
Pericardial NT-Pro-BNP and GDF-15 as Biomarkers of Atrial Fibrillation and Atrial Matrix Remodeling in Aortic Stenosis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Endpoints
2.4. Sample Collection and Preparation
2.5. GDF-15 and NT-Pro-BNP
2.6. Histomorphometric Quantification
2.7. Gene Expression Analysis
2.8. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Baseline Echocardiographic Assessment
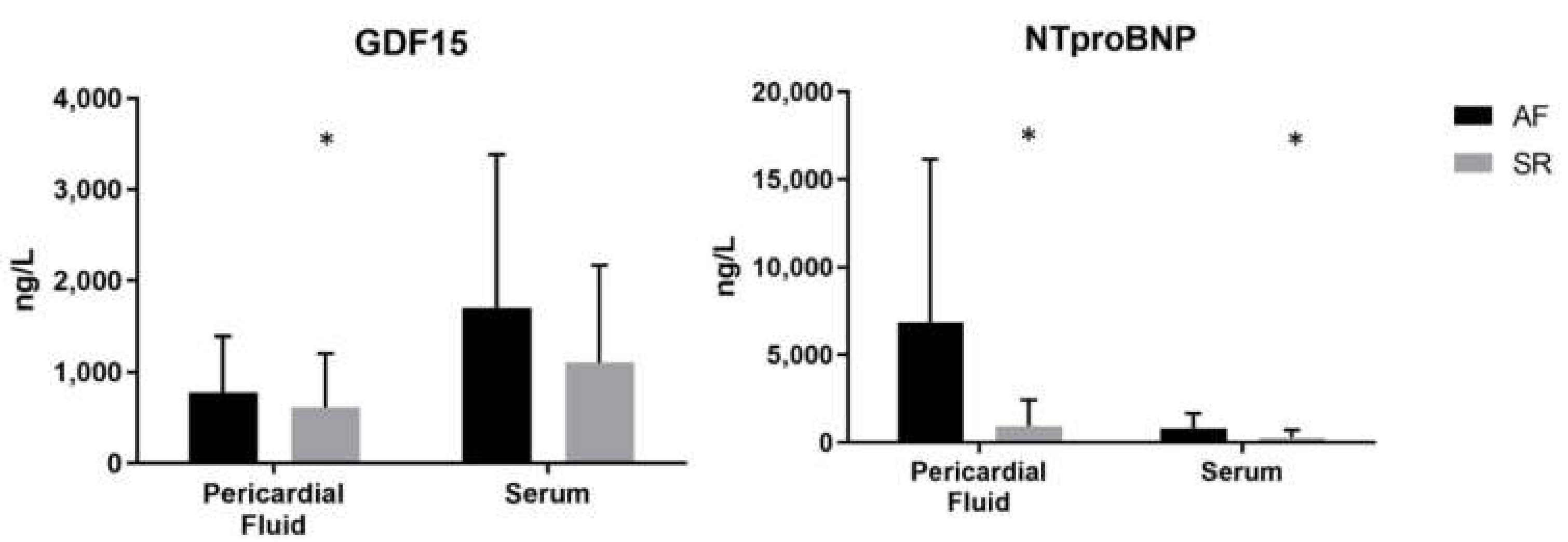
3.3. Pericardial Fluid and Serum GDF-15 and NT-Pro-BNP
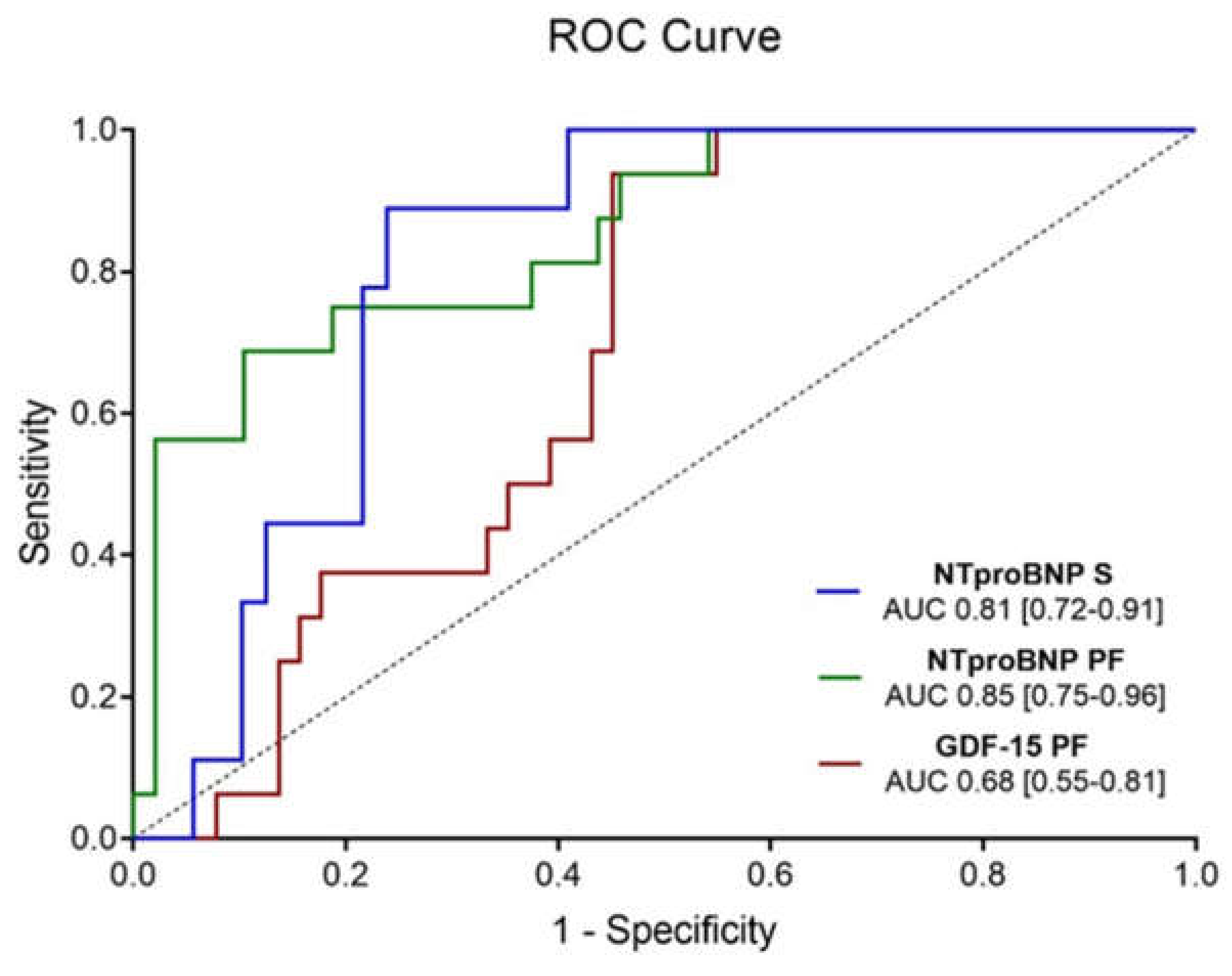
3.3.1. Atrial Fibrillation
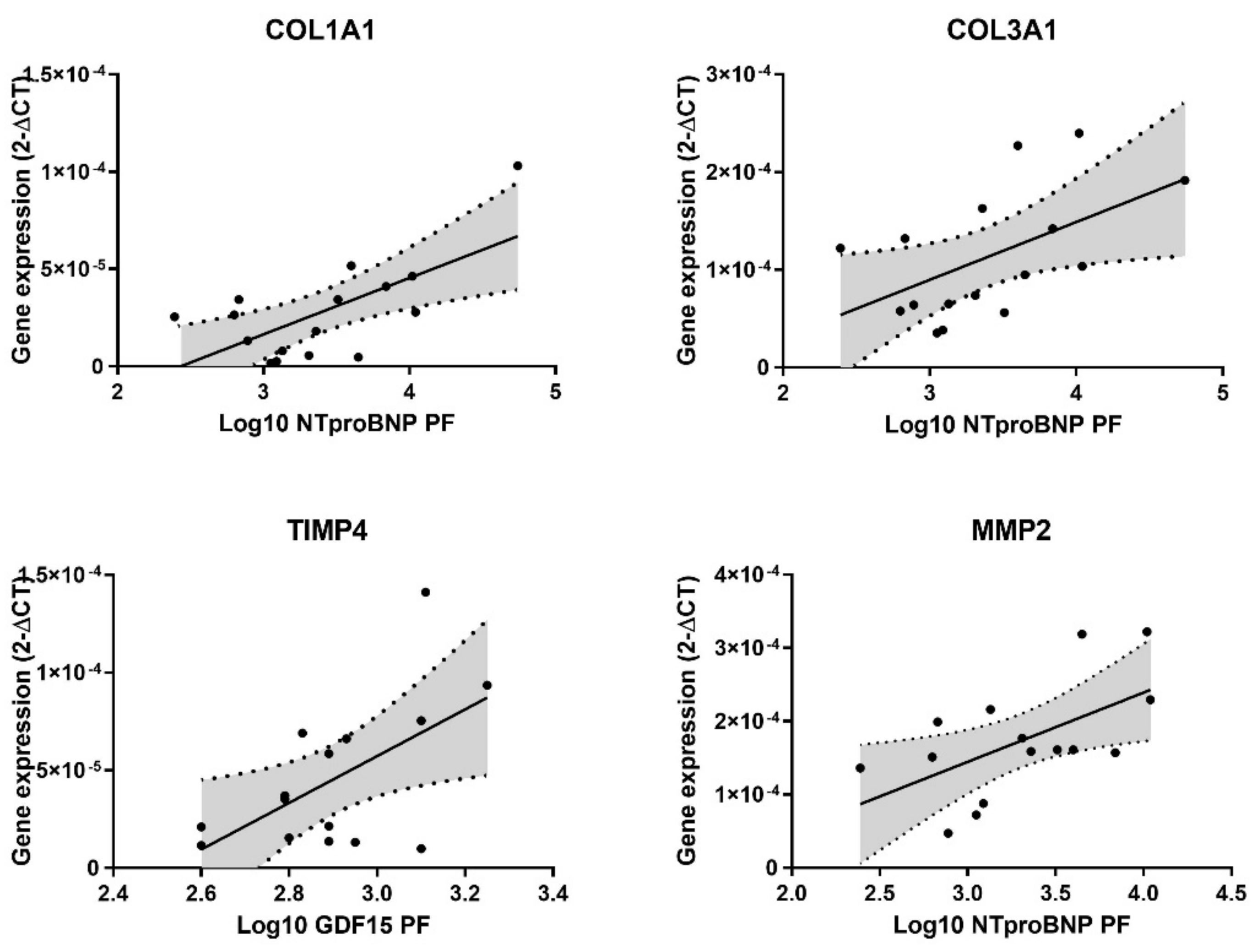
3.3.2. Atrial Matrix Remodeling
3.4. Thirty-Day Postoperative Outcomes
3.4.1. Atrial Fibrillation
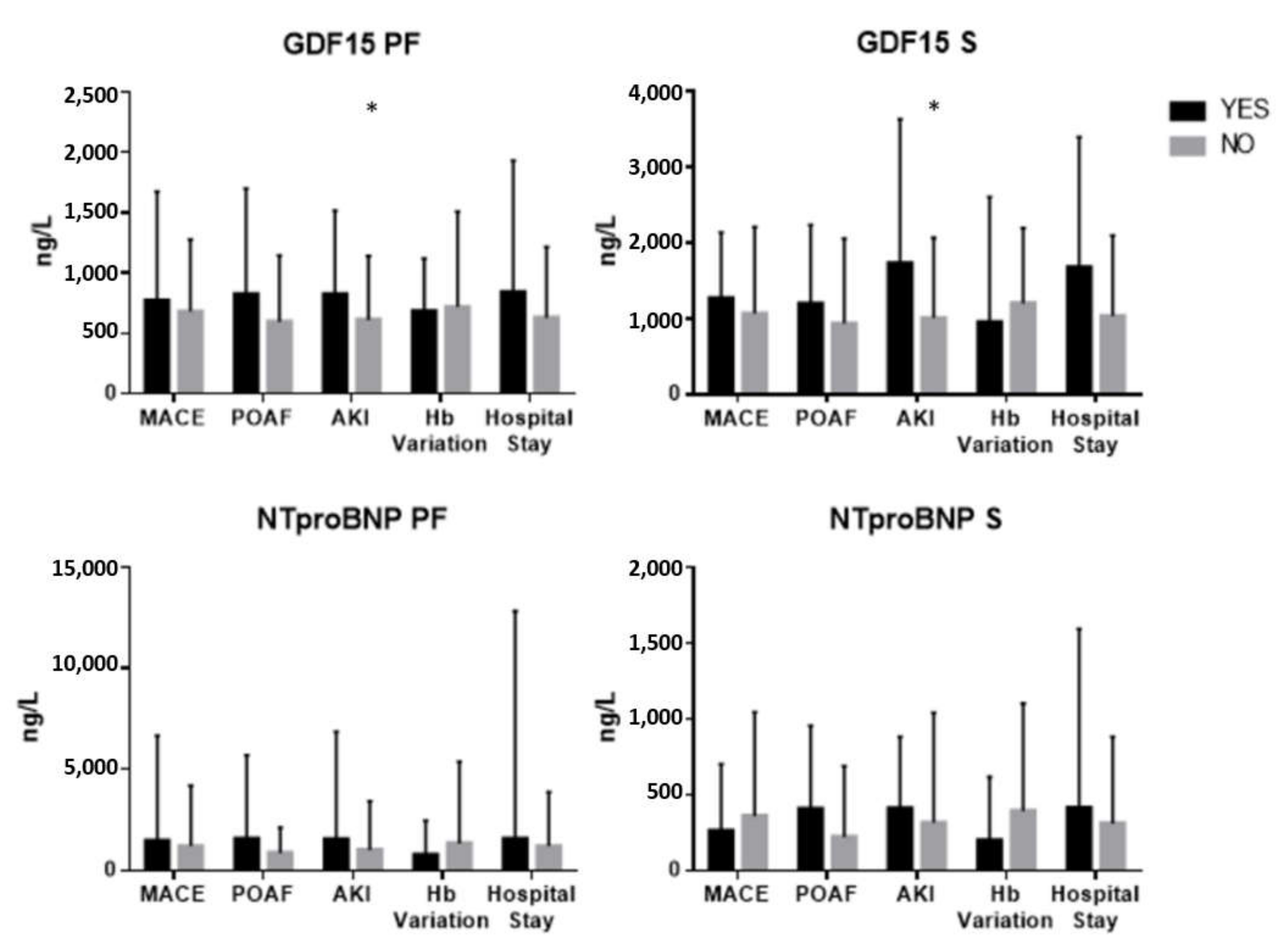
3.4.2. Pericardial Fluid and Serum GDF-15 and NT-Pro-BNP
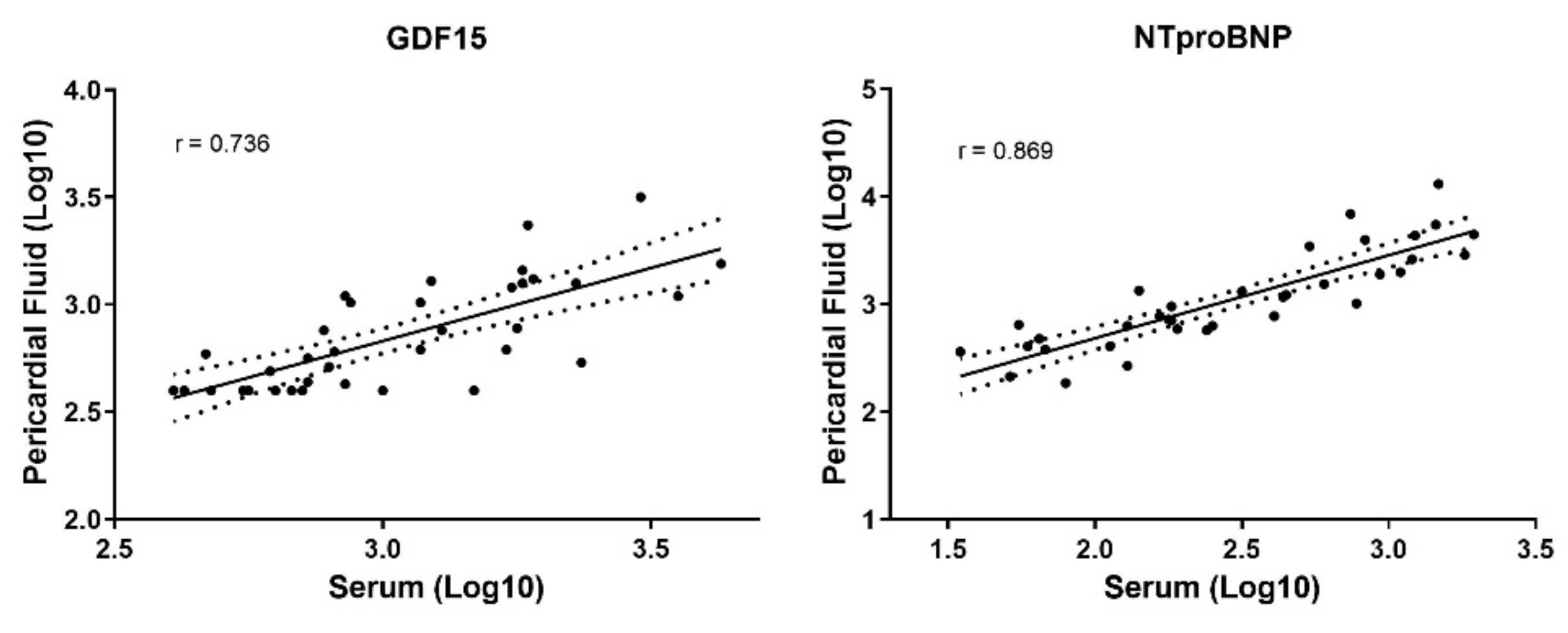
3.5. Comparison between Pericardial Fluid and Serum Measurements
4. Discussion
4.1. GDF-15 in Atrial Fibrillation
4.2. GDF-15 in Pericardial Fluid
4.3. GDF-15 and Extracellular Matrix Remodeling
4.4. NT-Pro-BNP in Atrial Fibrillation
4.5. NT-Pro-BNP in Pericardial Fluid and Atrial Matrix Remodeling
4.6. GDF-15 and Acute Kidney Injury
4.7. Translational Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AF | Atrial Fibrillation |
| AKI | Acute Kidney Injury |
| AMG | Aortic Valve Maximum Gradient |
| AMeanG | Aortic Valve Mean Gradient |
| AUROC | Area Under the Receiver Operating Curve |
| AVA | Aortic Valve Area |
| AVR | Aortic Valve Replacement |
| BNP | Brain Natriuretic Peptide |
| CAD | Coronary Artery Disease |
| CLD | Chronic Lung Disease |
| COL1A1 | Type I Collagen Gene |
| COL3A1 | Type III Collagen Gene |
| EKG | Electrocardiogram |
| GDF-15 | Growth Differentiation Factor 15 |
| Hb | Hemoglobin |
| IQR | Interquartil Range |
| IVS | Interventricular Septum |
| LAD | Left Atrium Diameter |
| LOS | Length of Stay |
| LVED | Left Ventricle End-diastolic Diameter |
| LVPW | Left Ventricle Posterior Wall |
| MMP | Matrix Metalloproteinase |
| NYHA | New York Heart Association |
| POAF | Postoperative Atrial Fibrillation |
| Sd | Standard Deviation |
| TIMP | Tissue Inhibitor of Matrix Metalloproteinase |
References
- Oliveira, J.P.; Fragão-marques, M. Adverse remodeling in atrial fibrillation following isolated aortic valve replacement surgery. Perfusion 2021, 36, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56-e528. [Google Scholar] [CrossRef]
