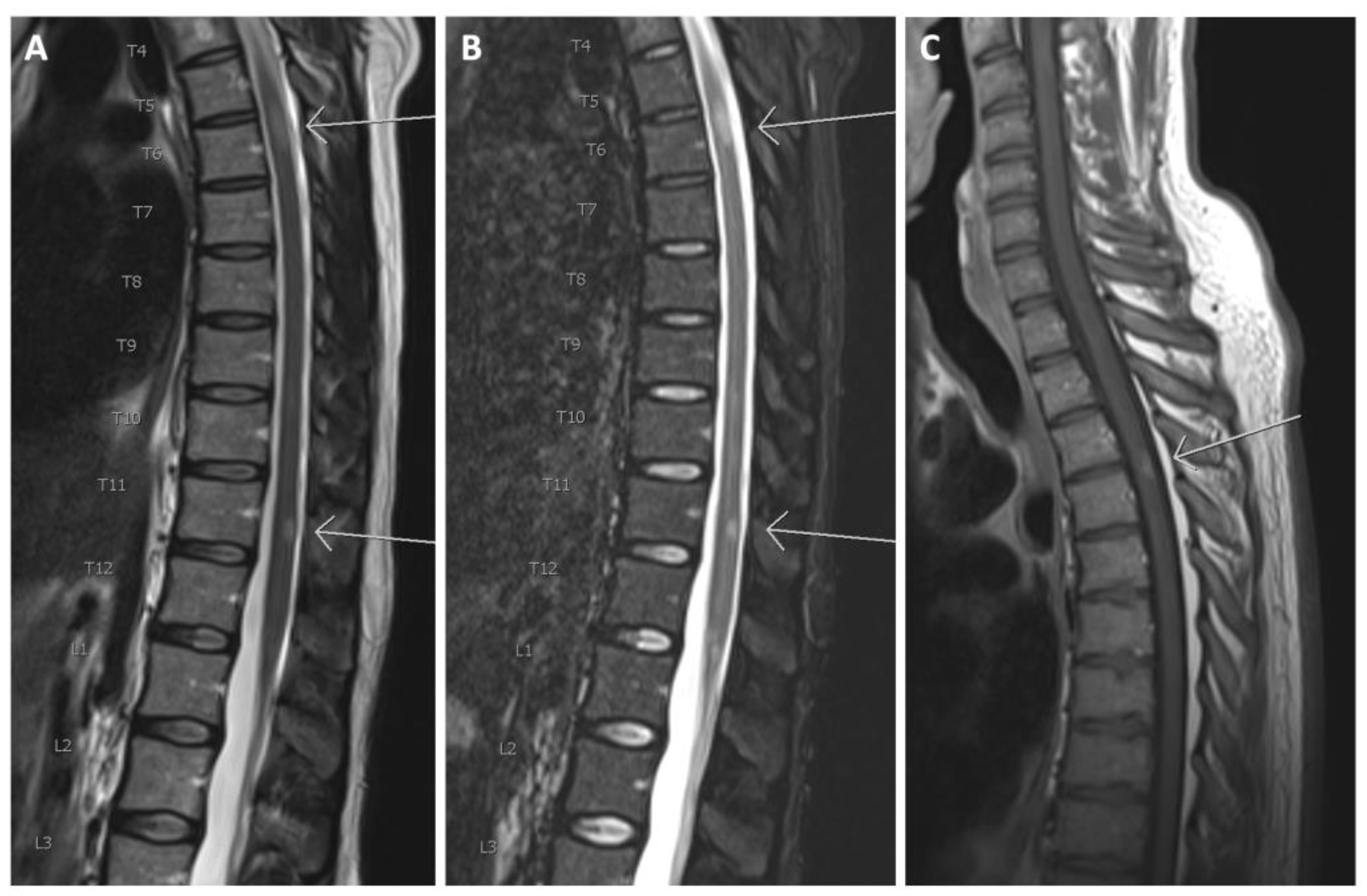
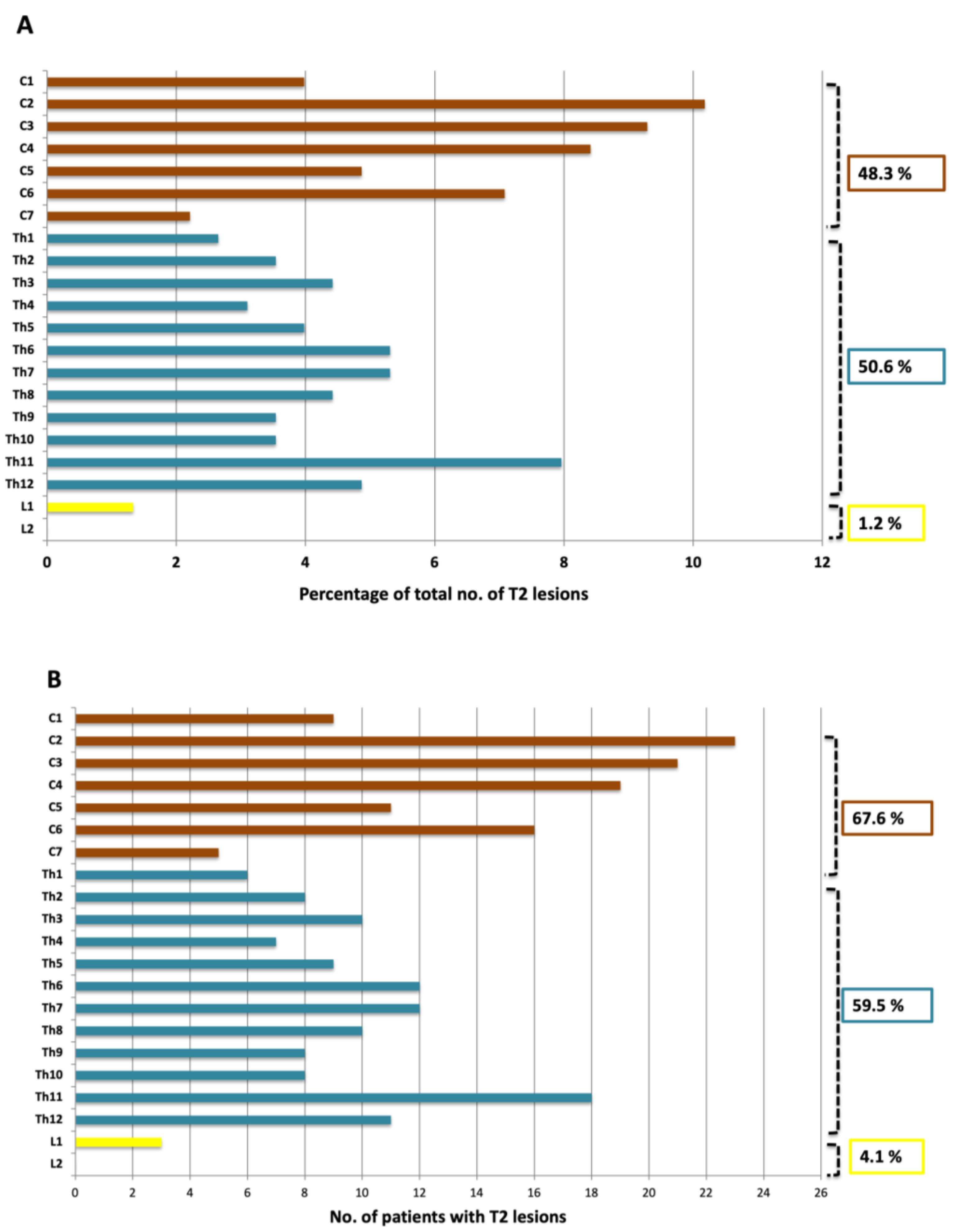
3.3. The Spinal Cord
3.4. Dissemination in Space and Time
3.5. EDSS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Y.; Haacke, E.M.; Bernitsas, E. Imaging of the Spinal Cord in Multiple Sclerosis: Past, Present, Future. Brain Sci. 2020, 10, 857. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Baranzini, S.E.; Geurts, J.; Hemmer, B.; Ciccarelli, O. Multiple sclerosis. Lancet 2018, 391, 1622–1636. [Google Scholar] [CrossRef]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- Kennedy, P.M. Impact of delayed diagnosis and treatment in clinically isolated syndrome and multiple sclerosis. J. Neurosci. Nurs. 2013, 45. [Google Scholar] [CrossRef] [PubMed]
- Lebrun-Frenay, C.; Kobelt, G.; Berg, J.; Capsa, D.; Gannedahl, M. New insights into the burden and costs of multiple sclerosis in Europe: Results for France. Mult. Scler. J. 2017, 23, 65–77. [Google Scholar] [CrossRef]
- Kobelt, G.; Thompson, A.; Berg, J.; Gannedahl, M.; Eriksson, J. New insights into the burden and costs of multiple sclerosis in Europe. Mult. Scler. 2017, 23, 1123–1136. [Google Scholar] [CrossRef]
- Faissner, S.; Gold, R. Efficacy and Safety of the Newer Multiple Sclerosis Drugs Approved Since 2010. CNS Drugs 2018, 32, 269–287. [Google Scholar] [CrossRef]
- Tuohy, O.; Costelloe, L.; Hill-Cawthorne, G.; Bjornson, I.; Harding, K.; Robertson, N.; May, K.; Button, T.; Azzopardi, L.; Kousin-Ezewu, O.; et al. Alemtuzumab treatment of multiple sclerosis: Long-term safety and efficacy. J. Neurol. Neurosurg. Psychiatry 2015, 86, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Rovira, Á.; Wattjes, M.P.; Tintoré, M.; Tur, C.; Yousry, T.A.; Sormani, M.P.; De Stefano, N.; Filippi, M.; Auger, C.; Rocca, M.A.; et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis—Clinical implementation in the diagnostic process. Nat. Rev. Neurol. 2015, 11, 471–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, W.I.; Compston, A.; Edan, G.; Goodkin, D.; Hartung, H.P.; Lublin, F.D.; McFarland, H.F.; Paty, D.W.; Polman, C.H.; Reingold, S.C.; et al. Recommended diagnostic criteria for multiple sclerosis: Guidelines from the International Panel on the Diagnosis of Multiple Sclerosis. Ann. Neurol. 