- Andrade, J.; Khairy, P.; Dobrev, D.; Nattel, S. The Clinical Profile and Pathophysiology of Atrial Fibrillation. Circ. Res. 2014, 114, 1453–1468. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Mojoli, M.; Urena, M.; Vahanian, A. Atrial fibrillation in patients undergoing transcatheter aortic valve implantation: Epidemiology, timing, predictors, and outcome. Eur. Heart J. 2017, 38, 1285–1293. [Google Scholar] [CrossRef]
- Hijazi, Z.; Oldgren, J.; Lindbäck, J.; Alexander, J.H.; Connolly, S.J.; Eikelboom, J.W.; Ezekowitz, M.D.; Held, C.; Hylek, E.M.; Lopes, R.D.; et al. The novel biomarker-based ABC (age, biomarkers, clinical history)-bleeding risk score for patients with atrial fibrillation: A derivation and validation study. Lancet 2016, 387, 2302–2311. [Google Scholar] [CrossRef]
- Lind, L.; Sundström, J.; Stenemo, M.; Hagström, E.; Ärnlöv, J. Discovery of new biomarkers for atrial fibrillation using a custom-made proteomics chip. Heart 2017, 103, 377–382. [Google Scholar] [CrossRef]
- Bouchot, O.; Guenancia, C.; Kahli, A.; Pujos, C.; Malapert, G.; Vergely, C.; Laurent, G. Low Circulating Levels of Growth Differentiation Factor-15 before Coronary Artery Bypass Surgery May Predict Postoperative Atrial Fibrillation. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Bening, C.; Mazalu, E.A.; Yaqub, J.; Alhussini, K.; Glanowski, M.; Kottmann, T.; Leyh, R. Atrial contractility and fibrotic biomarkers are associated with atrial fibrillation after elective coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2019, 59, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wu, L.; Zheng, L.; Ding, L.; Chen, G.; Fan, X.; Yao, Y. Associations between multiple circulating biomarkers and the presence of atrial fibrillation in hypertrophic cardiomyopathy with or without left ventricular outflow tract obstruction. Int. Heart J. 2019, 60, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Xu, H.; Zhang, H.; Liu, Q.; Ye, Y.; Hao, J.; Zhao, Q.; Qi, X.; Liu, S.; Zhang, E.; et al. Prognostic Value of N-Terminal Pro–B-Type Natriuretic Peptide in Elderly Patients with Valvular Heart Disease. J. Am. Coll. Cardiol. 2020, 75, 1659–1672. [Google Scholar] [CrossRef]
- Trindade, F.; Vitorino, R.; Leite-Moreira, A.; Falcão-Pires, I. Pericardial fluid: An underrated molecular library of heart conditions and a potential vehicle for cardiac therapy. Basic Res. Cardiol. 2019, 114, 10. [Google Scholar] [CrossRef]
- Iskandar, R.; Liu, S.; Xiang, F.; Chen, W.; Li, L.; Qin, W.; Huang, F.; Chen, X. Expression of pericardial fluid T-cells and related inflammatory cytokines in patients with chronic heart failure. Exp. Ther. Med. 2017, 13, 1850–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guclu, O.; Karahan, O.; Karabacak, M.; Yuksel, V.; Huseyin, S.; Mavitas, B. Evaluation of Pericardial Fluid C-Type Natriuretic Peptide Levels in Patients Undergoing Coronary Bypass Surgery. Thorac. Cardiovasc. Surg. 2017, 65, 311–314. [Google Scholar] [PubMed]
- Dolgin, M.; Association, N.Y.H.; Fox, A.C.; Gorlin, R.; Levin, R.I.; Criteria Committee. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, 9th ed.; Lippincott Williams Wilkins: Boston, MA, USA, 1994. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the European association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anke, S.D. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Pol. Heart J. 2016, 74, 1037–1147. [Google Scholar]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [Green Version]
- Fragão-Marques, M.; Mancio, J.; Oliveira, J.; Falcão-Pires, I.; Leite-Moreira, A. Gender Differences in Predictors and Long-Term Mortality of New-Onset Postoperative Atrial Fibrillation Following Isolated Aortic Valve Replacement Surgery. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 342. [Google Scholar] [CrossRef]
- Fragão-Marques, M.; Miranda, I.; Martins, D.; Barroso, I.; Mendes, C.; Pereira-Neves, A.; Falcão-Pires, I.; Leite-Moreira, A. Atrial matrix remodeling in atrial fibrillation patients with aortic stenosis. BMC Cardiovasc. Disord. 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hua, R.; Adamczyk, A.; Robbins, C.; Ray, G.; Rose, R.A. Distinct Patterns of Constitutive Phosphodiesterase Activity in Mouse Sinoatrial Node and Atrial Myocardium. PLoS ONE 2012, 7, e47652. [Google Scholar] [CrossRef] [Green Version]
- Wallentin, L.; Hijazi, Z.; Andersson, U.; Alexander, J.H.; De Caterina, R.; Hanna, M.; Horowitz, J.D.; Hylek, E.M.; Lopes, R.D.; Åsberg, S.; et al. Growth differentiation factor 15, a marker of oxidative stress and inflammation, for risk assessment in patients with atrial fibrillation: Insights from the Apixaban for reduction in stroke and other thromboembolic events in atrial fibrillation (ARISTOTLE) trial. Circulation 2014, 130, 1847–1858. [Google Scholar]