2001, 50, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Vattoth, S.; Kadam, G.H.; Gaddikeri, S. Revised McDonald Criteria, MAGNIMS Consensus and Other Relevant Guidelines for Diagnosis and Follow Up of MS: What Radiologists Need to Know? Curr. Probl. Diagn. Radiol. 2021, 50, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Oztek, M.A.; Brunnquell, C.L.; Hoff, M.N.; Boulter, D.J.; Mossa-Basha, M.; Beauchamp, L.H.; Haynor, D.L.; Nguyen, X.V. Practical Considerations for Radiologists in Implementing a Patient-friendly MRI Experience. Top. Magn. Reson. Imaging 2020, 29, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Olsson, A.; Gustavsen, S.; Hasselbalch, I.C.; Langkilde, A.R.; Sellebjerg, F.; Oturai, A.B.; Søndergaard, H.B. Biomarkers of inflammation and epithelial barrier function in multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 46, 102520. [Google Scholar] [CrossRef] [PubMed]
- Olsson, A.; Gustavsen, S.; Nguyen, T.D.; Nyman, M.; Langkilde, A.R.; Hansen, T.H.; Sellebjerg, F.; Oturai, A.B.; Bach Søndergaard, H. Serum Short-Chain Fatty Acids and Associations With Inflammation in Newly Diagnosed Patients With Multiple Sclerosis and Healthy Controls. Front. Immunol. 2021, 12, 661493. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Weier, K.; Mazraeh, J.; Naegelin, Y.; Thoeni, A.; Hirsch, J.G.; Fabbro, T.; Bruni, N.; Duyar, H.; Bendfeldt, K.; Radue, E.W.; et al. Biplanar MRI for the assessment of the spinal cord in multiple sclerosis. Mult. Scler. J. 2012, 18, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Bag, A.K.; Patel, B.N.; Osman, S.; Roberson, G.H. Clinico-radiologic profile of spinal cord multiple sclerosis in adults. Neuroradiol. J. 2011, 24, 511–518. [Google Scholar] [CrossRef]
- Nair, G.; Absinta, M.; Reich, D.S. Optimized T1-MPRAGE sequence for better visualization of spinal cord multiple sclerosis lesions at 3T. Am. J. Neuroradiol. 2013, 34, 2215–2222. [Google Scholar] [CrossRef]