- Chan, M.M.Y.; Santhanakrishnan, R.; Chong, J.P.C.; Chen, Z.; Tai, B.C.; Liew, O.W.; Ng, T.P.; Ling, L.H.; Sim, D.; Leong, K.T.G.; et al. Growth differentiation factor 15 in heart failure with preserved vs. reduced ejection fraction. Eur. J. Heart Fail. 2016, 18, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Santema, B.T.; Chan, M.M.Y.; Tromp, J.; Dokter, M.; van der Wal, H.H.; Emmens, J.E.; Takens, J.; Samani, N.J.; Ng, L.L.; Lang, C.C.; et al. The influence of atrial fibrillation on the levels of NT-proBNP versus GDF-15 in patients with heart failure. Clin. Res. Cardiol. 2020, 109, 331–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rienstra, M.; Yin, X.; Larson, M.G.; Fontes, J.D.; Magnani, J.W.; McManus, D.D.; McCabe, E.L.; Coglianese, E.E.; Amponsah, M.; Ho, J.E.; et al. Relation between soluble ST2, growth differentiation factor-15, and high-sensitivity troponin i and incident atrial fibrillation. Am. Heart J. 2014, 167, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Biancotto, A.; Ruin Moaddel, R.; Moore, Z.; Gonzalez-Freire, M.; Aon, M.A.; Candia, J.; Zhang, P.; Cheung, F.; Fantoni, G.; et al. Plasma proteomic signature of age in healthy humans. Aging Cell 2018, 17, e12799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benes, J.; Kotrc, M.; Wohlfahrt, P.; Conrad, M.J.; Franekova, J.; Jabor, A.; Lupinek, P.; Kautzner, J.; Melenovsky, V.; Jarolim, P. The Role of GDF-15 in Heart Failure Patients with Chronic Kidney Disease. Can. J. Cardiol. 2019, 35, 462–470. [Google Scholar] [CrossRef]
- Yuan, Z.; Li, H.; Sun, Y.; Qiu, J.; Xu, H.; Liu, J.; Zhou, M.; Chen, A.; Ye, X.; Wang, Z.; et al. Pericardial fluid levels of growth differentiation factor 15 in patients with or without coronary artery disease: A prospective study. Ann. Transl. Med. 2020, 8, 113. [Google Scholar]
- Sun, Y.; Huang, Z.Y.; Wang, Z.H.; Li, C.P.; Meng, X.L.; Zhang, Y.J.; Su, F.; Ma, N. TGF-β1 and TIMP-4 regulate atrial fibrosis in atrial fibrillation secondary to rheumatic heart disease. Mol. Cell. Biochem. 2015, 406, 131–138. [Google Scholar] [CrossRef]
- Wakula, P.; Neumann, B.; Kienemund, J.; Thon-Gutschi, E.; Stojakovic, T.; Manninger, M.; Scherr, D.; Scharnagl, H.; Kapl, M.; Pieske, B.; et al. CHA2DS2-VASc score and blood biomarkers to identify patients with atrial high-rate episodes and paroxysmal atrial fibrillation. Europace 2017, 19, 544–551. [Google Scholar] [CrossRef]
- Nair, N.; Gongora, E. Correlations of GDF-15 with sST2, MMPs, and worsening functional capacity in idiopathic dilated cardiomyopathy: Can we gain new insights into the pathophysiology? J. Circ. Biomarkers 2018, 7, 1849454417751735. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.M.; Li, M.J.; Zhou, Y.L.; Ma, L.L.; Yi, X. Growth differentiation factor-15 (GDF-15), novel biomarker for assessing atrial fibrosis in patients with atrial fibrillation and rheumatic heart disease. Int. J. Clin. Exp. Med. 2015, 8, 21201–21207. [Google Scholar] [PubMed]
- Thaman, R.; Esteban, M.T.; Barnes, S.; Gimeno, J.R.; Mist, B.; Murphy, R.; Collinson, P.O.; McKenna, W.J.; Elliott, P.M. Usefulness of N-Terminal Pro-B-Type Natriuretic Peptide Levels to Predict Exercise Capacity in Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2006, 98, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Michaud, K.; Augsburger, M.; Donzé, N.; Sabatasso, S.; Faouzi, M.; Bollmann, M.; Mangin, P. Evaluation of postmortem measurement of NT-proBNP as a marker for cardiac function. Int. J. Legal Med. 2008, 122, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Tziakas, D.N.; Chalikias, G.K.; Hatzinikolaou, E.I.; Stakos, D.A.; Tentes, I.K.; Kortsaris, A.; Hatseras, D.I.; Kaski, J.C. N-terminal pro-B-type natriuretic peptide and matrix metalloproteinases in early and late left ventricular remodeling after acute myocardial infarction. Am. J. Cardiol. 2005, 96, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Xue, L.; Wu, Y.; Ma, H.; Chen, L.; Wang, X.; Zhu, Q.; Dai, N.; Chen, Y. Natriuretic peptides and right atrial fibrosis in patients with paroxysmal versus persistent atrial fibrillation. Peptides 2010, 31, 1531–1539. [Google Scholar] [CrossRef]
- Lin, C.S.; Pan, C.H. Regulatory mechanisms of atrial fibrotic remodeling in atrial fibrillation. Cell. Mol. Life Sci. 2008, 65, 1489–1508. [Google Scholar] [CrossRef]
- Hijazi, Z.; Verdecchia, P.; Oldgren, J.; Andersson, U.; Reboldi, G.; Di Pasquale, G.; Mazzotta, G.; Angeli, F.; Eikelboom, J.W.; Ezekowitz, M.D.; et al. Cardiac Biomarkers and Left Ventricular Hypertrophy in Relation to Outcomes in Patients with Atrial Fibrillation: Experiences From the RE-LY Trial. J. Am. Heart Assoc. 2019, 8, e010107. [Google Scholar] [CrossRef] [Green Version]
- Heringlake, M.; Charitos, E.I.; Erber, K.; Berggreen, A.E.; Heinze, H.; Paarmann, H. Preoperative plasma growth-differentiation factor-15 for prediction of acute kidney injury in patients undergoing cardiac surgery. Crit. Care 2016, 20, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Guenancia, C.; Kahli, A.; Laurent, G.; Hachet, O.; Malapert, G.; Grosjean, S.; Girard, C.; Vergely, C.; Bouchot, O. Pre-operative growth differentiation factor 15 as a novel biomarker of acute kidney injury after cardiac bypass surgery. Int. J. Cardiol. 2015, 197, 66–71. [Google Scholar] [CrossRef]