- Bot, J.C.J.; Barkhof, F.; Polman, C.H.; Lycklama À Nijeholt, G.J.; De Groot, V.; Bergers, E.; Ader, H.J.; Castelijns, J.A. Spinal cord abnormalities in recently diagnosed MS patients: Added value of spinal MRI examination. Neurology 2004, 62, 226–233. [Google Scholar] [CrossRef]
- Qiu, W.; Raven, S.; James, I.; Luo, Y.; Wu, J.; Castley, A.; Christiansen, F.T.; Carroll, W.M.; Mastaglia, F.L.; Kermode, A.G. Spinal cord involvement in multiple sclerosis: A correlative MRI and high-resolution HLA-DRB1 genotyping study. J. Neurol. Sci. 2011, 300, 114–119. [Google Scholar] [CrossRef]
- Hua, L.H.; Donlon, S.L.; Sobhanian, M.J.; Portner, S.M.; Okuda, D.T. Thoracic spinal cord lesions are influenced by the degree of cervical spine involvement in multiple sclerosis. Spinal Cord 2015, 53, 520–525. [Google Scholar] [CrossRef] [Green Version]
- De Leener, B.; Taso, M.; Cohen-Adad, J.; Callot, V. Segmentation of the human spinal cord. Magn. Reson. Mater. Phys. Biol. Med. 2016, 29, 125–153. [Google Scholar] [CrossRef]
- Jacobi, C.; Hähnel, S.; Martinez-Torres, F.; Rieger, S.; Jüttler, E.; Heiland, S.; Jarius, S.; Meyding-Lamadè, U.; Storch-Hagenlocher, B.; Wildemann, B. Prospective combined brain and spinal cord MRI in clinically isolated syndromes and possible early multiple sclerosis: Impact on dissemination in space and time. Eur. J. Neurol. 2008, 15, 1359–1364. [Google Scholar] [CrossRef]
- Solomon, A.J.; Pettigrew, R.; Naismith, R.T.; Chahin, S.; Krieger, S.; Weinshenker, B. Challenges in multiple sclerosis diagnosis: Misunderstanding and misapplication of the McDonald criteria. Mult. Scler. J. 2021, 27, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Eden, D.; Gros, C.; Badji, A.; Dupont, S.M.; De Leener, B.; Maranzano, J.; Zhuoquiong, R.; Liu, Y.; Granberg, T.; Ouellette, R.; et al. Spatial distribution of multiple sclerosis lesions in the cervical spinal cord. Brain 2019, 142, 633–646. [Google Scholar] [CrossRef] [PubMed]
- Lycklama, G.; Thompson, A.; Filippi, M.; Miller, D.; Polman, C.; Fazekas, F.; Barkhof, F. Spinal-cord MRI in multiple sclerosis. Lancet Neurol. 2003, 2, 555–562. [Google Scholar] [CrossRef]
- Pravatà, E.; Valsasina, P.; Gobbi, C.; Zecca, C.; Riccitelli, G.; Filippi, M.; Rocca, M.A. Influence of CNS T2-focal lesions on cervical cord atrophy and disability in multiple sclerosis. Mult. Scler. J. 2020, 26, 1402–1409. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T2 Lesions | |||
|---|---|---|---|
| Patients, n | Pct. of Total | Median EDSS Score | |
| Total Number of Patients: | 74 | 100 | 2 |
| No. of lesions: | |||
| <10 | 23 | 31.0 | 1.5 |
| 10–20 | 21 | 28.4 | 2 |
| >20 | 30 | 40.5 | 2.5 |
| Location: | |||
| Periventricular | 72 | 97.3 | 2 |
| Infratentorial | 51 | 68.0 | 2 |
| Juxtacortical/cortical | 44 | 59.5 | 2 |
| Gadolinium-enhancing lesions | |||
| Patients, n | Pct. of total | ||
| Patients receiving contrast (brain + spinal cord): | 65 | - | |
| Patients with enhancing lesions: | 17 | 26.2 | |
| Number of lesions | |||
| Gadolinium-enhancing lesions: | 60 | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poulsen, E.N.; Olsson, A.; Gustavsen, S.; Langkilde, A.R.; Oturai, A.B.; Carlsen, J.F. MRI of the Entire Spinal Cord—Worth the While or Waste of Time? A Retrospective Study of 74 Patients with Multiple Sclerosis. Diagnostics 2021, 11, 1424. https://doi.org/10.3390/diagnostics11081424
Poulsen EN, Olsson A, Gustavsen S, Langkilde AR, Oturai AB, Carlsen JF. MRI of the Entire Spinal Cord—Worth the While or Waste of Time? A Retrospective Study of 74 Patients with Multiple Sclerosis. Diagnostics. 2021; 11(8):1424. https://doi.org/10.3390/diagnostics11081424
Chicago/Turabian StylePoulsen, Esben Nyborg, Anna Olsson, Stefan Gustavsen, Annika Reynberg Langkilde, Annette Bang Oturai, and Jonathan Frederik Carlsen. 2021. "MRI of the Entire Spinal Cord—Worth the While or Waste of Time? A Retrospective Study of 74 Patients with Multiple Sclerosis" Diagnostics 11, no. 8: 1424. https://doi.org/10.3390/diagnostics11081424
APA StylePoulsen, E. N., Olsson, A., Gustavsen, S., Langkilde, A. R., Oturai, A. B., & Carlsen, J. F. (2021). MRI of the Entire Spinal Cord—Worth the While or Waste of Time? A Retrospective Study of 74 Patients with Multiple Sclerosis. Diagnostics, 11(8), 1424. https://doi.org/10.3390/diagnostics11081424