- Ho, J.E.; Hwang, S.-J.; Wollert, K.C.; Larson, M.G.; Cheng, S.; Kempf, T.; Vasan, R.S.; Januzzi, J.L.; Wang, T.J.; Fox, C.S. Biomarkers of Cardiovascular Stress and Incident Chronic Kidney Disease. Clin. Chem. 2013, 59, 1613–1620. [Google Scholar] [CrossRef] [Green Version]
- Lajer, M.; Jorsal, A.; Tarnow, L.; Parving, H.H.; Rossing, P. Plasma growth differentiation factor-15 independently predicts all-cause and cardiovascular mortality as well as deterioration of kidney function in type 1 diabetic patients with nephropathy. Diabetes Care 2010, 33, 1567–1572. [Google Scholar] [CrossRef] [Green Version]
- Zimmers, T.A.; Jin, X.; Hsiao, E.C.; McGrath, S.A.; Esquela, A.F.; Koniaris, L.G. Growth differentiation factor-15/macrophage inhibitory cytokine-1 induction after kidney and lung injury. Shock 2005, 23, 543–548. [Google Scholar] [PubMed]
- Azevedo, C.F.; Nigri, M.; Higuchi, M.L.; Pomerantzeff, P.M.; Spina, G.S.; Sampaio, R.O.; Tarasoutchi, F.; Grinberg, M.; Rochitte, C.E. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J. Am. Coll. Cardiol. 2010, 56, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Dzeshka, M.S.; Lip, G.Y.H.; Snezhitskiy, V.; Shantsila, E. Cardiac Fibrosis in Patients with Atrial Fibrillation: Mechanisms and Clinical Implications. J. Am. Coll. Cardiol. 2015, 66, 943–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable [%(n)] | Total (n = 126) | AF (n = 19) | SR (n = 107) | p Value |
|---|---|---|---|---|
| Age, years [mean ± sd] | 72.2 ± 8.4 | 74.0 ± 9.1 | 71.9 ± 8.3 | 0.306 |
| Gender | ||||
| Male | 48.4 (61) | 42.1 (8) | 49.5 (53) | 0.551 |
| Dyslipidemia | 66.7 (84) | 73.7 (14) | 67.3 (70) | 0.583 |
| Hypertension | 75.4 (95) | 72.2 (13) | 78.8 (82) | 0.532 |
| Diabetes Mellitus | 31.7 (40) | 26.3 (5) | 33.3 (35) | 0.547 |
| Chronic Lung Disease | 26.2 (33) | 26.3 (5) | 26.4 (28) | 0.993 |
| Smoking | 7.1 (9) | 0.0 (0) | 8.9 (9) | 0.352 |
| PAD | 0.8 (1) | 0.0 (0) | 1.0 (1) | 1.000 |
| CVD | 10.3 (13) | 11.1 (2) | 11.6 (11) | 1.000 |
| Previous AMI | 3.2 (4) | 0.0 (0) | 4.1 (4) | 1.000 |
| CAD | 18.3 (23) | 10.5 (2) | 21.2 (21) | 0.360 |
| NYHA ≥ II | 64.3 (81) | 75.0 (12) | 78.4 (69) | 0.749 |
| Angina | 17.5 (22) | 3.0 (20) | 19.0 (22.4) | 1.000 |
| Syncope/Lipothymia | 8.7 (11) | 0.0 (0) | 11.0 (12.9) | 0.209 |
| Basal Creatinine, mg/dL [median (Q1-Q3)] | 0.8 (0.7–1.0) | 0.9 (0.8–1.0) | 0.8 (0.6–1.0) | 0.165 |
| Basal Hemoglobin, g/dL [mean ± sd] | 13.2 ± 1.4 | 13.1 ± 0.8 | 13.2 ± 1.5 | 0.912 |
| Echocardiography | ||||
| Ejection Fraction, % [mean ± sd] | 61.1 ± 7.1 | 58.6 ± 2.7 | 61.6 ± 7.6 | 0.305 |
| LAD, mm [mean ± sd] | 42.8 ± 9.7 | 49.4 ± 7.2 | 41.0 ± 9.6 | 0.038 |
| LVED, mm [mean ± sd] | 49.6 ± 5.4 | 52.0 ± 6.6 | 49.0 ± 5.0 | 0.196 |
| IVS, mm [mean ± sd] | 13.4 ± 2.4 | 12.9 ± 3.4 | 13.6 ± 2.2 | 0.505 |
| LVPW, mm [mean ± sd] | 11.3 ± 1.7 | 11.5 ± 1.8 | 11.2 ± 1.7 | 0.736 |
| AMG, mmHg [mean ± sd] | 82.1 ± 21.2 | 78.4 ± 19.7 | 82.9 ± 21.6 | 0.444 |
| AMeanG, mmHg [mean ± sd] | 50.4 ± 12.6 | 48.8 ± 12.7 | 50.8 ± 12.6 | 0.559 |
| AVA, cm2 [mean ± sd] | 0.8 ± 0.2 | 0.7 ± 0.2 | 0.8 ± 0.2 | 0.576 |
| Variable | PF GDF-15 | S GDF-15 | PF NT-Pro-BNP | S NT-Pro-BNP |
|---|---|---|---|---|
| Fibrosis | 0.001 [−0.119–0.121], p = 0.983 | −0.037 [−0.180–0.106], p = 0.579 | 0.007 [−0.046–0.059], p = 0.794 | 0.011 [−0.062–0.085], p = 0.741 |
| COL1A1 | 2.1 × 10−5 [−6.2 × 10−5–1.0 × 10−4], p = 0.601 | 3.5 × 10−5 [−3.3 × 10−5–1.0 × 10−4], p = 0.226 | 2.9 × 10−5 [1.0 × 10−5–4.8 × 10−5], p = 0.005 | 4.0 × 10−6 [−4.9 × 10−5–5.7 × 10−5], p = 0.845 |
| COL3A1 | −1.6 × 10−5 [−2.3 × 10−4–1.9 × 10−4], p = 0.873 | 7.5 × 10−5 [−2.2 ×10−4–3.7 × 10−4], p = 0.516 | 6.0 × 10−5 [6.0 × 10−6–1.1 × 10−4], p = 0.033 | 5.4 × 10−5 [−1.3 × 10−4–2.4 × 10−4], p = 0.460 |
| TIMP4 | 1.2 × 10−4 [1.8 × 10−5–2.2 × 10−4], p = 0.025 | 1.1 × 10−5 [−1.7 × 10−4–1.9 × 10−4], p = 0.861 | −9.4 × 10−6 [1.2 × 10−4–9.9 × 10−5], p = 0.801 | 1.8 × 10−5 [−1.8 × 10−5–5.4 × 10−5], p = 0.309 |
| TIMP1 | −0.001 [−0.002–0.001], p = 0.339 | 7.0 × 10−5 [−0.003–0.004], p = 0.959 | 7.8 × 10−5 [-4.2 × 10−4–0.001], p = 0.739 | 0.001 [-4.1 × 10−4–0.003], p = 0.108 |
| MMP2 | −5.5 × 10−5 [−3.0 × 10−4–1.9 × 10−4], p = 0.632 | -9.2 × 10−5 [-0.001–3.3 × 10−4], p = 0.574 | 9.5 × 10−5 [1.6 × 10−5–1.7 × 10−4], p = 0.023 | 9.3 × 10−5 [-1.6 × 10−4–3.4 × 10−4], p = 0.359 |
| MMP9 | −2.2 × 10−6 [−2.9 × 10−5–2.4 × 10−5], p = 0.860 | −3.7 × 10−5 [−1.1 × 10−4–4.1 × 10−5], p = 0.257 | 9.0 × 10−8 [−1.0 × 10−6–2.0 × 10−6], p = 0.900 | 1.7 × 10−5 [−7.2 × 10−5–3.9 × 10−5], p = 0.446 |
| Variable [%(n)] | AF | SR | p Value |
|---|---|---|---|
| MACE | 15.8 (3) | 19.6 (21) | 1.000 |
| AKI | 57.9 (11) | 21.5 (23) | 0.001 |
| Hb Variation, g/dL [mean ± sd] | 4.6 ± 1.1 | 3.9 ± 1.6 | 0.017 |
| Hospital Stay (>75th Percentile) | 9.0 (3) | 7.0 (5) | 0.053 |
| Outcome [Median (Q1–Q3)] | PF GDF-15 | p Value | S GDF-15 | p Value | PF NT-Pro-BNP | p Value | S NT-Pro-BNP | p Value | |
|---|---|---|---|---|---|---|---|---|---|
| MACE | Y | 714.1 (400.0–1009.8) | 0.760 | 1268.0 (807.7–1675.0) | 0.602 | 1479.4 (593.8–5782.5) | 0.824 | 260.1 (159.8–602.8) | 0.856 |
| n | 703.5 (476.2–1044.3) | 1069.0 (769.3–1910.0) | 1201.5 (633.1–3625.5) | 358.6 (155.2–840.1) | |||||
| AKI | Y | 826.5 (622.9–1316.0) | 0.027 | 1728.5 (963.2–2863.0) | 0.015 | 1554.0 (864.5–6178.5) | 0.096 | 409.7 (171.4–643.7) | 0.654 |
| n | 621.2 (406.7–912.0) | 1007.0 (717.9–1777.0) | 1014.0 (476.6–2902.0) | 316.6 (155.8–878.7) | |||||
| POAF | Y | 826.5 (419.3–1230.5) | 0.435 | 1194.0 (902.5–1942.5) | 0.076 | 1578.5 (586.4–4712.8) | 0.298 | 407.4 (199.1–745.6) | 0.096 |
| n | 606.6 (400.0–962.0) | 935.2 (700.5–1821.0) | 864.6 (460.2–1729.8) | 221.7 (129.0–596.3) | |||||
| Hb Variation (>75th Percentile) | Y | 686.7 (403.4–838.5) | 0.291 | 954.2 (692.4–2337.5) | 0.530 | 784.4 (408.6–2090.5) | 0.146 | 199.1 (104.8–522.6) | 0.182 |
| n | 733.2 (494.0–1205.8) | 1203.0 (856.9–1849.3) | 1342 (664.5–4712.8) | 392.5 (166.8–876.0) | |||||
| Hospital Stay (>75th Percentile) | Y | 826.5 (467.3–1287.5) | 0.348 | 1675.0 (860.8–2574.0) | 0.085 | 1579.5 (633.1–11867.3) | 0.314 | 412.0 (151.8–1331.5) | 0.386 |
| n | 654.3 (437.4–1024) | 1035.5 (760.0–1820.5) | 1201.5 (596.0–3279.8) | 310.3 (156.8–727.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fragão-Marques, M.; Barroso, I.; Farinha, R.; Miranda, I.M.; Martins, D.; Mancio, J.; Rocha-Neves, J.; Guimarães, J.T.; Leite-Moreira, A.; Falcão-Pires, I. Pericardial NT-Pro-BNP and GDF-15 as Biomarkers of Atrial Fibrillation and Atrial Matrix Remodeling in Aortic Stenosis. Diagnostics 2021, 11, 1422. https://doi.org/10.3390/diagnostics11081422
Fragão-Marques M, Barroso I, Farinha R, Miranda IM, Martins D, Mancio J, Rocha-Neves J, Guimarães JT, Leite-Moreira A, Falcão-Pires I. Pericardial NT-Pro-BNP and GDF-15 as Biomarkers of Atrial Fibrillation and Atrial Matrix Remodeling in Aortic Stenosis. Diagnostics. 2021; 11(8):1422. https://doi.org/10.3390/diagnostics11081422
Chicago/Turabian StyleFragão-Marques, Mariana, Isaac Barroso, Rui Farinha, Isabel M Miranda, Diana Martins, Jennifer Mancio, João Rocha-Neves, João T Guimarães, Adelino Leite-Moreira, and Inês Falcão-Pires. 2021. "Pericardial NT-Pro-BNP and GDF-15 as Biomarkers of Atrial Fibrillation and Atrial Matrix Remodeling in Aortic Stenosis" Diagnostics 11, no. 8: 1422. https://doi.org/10.3390/diagnostics11081422
APA StyleFragão-Marques, M., Barroso, I., Farinha, R., Miranda, I. M., Martins, D., Mancio, J., Rocha-Neves, J., Guimarães, J. T., Leite-Moreira, A., & Falcão-Pires, I. (2021). Pericardial NT-Pro-BNP and GDF-15 as Biomarkers of Atrial Fibrillation and Atrial Matrix Remodeling in Aortic Stenosis. Diagnostics, 11(8), 1422. https://doi.org/10.3390/diagnostics11081422